Factors Associated with Outpatient Satisfaction in Tertiary Hospitals in China: A Systematic Review



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Inclusion and Exclusion Criteria
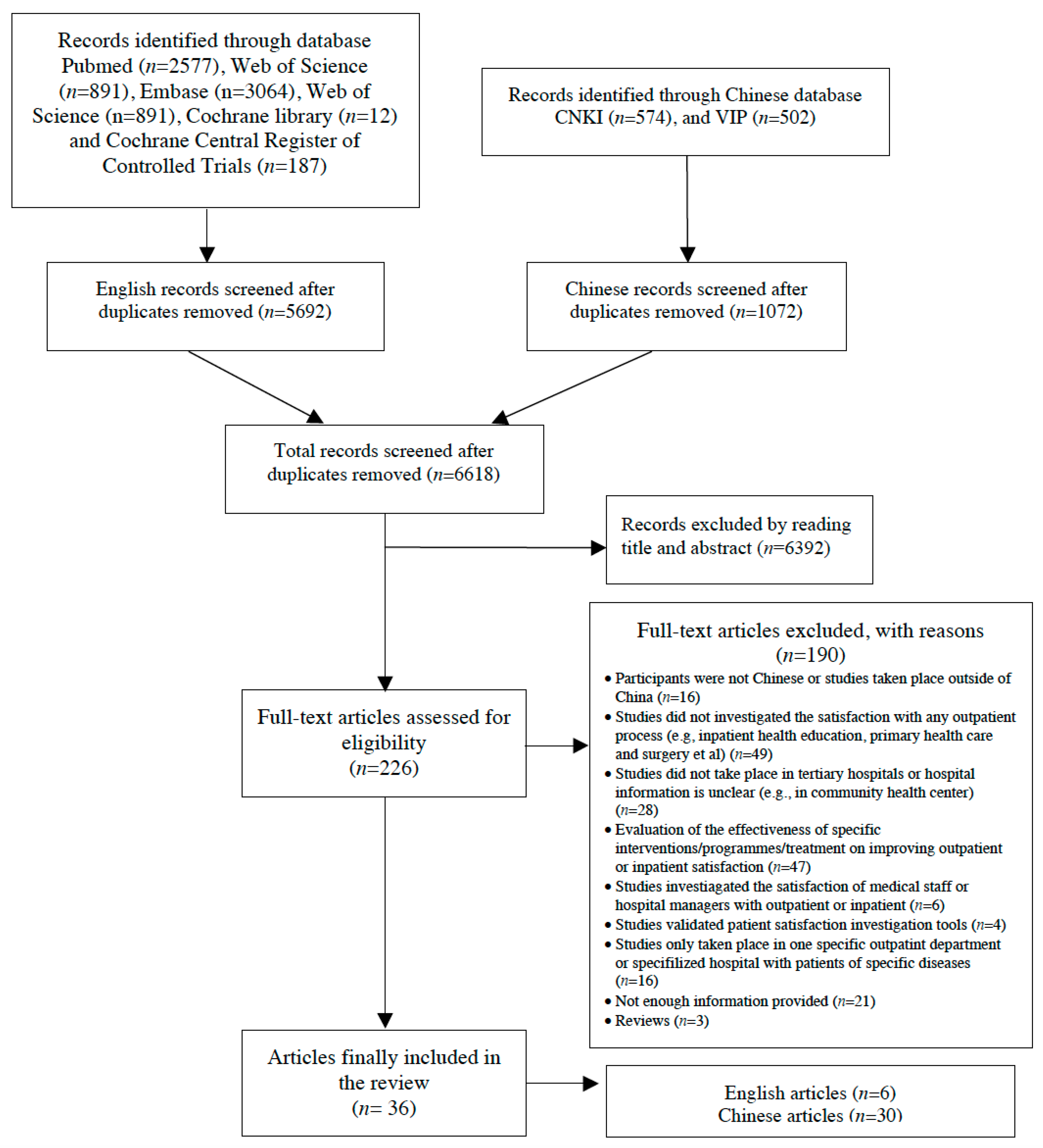
2.2. Search Strategy and Selection Criteria
2.3. Data Extraction and Analysis
2.4. Quality Assessment
3. Results
3.1. Characteristics of Included Studies
3.2. Measures of Outpatient Satisfaction and the Study Quality
3.3. Overall Satisfaction Level
3.4. Relationships between Outpatient Satisfaction and Influencing Factors
3.4.1. Patient Social-Demographic Factors
3.4.2. Medical Staff Factors
3.4.3. Hospital Indoor Hygiene, Facilities, and Process Management Factors
4. Discussion
4.1. Methodological Issues and Study Quality
4.2. Overall Satisfaction
4.3. Patient Social-Demographic Factors
4.4. Medical Staff Factors
4.5. Process Management Factors
4.6. Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Zhang, W.; Deng, Z.; Evans, R.; Xiang, F.; Ye, Q.; Zeng, R. Social media landscape of the tertiary referral hospitals in china: Observational descriptive study. J. Med. Internet Res. 2018, 20, e249. [Google Scholar] [CrossRef] [PubMed]
- National Health and Family Planning Commission of the People’s Republic of China. The Situation of National Medical Service Delivery in China in 2014. Available online: http://www.nhfpc.gov.cn/mohwsbwstjxxzx/s7967/201501/0faf05af332b4f9f83bc1244b84f6dfb.html (accessed on 28 August 2019).
- Liu, C.; Liu, W.; Wang, Y.; Zhang, Z.; Wang, P. Patient safety culture in China: A case study in an outpatient setting in Beijing. Bmj Qual. Saf. 2014, 23, 556–564. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.Q.; Wang, X.T.; Zheng, J.J. How to end violence against doctors in china. Lancet 2012, 380, 647–648. [Google Scholar] [CrossRef]
- Jiang, Y.; Ying, X.; Kane, S.; Mukhopadhyay, M.; Qian, X. Violence against doctors in china. Lancet 2014, 384, 744–745. [Google Scholar] [CrossRef]
- Chinese doctors becoming the targets of patients’ anger. Available online: https://sinosphere.blogs.nytimes.com/2013/11/01/doctors-the-targets-of-patients-anger/ (accessed on 23 September 2020).
