Effectiveness of Nurse-Led Heart Failure Self-Care Education on Health Outcomes of Heart Failure Patients: A Systematic Review and Meta-Analysis


Abstract
1. Introduction
2. Methods
2.1. Search Strategies
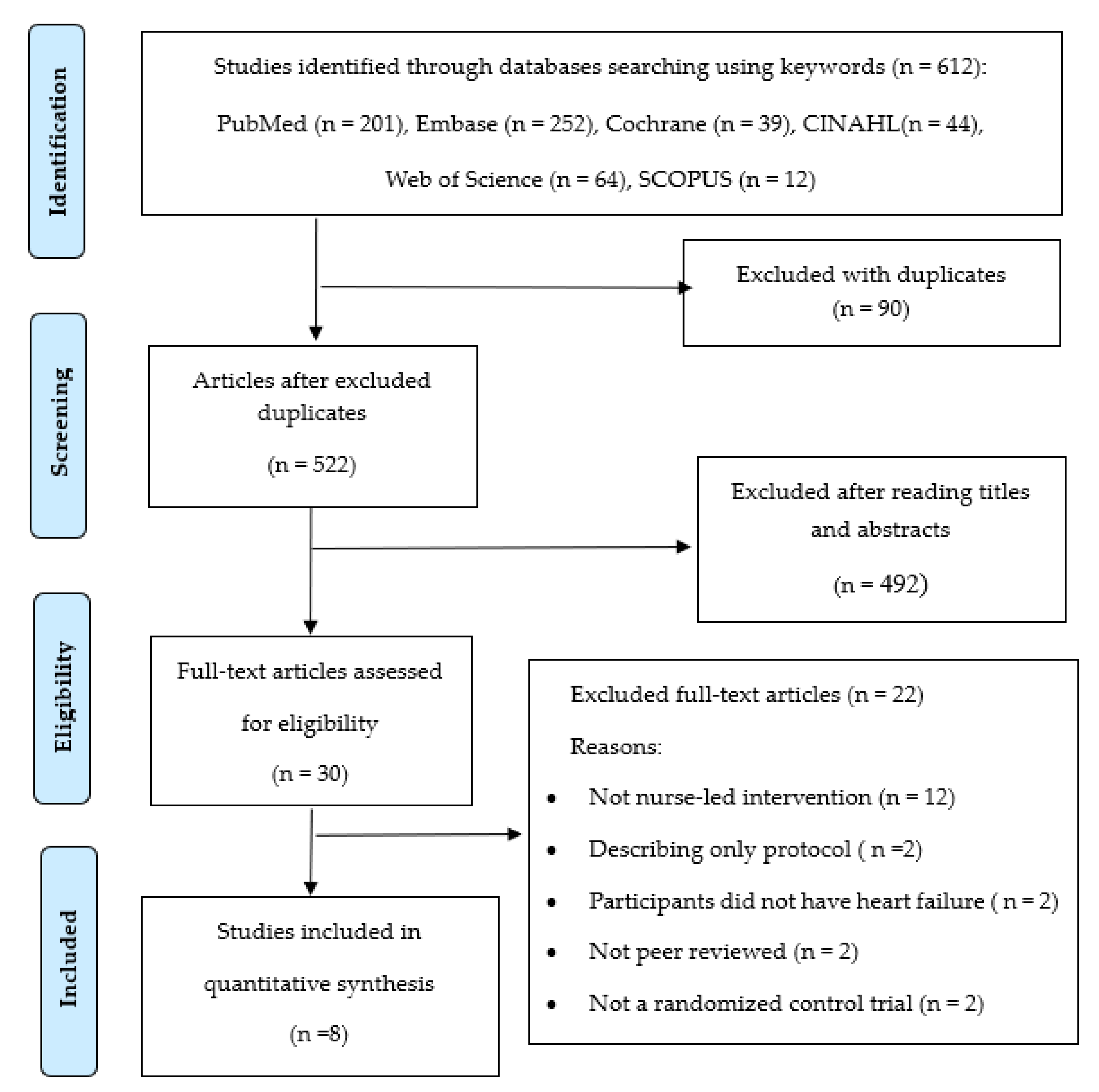
2.2. Study Selection
2.3. Data Extraction
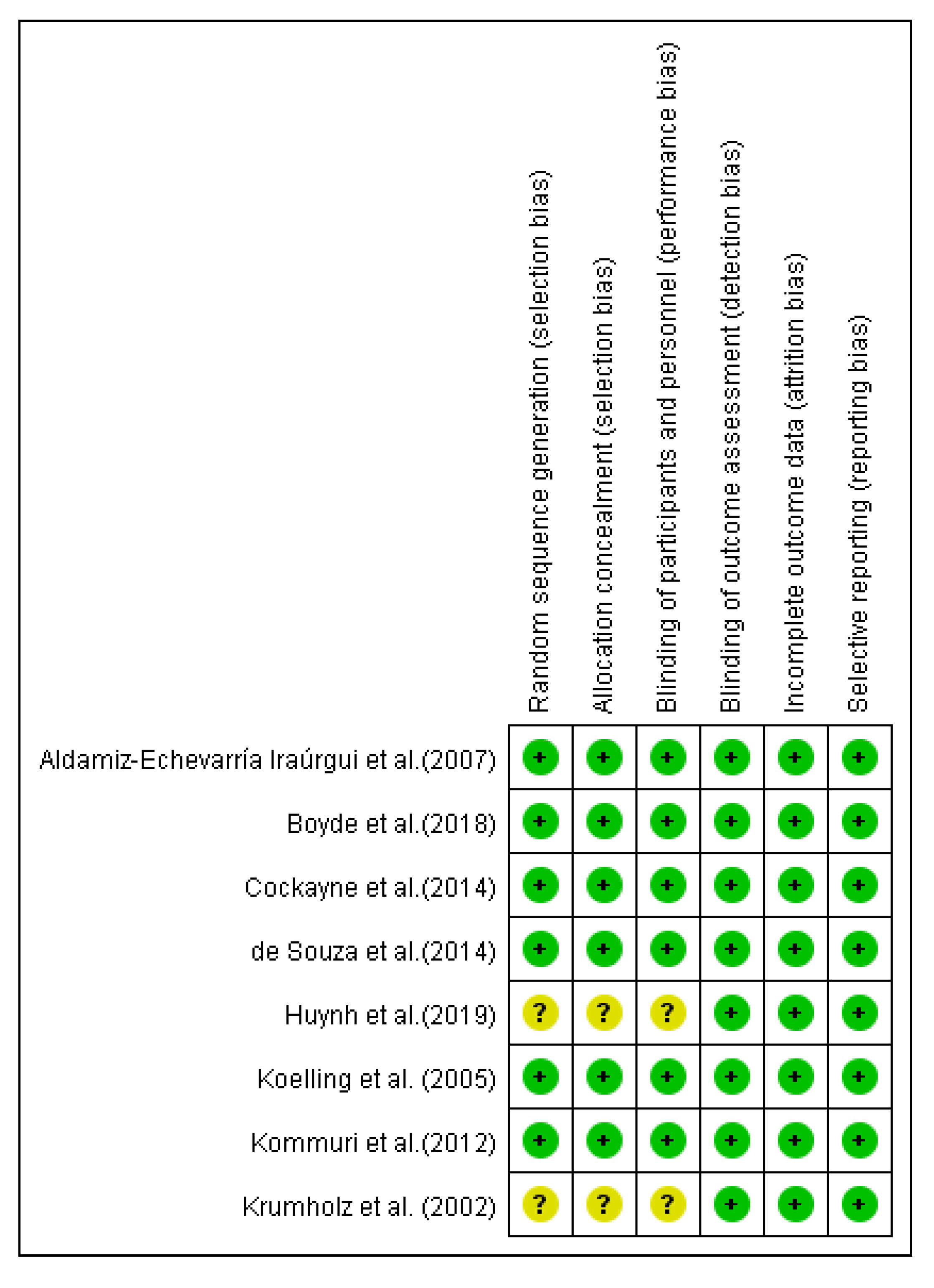
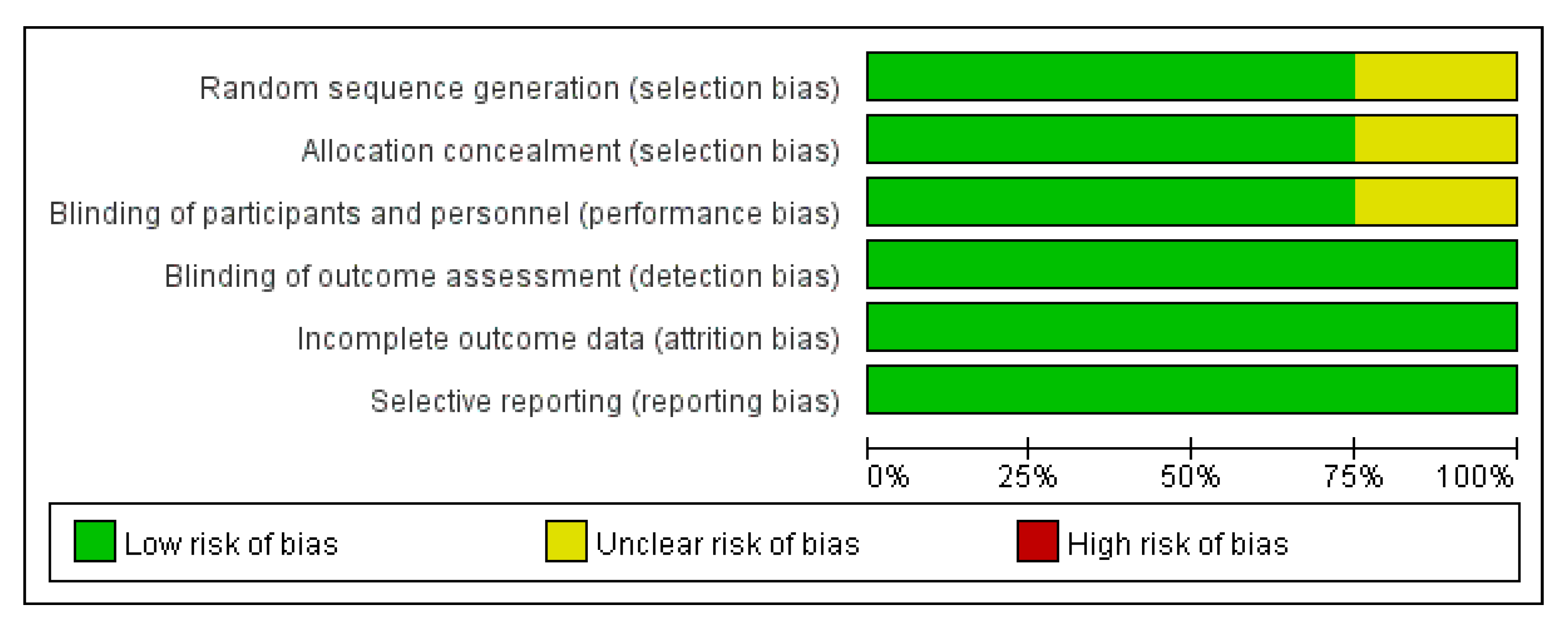
2.4. Assessment of Methodological Quality
2.5. Data Synthesis
3. Results
3.1. Study Quality Appraisal
3.2. Study Settings and Patient Characteristics Included
3.3. Components of Heart Failure Self-Care Education Interventions
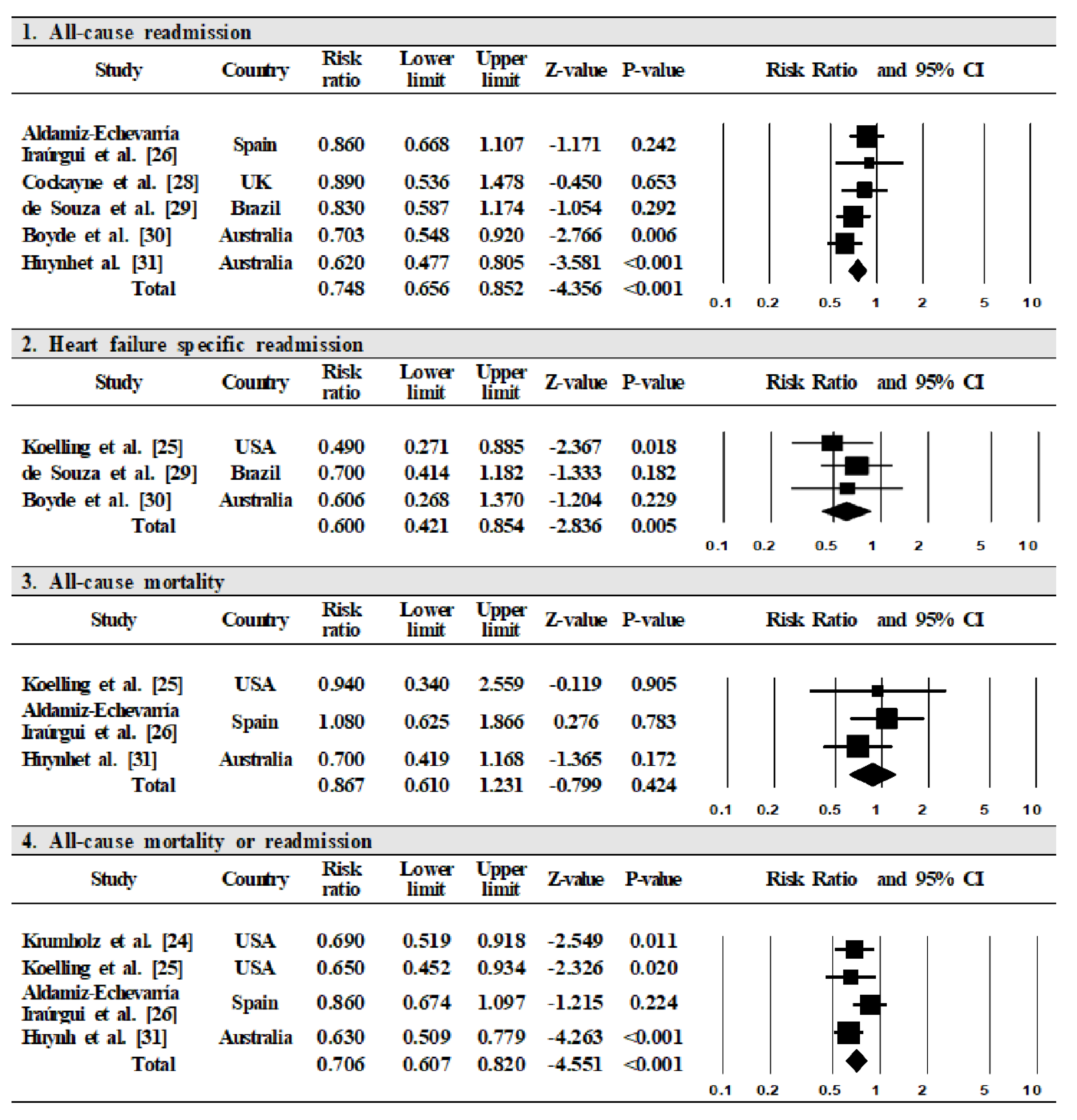
3.4. Study Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Von Lueder, T.G.; Agewall, S. The burden of heart failure in the general population: A clearer and more concerning picture. J. Thorac. Dis. 2018, 10, S1934–S1937. [Google Scholar] [CrossRef]
- Savarese, G.; Lund, L.H. Global public health burden of heart failure. Card. Fail. Rev. 2017, 3, 7–11. [Google Scholar] [CrossRef]
- Go, A.S.; Mozaffarian, D.; Roger, V.L.; Benjamin, E.J.; Berry, J.D.; Blaha, M.J.; Dai, S.; Ford, E.S.; Fox, C.S.; Franco, S.; et al. Heart disease and stroke statistics—2014 update: A report from the American Heart Association. Circulation 2014, 129, e28–e292. [Google Scholar] [CrossRef] [PubMed]
- Lesyuk, W.; Kriza, C.; Kolominsky-Rabas, P. Cost-of-illness studies in heart failure: A systematic review 2004-2016. BMC Cardiovasc. Disord. 2018, 18. [Google Scholar] [CrossRef] [PubMed]
- Salahodinkolah, M.K.; Ganji, J.; Moghadam, S.H.; Shafipour, V.; Jafari, H.; Salari, S. Educational intervention for improving self-care behaviors in patients with heart failure: A narrative review. J. Nurs. Midwifery Sci. 2020, 7, 60–68. [Google Scholar] [CrossRef]
- Ba, H.M.; Son, Y.; Lee, K.; Kim, B.-H. Transitional Care Interventions for Patients with Heart Failure: An Integrative Review. Int. J. Environ. Res. Public Health 2020, 17, 2925. [Google Scholar] [CrossRef]
