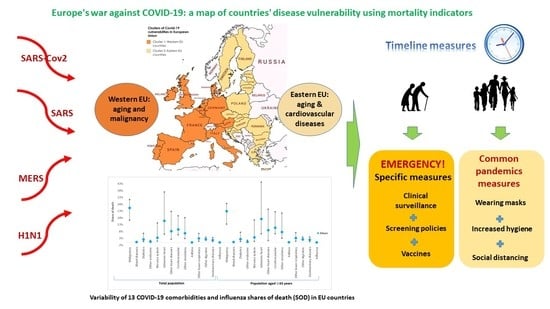
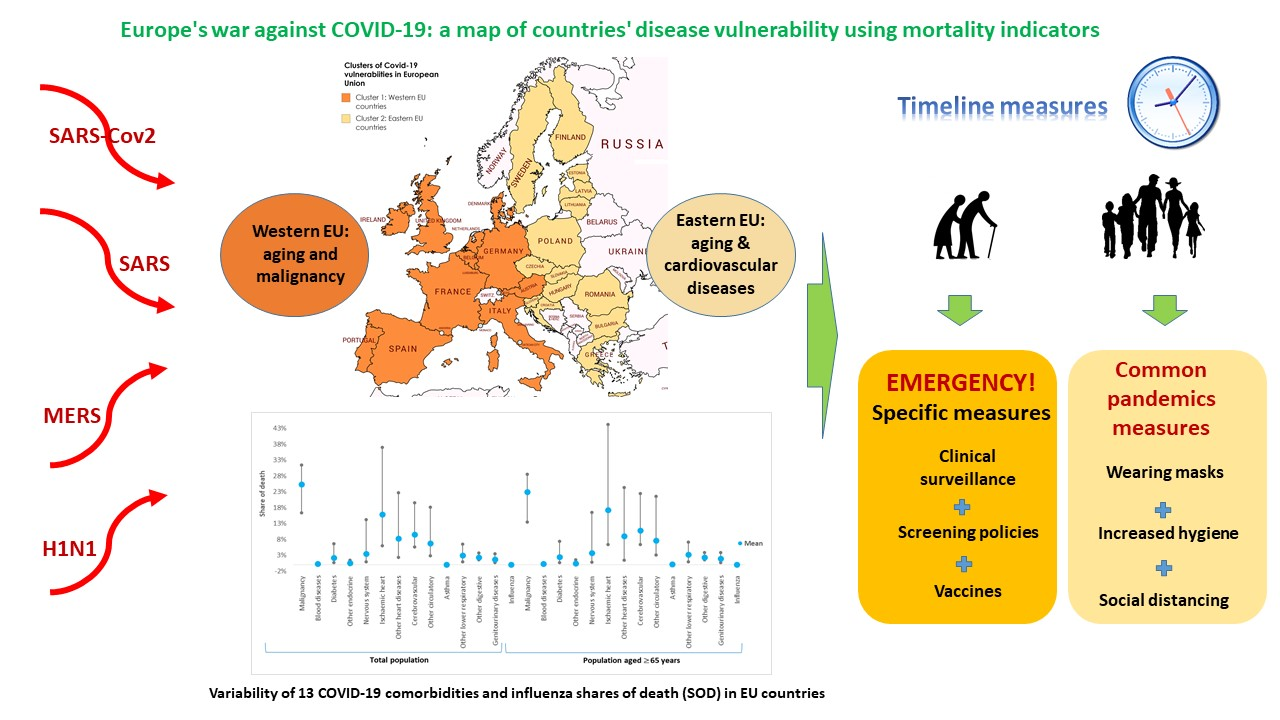
Europe’s War against COVID-19: A Map of Countries’ Disease Vulnerability Using Mortality Indicators




Abstract
1. Introduction
2. Methods
- (1)
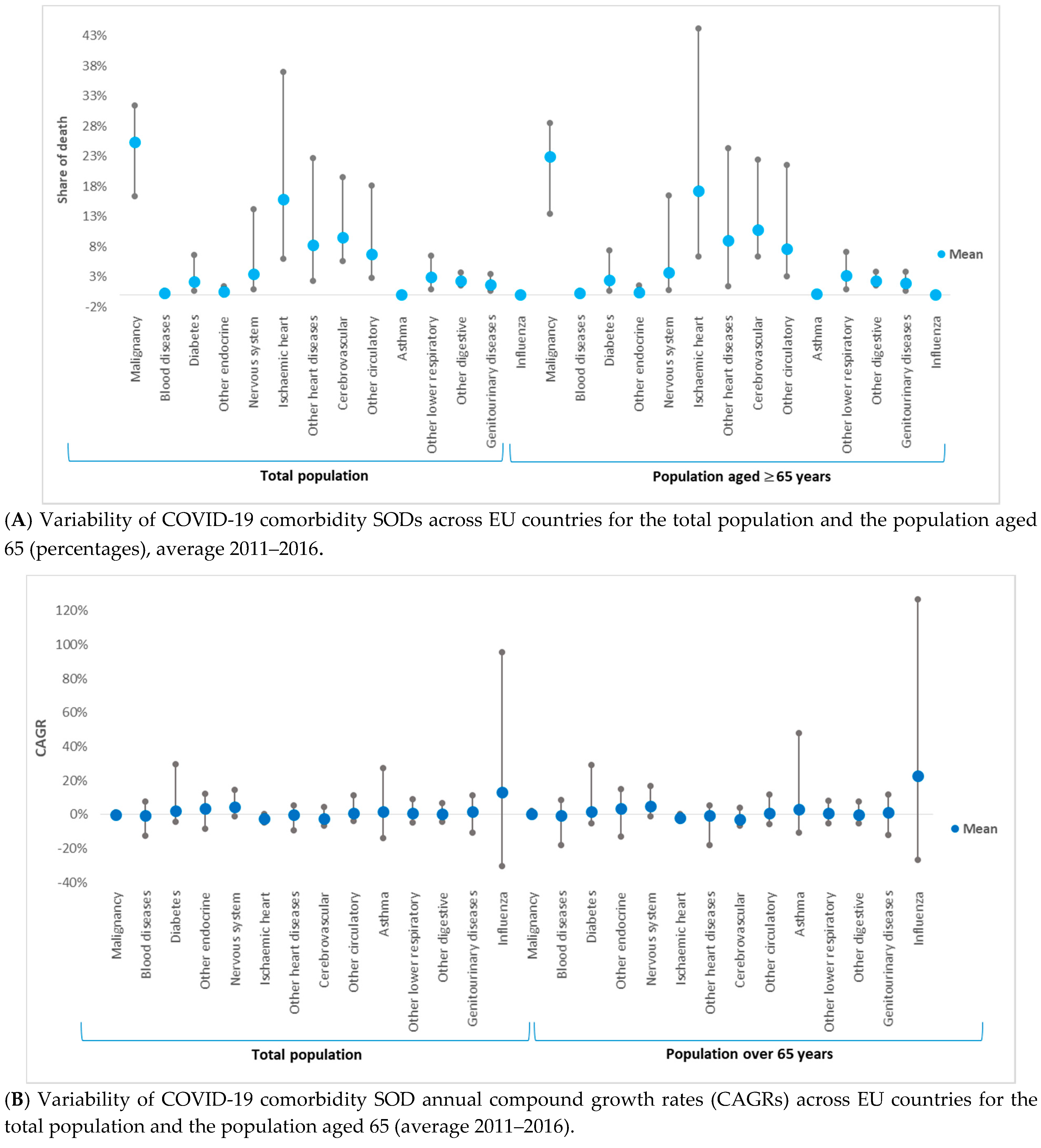
- thirteen COVID-19 comorbidity SODs and their corresponding annual growth rates, for the total population and the population aged 65, and