- Li, J.; Wang, P.; Kong, X.; Liang, H.; Zhang, X.; Shi, L. Patient satisfaction between primary care providers and hospitals: A cross-sectional survey in jilin province, china. Int. J. Qual. Health Care 2016, 28, 346–354. [Google Scholar] [CrossRef]
- Wang, W.Y. Multivariate analysis on satisfaction with health care services of outpatients. J. Occup. Health 2010, 26, 92–94. [Google Scholar]
- Liao, H.Q.; Zen, X.Y.; Ren, Y.Q.; Zen, Q.X. Analysis of outpatient satisfaction and influencing factors in a certain hospital of shenzhen. Chin. J. Health Stat. Med. 2010, 27, 375–376. [Google Scholar]
- Wang, C.M. Survey and analysis of outpatient satisfaction. J. North Pharm. 2013, 10, 138–139. [Google Scholar]
- Xie, Z.Z.; Or, C. Associations between waiting times, service times, and patient satisfaction in an endocrinology outpatient department: A time study and questionnaire survey. Inq. J. Med Care Organ. Provis. Financ. 2017, 54, 46958017739527. [Google Scholar] [CrossRef]
- Yu, W.; Li, M.; Xue, C.; Wang, J.; Liu, J.; Chen, H.; Zhang, L. Determinants and influencing mechanism of outpatient satisfaction: A survey on tertiary hospitals in the people’s republic of china. Patient Prefer. Adher. 2016, 10, 601–612. [Google Scholar]
- Yan, Z.; Wan, D.; Li, L. Patient satisfaction in two Chinese provinces: Rural and urban differences. Int. J. Qual. Health Care 2011, 23, 384–389. [Google Scholar] [CrossRef] [PubMed]
- Violence against doctors: Why china? Why now? What next? Lancet 2014, 383, 1013. [CrossRef]
- Xu, G.C.; Zheng, J.; Zhou, Z.J.; Zhou, C.K.; Zhao, Y. Comparative study of three commonly used methods for hospital efficiency analysis in beijing tertiary public hospitals, china. Chin. Med. J. 2015, 128, 3185–3190. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The prisma statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed]
- Ryan, R.; Synnot, A.; Prictor, M.; Hill, S. Cochrane Consumers and Communication Group Data Extraction Template for Included Studies. Available online: http://cccrg.cochrane.org/author-resources. (accessed on 23 September 2020).
- Tang, L. The influences of patient’s trust in medical service and attitude towards health policy on patient’s overall satisfaction with medical service and sub satisfaction in china. BMC Public Health 2011, 11, 472. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.Y.; Sun, J.; Hu, G.Y.; Liu, Y.L. Satisfaction of elderly patients with out-patient services: A study based on the 2015 evaluation of the national health care improvement initiative. Chin J Evid-based Med. 2016, 16, 1256–1262. [Google Scholar]
- Sun, J.; Li, S. Experience and associated factors of consultation among primary care outpatients from the grade a tertiary general hospital. Chin. Gen. Pract. 2018, 21, 774–777. [Google Scholar]
- Bao, C.; Zhou, Y.; Li, J.; Wu, F.; Cao, J.; Tian, J. Investigation and analysis of outpatients’ satisfaction of 2170 cases. Chin. Hosp. Manag. 2015, 35, 34–36. [Google Scholar]
- Luan, J.; Dong, J.; Bao, Y. Relevance of patient satisfaction with health care to trust in residents from nantong area. Chin. J. Gen. Pract. 2013, 11, 1928–1931. [Google Scholar]
- Han, C.; Zhang, Y.; Ding, R. The outpatient satisfaction investigation in new health reform background. Chin. J. Health Stat. 2012, 29, 849–851. [Google Scholar]
- Teng, Z.; Li, G.; Lan, Y. Exploration of the associate between the health seeking experience and the outpatient satisfaction. Chin. J. Health Stat. 2009, 26, 413–414. [Google Scholar]
- Hu, W.L.; Wang, S.Y.; Xie, L.W. Analysis of satisfaction investigation to outpatient service in xuzhou tertiary hospital. Chin. J. Hosp. Stat. 2007, 14, 251–253. [Google Scholar]
- Sun, J.; Hu, G.; Ma, J.; Chen, Y.; Wu, L.; Liu, Q.; Hu, J.; Livoti, C.; Jiang, Y.; Liu, Y. Consumer satisfaction with tertiary healthcare in china: Findings from the 2015 china national patient survey. Int. J. Qual. Health Care 2017, 29, 213–221. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Li, J.; Cao, X. An empirical study on influencing factors of patient satisfaction with medical treatment. Jouenal Beijing Inst. Technol. Soc. Sci. Ed. 2018, 20, 102–109. [Google Scholar]
- Xie, J.; Hu, Y.; Lu, C. Factors associated with outpatient experience of chinese public hospitals: A cross-sectional study. Lancet 2017, 390, s38. [Google Scholar] [CrossRef]
- Lu, Q.; Zhang, T.; Zeng, L.; Wu, T.; Li, X. Investigation and analysis on the satisfaction degree of outpatients in public hospitals in beijing. Mod. Hosp. 2016, 16, 225–230. [Google Scholar]
- Zhou, Z.; Mei, C.; Zhang, Y.; Shao, J. Study on satisfaction degree of outpatients in a notched hospital. Mod. Prev. Med. 2011, 38, 1262–1265. [Google Scholar]
- Pan, J.; Liu, D.; Ali, S. Patient dissatisfaction in china: What matters. Soc. Sci. Med. 2015, 143, 145–153. [Google Scholar] [CrossRef]
- Xu, R.; Jing, X. Study on satisfaction degree in outpatients. Soft Sci. Health 2004, 18, 252–256. [Google Scholar]
- Yang, Y.; Zhang, C. Analysis on the factors of polyclinic patients satisfaction. Soft Sci. Health 2015, 29, 147–149. [Google Scholar]
- Zhao, J.; Wang, L.; Chen, K. Outpatient satisfaction in tertiary hospital. Southwest Natl. Def. Med. 2015, 26, 228–230. [Google Scholar]
- Xun, M.J.; Xiang, J.Z.; Shu, L.Z. Study on patient satisfaction measurement and outpatient service process reengineering based on different treatment chains. Chin. Hosp. 2010, 14, 13–15. [Google Scholar]
- Deng, M.; Geng, Y. Investigation and analysis of outpatient satisfaction on non-technical quality. Chin. Hosp. Manag. 2013, 33, 35–37. [Google Scholar]
- Li, Y.; Wang, X.; Yang, H.; Zhu, Y. Investigation on outpatient service needs and satisfaction in five tertiary comprehensive hospitals in tianjin city. Chin. Hosp. Manag. 2011, 31, 57–59. [Google Scholar]
- Meng, F.Z.; Zhang, F.Y.; Gonggacizhen; Zhaxideji; Ma, S.P.; Zhaxidawa. Hospital visit and satisfaction with medical treatment among poor farmers and herdsmen in Tibet. Chin. Rural Health Serv. Adm. 2016, 36, 959–962. [Google Scholar]
- Shu, J.; Zhou, D. Outpatients satisfaction in a tertiary hospital of anhui province. Chin. Rural Health Serv. Adm. 2016, 36, 725–729. [Google Scholar]
- Ren, C.; Wang, Y.; Zhao, S. Investigation of the outpatient satisfaction in changchun. Contemp. Econ. 2014, 4, 36–38. [Google Scholar]
- Zhang, Q.; Liu, Z. Investigation of the outpatient satisfaction. Hebei Med. 2011, 33, 3000–3001. [Google Scholar]
- Song, J.; Xu, R.; Chen, Y. Investigation and analysis on the satisfaction of current outpatient service flow. Jiangsu Healthc. Adm. 2007, 18, 22–23. [Google Scholar]
- Luo, H.; Peng, C.; Wang, J. Analysis of factors related to outpatients dissatisfaction and strategies improving satisfaction. J. Qiqihar Med Coll. 2010, 31, 1608–1612. [Google Scholar]
- Guo, S.; Hu, H.; Wang, B. Investigation on the patient satisfaction on the outpatient clinic of a general hospital basis. J. Wannan Med. Coll. 2014, 33, 80–83. [Google Scholar]
