Is Fear of Harm (FoH) in Sports-Related Activities a Latent Trait? The Item Response Model Applied to the Photographic Series of Sports Activities for Anterior Cruciate Ligament Rupture (PHOSA-ACLR)

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measurements
2.3. Analysis
3. Results
3.1. This Description of the Samples
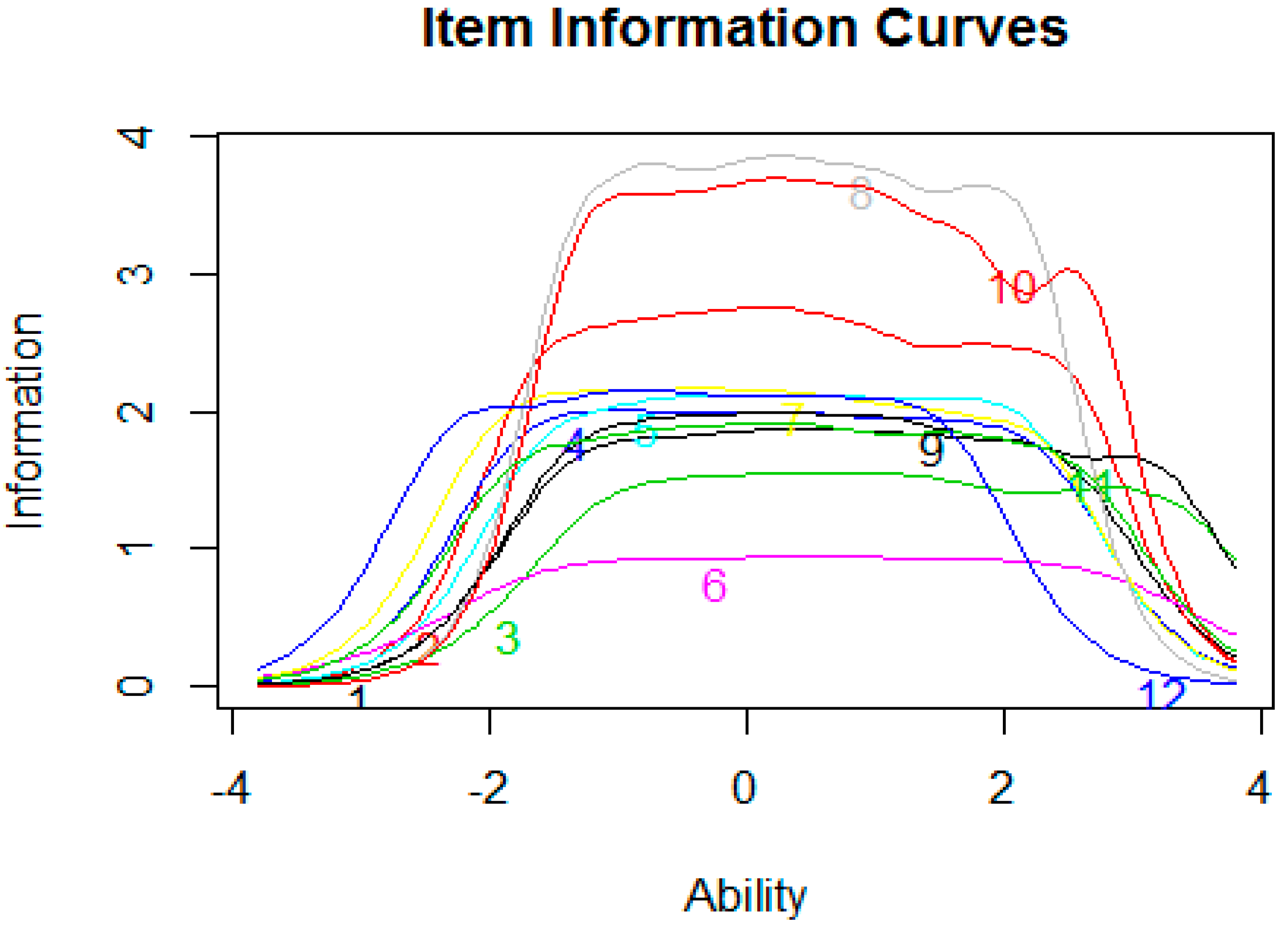
3.2. Assessment of Graded Response Model
3.3. Difference between Groups in FoH Assessed with the PHOSA-ACLR
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Availability of Data and Materials
Ethics Approval and Consent to Participate
Abbreviations
| ACL | Anterior Cruciate Ligament |
| ACLR | Anterior Cruciate Ligament Reconstruction |
| ADL | Activities of Daily Life |
| ANCOVA | Univariate Analysis of Covariance |
| FoH | Fear of Harm |
| GRM | Graded Response Model |
| IRT | Item Response Theory |
| PHODA | Photographic Series of Daily Activities |
| PHOSA-ACLR | Photographic Series of Sport Activities related to ACLR |
| KOOS | Knee injury and Osteoarthritis Outcome Scale |
| SD | Standard Deviation |
| TSK | Tampa Scale of Kinesiophobia |
| QOL | Quality of Life |
References
- Sanders, T.L.; Kremers, H.M.; Bryan, A.J.; Larson, D.R.; Dahm, D.L.; Levy, B.A.; Stuart, M.J.; Krych, A.J. Incidence of anterior cruciate ligament tears and reconstruction: A 21-year population-based study. Am. J. Sports Med. 2016, 44, 1502–1507. [Google Scholar] [CrossRef] [PubMed]
- van Melick, N.; van Cingel, R.E.; Brooijmans, F.; Neeter, C.; van Tienen, T.; Hullegie, W.; Nijhuis-van der Sanden, M.W. Evidence-based clinical practice update: Practice guidelines for anterior cruciate ligament rehabilitation based on a systematic review and multidisciplinary consensus. Br. J. Sports Med. 2016, 50, 1506–1515. [Google Scholar] [CrossRef] [PubMed]
- Kvist, J.; Ek, A.; Sporrstedt, K.; Good, L. Fear of re-injury: A hindrance for returning to sports after anterior cruciate ligament reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2005, 13, 393–397. [Google Scholar] [CrossRef]
- Flanigan, D.C.; Everhart, J.S.; Pedroza, A.; Smith, T.; Kaeding, C.C. Fear of reinjury (kinesiophobia) and persistent knee symptoms are common factors for lack of return to sport after anterior cruciate ligament reconstruction. Arthrosc. J. Arthrosc. Relat. Surg. 2013, 29, 1322–1329. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.J.; Meierbachtol, A.; George, S.Z.; Chmielewski, T.L. Fear of reinjury in athletes: Implications for rehabilitation. Sports Health 2017, 9, 162–167. [Google Scholar] [CrossRef] [PubMed]
- Czuppon, S.; Racette, B.A.; Klein, S.E.; Harris-Hayes, M. Variables associated with return to sport following anterior cruciate ligament reconstruction: A systematic review. Br. J. Sports Med. 2014, 48, 356–364. [Google Scholar] [CrossRef]