- (2)
- influenza SODs and their corresponding annual growth rates, for the total population and the population aged 65.
3. Results
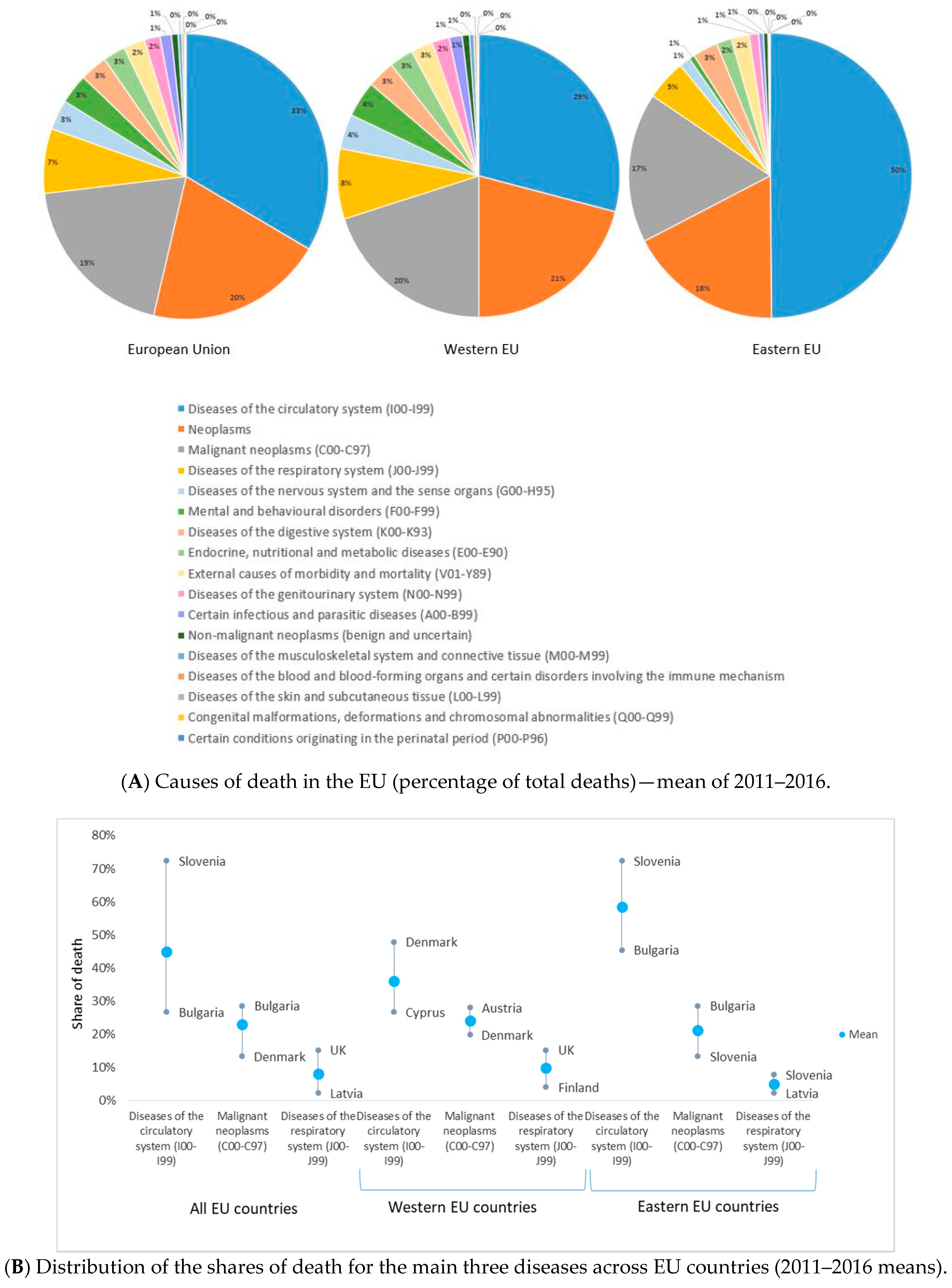
3.1. COVID-19 Comorbidities—Data Description
3.2. Influenza—Data Description
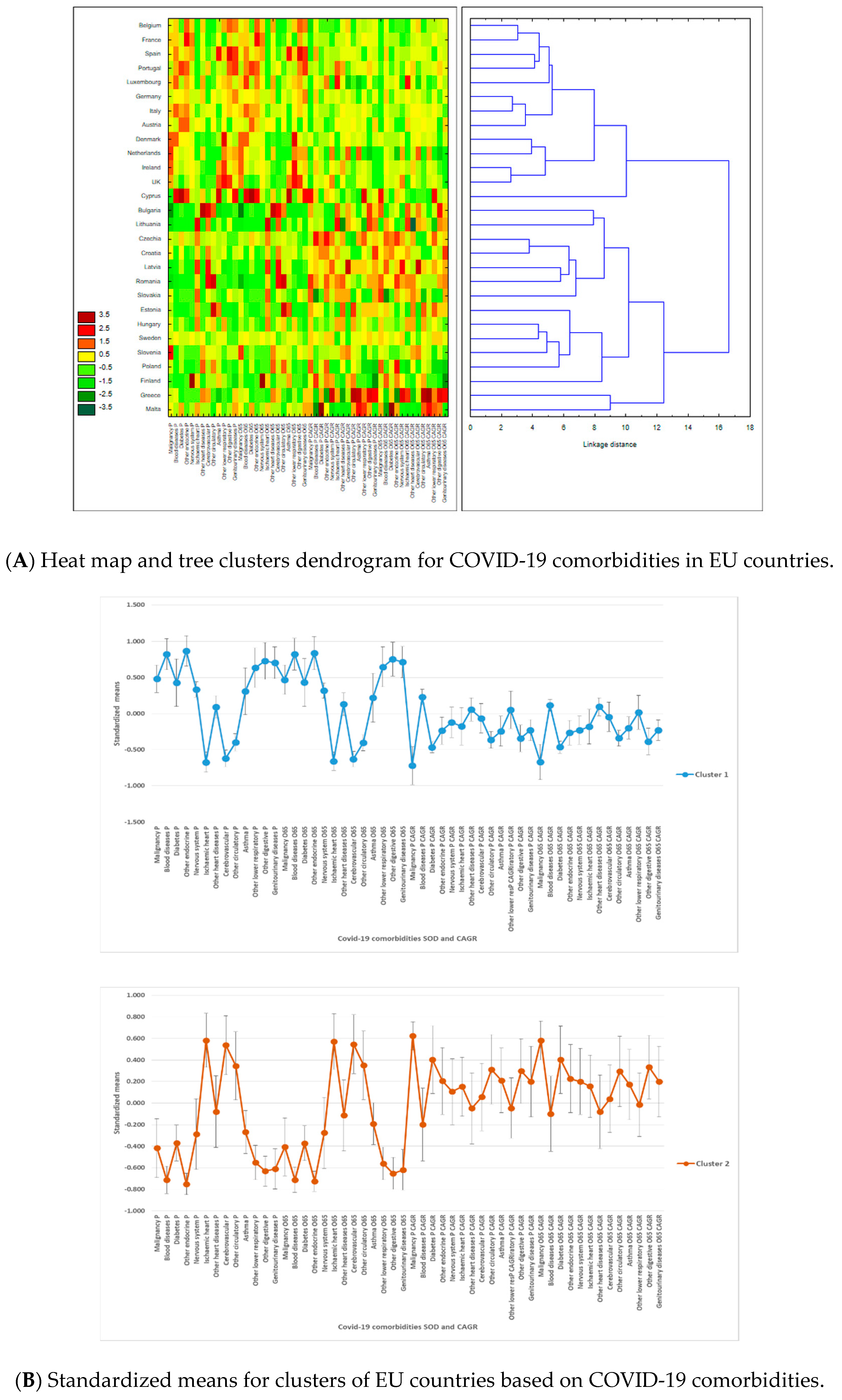
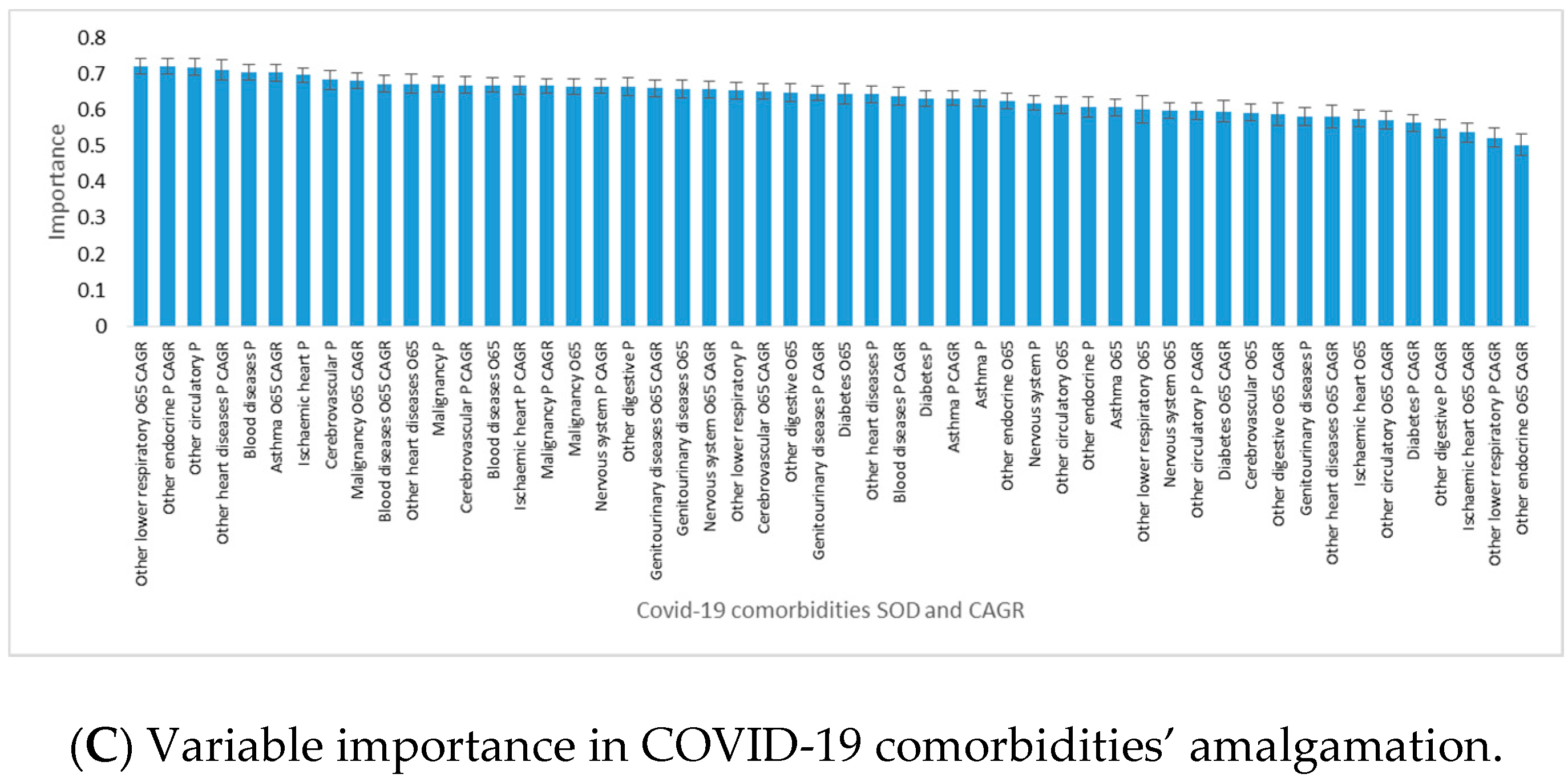
3.3. Results of Tree Clustering Algorithms
3.3.1. Clusters Based on COVID-19 Comorbidity SOD and CAGR
3.3.2. Clusters of Influenza SOD and CAGR
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Availability of Data and Materials
Abbreviations
| SARS-Cov2 | Severe Acute Respiratory Syndrome Coronavirus 2 |
| COVID-19 | coronavirus disease |
| EU | the European Union |
| CDs | communicable diseases |
| NCDs | noncommunicable diseases |
| ICD-10 | the International Statistical Classification of Diseases and Related Health Problems 10th Revision |
| ICU | intensive care unit |
| SOD | share of death |
| CAGR | annual compound growth of rate |
References
- University of Oxford. Oxford Martin School—Our World in Data. Available online: https://ourworldindata.org/covid-cases (accessed on 10 July 2020).
