The Effects of Cognitive Task and Change of Height on Postural Stability and Cardiovascular Stress in Workers Working at Height




Abstract
1. Introduction
2. Materials and Methods
2.1. Characteristics of the Study Group
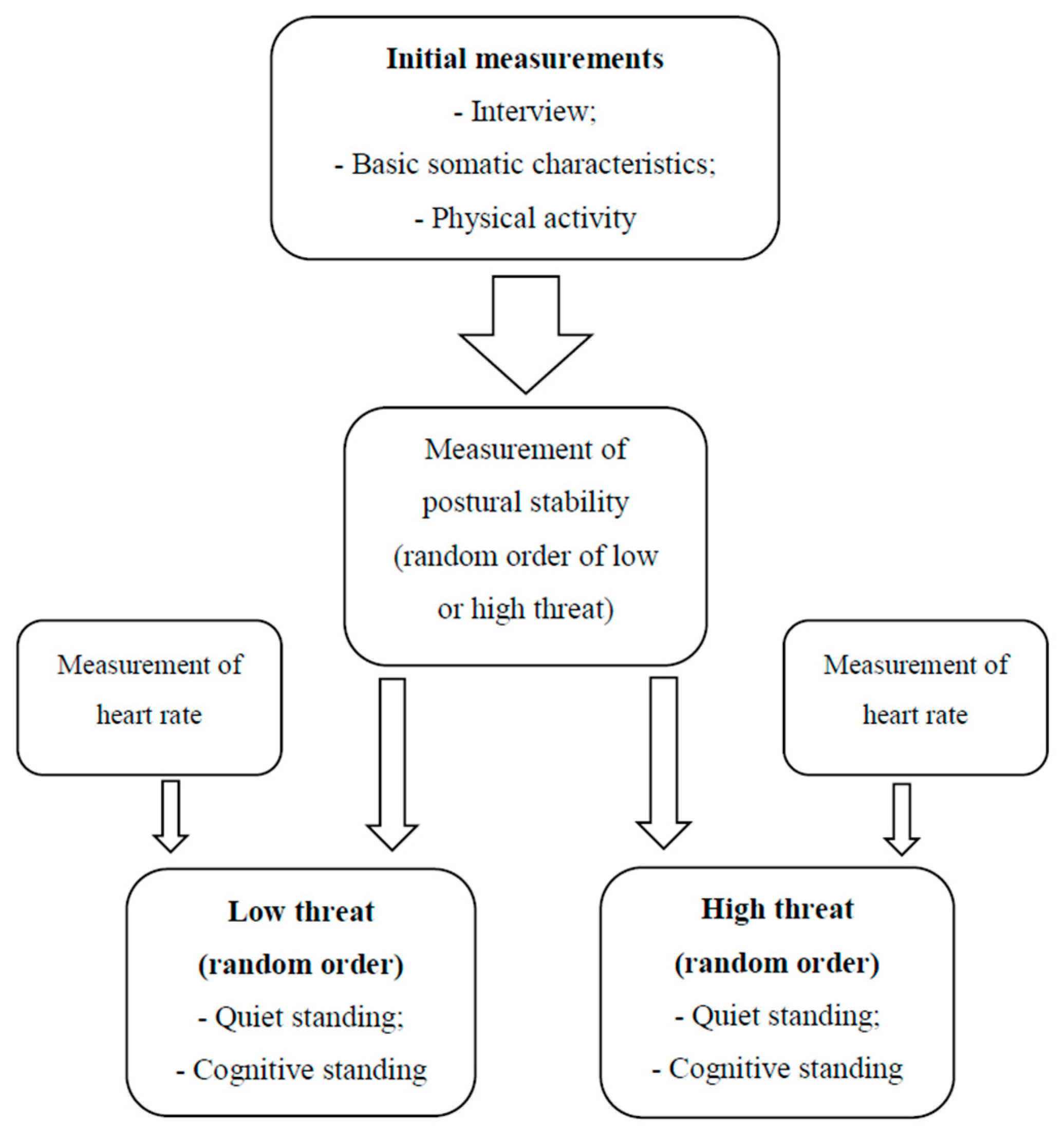
2.2. Procedures
- Quiet standing with one’s eyes open: the subject stood still in the center of the platform with bare feet hip-width apart and arms down at sides. The posturography platform was placed three meters in front of a white wall, which subjects were asked to look directly at.