- Heil, J. The Injured Athlete. Emot. Sport 2000, 2000, 245–265. [Google Scholar] [CrossRef]
- Trigsted, S.M.; Cook, D.B.; Pickett, K.A.; Cadmus-Bertram, L.; Dunn, W.R.; Bell, D.R. Greater fear of reinjury is related to stiffened jump-landing biomechanics and muscle activation in women after ACL reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2018, 26, 3682–3689. [Google Scholar] [CrossRef]
- Vlaeyen, J.W.S.; Linton, S.J. Fear-avoidance model of chronic musculoskeletal pain: 12 years on. Pain 2012, 153, 1144–1147. [Google Scholar] [CrossRef]
- Ardern, C.L.; Taylor, N.F.; Feller, J.A.; Webster, K.E. A systematic review of the psychological factors associated with returning to sport following injury. Br. J. Sports Med. 2013, 47, 1120–1126. [Google Scholar] [CrossRef]
- Everhart, J.S.; Best, T.M.; Flanigan, D.C. Psychological predictors of anterior cruciate ligament reconstruction outcomes: A systematic review. Knee Surg. Sports Traumatol. Arthrosc. 2015, 23, 752–762. [Google Scholar] [CrossRef] [PubMed]
- Lundberg, M.; Larsson, M.; Ostlund, H.; Styf, J. Kinesiophobia among patients with musculoskeletal pain in primary healthcare. J. Rehabil. Med. 2006, 38, 37–43. [Google Scholar] [CrossRef]
- Gatchel, R.J.; Neblett, R.; Kishino, N.; Ray, C.T. Fear-avoidance beliefs and chronic pain. J. Orthop. Sports Phys. Ther. 2016, 46, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Ardern, C.L.; Kvist, J. What is the evidence to support a psychological component to rehabilitation programs after anterior cruciate ligament reconstruction? Curr. Orthop. Pract. 2016, 27, 263–268. [Google Scholar] [CrossRef]
- Christino, M.A.; Fantry, A.J.; Vopat, B.G. Psychological Aspects of Recovery Following Anterior Cruciate Ligament Reconstruction. J. Am. Acad. Orthop. Surg. 2015, 23, 501–509. [Google Scholar] [CrossRef]
- Vlaeyen, J.W.; Morley, S.; Linton, S.J.; Boersma, K.; de Jong, J. Pain-Related Fear: Exposure Based Treatment for Chronic Pain; IASP Press: Seattle, WA, USA, 2012. [Google Scholar]
- McArdle, S. Psychological Rehabilitation from Anterior Cruciate Ligament–Medial Collateral Ligament Reconstructive Surgery: A Case Study. Sports Health 2009, 2, 73–77. [Google Scholar] [CrossRef]
- Miller, R.; Kori, S.; Todd, D. The tampa scale for kinisophobia. Unpublished work. 1991. [Google Scholar]
- Webster, K.E.; Feller, J.A.; Lambros, C. Development and preliminary validation of a scale to measure the psychological impact of returning to sport following anterior cruciate ligament reconstruction surgery. Phys. Ther. Sport 2008, 9, 9–15. [Google Scholar] [CrossRef]
- van Lankveld, W.; van Melick, N.; Habets, B.; Roelofsen, E.G.; Staal, J.B.; van Cingel, R. Measuring individual hierarchy of anxiety invoking sports related activities: Development and validation of the Photographic Series of Sports Activities for Anterior Cruciate Ligament Reconstruction (PHOSA-ACLR). BMC Musculoskelet. Disord. 2017, 18, 287. [Google Scholar] [CrossRef]