- Jing, G.; Piao, S. Investigation of the factors influencing the outpatient satisfaction and interventions. Med. Inf. 2011, 24, 11. [Google Scholar]
- Deng, L.; Rao, S. Analysis of the factors influencing the outpatient satisfaction and interventions. Med. Soc. 2006, 19, 54–55. [Google Scholar]
- Ling, K.; Yang, M.; Zhong, Q.; CHen, M. Survey and strategies of outpatients satisfaction of senior patients. Mod. Hosp. 2009, 19, 123–124. [Google Scholar]
- Zou, Y.; Wang, L.; Peng, Q. Survey of satisfaction of outpatients based on different clinics. Nurs. Res. 2014, 28, 3231–3233. [Google Scholar]
- Ren, L.; Xu, H. Investigation of outpatient satisfaction in a tertiary hospital. Qilu J. Nurs. 2016, 22, 51–52. [Google Scholar]
- Shao, W.; Liu, D.; Lv, M. Survey of outpatient satisfaction of a tertiary hospital in xinjiang province. World Latest Med. Inf. Electron. Version 2017, 17, 136–137. [Google Scholar]
- Zulipiye, T.; Liu, C.; Yang, Y.; Bahaer, A. Investigation and analysis on the satisfaction of outpatients in a general hospital in xinjiang. Xinjiang Med. J. 2016, 46, 688–689. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Prisma Group. Preferred reporting items for systematic reviews and meta-analyses: The prisma statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef]
- Mahtani, K.; Heneghan, C.; Aronson, J. Single screening or double screening for study selection in systematic reviews? BMJ Evid. Based Med. 2020, 25, 149–150. [Google Scholar] [CrossRef]
- Wei, J.; Shen, L.; Yang, H.B.; Qin, J.B.; Huang, W.; Zhang, J.J.; Gonga, Q.-Y.; Lia, X.-X.; Yanga, T.-B. Development and validation of a Chinese outpatient satisfaction questionnaire: Evidence from 46 public general hospitals and 5151 outpatients. Public Health 2015, 129, 1523–1529. [Google Scholar] [CrossRef] [PubMed]
- Brent Graham. Defining and Measuring Patient Satisfaction. J. Hand Surg. 2016, 14, 929–931. [Google Scholar]
- Centers for Medicare & Medicaid Services. Consumer Assessment of Health Care Providers and Systems (CAHPS) Hospital Survey. Available online: https://hcahpsonline.org (accessed on 22 August 2020).
- Hu, Y.; Zhang, Z. Skilled doctors in tertiary hospitals are already overworked in china. Lancet Glob. Health 2015, 3, 737. [Google Scholar] [CrossRef]
- Mohd, A.; Chakravarty, A. Patient satisfaction with services of the outpatient department. Med. J. Armed Forces India. 2014, 70, 237–242. [Google Scholar] [CrossRef] [PubMed]
- McCollum, R.; Chen, L.; ChenXiang, T.; Liu, X.; Starfield, B.; Jinhuan, Z.; Tolhurst, R. Experiences with primary healthcare in fuzhou, urban china, in the context of health sector reform: A mixed methods study. Int. J. Health plan. M. 2014, 29, 107–126. [Google Scholar] [CrossRef]
- Hall, J.A.; Irish, J.T.; Roter, D.L.; Ehrlich, C.M.; Miller, L.H. Satisfaction, gender and communication in medical visits. Med. Care 1994, 32, 1216–1231. [Google Scholar] [CrossRef]
- Hall, J.A.; Dornan, M.C. Patient sociodemographic characteristics as predictors of satisfaction with medical care: A meta-analysis. Soc. Sci. Med. 1990, 30, 811–818. [Google Scholar] [CrossRef]
- Ware, J.E., Jr.; Davies-Avery, A.; Stewart, A.L. The measurement and meaning of patient satisfaction. Health Med. Care Serv. Rev. 1978, 1, 1–3. [Google Scholar]
- Harpole, L.H.; Orav, E.J.; Hickey, M.; Posther, K.E.; Brennan, T.A. Patient satisfaction in the ambulatory setting: Influence of data collection methods and socioeconomic factors. J. Gen. Intern. Med. 1996, 11, 431–434. [Google Scholar] [CrossRef]
- Blendon, R.J.; Aiken, L.H.; Freeman, H.E.; Corey, C.R. Access to medical care for black and white Americans: A matter of continuing concern. JAMA 1989, 261, 278–281. [Google Scholar] [CrossRef]
- Li, S.; Liu, Y. The achievements, problems and experiences of the health service development in china’s 30 year reform and opening-up. Chin. J. Health Policy 2008, 11, 3–8. [Google Scholar]
- Peng, L.; Ran, S.J. Teaching doctor–patient communication for medical students: A situation and reflection on curriculum design. Chongqing Med. 2011, 40, 2594–2595. [Google Scholar]
- Liu, X.; Rohrer, W.; Luo, A.; Fang, Z.; He, T.; Xie, W. Doctor-patient communication skills training in mainland china: A systematic review of the literature. Patient Educ. Couns. 2015, 98, 3–14. [Google Scholar] [CrossRef]
- Bleustein, C.; Rothschild, D.B.; Valen, A.; Valatis, E.; Schweitzer, L.; Jones, R. Wait times, patient satisfaction scores, and the perception of care. Am. J. Manag. Care 2014, 20, 393–400. [Google Scholar] [PubMed]
- Anderson, R.T.; Camacho, F.T.; Balkrishnan, R. Willing to wait?: The influence of patient wait time on satisfaction with primary care. BMC Health Serv. Res. 2007, 7, 31. [Google Scholar] [CrossRef] [PubMed]
- Shen, Q.; Tang, L.; Feng, Y.; Tang, J. The imbalance between patients needs and the limited competence of top-level health providers in urban china: An empirical study. Med. Eco. Applied Eco. Mod. J. 2010. [Google Scholar] [CrossRef]
- Huang, X.M. Patient attitude towards waiting in an outpatient clinic and its applications. Health Serv. Manag. Res. 1994, 7, 2–8. [Google Scholar] [CrossRef]
- Vesna, V.S.; Miodraga, S.P. Patient satisfaction in outpatient healthcare services at secondary level vs. tertiary level. Srpski Arhiv za Celokupno Lekarstvo 2014, 142, 579–585. [Google Scholar]
- Ho, E.T. Improving waiting time and operational clinic flow in a tertiary diabetes center. BMJ Qual. Improv. Rep. 2014, 2, 2. [Google Scholar] [CrossRef]
- Prakash, B. Patient satisfaction. J. Cutan. Aesthet. Surg. 2010, 3, 151–155. [Google Scholar] [CrossRef]
- Liu, G.G.; Vortherms, S.A.; Hong, X. China’s health reform update. Annu. Rev. Public Health. 2017, 38, 431–448. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Author and Year | Study Context | Number of Participants | Participant Information | Sampling Methods | Study Design |
|---|---|---|---|---|---|
| Wenya, Yu et al., 2016 | 11 tertiary hospitals in Shanghai | 1050 outpatients from different clinical departments with varying diseases | Male: 439 Female: 532 Age was normally distributed, with the most prevalent age group 30–39 (24.41%). | Random selection | cross-sectional survey |
| Liyang, Tang. 2011 | A household survey in 17 provinces | 3424 residents | Urban residents: 3209 (93.76%) Rural residents: 34 (6.24%) | NR * | cross-sectional survey |
| Jing Sun et al., 2017 Laiyang, Wu et al., 2016 † | 136 tertiary hospitals from 31 provinces | 27,475 outpatients, of which 3923 are senior outpatients older than 60 | Male: 8792 Female: 18,683 | Random selection and convenient sampling | cross-sectional survey |
| Jay Pan et al., 2015 | Survey with residents who had visited hospitals in the past 2 weeks | 6393 residents | 2621 male, 3772 female Mean age: 57.3 y | A multistage cluster sampling | cross-sectional survey |