- Sanche, S.; Lin, Y.; Xu, C.; Romero-Severson, E.; Hengartner, N.; Ke, R. High contagiousness and rapid spread of severe acute respiratory syndrome coronavirus 2. Emerg. Infect. Dis. 2020, 26, 1470–1477. [Google Scholar] [CrossRef]
- Wu, J.T.; Leung, K.; Leung, G.M. Nowcasting and forecasting the potential domestic and international spread of the 2019-nCoV outbreak originating in Wuhan, China: A modelling study. Lancet 2020, 395, 689–697. [Google Scholar] [CrossRef]
- Bi, Q.; Wu, Y.; Mei, S.; Ye, C.; Zou, X.; Zhang, Z.; Liu, X.; Wei, L.; Truelove, S.A.; Zhang, T.; et al. Epidemiology and Transmission of COVID-19 in Shenzhen China: Analysis of 391 cases and 1,286 of their close contacts. Lancet Inf. Dis. 2020, 20, 911–919. [Google Scholar] [CrossRef]
- Linton, N.M.; Kobayashi, T.; Yang, Y.; Hayashi, K.; Akhmetzhanov, A.R.; Jung, S.M.; Yuan, B.; Kinoshita, R.; Nishiura, H. Incubation period and other epidemiological characteristics of 2019 novel coronavirus infections with right truncation: A statistical analysis of publicly available case data. J. Clin. Med. 2020, 9, 538. [Google Scholar] [CrossRef] [PubMed]
- Hauser, A.; Counotte, M.J.; Margossian, C.C.; Konstantinoudis, G.; Low, N.; Althaus, C.L.; Riou, J. Estimation of SARS-CoV-2 mortality during the early stages of an epidemic: A modelling study in Hubei, China, and six regions in Europe. PLoS Med. 2020, 17, e1003189. [Google Scholar] [CrossRef] [PubMed]
- The Global Fund. COVID-19. Available online: https://www.theglobalfund.org/en/covid-19/ (accessed on 10 July 2020).
- European Open Science Cloud (EOSC). Fast-Track Co-Creation Funding for COVID-19 Related Activities Launched by EOSCsecretariat.eu. Available online: https://www.eosc-portal.eu/news/funding-covid-19-eoscsecretariat (accessed on 10 July 2020).
- Wilder-Smith, A.; Freedman, D.O. Isolation, quarantine, social distancing and community containment: Pivotal role for old-style public health measures in the novel coronavirus (2019-nCoV) outbreak. J. Travel Med. 2020, 27, taaa020. [Google Scholar] [CrossRef] [PubMed]
- Van Kerkhove, M.D.; Vandemaele, K.A.; Shinde, V.; Jaramillo-Gutierrez, G.; Koukounari, A.; Donnelly, C.A.; Carlino, L.O.; Owen, R.; Paterson, B.; Pelletier, L.; et al. Risk factors for severe outcomes following 2009 influenza A (H1N1) infection: A global pooled analysis. PLoS Med. 2011, 8, e1001053. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Seasonal Influenza Vaccination and Antiviral use in EU/EEA Member States. Available online: https://www.ecdc.europa.eu/en/publications-data/seasonal-influenza-vaccination-antiviral-use-eu-eea-member-states (accessed on 10 July 2020).
- Tomlins, J.; Hamilton, F.; Gunning, S.; Shehy, C.; Moran, E.; MacGowan, A. Clinical features of 95 sequential hospitalized patients with novel coronavirus 2019 disease (COVID-19), the first UK cohort. J. Infect. 2020, 81, e59–e61. [Google Scholar] [CrossRef]
- Lagi, F.; Piccica, M.; Graziani, L.; Vellere, I.; Botta, A.; Tilli, M.; Ottino, L.; Borchi, B.; Pozzi, M.; Bartalesi, F.; et al. Early experience of an infectious and tropical diseases unit during the coronavirus disease (COVID-19) pandemic, Florence, Italy, February to March 2020. Euro Surveill. 2020, 5. [Google Scholar] [CrossRef]
- Liverman, D.M. Vulnerability to global environmental change. In Global Environmental Risk; Kasperson, J.X., Kasperson, R.E., Eds.; United Nations University Press: Tokyo, Japan, 2001; pp. 27–44. [Google Scholar]
- Confalonieri, U.E.C.; Wilson, M.E.; Najar, A.L. Social and environmental vulnerability to emerging infectious diseases. In Interactions between Global Change and Human Health; Pontifical Academy of Sciences, Scripta Varia 106: Vatican City, Italy, 2006; Available online: http://www.pas.va/content/dam/accademia/pdf/sv106/sv106-confalonieri.pdf (accessed on 10 July 2020).
- European Commission. State of Health in the EU 2019. Available online: https://ec.europa.eu/commission/presscorner/detail/en/IP_19_6336 (accessed on 10 July 2020).
- European Commission. Country Health Profiles. Available online: https://ec.europa.eu/health/state/country_profiles_en (accessed on 7 February 2020).
- Narayan, K.M.; Ali, M.K.; Koplan, J.P. Global noncommunicable diseases—Where worlds meet. N. Engl. J. Med. 2010, 363, 1196–1198. [Google Scholar] [CrossRef]
- World Health Organization. Non-Communicable Diseases. Available online: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 23 July 2020).