- Tesio, L. Outcome measurement in behavioural sciences: A view on how to shift attention from means to individuals and why. Int. J. Rehabil. Res. 2012, 35, 1–12. [Google Scholar] [CrossRef]
- Roos, E.M.; Roos, H.P.; Lohmander, L.S.; Ekdahl, C.; Beynnon, B.D. Knee Injury and Osteoarthritis Outcome Score (KOOS)—Development of a Self-Administered Outcome Measure. J. Orthop. Sports Phys. Ther. 1998, 28, 88–96. [Google Scholar] [CrossRef]
- Vlaeyen, J.W.; Kole-Snijders, A.M.; Boeren, R.G.; Van Eek, H. Fear of movement/(re)injury in chronic low back pain and its relation to behavioral performance. Pain 1995, 62, 363–372. [Google Scholar] [CrossRef]
- Lord, F.M. Applications of Item Response Theory to Practical Testing Problems; Routledge: London, UK, 1980. [Google Scholar]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155. [Google Scholar] [CrossRef] [PubMed]
- Darlow, B. Beliefs about back pain: The confluence of client, clinician and community. Int. J. Osteopat. Med. 2016, 20, 53–61. [Google Scholar] [CrossRef]
- Buer, N.; Linton, S.J. Fear-avoidance beliefs and catastrophizing: Occurrence and risk factor in back pain and ADL in the general population. Pain 2002, 99, 485–491. [Google Scholar] [CrossRef]
- Houben, R.M.; Ostelo, R.W.; Vlaeyen, J.W.; Wolters, P.M.; Peters, M.; Stomp-van Den Berg, S.G. Health care providers’ orientations towards common low back pain predict perceived harmfulness of physical activities and recommendations regarding return to normal activity. Eur. J. Pain 2005, 9, 173–183. [Google Scholar] [CrossRef]
- Caneiro, J.P.; O’Sullivan, P.; Lipp, O.V.; Mitchinson, L.; Oeveraas, N.; Bhalvani, P.; Abrugiato, R.; Thorkildsen, S.; Smith, A. Evaluation of implicit associations between back posture and safety of bending and lifting in people without pain. Scand. J. Pain 2018, 18, 719–728. [Google Scholar] [CrossRef]
- Goubert, L.; Crombez, G.; Hermans, D.; Vanderstraeten, G. Implicit attitude towards pictures of back-stressing activities in pain-free subjects and patients with low back pain: An affective priming study. Eur. J. Pain 2003, 7, 33–42. [Google Scholar] [CrossRef]
- Gardner, T.; Refshauge, K.; Smith, L.; McAuley, J.; Hübscher, M.; Goodall, S. Physiotherapists’ beliefs and attitudes influence clinical practice in chronic low back pain: A systematic review of quantitative and qualitative studies. J. Physiother. 2017, 63, 132–143. [Google Scholar] [CrossRef]
- Coudeyre, E.; Rannou, F.; Tubach, F.; Baron, G.; Coriat, F.; Brin, S.; Revel, M.; Poiraudeau, S. General practitioners’ fear-avoidance beliefs influence their management of patients with low back pain. Pain 2006, 124, 330–337. [Google Scholar] [CrossRef]