| Jinghua, Li et al., 2016 | Household survey in health care facilities in Jiling Province | 68 residents had at least one outpatient visit in the past 2 weeks in tertiary hospitals. | 29 male 39 female Age range: 45–64 y; | A multi-stage stratified sampling | cross-sectional survey |
| Jinzhu, Xie et al., 2017 | Three tertiary hospitals in Hubei Province | 300 outpatients | NR | NR | cross-sectional survey |
| Chunlei, Han et al., 2012 | One Tertiary hospital in Shandong Province | 338 outpatients | Male 148 Female 190 | A stratified random sampling | cross-sectional survey |
| Qing Lu et al., 2016 | 3 public hospitals in Beijing | 318 outpatients | Male: 137 Female: 181 | Random sampling | cross-sectional survey |
| Jing Zhao et al., 2016 | A tertiary hospital | 197 outpatients | Male: 108 Female: 89 Mean age: 43.3 ± 7.3 | Random sampling | cross-sectional survey |
| Wenlong, Hu et al., 2007 | 2 tertiary hospital in Xuzhou | 386 outpatients | Male: 253 Female: 132 | Random sampling | cross-sectional survey |
| Yanxia, Yang et al., 2015 | A tertiary hospital | 1998 outpatients | 1998 outpatients Male: 993 Female: 995 Aged range: 20–70 | NR | cross-sectional survey |
| Rong Xu and Xinzhen, Jing. 2004 | A tertiary hospital in Guangdong Province | 304 outpatients | 304 outpatients Male: 120 Female: 175 | NR | cross-sectional survey |
| Junjie, Sun and Shuangqing, Li. 2018 | A tertiary hospital in Sichuan Province | 185 outpatients | Male: 68 Female: 117 | Random sampling | cross-sectional survey |
| Zhanwei, Zhou et al., 2011 | A tertiary hospital | 363 outpatients | Male: 211 Female: 152 Mean age: 45.3 ± 11.8 | Random sampling | cross-sectional survey |
| Caoxin, Bao et al., 2015 | 5 tertiary hospitals | 2170 outpatient | 2170 outpatients Male: 870 Female: 1300 | Random sampling | cross-sectional survey |
| Zhixiang, Teng et al., 2009 | Residents survey | 134 residents who visited the hospitals in the last year, of whom, 40 visited the tertiary hospital | NR | Convenient sampling | cross-sectional survey |
| Jing Luan et al., 2013 | Residents survey | 510 residents | Male: 178 Female: 332 | Random sampling | cross-sectional survey |
| Jianjie, Zhang. 2018 | Residents survey | 484 residents | NR | Random sampling | cross-sectional survey |
| Chunhui, Ren. 2014 | Residents Survey | 329 participants | NR | NR | cross-sectional survey |
| Weiming, Shao et al., 2017 | A tertiary hospital | 600 outpatients | NR | Random sampling | cross-sectional survey |
| Ying Zou et al., 2014 | A Tertiary hospital in Xiniiang Province | 1300 outpatients | NR | Random sampling | cross-sectional survey |
| Mengzhu, Deng et al., 2013 | A Tertiary hospital in Guangdong Province | 200 outpatients | Male: 110 Female: 90 | Random sampling | cross-sectional survey |
| Huilan, Luo et al., 2010 | A tertiary hospital in Guangdong Province | 1591 outpatients | NR | Random sampling | cross-sectional survey |
| Zulipiye.et al., 2016 | A tertiary hospital in Xinjiang Province | 1300 outpatients | Female: 736 Male: 564 Age range: 18–69 y | Random sampling | cross-sectional survey |
| Jinping, Shu and Dian Zhou. 2016 | A tertiary hospital in Anhui Province | 396 outpatients | Male: 171 Female: 225 | Stratified cluster sampling | cross-sectional survey |
| Kai ling et al., 2009 | A tertiary hospital | 500 outpatients | Male: 307 Female: 193 Aged range: 60–85 | NR | cross-sectional survey |
| Yu Li et al., 2011 | Five tertiary Hospitals in Tianjian City | 995 outpatients | Male: 438 Female: 557 Aged range: 20–70 | Random sampling | cross-sectional survey |
| Qinghua, Zhang and Zhanhe, Liu. 2011 | A tertiary hospital in Hebei Province | 817 outpatients | NR | Random sampling | cross-sectional survey |
| Fanzhi, Meng et al., 2016 | Residents survey covering 2 cities, 3 counties and 5 villages in Tibet province | 777 residents | Male: 369 Female: 408 Age range: 18–40 | Stratified clustered random sampling | cross-sectional survey |
| Jun Song et al., 2007 | A tertiary hospital in Jiangsu Province | 93 outpatients | Male: 49 Female: 44 Mean age: 37.6 ± 4.3 y | Random sampling | cross-sectional survey |
| Shi Guo et al., 2014 | A tertiary hospital in Anhui Province | 239 outpatients | Male: 118 Female: 121 | Stratified random sampling | cross-sectional survey |
| Xunming, Ji et al., 2010 | A tertiary hospital in Beijing | 504 outpatients | Media age: 47 | Convenient sampling | cross-sectional survey |
| Li Ren and Haixuan, Xu. 2016 | A tertiary hospital in Shandong Province | 488 outpatients | Male: 216 Female: 272 | Random sampling | cross-sectional survey |
| Guanghao, Jing and Shunfu, Piao. 2011 | A tertiary hospital | 597 outpatients | NR | NR | cross-sectional survey |
| Lizhen, Deng and Suili, Rao. 2006 | A tertiary hospital | 1226 outpatients | NR | Random sampling | cross-sectional survey |
| Author and Year | Sample Selection Criteria (Maximum of 4 Stars) | Comparability (Maximum 2 Stars) | Outcome (Maximum 1 Star) | Summary Score (Maximum of 7 Stars) | |||
|---|---|---|---|---|---|---|---|
| Representativeness of the Sample | Sample Size | Non-Respondents | Ascertainment of the Satisfaction Level | Comparability of Subjects in Different Outcome Groups; Control of Confounding Factors. | Assessment of the Outcome from Patient’s Point of View | ||
| Wenya, Yu et al., 2016. Shanghai | Truly representative of the average in the target population * | Justified and satisfactory * | Comparability between respondents’ and nonrespondents’ characteristics is established, and the response rate is satisfactory * | Validated measurement tool * | The study controls for the most important factor **; | Self-report * | 7 |
| Liyang Tang, 2011 | Somewhat representative of the average in the target population * | Justified and satisfactory * | Comparability between respondents’ and nonrespondents’ characteristics is established, and the response rate is satisfactory * | Non validated measurement tool, but the tool is available or described *; | The study controls for the most important factor **; | Self-report * | 7 |
| Jing Sun, et al., 2017 Laiyang Wu, et al., 2016 | Truly representative of the average in the target population * | Justified and satisfactory * | No description | Non validated measurement tool, but the tool is available or described *; | The study controls for the most important factor **; | Self-report * | 6 |
| Jay Pan, et al., 2015 | Truly representative of the average in the target population * | Justified and satisfactory * | Comparability between respondents’ and nonrespondents’ characteristics is established, and the response rate is satisfactory * | Validated measurement tool * | The study controls for the most important factor **; | Self-report * | 7 |