- Greene, S.J.; Fonarow, G.C.; Vaduganathan, M.; Khan, S.S.; Butler, J.; Gheorghiade, M. The vulnerable phase after hospitalization for heart failure. Nat. Rev. Cardiol. 2015, 12, 220–229. [Google Scholar] [CrossRef]
- Lee, C.S.; Mudd, J.O.; Hiatt, S.O.; Gelow, J.M.; Chien, C.; Riegel, B. Trajectories of heart failure self-care management and changes in quality of life. Eur. J. Cardiovasc. Nurs. 2015, 14, 486–494. [Google Scholar] [CrossRef]
- McMurray, J.J.; Adamopoulos, S.; Anker, S.D.; Auricchio, A.; Böhm, M.; Dickstein, K.; Falk, V.; Filippatos, G.; Fonseca, C.; Gomez-Sanchez, M.A.; et al. ESC Committee for Practice Guidelines. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: The task force for the diagnosis and treatment of acute and chronic heart failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2012, 33, 1787–1847. [Google Scholar] [CrossRef]
- Toukhsati, S.R.; Driscoll, A.; Hare, D.L. Patient self-management in chronic heart failure—Establishing concordance between guidelines and practice. Card. Fail. Rev. 2015, 1, 128–131. [Google Scholar] [CrossRef]
- Jonkman, N.H.; Westland, H.; Groenwold, R.H.H.; Ågren, S.; Atienza, F.; Blue, L.; de la Bruggink-André Porte, P.W.F.; Darren A DeWalt, D.A.; Hebert, P.L.; Heisler, M.; et al. Do self-management interventions work in patients with heart failure? An individual patient data meta-analysis. Circulation 2016, 133, 1189–1198. [Google Scholar] [CrossRef] [PubMed]
- Herber, O.R.; Atkins, L.; Störk, S.; Wilm, S. Enhancing self-care adherence in patients with heart failure: A study protocol for developing a theory-based behaviour change intervention using the COM-B behaviour model (ACHIEVE study). BMJ Open 2018, 8, e025907. [Google Scholar] [CrossRef] [PubMed]