- Lakke, S.E.; Soer, R.; Krijnen, W.P.; van der Schans, C.P.; Reneman, M.F.; Geertzen, J.H. Influence of Physical Therapists’ Kinesiophobic Beliefs on Lifting Capacity in Healthy Adults. Phys. Ther. 2015, 95, 1224–1233. [Google Scholar] [CrossRef]
- Vlaeyen, J.W. The intricate relationship amongst pain intensity, fear and avoidance. Scand. J. Pain 2016, 13, 128–129. [Google Scholar] [CrossRef] [PubMed]
- Ardern, C.L.; Taylor, N.F.; Feller, J.A.; Webster, K.E. Fear of re-injury in people who have returned to sport following anterior cruciate ligament reconstruction surgery. J. Sci. Med. Sport 2012, 15, 488–495. [Google Scholar] [CrossRef]
- Rodriguez, R.M.; Marroquin, A.; Cosby, N. Reducing fear of reinjury and pain perception in athletes with first-time anterior cruciate ligament reconstructions by implementing imagery training. J. Sport Rehabil. 2019, 28, 385–389. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Theoretical Range | Mean (Standard Deviation) | Observed Range |
|---|---|---|---|
| KOOS Pain | 0–100 | 81.8 (17.7) | 33–100 |
| KOOS Symptoms | 0–100 | 63.2 (12.8) | 29–100 |
| KOOS Activities of Daily Life | 0–100 | 89.1 (14.2) | 35–100 |
| KOOS Sports and Leisure | 0–100 | 59.1 (30.6) | 00–100 |
| KOOS Quality of Life | 0–100 | 48.3 (14.1) | 06–75 |
| Tampa Scale of Kinesiophobia | 0–68 | 35.7 (7.1) | 20–51 |
| Variable | Regular Students n = 169 | Vitesse n = 30 |
|---|---|---|
| Average age (mean, SD) | 19.2 (2.0) | 18.3 (3.2) |
| Average hours active sporting (mean, SD) | 5.6 (2.8) | 14.9 (4.2) |
| Gender (% male) | 48% | 94% |
| Earlier complaints (% yes) | 71% | 60% |
| Knowledge of ACLR (% yes) | 35% | 65% |
| Chronic condition (% yes) | 10% | 7% |
| High risk sports (% yes) | 66% | 100% |
| Sports Related Activity | Observed Range | Mean Score (SD) | Median |
|---|---|---|---|
| 1. Running | 0–10 | 3.67 (2.73) | 3.0 |
| 2. Landing after jumping | 0–10 | 4.39 (2.90) | 4.0 |
| 3. Squats | 0–10 | 3.11 (2.63) | 3.0 |
| 4. Lateral lunging | 0–10 | 4.76 (2.83) | 5.0 |
| 5. Single leg jump | 0–10 | 3.88 (2.71) | 4.0 |
| 6. Sliding | 0–10 | 3.98 (2.79) | 4.0 |
| 7. Bring to a halt | 0–10 | 5.11 (2.85) | 6.0 |
| 8. Hopscotch | 0–10 | 4.11 (2.84) | 4.0 |
| 9. Lunge | 0–10 | 3.77 (2.78) | 4.0 |
| 10. Start to sprint | 0–10 | 4.09 (2.84) | 4.0 |
| 11. Jumping on a trampoline | 0–10 | 4.06 (2.77) | 4.0 |
| 12. Pivoting movement | 0–10 | 5.68 (2.86) | 6.0 |
| PHOSA Item | β.1 | β.2 | β.3 | β.4 | β.5 | β.6 | β.7 | β.8 | β.9 | β.10 | β |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 6. Sliding | −2.73 | −2.03 | −1.10 | −0.20 | 0.43 | 1.15 | 1.80 | 2.64 | 3.50 | 4.73 | 1.69 |
| 3. Squats | −2.42 | −1.15 | −0.19 | 0.80 | 1.59 | 2.30 | 2.70 | 3.75 | 5.82 | 7.25 | 2.18 |
| 1. Running | −3.30 | −2.04 | −0.63 | 0.30 | 0.86 | 1.79 | 2.73 | 3.85 | 5.39 | 5.96 | 2.40 |