| Jinghua Li et al., 2016 | Truly representative of the average in the target population * | Justified and satisfactory * | Comparability between respondents’ and nonrespondents’ characteristics is established, and the response rate is satisfactory * | Non validated measurement tool, but the tool is available or described *; | The study controls for the most important factor **; | Self-report * | 7 |
| Jinzhu Xie, et al., 2017 | Somewhat representative of the average in the target population * | Not justified | Comparability between respondents’ and nonrespondents’ characteristics is established, and the response rate is satisfactory * | Non validated measurement tool, but the tool is available or described *; | The study controls for the most important factor **; | Self-report * | 6 |
| Chunlei Han et al., 2000 | Truly representative of the average in the target population * | Not justified | Comparability between respondents’ and nonrespondents’ characteristics is established, and the response rate is satisfactory * | Non validated measurement tool, but the tool is available or described *; | data not adjusted for all relevant confounders | Self-report * | 4 |
| Qing Lu et al., 2016 | Truly representative of the average in the target population * | Not justified | Comparability between respondents’ and nonrespondents’ characteristics is established, and the response rate is satisfactory * | Non validated measurement tool, but the tool is available or described *; | NA | Self-report * | 4 |
| Jing Zhao et al., 2015 | Truly representative of the average in the target population * | Not justified | Comparability between respondents’ and nonrespondents’ characteristics is established, and the response rate is satisfactory * | Non validated measurement tool, but the tool is available or described *; | NA | Self-report * | 4 |
| Wenlong Hu et al., 2007 | Truly representative of the average in the target population * | Not justified | Comparability between respondents’ and nonrespondents’ characteristics is established, and the response rate is satisfactory * | Non validated measurement tool, but the tool is available or described *; | NA | Self-report * | 4 |
| Yanxia Yang et al., 2015 | Truly representative of the average in the target population * | Not justified | Comparability between respondents’ and nonrespondents’ characteristics is established, and the response rate is satisfactory * | Non validated measurement tool, but the tool is available or described *; | data not adjusted for all relevant confounders | Self-report * | 4 |
| Rong Xu and Xinzhen Jing. 2004 | Somewhat representative of the average in the target population * | Not justified | No description | Validated measurement tool * | NA | Self-report * | 3 |
| Junjie Sun and Shuangqing Li, 2018 | Somewhat representative of the average in the target population * | Not justified | Comparability between respondents’ and nonrespondents’ characteristics is established, and the response rate is satisfactory * | Validated measurement tool * | data not adjusted for all relevant confounders | Self-report * | 4 |
| Zhanwei Zhou, et al., 2011 | Truly representative of the average in the target population * | Justified and satisfactory * | Comparability between respondents’ and nonrespondents’ characteristics is established, and the response rate is satisfactory * | No description | data not adjusted for all relevant confounders | Self-report * | 3 |
| Caoxin, Bao, et al., 2015 | Truly representative of the average in the target population * | Justified and satisfactory * | No description | Validated measurement tool * | NA | Self-report * | 4 |
| Zhixiang, Teng, et al., 2009 | Somewhat representative of the average in the target population * | Not justified | Response rate is unsatisfactory, or the comparability between respondents and nonrespondens is unsatisfactory; | Validated measurement tool * | NA | Self-report * | 3 |
| Jing Luan, et al., 2013 | Truly representative of the average in the target population * | Justified and satisfactory * | Comparability between respondents’ and nonrespondents’ characteristics is established, and the response rate is satisfactory * | Validated measurement tool * | NA | Self-report * | 5 |
| Jianjie Zhang. 2018 | Truly representative of the average in the target population * | Not justified | Comparability between respondents’ and nonrespondents’ characteristics is established, and the response rate is satisfactory * | Validated measurement tool * | The study controls for the most important factor **; | Self-report * | 6 |
| Chunhui, Ren. 2014 | Selected group of patients | Not justified | Comparability between respondents’ and nonrespondents’ characteristics is established, and the response rate is satisfactory * | Validated measurement tool * | NA | Self-report * | 3 |
| Weiming Shao et al., 2017 | Truly representative of the average in the target population * | Not justified | Comparability between respondents’ and nonrespondents’ characteristics is established, and the response rate is satisfactory * | Non validated measurement tool, but the tool is available or described *; | NA | Self-report * | 4 |
| Ying Zou et al., 2014 | Truly representative of the average in the target population * | Not justified | Comparability between respondents’ and nonrespondents’ characteristics is established, and the response rate is satisfactory * | Validated measurement tool * | NA | Independent blind assessment * | 4 |
| Mengzhu Deng et al., 2013 | Somewhat representative of the average in the target population * | Not justified | Comparability between respondents’ and nonrespondents’ characteristics is established, and the response rate is satisfactory * | Validated measurement tool * | data not adjusted for all relevant confounders | Self-report * | 4 |
| Huilan Luo et al., 2010 | Truly representative of the average in the target population * | Not justified | Comparability between respondents’ and nonrespondents’ characteristics is established, and the response rate is satisfactory * | Validated measurement tool * | NA | Self-report * | 4 |
| Zulipiye Tuerxun et al., 2016 | Truly representative of the average in the target population * | Not justified | Comparability between respondents’ and nonrespondents’ characteristics is established, and the response rate is satisfactory * | Non validated measurement tool, but the tool is available or described *; | NA | Self-report * | 4 |
| Jinping Shu and Dian Zhou, 2016 | Truly representative of the average in the target population * | Not justified | Comparability between respondents’ and nonrespondents’ characteristics is established, and the response rate is satisfactory * | Validated measurement tool * | The study controls for the most important factor **; | Self-report * | 6 |
| Kai Ling et al., 2009 | Somewhat representative of the average in the target population * | Not justified | Comparability between respondents’ and nonrespondents’ characteristics is established, and the response rate is satisfactory * | Non validated measurement tool, but the tool is available or described *; | NA | No description. | 3 |