- Seid, M.A.; Abdela, O.A.; Zeleke, E.G. Adherence to self-care recommendations and associated factors among adult heart failure patients. From the patients’ point of view. PLoS ONE 2019, 14, e0211768. [Google Scholar] [CrossRef] [PubMed]
- Jaarsma, T.; Cameron, J.; Riege, B.; Stromberg, A. Factors related to self-care in heart failure patients according to the middle-range theory of self-care of chronic illness: A literature update. Curr. Heart Fail. Rep. 2017, 14, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Francis, L.P.; Spaulding, E.; Turkson-Ocran, R.A.; Allen, J. Randomized trials of nurse-delivered interventions in weight management research: A systematic review. West. J. Nurs. Res. 2017, 39, 1120–1150. [Google Scholar] [CrossRef]
- Rasmusson, K.; Flattery, M.; Baas, L.S. American association of heart failure nurses position paper on educating patients with heart failure. Heart Lung 2015, 44, 173–177. [Google Scholar] [CrossRef]
- Clark, C.E.; Smith, L.F.P.; Taylor, R.S.; Campbell, J.L. Nurse led interventions to improve control of blood pressure in people with hypertension: Systematic review and meta-analysis. BMJ 2010, 341, c3995. [Google Scholar] [CrossRef]
- Lambrinou, E.; Kalogirou, F.; Lamnisos, D.; Sourtzi, P. Effectiveness of heart failure management programmes with nurse-led discharge planning in reducing re-admissions: A systematic review and meta-analysis. Int. J. Nurs. Stud. 2012, 49, 610–624. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Haynes, R.B.; Sacket, D.L.; Guyatt, G.H.; Tugwell, P. Clinical Epidemiology: How Clinical Practice Research, 3rd ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2006; ISBN 078-174-524-1. [Google Scholar]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration′s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analysis. BMJ 2003, 327, 557. [Google Scholar] [CrossRef] [PubMed]