- Cognitive standing: the subject stood freely in the above-mentioned position and additionally performed a mathematical task, which consisted of counting backwards every third number down from the number 200 during the time of recording the data [37].
2.3. Measurement
2.3.1. Level of Physical Activity (PA)
2.3.2. Postural Stability (PS)
2.3.3. Cardiovascular Stress
2.3.4. Statistical analysis
3. Results
3.1. Influence of Height on the Postural Stability of Employees
3.2. The Impact of Performing a Cognitive Task on Employees’ Postural Stability
3.3. The Influence of Altitude on Cardiovascular Stress
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- European Commission. Causes and Circumstances of Accidents at Work. Luxembourg: European Commission DG Employment, Social Affairs and Equal Opportunities. 2009. Available online: https://op.europa.eu/en/publication-detail/-/publication/f73a06d6-c488-44a1-8c08-80f53e0de160 (accessed on 18 August 2020).
- Occupational Safety and Health Administration (OSHA). Walking-Working Surfaces and Personal Protective Equipment (Fall Protection Systems). Federal Registered The Daily Journal of the United State Government. 2016. Available online: https://www.federalregister.gov/documents/2016/11/18/2016-24557/walking-workingsurfaces-and-personal-protective-equipment-fall-protection-systems (accessed on 18 August 2020).
- Regulation of the Minister of Health and Social Welfare of 30 May 1996 on Carrying out Medical Examinations for Workers, the Scope of Preventive Health Care for Workers, and Medical Certificates Issued for the Purposes Set out in the Labor Code. Journal of Laws 1996, No.69, Item 332. Available online: http://isap.sejm.gov.pl/isap.nsf/DocDetails.xsp?id=WDU19960690332 (accessed on 7 September 2020). (In Polish)
- Central Statistical Office. Labor Market Monitoring. Accidents at Work in 2012. Department of Demography and Labor Market Research. 2012. Available online: https://stat.gov.pl/obszary-tematyczne/rynek-pracy/warunki-pracy-wypadki-przy-pracy/wypadki-przy-pracy-w-2012-r-,4,5.html (accessed on 7 September 2020). (In Polish)
- Hu, K.; Rahmandad, H.; Jackson, T.S.; Winchester, W. Factors influencing the risk of falls in the construction industry: A review of the evidence. Constr. Manag. Econ. 2011, 29, 397–416. [Google Scholar] [CrossRef]
- National Census of Fatal Occupational Injuries in 2015, Bureau of Labor Statistics. 2016. Available online: https://www.bls.gov/news.release/archives/cfoi_12162016.pdf (accessed on 18 August 2020).
- Chinda, T.; Pongsayaporn, P. Relationships among factors affecting construction safety equipment selection: Structural equation modelling approach. Civ. Eng. Environ. Syst. 2020, 37, 1–20. [Google Scholar] [CrossRef]
- Bureau of Labor Statistics (BLS). Fatal Work Injuries, by Industry and Contractor Adjusted Industry, by Selected Industry, 2012; Injuries, Illnesses, and Fatalities, U.S. Dept. of Labor: Washington, DC, USA, 2016. Available online: https://www.bls.gov/opub/mlr/2013/ (accessed on 18 August 2020).
- Li, R.Y.M.; Poon, S.W. Workers’ compensation for non-fatal construction accidents: Review of Hong Kong court cases. Asian Soc. Sci. 2009, 5, 15–24. [Google Scholar] [CrossRef]
- European Statistical Office. Accidents at Work Statistics. Luxembourg: European Commission DG Employment, Social Affairs and Equal Opportunities. 2015. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php/Accidents_at_work_statistics (accessed on 18 August 2020).