| Yu Li, et al., 2011 | Truly representative of the average in the target population * | Not justified | Comparability between respondents’ and nonrespondents’ characteristics is established, and the response rate is satisfactory * | Non validated measurement tool, but the tool is available or described *; | NA | Self-report * | 4 |
| Qinghua Zhang and Zhanhe Liu. 2011 | Truly representative of the average in the target population * | Not justified | Comparability between respondents’ and nonrespondents’ characteristics is established, and the response rate is satisfactory * | Non validated measurement tool, but the tool is available or described *; | NA | Self-report * | 4 |
| Zhifan Meng, et al., 2016 | Truly representative of the average in the target population * | Not justified | Comparability between respondents’ and nonrespondents’ characteristics is established, and the response rate is satisfactory * | Non validated measurement tool, but the tool is available or described *; | NA | Self-report * | 4 |
| Jun Song, et al., 2007 | Truly representative of the average in the target population * | Not justified | Comparability between respondents’ and nonrespondents’ characteristics is established, and the response rate is satisfactory * | Non validated measurement tool, but the tool is available or described *; | NA | Self-report * | 4 |
| Shi Guo, et al., 2014 | Truly representative of the average in the target population * | Not justified | Comparability between respondents’ and nonrespondents’ characteristics is established, and the response rate is satisfactory * | Non validated measurement tool, but the tool is available or described *; | NA | Self-report * | 4 |
| Xunming Ji, et al., 2010 | Somewhat representative of the average in the target population * | Not justified | No description | Non validated measurement tool, but the tool is available or described *; | NA | Self-report * | 3 |
| Li Ren and Haixuan Xu.2016 | Truly representative of the average in the target population * | Not justified | No description | Non validated measurement tool, but the tool is available or described *; | NA | Self-report * | 3 |
| Guanghao Jing and Shunfu Piao. 2011 | Truly representative of the average in the target population * | Not justified | Comparability between respondents’ and nonrespondents’ characteristics is established, and the response rate is satisfactory * | Non validated measurement tool, but the tool is available or described *; | NA | Self-report * | 4 |
| Lizhen, Deng and Suili, Rao 2006 | Truly representative of the average in the target population * | Not justified | Comparability between respondents’ and nonrespondents’ characteristics is established, and the response rate is satisfactory * | Non validated measurement tool, but the tool is available or described *; | NA | Self-report * | 4 |
| Author and Year | Assessment Instrument | Response Rate (%) | Findings on Levels of Outpatient Satisfaction |
|---|---|---|---|
| Wenya, Yu et al., 2016 | Adapted questionnaire from the IPSQ ‡ (A 5-point Likert scale questionnaire) | 92.48 | The mean overall outpatient satisfaction was 4.0 ± 0.7. Satisfaction with service attitude was the highest, while satisfaction with medical needs being met by doctors was the lowest. |
| Liyang, Tang. 2011 | A self-designed 5-point Likert scale questionnaire | 100 | The mean overall outpatient satisfaction was 3.7 ± 0.76 Satisfaction with doctor-patient interaction was the highest, while satisfaction with waiting time in hospital was the lowest. |
| Jing Sun et al., Laiyang, Wu et al., 2016 | A self-designed 5-point Likert scale questionnaire. | NR | The overall satisfaction score is 4.42 ± 0.68 Satisfaction with diagnosis and treatment was the highest, while satisfaction with long waiting time in hospital was the lowest |
| Jay Pan et al., 2015 | A self-designed 5-point Likert scale questionnaire | 100% | Satisfaction with medical charges was the lowest. |
| Jinghua, Li et al., 2016 | A self-designed questionnaire (mixed up with 3-point and 5-point Likert scale) | NR | The satisfaction of outpatients from county and tertiary hospitals were significantly lower than those visited village/township clinics. |
| Jinzhu, Xie et al., 2017 | A self-designed 5-point Likert scale questionnaire. | 97.2 | Satisfaction with information got was the highest, while satisfaction with medical cost was the lowest |
| Chunlei, Han et al., 2012 | A self-designed questionnaire based on IPSQ | 99.4 | Satisfaction with hospital management is high, while satisfaction with waiting time is low. |
| Qing Lu et al., 2016 | A self-designed five-point Likert scale questionnaire | 90.9 | 82. 70% (263 /318) of the study participants stated general satisfaction with the outpatient. |
| Jing Zhao et al., 2016 | A self-designed five-point Likert scale questionnaire | 98.5 | Satisfaction with professional skills of doctors was highest, with outpatient management is lowest. |
| Wenlong, Hu et al., 2007 | NR | 96 | The overall satisfaction to the outpatient medical service is 76.9%. The top 3 factors outpatients mostly satisfied with are doctors’ professionalism, hospital hygiene and clear diagnosis. The top 3 factors outpatients mostly dissatisfied with are high medical costing, long waiting time and complicated formalities. |
| Yanxia, Yang et al., 2015 | A self-designed questionnaire | 99.42 | Waiting time, personal health conditions, and knowledge about the diseases are important factors related to outpatient satisfaction. |
| Rong Xu and Xinzhen, Jing. 2004 | A self-designed five-point Likert scale questionnaire | 98.7 | Satisfaction with hospital hygiene was highest, and satisfaction with waiting time of medical examinations was lowest. |
| Junjie, Sun and Shuangqing, Li. 2018 | A self-designed five-point Likert scale questionnaire | 92.5 | The satisfaction of the outpatients is 87.6% (162/185) |
| Zhanwei, Zhou et al., 2011 | A self-designed questionnaire | 97.4 | The outpatients generally showed a high degree of satisfaction with doctors and a low satisfaction with the service staff (Hospital billing collector) |
| Caoxin, Bao et al., 2015 | A self-designed five-point Likert scale questionnaire | NR | The outpatients’ satisfaction score is 82.48. Satisfaction with the overall evaluation of the work and the medical staff was highest; atisfaction with the treatment effect, cost, and the administrative staff was lowest |
| Zhixiang, Teng et al., 2009 | A self-designed seven-point Likert scale questionnaire | 68.7 | The outpatient satisfaction score is 4.23 ± 1.14. |
| Jing Luan et al., 2013 | A self-designed five-point Likert scale questionnaire | 92.8 | NR * |
| Jianjie Zhang. 2018 | A self-designed seven-point Likert scale questionnaire | 90.1 | NR |