- Song, F.; Khan, K.S.; Dinne, J.; Sutton, A.J. Asymmetric funnel plots and publication bias in meta-analyses of diagnostic accuracy. Int. J. Epidemiol. 2002, 31, 88–95. [Google Scholar] [CrossRef] [PubMed]
- Krumholz, H.M.; Amatruda, J.; Smith, G.L.; Mattera, J.A.; Roumanis, S.A.; Radford, M.J.; Crombie, P.; Vaccarino, V. Randomized trial of an education and support intervention to prevent readmission of patients with heart failure. J. Am. Coll. Cardiol. 2002, 39, 83–89. [Google Scholar] [CrossRef]
- Koelling, T.M.; Johnson, M.L.; Cody, R.J.; Aaronson, K.D. Discharge education improves clinical outcomes in patients with chronic heart failure. Circulation 2005, 111, 179–185. [Google Scholar] [CrossRef]
- Aldamiz-Echevarría Iraúrgui, B.; Muñiz, J.; Rodríguez-Fernández, J.A.; Vidán-Martínez, L.; Silva-César, M.; Lamelo-Alfonsín, F.; Díaz-Díaz, J.L.; Ramos-Polledo, V.; Castro-Beiras, A. Randomized controlled clinical trial of a home care unit intervention to reduce readmission and death rates in patients discharged from hospital following admission for heart failure. Rev. Esp. Cardiol. 2007, 60, 914–922. [Google Scholar] [CrossRef][Green Version]
- Kommuri, N.V.A.; Johnson, M.L.; Koelling, T.M. Relationship between improvements in heart failure patient disease specific knowledge and clinical events as part of a randomized controlled trial. Patient Educ. Couns. 2012, 86, 233–238. [Google Scholar] [CrossRef]
- Cockayne, S.; Pattenden, J.; Worthy, G.; Richardson, G.; Lewin, R. Nurse facilitated self-management support for people with heart failure and their family carers (SEMAPHFOR): A randomised controlled trial. Int. Nurs. Stud. 2014, 5, 1207–1213. [Google Scholar] [CrossRef]
- De Souza, E.N.; Rohde, L.E.; Ruschel, K.B.; Mussi, C.M.; Beck-da-Silva, L.; Biolo, A.; Clausell, N.; Rabelo-Silva, E.R. A nurse-based strategy reduces heart failure morbidity in patients admitted for acute decompensated heart failure in Brazil: The HELEN-II clinical trial. Eur. J. Heart Fail. 2014, 16, 1002–1008. [Google Scholar] [CrossRef]