- Lehtola, M.M.; Van Der Molen, H.F.; Lappalainen, J.; Hoonakker, P.L.T.; Hsiao, H.; Haslam, R.A.; Hale, A.R.; Verbeek, J.H. The effectiveness of interventions for preventing injuries in the construction industry: A systematic review. Am. J. Prev. Med. 2008, 35, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Duarte, M.; Freitas, S.M. Revision of posturography based on force plate for balance evaluation. Rev. Bras. Fisioter. 2010, 14, 183–192. [Google Scholar] [CrossRef]
- Koepp, G.A.; Snedden, B.J.; Levine, J.A. Workplace slip, trip and fall injuries and obesity. Ergonomics 2015, 58, 674–679. [Google Scholar] [CrossRef]
- Tao, G.; Khan, A.Z.; Blohm, G. Corrective response times in a coordinated eye-head-arm countermanding task. J. Neurophysiol. 2018, 119, 2036–2051. [Google Scholar] [CrossRef]
- Töllner, T.; Rangelov, D.; Müller, H.J. How the speed of motor-response decisions, but not focal-attentional selection, differs as a function of task set and target prevalence. Proc. Natl. Acad. Sci. USA 2012, 109, 1990–1999. [Google Scholar] [CrossRef]
- Young, W.R.; Williams, A.M. How fear of falling can increase fall-risk in older adults: Applying psychological theory to practical observations. Gait Posture 2015, 41, 7–12. [Google Scholar] [CrossRef]
- Sawicki, M.; Szóstak, M. Quantitative Assessment of the State of Threat of Working on Construction Scaffolding. Int. J. Environ. Res. Public Health 2020, 17, 5773. [Google Scholar] [CrossRef]
- Chang, F.L.; Sun, Y.M.; Chuang, K.H.; Hsu, F.W. Work fatigue and physiological symptoms in different occupations of high-elevation construction workers. Appl. Ergon. 2009, 40, 591–596. [Google Scholar] [CrossRef] [PubMed]
- Davis, J.R.; Campbell, A.D.; Adkin, A.L.; Carpenter, M.G. The relationship between fear of falling and human postural control. Gait Posture 2009, 29, 275–279. [Google Scholar] [CrossRef] [PubMed]
- Hauck, L.J.; Carpenter, M.G.; Frank, J.S. Task-specific measures of balance efficacy, anxiety, and stability and their relationship to clinical balance performance. Gait Posture 2008, 27, 676–682. [Google Scholar] [CrossRef] [PubMed]
- Huffman, J.L.; Horslen, B.C.; Carpenter, M.G.; Adkin, A.L. Does increased postural threat lead to more conscious control of posture? Gait Posture 2009, 30, 528–532. [Google Scholar] [CrossRef] [PubMed]
- Orrell, A.J.; Masters, R.S.; Eves, F.F. Reinvestment and movement disruption following stroke. Neurorehabilit. Neural Repair 2009, 23, 177–183. [Google Scholar] [CrossRef] [PubMed]
- Habibnezhada, M.; Puckett, J.; Jebelli, H.; Karji, A.; Fardhosseini, M.S.; Asadi, S. Neurophysiological testing for assessing construction workers’ task performance at virtual height. Autom. Constr. 2020, 113, 103143. [Google Scholar] [CrossRef]
- Boucher, L.; Stuphorn, V.; Logan, G.D.; Schall, J.D.; Palmeri, T.J. Stopping eye and hand movements: Are the processes independent? Percept Psychophys. 2007, 69, 785–801. [Google Scholar] [CrossRef]
- Zaback, M.; Adkin, A.L.; Carpenter, M.G. Adaptation of emotional state and standing balance parameters following repeated exposure to height-induced postural threat. Sci. Rep. 2019, 9, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Sturnieks, D.L.; Delbaere, K.; Brodie, M.A.; Lord, S.R. The influence of age, anxiety and concern about falling on postural sway when standing at an elevated level. Hum. Mov. Sci. 2016, 49, 206–215. [Google Scholar] [CrossRef] [PubMed]