| Chunhui, Ren. 2014 | A self-designed questionnaire | 98 | The outpatients were mostly satisfied with the service facilities, followed by medical equipment, and hygiene et al., and mostly dissatisfied with service attitude and medical costs. |
| Weiming, Shao et al., 2017 | A self-designed five-point Likert scale questionnaire | 100 | The outpatients were mostly satisfied with clean hospital hygiene, and mostly dissatisfied with long waiting time. |
| Ying Zou et al., 2014 | A self-designed questionnaire | 99 | The outpatients were mostly satisfied with the hospital hygiene, and mostly dissatisfied with the arrangement of the outpatient department, long waiting time, and shortage of expert outpatients. |
| Mengzhu, Deng et al., 2013 | A self-designed questionnaire | 96.15 | The outpatients were mostly satisfied with the service attitude and environmental facility, and mostly dissatisfied with the waiting time and medical expenses. |
| Huilan, Luo et al., 2010 | A self-designed three- point Likert scale questionnaire based on IPSQ | 99 | The outpatients were mostly dissatisfied with long waiting time, hospital hygiene and outpatient procedures guidance. |
| Zulipiye.et al., 2016 | A self-designed five- point Likert scale questionnaire | 100 | Outpatients were mostly satisfied with hospital hygiene and medical service, and were mostly dissatisfied with long waiting time and complicated formalities during outpatients. |
| Jinping, Shu and Dian Zhou. 2016 | A self-designed five-point Likert scale questionnaire | 94 | Outpatients were mostly dissatisfied with the outpatient process, including the registration and taking drugs et al., |
| Kai ling et al., 2009 | A self-designed four-point Likert scale questionnaire | 100 | Senior outpatients were mostly dissatisfied with the long waiting time. |
| Yu Li et al., 2011 | A self-designed five-point Likert scale questionnaire | 99.5 | The outpatients were mostly satisfied with the doctor service attitude and environmental, and were mostly dissatisfied with the treatment time and health care costs. |
| Qinghua, Zhang and Zhanhe, Liu. 2011 | A self-designed three-point Likert scale questionnaire | 91 | The outpatients were mostly dissatisfied with charge offices and pharmacy. |
| Fanzhi, Meng et al., 2016 | NR | 100 | 94.6% residents showed satisfaction with the outpatient. The residents were mostly dissatisfied with low accessibility to various of drugs. |
| Jun Song et al., 2007 | A self-designed four-point Likert scale questionnaire | 93 | The patients were mostly satisfied with the examination time and guidance during outpatient. |
| Shi Guo et al., 2014 | A self-designed five-point Likert scale questionnaire | 97.5 | Patients were mostly satisfied with the medical diagnosis and treatment, and were mostly dissatisfied with waiting time before seeing the doctors and medical costs. |
| Xunming, Ji et al., 2010 | A self-designed five-point Likert scale questionnaire | 98.82 | 86% outpatients were satisfied with the medical care at outpatients’ departments, and were mostly dissatisfied with professional skills, service attitude and time consuming. |
| Li Ren and Haixuan, Xu. 2016 | A self-designed five-point Likert scale questionnaire | 97.6 | The outpatients were mostly satisfied with examination time of the doctors, and mostly dissatisfied with waiting time for the examination and reports. |
| Guanghao, Jing and Shunfu, Piao. 2011 | A self-designed three-point Likert scale questionnaire | 99.5 | 90.3% outpatients were satisfied with the outpatient. The outpatients were mostly dissatisfied with complicated outpatient process, cold service attitude, unclear explanation, and long waiting time. |
| Lizhen, Deng and Suili, Rao. 2006 | A self-designed questionnaire based on the outpatient questionnaire designed by the ministry of health Guangzhou city | 85 | Outpatients were mostly satisfied with no corruption and good service attitude of the doctors and nurses. Outpatients were mostly dissatisfied with the service attitude of registration and payment offices. |
| Studies | Satisfaction with Hospital Staff | Satisfaction with Hospital Indoor Hygiene and Facilities (The Arrangement, Clear Instruction, Signs, Hygiene, and Enough Seats) | Satisfaction with Outpatient Process and Management | Satisfaction with Medical Costs | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Author and Year | Service Attitude or Communication with the Doctors | Service Attitude or Communication with the Nurses | Professional Skills | Service of the Guidance Medical Staff/Pre-Diagnosis Counters | Service Attitude of the Registration/Payment Offices | Easy Access to Hospital and Registration | Waiting Time | Diagnosis and Treatment Process | Ease of Complain (a Clear and Reliable Channel for Praise and Complain) | Medical Needs Being Met | ||
| Wenya, Yu et al., 2016 | * | * | * | * | * | * | * | * | ||||
| Jing Sun et al., 2015 Laiyang wu, et al., 2016 | * | * | * | * | * | * | * | * | ||||
| Weiming Shao et al., 2017 | * | * | * | * | * | * | * | * | ||||
| Ying Zou et al., 2014 | * | * | * | * | * | * | ||||||
| Mengzhu Deng et al., 2013 | * | * | * | * | * | |||||||
| Qing Lu et al., 2016 | * | * | * | * | * | * | * | |||||
| Jing Zhao et al., 2015 | * | * | * | * | * | |||||||
| Huilan Luo et al., 2010 | * | * | * | |||||||||
| Zulipiye Tuerxun et al., 2016 | * | * | * | * | * | * | * | * | ||||
| Jinping Shu and Dian Zhou, 2016 | * | * | * | * | * | * | * | * | * | |||
| Kai Ling et al., 2009 | * | * | * | |||||||||
| Yu Li, et al., 2011 | * | * | * | * | * | * | * | * | * | |||
| Rong Xu and Xinzhen Jing. 2004 | * | * | * | * | * | * | * | * | ||||
| Qinghua Zhang and Zhanhe Liu. 2011 | * | * | * | * | * | * | * | |||||
| Zhifan Meng, et al., 2016 | * | * | * | * | * | |||||||
| Jun Song et al., 2007 | * | * | * | * | * | * | ||||||
| Shi Guo, et al., 2014 | * | * | * | * | * | * | ||||||
| Xunming Ji, et al., 2010 | * | * | * | |||||||||
| Li Ren and Haixuan Xu. 2016 | * | * | * | * | * | * | ||||||
| Guanghao Jing and Shunfu Piao. 2011 | * | * | * | * | * | * | ||||||
| Lizhen, Deng and Suili, Rao 2006 | * | * | * | * | * | * | * | * | ||||
| Chunhui, Ren. 2014 | * | * | * | * | * | |||||||
| Author and Year | Main Findings on the Relationship between Outpatient Satisfaction and Influencing Factors | ||
|---|---|---|---|
| Patient Social-Demographic Factors | Medial Staff Factors | hygiene and Process Management | |
| Wenya, Yu et al., 2016 | (1) Outpatients’ socio-demographic characteristics (including sex, age, occupation, monthly income, residence, and marital status) were related to satisfaction to varying degrees. (2) Outpatients who were male, older, married, with low or middle incomes (2000–4999 Yuan), living in Shanghai, or students were more satisfied than those without these characteristics. (3) Young and middle-aged adults (20–39 years), and divorced or widowed patients had lower odds of high satisfaction with doctors. | Satisfactions with doctors and with nurses were significantly related to the overall satisfaction. | Satisfaction with hygiene had the weakest contribution to overall satisfaction. |