- Boyde, M.; Peters, R.; New, N.; Hwang, R.; Ha, T.; Korczyk, D. Self-care educational intervention to reduce hospitalisations in Heart Failure: A randomised controlled trial. Eur. J. Cardiovasc. Nurs. 2018, 17, 178–185. [Google Scholar] [CrossRef]
- Huynh, Q.L.; Whitmore, K.; Negishi, K.; Marwick, T.H.; ETHELRED Investigators. Influence of risk on reduction of readmission and death by disease management programs in heart failure. J. Card. Fail. 2019, 25, 330–339. [Google Scholar] [CrossRef]
- Albert, N.M.; Cohen, B.; Liu, X.; Best, C.H.; Aspinwall, L.; Prarr, L. Hospital nurses’ comfort in and frequency of delivering heart failure self-care education. Eur. J. Cardiovasc. Nurs. 2015, 14, 431–440. [Google Scholar] [CrossRef] [PubMed]
- Bramhall, E. Effective communication skills in nursing practice. Nurs. Stand. 2014, 29, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Weiss, E.M.; Costa, L.L.; Yakusheva, O.; Bobay, K.L. Validation of patient and nurse short forms of the readiness for hospital discharge scale and their relationship to return to the hospital. Health Serv. Res. 2014, 49, 304–317. [Google Scholar] [CrossRef] [PubMed]
- Halcomb, E.J.; McInnes, S.; Patterson, C.; Moxham, L. Nurse-delivered interventions for mental health in primary care: A systematic review of randomized controlled trials. Fam. Pract. 2019, 36, 64–71. [Google Scholar] [CrossRef]
- Gonzalez, Y.; Kozachik, S.L.; Hansen, B.R.; Sanchez, M.; Finnell, D.S. Nurse-led delivery of brief interventions for at- risk alcohol use: An integrative review. J. Am. Psychiatr. Nurses. Assoc. 2020, 26, 27–42. [Google Scholar] [CrossRef]
- Davis, E.M.; Packard, K.A.; Jackevicius, C.A. The pharmacist role in predicting and improving medication adherence in heart failure patients. J. Manag. Care Spec. Pharm. 2014, 20, 741–755. [Google Scholar] [CrossRef]