- Zamysłowska-Szmytke, E.; Śliwińska-Kowalska, M. Studies of the balance system for the needs of occupational medicine. Otorhinolaryngology 2012, 11, 139–145. [Google Scholar]
- Adkin, A.L.; Frank, J.S.; Carpenter, M.G.; Peysar, G.W. Postural control is scaled to level of postural threat. Gait Posture 2000, 12, 87–93. [Google Scholar] [CrossRef]
- Vuillerme, N.; Nafati, G. How attentional focus on body sway affects postural control during quiet standing. Psychol. Res. 2007, 71, 192–200. [Google Scholar] [CrossRef] [PubMed]
- Gatti, G.C.; Schneider, S.; Migliaccio, G.C. Physiological condition monitoring of construction workers. Autom. Constr. 2014, 44, 227–233. [Google Scholar] [CrossRef]
- Min, S.N.; Kim, J.Y.; Parnianpour, M. The effects of safety handrails and the heights of scaffolds on the subjective and objective evaluation of postural stability and cardiovascular stress in novice and expert construction workers. Appl. Ergon. 2012, 43, 574–581. [Google Scholar] [CrossRef] [PubMed]
- Chander, H.; Shojaei, A.; Deb, S.; Kodithuwakku Arachchige, S.N.K.; Hudson, C.; Knight, A.C.; Carruth, D.W. Impact of Virtual Reality–Generated Construction Environments at Different Heights on Postural Stability and Fall Risk. Workplace Health Saf. 2020, 19. [Google Scholar] [CrossRef]
- Yiou, E.; Deroche, T.; Do, M.C.; Woodman, T. Influence of fear of falling on anticipatory postural control of medio-lateral stability during rapid leg flexion. Eur. J. Appl. Physiol. 2011, 111, 611–620. [Google Scholar] [CrossRef]
- Johnson, K.J.; Zaback, M.; Tokuno, C.; Adkin, A.L.; Carpenter, M.G. Repeated exposure to the threat of perturbation induces emotional, cognitive, and postural adaptations in young and older adults. Exp. Gerontol. 2019, 15, 109–115. [Google Scholar] [CrossRef]
- Adkin, A.L.; Carpenter, M.G. New insights on emotional contributions to human postural control. Front. Neurol. 2018, 9, 789. [Google Scholar] [CrossRef]
- Zaback, M.; Cleworth, T.W.; Carpenter, M.G.; Adkin, A.L. Personality traits and individual diferences predict threat-induced changes in postural control. Hum. Mov. Sci. 2015, 40, 393–409. [Google Scholar] [CrossRef]
- Sample, R.B.; Jackson, K.; Kinney, A.L.; Diestelkamp, W.S.; Reinert, S.S.; Bigelow, K.E. Manual and cognitive dual tasks contribute to fall-risk differentiation in posturography measures. J. Appl. Biomech. 2016, 32, 541–547. [Google Scholar] [CrossRef]
- Stephan, D.N.; Hensen, S.; Fintor, E.; Krampe, R.; Koch, I. Influences of Postural Control on Cognitive Control in Task Switching. Front. Psychol. 2018, 9, 1153. [Google Scholar] [CrossRef] [PubMed]
- Cullen, R.H.; Agnew, M.J. Comparing different measures of overall workload in a multimodal postural/auditory dual-task environment. J. IIE Trans. Occup. Ergon. Hum. Factors 2016, 4, 2–3. [Google Scholar] [CrossRef]
- Schnittjer, A.J. The Effects of a Cognitive Dual Task on Jump-Landing Mechanics. A Thesis Presented to the Faculty of the College of Health Sciences and Professions of Ohio University. 2017. Available online: http://rave.ohiolink.edu/etdc/view?acc_num=ohiou1491425508104132 (accessed on 18 August 2020).