- Jain, V.; Duse, A.; Bausch, D.G. Planning for large epidemics and pandemics: Challenges from a policy perspective. Curr. Opin. Infect. Dis. 2018, 31, 316–324. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. World Health Statistics 2020: Monitoring Health for the SDGs, Sustainable Development Goals. Available online: https://www.who.int/publications-detail-redirect/9789240005105 (accessed on 10 July 2020).
- Palladino, R.; Bollon, J.; Ragazzoni, R.; Barone-Adesi, F. Excess deaths and hospital admissions for Covid-19 due to a late implementation of the lockdown in Italy. Int. J. Environ. Res. Public Health 2020, 17, 5644. [Google Scholar] [CrossRef]
- World Health Organization. European Mortality Database (MDB). Available online: https://gateway.euro.who.int/en/datasets/european-mortality-database/ (accessed on 15 April 2020).
- Eurostat Database. Causes of Death—Deaths by Country of Residence and Occurrence. Available online: https://appsso.eurostat.ec.europa.eu/nui/show.do?dataset=hlth_cd_aro&lang=en (accessed on 16 April 2020).
- International Statistical Classification of Diseases and Related Health Problems 10th Revision. Available online: https://icd.who.int/browse10/2016/en. (accessed on 15 April 2020).
- Breiman, L.; Friedman, J.H.; Olshen, R.; Stone, C.J. Classification and Regression Tree (Wadsworth Statistics/Probability), 1st ed.; Chapman and Hall/CRC Press: Boca Raton, FL, USA, 1984. [Google Scholar]
- Ward, J.H., Jr. Hierarchical grouping to optimize an objective function. J. Am. Stat. Assoc. 1963, 58, 236–244. [Google Scholar] [CrossRef]
- Murtagh, F.; Legendre, P. Ward’s hierarchical agglomerative clustering method: Which algorithms implement Ward’s criterion? J. Classif. 2014, 31, 274–295. [Google Scholar] [CrossRef]
- Calinski, T.; Harabasz, J. A dendrite method for cluster analysis. Commun. Stat. 1974, 3, 1–27. [Google Scholar]
- Roso-Llorach, A.; Violán, C.; Foguet-Boreu, Q.; Rodriguez-Blanco, T.; Pons-Vigues, M.; Pujol-Ribera, E.; Valderas, J.M. Comparative analysis of methods for identifying multimorbidity patterns: A study of ‘real-world’ data. BMJ Open 2018, 8, e018986. [Google Scholar] [CrossRef] [PubMed]
- Meslé, F.; Vallin, J.; Andreyev, Z.; Mesle, F. Mortality in Europe: The divergence between East and West. Population 2002, 57, 157. [Google Scholar] [CrossRef]
- Li, T.S.; Buckley, T.A.; Yap, F.H.; Sung, J.J.; Joynt, G.M. Severe acute respiratory syndrome (SARS): Infection control. Lancet 2003, 361, 1386. [Google Scholar] [CrossRef]
- Joossens, L.; Raw, M. The Tobacco Control Scale: A new scale to measure country activity. Tob. Control 2006, 15, 247–253. [Google Scholar] [CrossRef]
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Dyba, T.; Randi, G.; Bettio, M.; Gavin, A.; Visser, O.; Bray, F. Cancer incidence and mortality patterns in Europe: Estimates for 40 countries and 25 major cancers in 2018. Eur. J. Cancer 2018, 103, 356–387. [Google Scholar] [CrossRef]
- Movsisyan, N.K.; Vinciguerra, M.; Medina-Inojosa, J.R.; Lopez-Jimenez, F. Cardiovascular diseases in Central and Eastern Europe: A call for more surveillance and evidence-based health promotion. Ann. Glob. Health 2020, 86, 21. [Google Scholar] [CrossRef] [PubMed]
- Kashnitsky, I.; Aburto, J.M. The Pandemic Threatens Aged Rural Regions. Available online: https://doi.org/10.31219/osf.io/abx7s (accessed on 10 July 2020).
- The World Bank. World Bank Country and Lending Groups—World Bank Data Help Desk. Available online: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups (accessed on 15 July 2020).