- Arcand, J.A.L.; Brazel, S.; Joliffe, C.; Choleva, M.; Berkoff, F.; Allard, J.P.; Newton, G.E. Education by a dietitian in patients with heart failure results in improved adherence with a sodium-restricted diet: A randomized trial. Am. Heart J. 2005, 150, 716.e1–716.e5. [Google Scholar] [CrossRef]
- Riegel, B.; Dickson, V.V.; Faulkner, K.M. The situation-specific theory of heart failure self-care: Revised and updated. J. Cardiovasc. Nurs. 2016, 31, 226–235. [Google Scholar] [CrossRef]
- Gabet, A.; Juillière, Y.; Lamarche-Vadel, A.; Vernay, M.; Olié, V. National trends in rate of patients hospitalized for heart failure and heart failure mortality in France, 2000-2012. Eur. J. Heart Fail. 2015, 17, 583–590. [Google Scholar] [CrossRef]
- Dinatolo, E.; Sciatti, E.; Anker, M.S.; Lombardi, C.; Dasseni, N.; Metra, M. Updates in heart failure: What last year brought to us. ESC Heart Fail. 2018, 5, 989–1007. [Google Scholar] [CrossRef]
- Lee, H.J.; Kim, Y.; Oh, E.G. A systematic review on nurse-led transitional care programs for discharged patients from hospital to home. J. Korean Clin. Res. 2017, 23, 376–387. [Google Scholar] [CrossRef]
- Van der Wal, M.H.L.; Jaarsma, T.; Moser, D.K.; van Veldhuisen, D.J. Development and testing of the Dutch Heart Failure Knowledge Scale. Eur. J. Cardiovasc. Nurs. 2005, 4, 273–277. [Google Scholar] [CrossRef] [PubMed]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.; Coats, A.J.; Falk, V.; González-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Heart Fail. 2016, 18, 891–975. [Google Scholar] [CrossRef] [PubMed]
- The Joint Commission. Advancing Effective Communication, Cultural Competence, and Patient-and Family-Centered Care: A Roadmap for Hospitals. Available online: https://www.jointcommission.org/assets/1/6/ARoadmapforHospitalsfinalversion727.pdf (accessed on 10 May 2020).