- Siu, K.C.; Woollacott, M.H. Attentional demands of postural control: The ability to selectively allocate information-processing resources. Gait Posture 2007, 25, 121–126. [Google Scholar] [CrossRef] [PubMed]
- Cyma, M.; Marciniak, K.; Tomczak, M.; Stemplewski, R. Postural stability and physical activity of workers working at height. Am. J. Men’s Health 2018, 12, 1068–1073. [Google Scholar] [CrossRef] [PubMed]
- Umer, W.; Li, H.; Lu, W.; Szeto, G.P.Y.; Wong, A.Y.L. Development of a tool to monitor static balance of construction workers for proactive fall safety management. Autom. Constr. 2018, 94, 438–448. [Google Scholar] [CrossRef]
- Willmann, M.; Langlet, C.; Hainaut, J.P.; Benoit, B. The time course of autonomic parameters and muscle tension during recovery following a moderate cognitive stressor: Dependency on trait anxiety level. Int. J. Psychophysiol. 2012, 84, 51–58. [Google Scholar] [CrossRef]
- Zaback, M.; Carpenter, M.G.; Adkin, A.L. Threat-induced changes in attention during tests of static and anticipatory postural control. Gait Posture 2016, 45, 19–24. [Google Scholar] [CrossRef]
- Huweler, R.; Kandil, F.I.; Alpers, G.W.; Gerlach, A.L. The impact of visual flow stimulation on anxiety, dizziness, and body sway in individuals with and without fear of heights. Behav. Res. Ther. 2009, 47, 345–352. [Google Scholar] [CrossRef]
- Redfern, M.S.; Yardley, L.; Bronstein, A.M. Visual influences on balance. J. Anxiety Disord. 2001, 15, 81–94. [Google Scholar] [CrossRef]
- World Medical Association. World Medical Association Declaration of Helsinki Ethical Principles for Medical Research Involving Human Subjects. J. Am. Med. Assoc. 2013, 310, 2191–2194. [Google Scholar] [CrossRef]
- Stemplewski, R.; Maciaszek, J.; Salamon, A.; Tomczak, M.; Osiński, W. Effect of moderate physical exercise on postural control among 65–74 years old men. Arch. Gerontol. Geriatr. 2012, 54, 279–283. [Google Scholar] [CrossRef] [PubMed]
- Pinsault, N.; Vuillerme, N. Test-retest reliability of centre of foot pressure measures to assess postural control during unperturbed stance. Med. Eng. Phys. 2009, 31, 276–286. [Google Scholar] [CrossRef] [PubMed]
- Prioli, A.C.; Freitas Júnior, P.B.; Barela, J.A. Physical Activity and Postural Control in the Elderly: Coupling between Visual Information and Body Sway. Gerontology 2005, 51, 145–148. [Google Scholar] [CrossRef] [PubMed]
- Punakallio, A. Balance Abilities of Different—Aged Workers in Physically Demanding Jobs. J. Occup. Rehabil. 2003, 13, 33–43. [Google Scholar] [CrossRef] [PubMed]
- Ballor, D.L.; Burke, L.M.; Knudson, D.V.; Olson, J.R.; Montoye, H.J. Comparison of three methods of estimating energy expenditure: Caltrac, heart rate and video analysis. Res. Q. Exerc. Sport 1989, 60, 362–368. [Google Scholar] [CrossRef] [PubMed]
- Bray, M.S.; Wong, W.W.; Morrow, J.R.; Butte, N.F.; Pivarnik, J.M. Caltrac versus calorimeter determination of 24-h energy expenditure in female children and adolescents. Med. Sci. Sports Exerc. 1994, 26, 1524–1530. [Google Scholar] [CrossRef]
- Błaszczyk, J. Sway ratio: A new measure for quantifying postural stability. Acta Neurobiol. Exp. 2008, 68, 51–57. [Google Scholar]
- Ruhe, A.; Fejer, R.; Walker, B. The test-retest reliability of centre of pressure measures in bipedal static task conditions: A systematic review of the literature. Gait Posture 2010, 32, 436–445. [Google Scholar] [CrossRef]
- Bizid, R.; Margnes, E.; François, Y.; Jully, J.; Gonzalez, G.; Dupui, P.; Paillard, T. Effects of knee and ankle muscle fatigue on postural control in the unipedal stance. Eur. J. Appl. Physiol. 2009, 106, 375–380. [Google Scholar] [CrossRef]