- Popic, T.; Schneider, S.M. An East–West comparison of healthcare evaluations in Europe: Do institutions matter? J. Eur. Soc. Policy 2018, 28, 517–534. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Comorbidity Identified in Tomlins et al. (2020) [12] | Cause of Death—ICD-10 Code | Cause of Death—ICD-10 Code Included in the Research | Cause of Death in the Study |
|---|---|---|---|
| Hypertension | I10–I15 Hypertensive diseases | Other diseases of the circulatory system (remainder of I00–I99) | Other circulatory |
| Ischaemic heart disease | I20–I25 Ischaemic heart diseases | Ischaemic heart diseases (I20–I25) | Ischaemic heart |
| Cardiac failure | I50 Heart failure | Other heart diseases (I30–I51) | Other heart diseases |
| Arrhythmia | I49 Other cardiac arrhythmias | Other heart diseases (I30–I51) | |
| Valve disease | I30–51 Other heart diseases | Other heart diseases (I30–I51) | |
| Cerebrovascular | I60–69 Cerebrovascular diseases | Cerebrovascular diseases (I60–I69) | Cerebrovascular |
| Asthma | J45–46 Asthma and status asthmaticus | Asthma and status asthmaticus (J45–J46) | Asthma |
| Chronic obstructive pulmonary diseases | J44 Other chronic obstructive pulmonary disease (COPD) | Other lower respiratory diseases (J40–44_47) | Other lower respiratory |
| Bronchiectasis | J47. Bronchiectasis | Other lower respiratory diseases (J40–44_47) | |
| Obstructive sleep apnoea | G47.3. Sleep apnoea | Other lower respiratory diseases (J40–44_47) | |
| Gastrointestinal disease | Disease of the digestive system, unspecified K92.2 | Other diseases of the digestive system (remainder of K00–K93) | Other digestive diseases |
| Endocrine disease | E34–35 Endocrine disorders | Another endocrine, nutritional and metabolic diseases (remainder of E00–E90) | Other endocrine diseases |
| Obesity | Obesity and other hyperalimentation (E65–E68) | Another endocrine, nutritional and metabolic diseases (remainder of E00–E90) | |
| Diabetes | Diabetes mellitus (E10–14) | Diabetes mellitus (E10–14) | Diabetes |
| Malignancy | Malignant neoplasms (C00–C97) | Malignant neoplasms (C00–C97) | Malignancy |
| Neurological disease | Diseases of the nervous system and the sense organs (G00–H95) | Diseases of the nervous system and the sense organs (G00–H95) | Nervous system |
| Renal disease | Diseases of kidney and ureter N00–N29 | Diseases of the genitourinary system (N00–N99) | Genitourinary |
| Immunocompromised | D80-D89 Certain disorders involving the immune mechanism | Diseases of the blood and blood-forming organs and certain disorders involving the immune mechanism (D50–89) | Blood |
| Influenza | J09–J11 Influenza (including swine flu) | Influenza (including swine flu) (J09–J11) | Influenza |
| Diseases | Total Population | Population Aged 65 | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | Median | Minimum | Maximum | SE of Mean | IQR | Std.Dev. | Mean | Median | Minimum | Maximum | SE of Mean | IQR | Std.Dev. | |
| Malignancy | 25.391 | 25.491 | 16.424 | 31.410 | 0.643 | 3.176 | 3.400 | 22.983 | 23.105 | 13.439 | 28.534 | 0.650 | 3.384 | 3.441 |
| Blood diseases | 0.263 | 0.228 | 0.054 | 0.705 | 0.031 | 0.240 | 0.165 | 0.264 | 0.219 | 0.043 | 0.710 | 0.033 | 0.265 | 0.176 |
| Diabetes | 2.246 | 1.974 | 0.741 | 6.595 | 0.236 | 1.247 | 1.247 | 2.411 | 2.128 | 0.749 | 7.402 | 0.265 | 1.388 | 1.405 |
| Other endocrine | 0.553 | 0.462 | 0.037 | 1.506 | 0.080 | 0.659 | 0.425 | 0.512 | 0.387 | 0.027 | 1.600 | 0.084 | 0.652 | 0.443 |
| Nervous system | 3.530 | 3.125 | 0.975 | 14.281 | 0.491 | 2.835 | 2.600 | 3.692 | 3.198 | 0.887 | 16.486 | 0.576 | 3.202 | 3.049 |
| Ischaemic heart | 15.863 | 13.266 | 5.987 | 36.983 | 1.505 | 12.545 | 7.962 | 17.311 | 13.792 | 6.363 | 44.269 | 1.831 | 14.591 | 9.686 |
| Other heart diseases | 8.354 | 7.638 | 2.289 | 22.696 | 0.818 | 5.438 | 4.326 | 9.114 | 8.323 | 1.473 | 24.385 | 0.942 | 6.503 | 4.983 |
| Cerebrovascular | 9.556 | 8.427 | 5.673 | 19.613 | 0.729 | 4.416 | 3.857 | 10.876 | 9.528 | 6.394 | 22.423 | 0.877 | 5.062 | 4.643 |
| Other circulatory | 6.770 | 5.439 | 2.862 | 18.131 | 0.739 | 3.363 | 3.911 | 7.645 | 5.908 | 3.080 | 21.550 | 0.907 | 3.959 | 4.799 |