- De Vecchis, R.; Manginas, A.; Noutsias, E.; Tschöpe, C.; Noutsias, M. Comorbidity “depression” in heart failure—Potential target of patient education and self-management. BMC Cardiovasc. Disord. 2017, 17, 48. [Google Scholar] [CrossRef] [PubMed]
- Buck, H.G.; Stromberg, A.; Chung, M.L.; Donovan, K.A.; Harkness, K.; Howard, A.M.; Kato, N.; Polo, R.; Evangelista, L.S. A systematic review of heart failure dyadic self-care interventions focusing on intervention components, contexts, and outcomes. Int. J. Nurs. Stud. 2018, 77, 232–242. [Google Scholar] [CrossRef]
- Scott, I.A. Preventing the rebound: Improving care transition in hospital discharge processes. Aust. Health Rev. 2010, 34, 445–451. [Google Scholar] [CrossRef]
- Jennings, J.H.; Thavarajah, K.; Mendez, M.P.; Eichenhorn, M.; Kvale, P.; Yessayan, L. Predischarge bundle for patients with acute exacerbations of COPD to reduce readmissions and ED visits: A randomized controlled trial. Chest 2015, 147, 1227–1234. [Google Scholar] [CrossRef]
- Riegel, B.; Driscoll, A.; Suwanno, J.; Moser, D.K.; Lennie, T.A.; Chung, M.L.; Wu, J.; Dickson, V.V.; Carlson, B.; Cameron, J. Heart failure self-care in developed and developing countries. J. Card. Fail. 2009, 15, 508–516. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors (Publication Year)/Location | Participants | Time of Initiation | Duration of Intervention Delivery | Follow-Up Period | Intervention | Outcome Variables | Main Findings | ||
|---|---|---|---|---|---|---|---|---|---|
| Intervention Group | Control Group | ||||||||
| Krumholz et al. (2002)/USA [24] | N = 44 Mean age: 75.9 yr M: 48%, F: 52% NYHA: unreported Mean LVEF: 38.0% | N = 44 Mean age: 71.6 yr M: 66%, F: 34% NYHA: unreported Mean LVEF: 37.0% | Prior to discharge | 12 months | 12 months | ·Intervention: Cardiac nurse reviewed (once/1 h) patient’s knowledge of heart failure in one to one and used phone call (17 times) to support heart failure care and management. ·Control: Not detail reported. | All-cause mortality or readmission, heart failure mortality or readmission, costs | Intervention group had significantly lower on all-cause mortality or hospital readmission (p = 0.01), heart failure mortality or readmission (p = 0.01), costs (p = 0.02) | |
| Koelling et al. (2005)/USA [25] | N = 107 Mean age: 65 yr M: 58%, F: 42% NYHA: unknown Mean LVEF: 26% | N = 116 Mean age: 64 yr M: 58%, F: 42% NYHA: unknown Mean LVEF: 27% | Prior to discharge | 1 day | 6 months | ·Intervention: Nurse educator discussed (once/1 h) heart failure-specific information that covered the basic principles of the causes of heart failure and rationale for pharmaceutical therapies. ·Control: Received standard written discharge information. | All-cause mortality or readmission, all-cause mortality, heart failure specific readmission, cost | Intervention group had significantly lower on all-cause mortality or readmission (p = 0.018), heart failure specific readmission (p = 0.015), cost (p = 0.035); No significant difference in all-cause mortality, QoL | |
| Aldamiz-Echevarría Iraúrgui et al. (2007)/Spain [26] | N = 137 Mean age: 75 yr M: 39%, F: 61% NYHA: unreported Mean LVEF: 50.9% | N = 142 Mean age: 76 yr M: 40%, F: 60% NYHA: unreported Mean LVEF: 48.3% | Within 15 days after hospital discharge | 15 days | 12 months | ·Intervention: Nurse visited home 3 times (1 h) after discharge to administer the education program, teaching patient and relatives basic facts about heart failure and its management (symptoms, lifestyle, diet, therapy) ·Control: Not detail reported. | All-cause mortality or readmission, all-cause mortality, all-cause readmission | No significant difference in all-cause mortality or readmission, all-cause mortality, all-cause readmission | |
| Kommuri et al. (2012)/USA [27] | N = 128 Mean age: 66 yr M: 61%, F: 39% NYHA: unknown Mean LVEF: 25% | N = 137 Mean age: 67 yr M: 61%, F: 39% NYHA: unknown Mean LVEF: 26.5% | Prior to discharge | 1 day | 3 months | ·Intervention: Nurse educated (once/1 h) the basic principles of heart failure, role of dietary sodium, importance of limitation of fluid intake, the mechanisms of diuretics, and the rationale for other pharmacotherapy. ·Control: Received standard discharge information. | Heart failure knowledge | Intervention group had significantly higher on heart failure knowledge (p = 0.007). | |