| Liyang, Tang. 2011 | Patients’ trust in medical service had the largest influence on patient’s satisfaction. | NR * | NR |
| Jing Sun et al., 2017 Laiyang, Wu et al., 2016 | (1) Outpatient with commercial insurance coverage is associated with satisfaction that is 1.73 times that of the uninsured (p = 0.03) (2) Satisfaction scores of the Chinese elderly outpatients were significantly higher than that of the young and middle-aged outpatients in the domains of hospital hygiene, process efficiency, and overall satisfaction (p < 0.001). On the contrary, the elderly outpatients were less satisfied in the domain of hospital informationization experience than the young and middle-aged outpatients. | (1) “Patient–doctor relationship” is the strongest predictor of overall patient satisfaction (OR = 3.19, 95% CI: 2.83–3.59); (2) Trustful doctor–patient relationship (OR = 3.45), respected and comfortable care (OR = 1.45), clear and reliable mechanism, length of communication time with doctors (OR = 1.35). and waiting time (OR = 1.29) were major factors associated with the overall satisfaction of the elderly outpatients | (1) Channel for praise and complain (OR = 1.39) was the major factors associated with the overall satisfaction of the elderly outpatient. (2) Hospital hygiene, process management, and healthcare experience significantly correlated with outpatient satisfaction; |
| Jay Pan et al., 2015 | (1) Female are less dissatisfied; (2) Higher income is associated with lower satisfaction level in outpatient satisfaction level; | NR | NR |
| Jinghua, Li et al., 2016 | (1) Men and singles were less likely to be satisfied with waiting time. (2) Individuals aged 15–44 years were less likely to be satisfied compared with those aged ≥65 years. (3) Higher education was associated with lower odds of satisfaction. (4) Employed individuals were much more likely to be satisfied. (5) People living in urban areas were less likely to report satisfaction than people living in rural areas (6) Insured patients were much more likely to be satisfied compared with uninsured patients | NR. | (1) Patients seeking outpatient care from tertiary hospitals were very satisfied with the care environment, whereas those in rural areas were less satisfied (p = 0.008); (2) Among patients seeking outpatient care from tertiary hospitals, the odds of satisfaction with waiting time and medical costs were significantly lower than those using village/township clinics. |
| Jinzhu, Xie et al., 2017 | Age, type of payment, and the self-rated health status were associated with outpatient satisfaction; Outpatients older than 65 years had the highest experience score, whereas outpatients paying out-of-pocket had the lowest experience score. | NR | NR |
| Chunlei, Han et al., 2012 | Patients’ demographic characteristics including occupation, monthly salary, and education level were associated with outpatient satisfaction. | NR | NR |
| Qing Lu et al., 2016 | Marital status, occupation, health insurance type, payment-method, and family income were correlated with outpatient satisfaction. | NR | NR |
| Jing Zhao et al., 2016 | NR | NR | Outpatient process was an independent factor influencing outpatient satisfaction. |
| Wenlong, Hu et al., 2007 | Age, gender and monthly income are not significantly associated with outpatient satisfaction, while level of education was significantly associated with outpatient satisfaction. | NR | NR |
| Yanxia, Yang et al., 2015 | There were no significant differences in patients’ sex, age, marriage, occupation and education on outpatient satisfaction. | NR | outpatient satisfaction was associated with waiting time. |
| Rong Xu and Xinzhen, Jing. 2004 | NR | The outpatient satisfaction was mostly associated with the satisfaction with the diagnosis and treatment of the doctor, and the service attitude of the doctors. | The outpatient satisfaction was mostly associated with the satisfaction with the medical cost and the arrangements during the wait. |
| Junjie, Sun and Shuangqing, Li. 2018 | NR | Communication with doctors, the degree of carefulness the doctors inquired, and the degree of the clarity the doctors explained the diseases are associated with outpatient satisfaction. | NR |
| Zhanwei, Zhou et al., 2011 | NR | Patients showed significant lower satisfaction with payment officers compared with doctors and nurses. The feeling of being respect during outpatient, professional skills of doctors and the service of the pre-diagnosis counters were associated with outpatient satisfaction. | Hospital hygiene and medical costs are associated with outpatient satisfaction. |
| Caoxin, Bao et al., 2015 | NR | The service attitude and professional skills of doctors are associated with outpatient satisfaction | Hospital reputation, the protection of privacy during diagnosis and waiting time are associated with outpatient satisfaction. |
| Zhixiang, Teng et al., 2009 | NR | NR | The levels of the hospitals are not associated with outpatient satisfaction in the first-time visit. |
| Jing Luan et al., 2013 | The age, gender, marital status, education level, monthly income and self-health evaluation are associated with outpatient satisfaction. | NR | NR |
| Jianjie Zhang. 2018 | Health-related knowledge is positively associated with outpatient satisfaction. | The professional skills were of significantly positive correlated with outpatient satisfaction. | Waiting time is not associated with outpatient satisfaction. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, Y.; Gong, W.; Kong, X.; Mueller, O.; Lu, G. Factors Associated with Outpatient Satisfaction in Tertiary Hospitals in China: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 7070. https://doi.org/10.3390/ijerph17197070
Li Y, Gong W, Kong X, Mueller O, Lu G. Factors Associated with Outpatient Satisfaction in Tertiary Hospitals in China: A Systematic Review. International Journal of Environmental Research and Public Health. 2020; 17(19):7070. https://doi.org/10.3390/ijerph17197070
Chicago/Turabian StyleLi, Yuping, Weijuan Gong, Xiang Kong, Olaf Mueller, and Guangyu Lu. 2020. "Factors Associated with Outpatient Satisfaction in Tertiary Hospitals in China: A Systematic Review" International Journal of Environmental Research and Public Health 17, no. 19: 7070. https://doi.org/10.3390/ijerph17197070
APA StyleLi, Y., Gong, W., Kong, X., Mueller, O., & Lu, G. (2020). Factors Associated with Outpatient Satisfaction in Tertiary Hospitals in China: A Systematic Review. International Journal of Environmental Research and Public Health, 17(19), 7070. https://doi.org/10.3390/ijerph17197070