| Asthma | 0.132 | 0.120 | 0.015 | 0.320 | 0.012 | 0.057 | 0.064 | 0.136 | 0.121 | 0.014 | 0.378 | 0.014 | 0.052 | 0.074 |
| Other lower respiratory | 2.980 | 2.671 | 0.933 | 6.565 | 0.265 | 1.806 | 1.404 | 3.266 | 2.901 | 0.966 | 7.190 | 0.290 | 1.989 | 1.535 |
| Other digestive | 2.338 | 2.348 | 1.630 | 3.700 | 0.098 | 0.721 | 0.518 | 2.396 | 2.384 | 1.527 | 3.899 | 0.113 | 0.834 | 0.600 |
| Genitourinary diseases | 1.751 | 1.658 | 0.642 | 3.424 | 0.134 | 1.026 | 0.711 | 1.989 | 1.960 | 0.732 | 3.888 | 0.155 | 1.299 | 0.820 |
| Influenza | 0.072 | 0.059 | 0.009 | 0.181 | 0.009 | 0.060 | 0.048 | 0.065 | 0.050 | 0.004 | 0.178 | 0.010 | 0.061 | 0.052 |
| Diseases | Total Population | Population Aged 65 | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | Median | Minimum | Maximum | SE of Mean | IQR | Std.Dev. | Mean | Median | Minimum | Maximum | SE of Mean | IQR | Std.Dev. | |
| Malignancy | 0.123 | 0.238 | −0.873 | 1.434 | 0.123 | 1.093 | 0.653 | 0.406 | 0.553 | −0.845 | 2.224 | 0.175 | 1.415 | 0.925 |
| Blood diseases | −0.356 | 0.306 | −12.237 | 7.891 | 0.867 | 4.684 | 4.587 | −0.615 | 0.093 | −17.871 | 8.631 | 1.190 | 6.015 | 6.296 |
| Diabetes | 2.101 | 0.704 | −4.231 | 29.480 | 1.190 | 3.338 | 6.295 | 1.868 | 0.602 | −4.934 | 29.287 | 1.205 | 3.876 | 6.375 |
| Other endocrine | 3.489 | 3.091 | −8.126 | 12.368 | 0.947 | 7.234 | 5.014 | 3.689 | 3.716 | −13.003 | 14.980 | 1.156 | 6.427 | 6.117 |
| Nervous system | 4.564 | 4.109 | −0.958 | 14.782 | 0.654 | 4.533 | 3.460 | 5.189 | 4.437 | −0.887 | 17.092 | 0.848 | 5.096 | 4.487 |
| Ischaemic heart | −2.324 | −2.538 | −4.490 | 0.550 | 0.286 | 2.746 | 1.512 | −2.044 | −2.211 | −3.902 | 0.471 | 0.234 | 1.968 | 1.237 |
| Other heart diseases | 0.103 | 0.483 | −9.167 | 5.511 | 0.686 | 3.956 | 3.628 | −0.487 | 0.133 | −17.935 | 5.391 | 0.899 | 3.699 | 4.759 |
| Cerebrovascular | −2.406 | −2.374 | −6.396 | 4.352 | 0.415 | 2.751 | 2.198 | −2.890 | −2.775 | −6.635 | 4.117 | 0.427 | 2.659 | 2.259 |
| Other circulatory | 1.033 | 0.760 | −3.568 | 11.220 | 0.562 | 2.709 | 2.975 | 0.717 | 0.362 | −5.603 | 11.710 | 0.628 | 3.110 | 3.325 |
| Asthma | 1.569 | 0.715 | −13.648 | 27.244 | 1.542 | 5.207 | 8.157 | 2.940 | 0.861 | −10.800 | 47.750 | 2.239 | 6.046 | 11.845 |
| Other lower respiratory | 0.979 | 1.140 | −4.496 | 8.991 | 0.553 | 3.114 | 2.925 | 0.624 | 0.770 | −5.150 | 8.017 | 0.582 | 3.254 | 3.079 |
| Other digestive | 0.240 | 0.155 | −4.299 | 6.736 | 0.473 | 2.769 | 2.501 | 0.109 | −0.259 | −5.104 | 7.863 | 0.543 | 3.172 | 2.871 |
| Genitourinary diseases | 1.582 | 2.098 | −10.691 | 11.418 | 0.919 | 6.527 | 4.865 | 1.469 | 1.962 | −12.027 | 11.895 | 0.988 | 6.993 | 5.226 |
| Influenza | 13.136 | 11.272 | −30.435 | 95.694 | 4.929 | 28.678 | 25.613 | 22.740 | 23.493 | −26.633 | 126.523 | 6.101 | 33.284 | 31.702 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Horobet, A.; Simionescu, A.A.; Dumitrescu, D.G.; Belascu, L. Europe’s War against COVID-19: A Map of Countries’ Disease Vulnerability Using Mortality Indicators. Int. J. Environ. Res. Public Health 2020, 17, 6565. https://doi.org/10.3390/ijerph17186565
Horobet A, Simionescu AA, Dumitrescu DG, Belascu L. Europe’s War against COVID-19: A Map of Countries’ Disease Vulnerability Using Mortality Indicators. International Journal of Environmental Research and Public Health. 2020; 17(18):6565. https://doi.org/10.3390/ijerph17186565
Chicago/Turabian StyleHorobet, Alexandra, Anca Angela Simionescu, Dan Gabriel Dumitrescu, and Lucian Belascu. 2020. "Europe’s War against COVID-19: A Map of Countries’ Disease Vulnerability Using Mortality Indicators" International Journal of Environmental Research and Public Health 17, no. 18: 6565. https://doi.org/10.3390/ijerph17186565
APA StyleHorobet, A., Simionescu, A. A., Dumitrescu, D. G., & Belascu, L. (2020). Europe’s War against COVID-19: A Map of Countries’ Disease Vulnerability Using Mortality Indicators. International Journal of Environmental Research and Public Health, 17(18), 6565. https://doi.org/10.3390/ijerph17186565