| Cockayne et al.(2014) /UK [28] | N = 95 Mean age: 70 yr M: 73%, F: 27% NYHA: Ⅰ-Ⅱ= 73%, Ⅲ-Ⅳ= 27%, Mean LVEF: unreported | N = 165 Mean age: 70 yr M: 72%, F: 28% NYHA: Ⅰ-Ⅱ= 66%, Ⅲ-Ⅳ= 34%, Mean LVEF: unreported | After discharge | 12 months | 12 months | ·Intervention: Specialist heart failure nurse provided (up to 6 times) self-management program (The heart plan) and accompanying DVD, relaxation tape, exercises, regular monitoring of symptoms, blood tests, clinical assessments, referrals.·Control: Given the same self-management manual. | All-cause readmission, QoL | No significant difference in all-cause readmission, QoL | |
| de Souza et al.(2014)/ Brazil [29] | N = 123 Mean age: 62 yr M: 61 %, F: 39% NYHA: Ⅰ-Ⅱ= 46%, Ⅲ-Ⅳ= 54%, Mean LVEF: 29% | N = 129 Mean age: 62 yr M: 64%, F: 36% NYHA: Ⅰ-Ⅱ= 42%, Ⅲ-Ⅳ= 58%, Mean LVEF: 30% | Within 10 days after hospital discharge | 4 months | 6 months | ·Intervention: Nurses provided a heart failure-focused physical examination (Clinical Congestion Score, blood pressure, jugular venous pressure) through a home visits (4 times/~60 min). Phone calls (4 times/~10 min) were used to reinforce recommendations given during home visits, check the use of prescribed medications. ·Control: Received instructions regarding pharmacological and non-pharmacological therapeutic strategies. | All-cause mortality, all-cause readmission, heart failure specific readmission & ED visits, heart failure knowledge | Intervention group had significantly higher on heart failure knowledge (p < 0.001); No significant difference in all-cause mortality, all-cause readmission, heart failure specific readmission & ED visits | |
| Boyde et al. (2018)/ Australia [30] | N = 100 Mean age: 64 yr M: 77%, F: 23% NYHA: Ⅰ-Ⅱ= 35%, Ⅲ-Ⅳ= 65%, LVEF: <36%: 75% | N = 100 Mean age: 64 yr M: 69%, F: 31% NYHA: Ⅰ-Ⅱ= 31%, Ⅲ-Ⅳ= 69%, LVEF: <36%: 83% | Unreported | 1 day | 12 months | ·Intervention: Patients watched the DVD for 30 min on the role model of self-care behaviors and participated in a one to one discussion with a specialist heart failure nurse (once/60~90 min) ·Control: Received 30–60 min of standard education and offered a short booklet outlining a brief overview of diagnosis, symptoms, and treatment of heart failure. | All-cause readmission, heart failure specific readmission, heart failure knowledge, self-care behaviors | Intervention group had significantly lower on all-cause readmission (p = 0.005); No significant difference in heart failure specific readmission, heart failure knowledge, self-care behaviors | |
| Huynh et al. (2019)/ Australia [31] | N = 215 Mean age: 73.9 yr M: 51%, F: 49% NYHA: Ⅰ–Ⅱ = 30%, Ⅲ–Ⅳ = 70%, Mean LVEF: 39% | N = 197 Mean age: 74.7 yr M: 58%, F: 42% NYHA: Ⅰ–Ⅱ = 35%, Ⅲ–Ⅳ = 65%, Mean LVEF: 40% | Prior to discharge | 2 weeks | 3 months | ·Intervention: Patients were checked for intravascular capacity before discharge and educated in self-care and exercise by leaflet and video instruction. Cardiac nurse’s phone calls (twice) for transition coach and support. Home visits (twice) provided an opportunity to react to any outstanding or emerging issues to prevent them from growing into more serious events, as well as to provide patients with mental and physical support. Control: Received a standard disease management program and standard discharge plan. | All-cause mortality or readmission, all-cause mortality, all-cause readmission | Intervention group had significantly lower on all-cause mortality or readmission (95% CI = 0.46–0.84), all-cause readmission (95% CI = 0.45–0.88); No significant difference in all-cause mortality | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Son, Y.-J.; Choi, J.; Lee, H.-J. Effectiveness of Nurse-Led Heart Failure Self-Care Education on Health Outcomes of Heart Failure Patients: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 6559. https://doi.org/10.3390/ijerph17186559
Son Y-J, Choi J, Lee H-J. Effectiveness of Nurse-Led Heart Failure Self-Care Education on Health Outcomes of Heart Failure Patients: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2020; 17(18):6559. https://doi.org/10.3390/ijerph17186559
Chicago/Turabian StyleSon, Youn-Jung, JiYeon Choi, and Hyeon-Ju Lee. 2020. "Effectiveness of Nurse-Led Heart Failure Self-Care Education on Health Outcomes of Heart Failure Patients: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 17, no. 18: 6559. https://doi.org/10.3390/ijerph17186559
APA StyleSon, Y.-J., Choi, J., & Lee, H.-J. (2020). Effectiveness of Nurse-Led Heart Failure Self-Care Education on Health Outcomes of Heart Failure Patients: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 17(18), 6559. https://doi.org/10.3390/ijerph17186559