| 11. Jumping | −4.31 | −2.56 | −1.32 | −0.35 | 0.49 | 1.24 | 1.92 | 3.52 | 4.42 | 6.19 | 2.42 |
| 9. Lunge | −3.40 | −2.03 | −0.97 | −0.07 | 0.70 | 1.63 | 2.53 | 3.47 | 5.34 | 7.82 | 2.47 |
| 4. Lateral Lunging | −4.48 | −3.45 | −2.49 | −1.60 | −0.40 | 0.65 | 1.36 | 2.76 | 4.12 | 5.67 | 2.49 |
| 5. Leg jump | −3.95 | −2.33 | −1.33 | −0.28 | 0.61 | 1.72 | 2.58 | 3.89 | 4.73 | 5.76 | 2.56 |
| 12. Pivoting | −5.92 | −5.32 | −3.56 | −2.59 | −1.91 | −1.03 | 0.37 | 1.44 | 2.80 | 4.03 | 2.58 |
| 7. Bring to Halt | −5.08 | −3.84 | −3.01 | −1.79 | −0.98 | −0.08 | 1.00 | 2.14 | 3.85 | 5.84 | 2.59 |
| 2. Landing | −4.73 | −3.12 | −1.74 | −0.69 | 0.31 | 1.02 | 1.67 | 3.14 | 5.23 | 7.28 | 2.92 |
| 10. Start sprint | −4.46 | −3.28 | −1.81 | −0.40 | 0.63 | 1.49 | 2.77 | 3.92 | 5.88 | 8.81 | 3.39 |
| 8. Hop | −4.69 | −3.09 | −2.11 | −0.53 | 0.68 | 1.43 | 2.78 | 4.12 | 6.07 | 7.67 | 3.48 |
| ACLR n = 58 | Regular Students n = 169 | Soccer n = 30 | Total n = 257 | |
|---|---|---|---|---|
| Average PHOSA | 3.1 | 4.9 | 2.6 | 4.2 |
| Range | 0–10 | 0–10 | 0–10 | 0–10 |
| Standard Deviation (SD) | 2.3 | 2.0 | 2.7 | 2.3 |
| 95% CI | 2.5–3.7 | 4.6–5.2 | 1.6–3.6 | 3.9–4.5 |
| Median | 2.5 | 5.5 | 1.6 | 4.8 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lankveld, W.v.; Pat-El, R.J.; Melick, N.v.; Cingel, R.v.; Staal, J.B. Is Fear of Harm (FoH) in Sports-Related Activities a Latent Trait? The Item Response Model Applied to the Photographic Series of Sports Activities for Anterior Cruciate Ligament Rupture (PHOSA-ACLR). Int. J. Environ. Res. Public Health 2020, 17, 6764. https://doi.org/10.3390/ijerph17186764
Lankveld Wv, Pat-El RJ, Melick Nv, Cingel Rv, Staal JB. Is Fear of Harm (FoH) in Sports-Related Activities a Latent Trait? The Item Response Model Applied to the Photographic Series of Sports Activities for Anterior Cruciate Ligament Rupture (PHOSA-ACLR). International Journal of Environmental Research and Public Health. 2020; 17(18):6764. https://doi.org/10.3390/ijerph17186764
Chicago/Turabian StyleLankveld, Wim van, Ron J. Pat-El, Nicky van Melick, Robert van Cingel, and J. Bart Staal. 2020. "Is Fear of Harm (FoH) in Sports-Related Activities a Latent Trait? The Item Response Model Applied to the Photographic Series of Sports Activities for Anterior Cruciate Ligament Rupture (PHOSA-ACLR)" International Journal of Environmental Research and Public Health 17, no. 18: 6764. https://doi.org/10.3390/ijerph17186764
APA StyleLankveld, W. v., Pat-El, R. J., Melick, N. v., Cingel, R. v., & Staal, J. B. (2020). Is Fear of Harm (FoH) in Sports-Related Activities a Latent Trait? The Item Response Model Applied to the Photographic Series of Sports Activities for Anterior Cruciate Ligament Rupture (PHOSA-ACLR). International Journal of Environmental Research and Public Health, 17(18), 6764. https://doi.org/10.3390/ijerph17186764