- Malik, M. Heart Rate Variability: Standards of measurement, physiological interpretation, and clinical use. Eur. Heart J. 1996, 17, 354–381. [Google Scholar] [CrossRef]
- Sandercock, G.R.H.; Bromley, D.P.; Brodie, D.A. The reliability of short-term measurements of heart rate variability. Int. J. Cardiol. 2005, 103, 238–247. [Google Scholar] [CrossRef]
- McCraty, R.; Shaffer, F. Heart Rate Variability: New Perspectives on Physiological Mechanisms, Assessment of Self-regulatory Capacity, and Health risk. Clin. Med. Surg. 2015, 4, 46–61. [Google Scholar] [CrossRef]
- Cleworth, T.W.; Carpenter, M.G. Postural threat influences conscious perception of postural sway. Neurosci. Lett. 2016, 620, 127–131. [Google Scholar] [CrossRef] [PubMed]
- Yang, K.; Ahn, C.R.; Vuran, M.C.; Kim, H. Collective sensing of workers’ gait patterns to identify fall hazards in construction. Autom. Constr. 2017, 82, 166–178. [Google Scholar] [CrossRef]
- DiDomenico, A.; McGorry, R.; Huang, Y.; Blair, M. Perceptions of postural stability after transitioning to standing among construction workers. Saf. Sci. 2010, 48, 166–172. [Google Scholar] [CrossRef]
- Davis, J.R.; Horslen, B.C.; Nishikawa, K.; Fukushima, K.; Chua, R.; Inglis, J.T.; Carpenter, M.G. Human proprioceptive adaptations during states of height-induced postural fear and anxiety. J. Neurophysiol. 2011, 106, 3082–3090. [Google Scholar] [CrossRef]
- Sibley, K.M.; Mochizuki, G.; Frank, J.S.; McIlroy, W.E. The relationship between physiological arousal and cortical and autonomic responses to postural instability. Exp. Brain Res. 2010, 203, 533–540. [Google Scholar] [CrossRef]
- Hainaut, J.P.; Caillet, G.; Lestienne, F.G.; Bolmont, B. The role of trait anxiety on static balance performance in control and anxiogenic situations. Gait Posture 2011, 33, 604–608. [Google Scholar] [CrossRef]
- Salassa, J.R.; Zapala, D.A. Love and fear of heights: The pathophysiology and psychology of height imbalance. Wilderness Environ. Med. 2009, 20, 378–382. [Google Scholar] [CrossRef]
- Horak, F. Postural orientation and equilibrium: What do we need to know about neural control of balance to prevent falls. Age Ageing 2006, 35, 7–11. [Google Scholar] [CrossRef]
- Redfern, M.S.; Furman, J.M.; Jacob, R.G. Visually induced postural sway in anxiety disorders. J. Anxiety Disord. 2007, 21, 704–716. [Google Scholar] [CrossRef] [PubMed]
- Pellecchia, G.L. Postural sway increases with attentional demands of concurrent cognitive task. Gait Posture 2003, 18, 29–34. [Google Scholar] [CrossRef]
- Jebelli, H.; Ahn, C.R.; Stentz, T.L. Fall risk analysis of construction workers using inertial measurement units: Validating the usefulness of the postural stability metrics in construction. Saf. Sci. 2015, 84, 161–170. [Google Scholar] [CrossRef]
- Kaskutas, V.; Dale, A.M.; Nolan, J.; Patterson, D.; Lipscomb, H.J.; Evanoff, B. Fall hazard control observed on residential construction sites. Am. J. Ind. Med. 2009, 52, 491–499. [Google Scholar] [CrossRef] [PubMed]
- Hsu, F.W.; Lin, C.J.; Lee, Y.H.; Chen, H.J. Effects of elevation change on mental stress in high-voltage transmission tower construction workers. Appl. Ergon. 2016, 56, 101–107. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | M (sd) HW | M (sd) OW | t df = 30 | p |
|---|---|---|---|---|
| Age [years] | 34.5(7.49) | 36.00(6.31) | −0.61 | 0.54 |
| Body height (m) | 1.82(0.05) | 1.79(0.08) | 1.25 | 0.22 |
| Body weight (kg) | 90.5(9.94) | 83.5(13.34) | 1.69 | 0.23 |
| BMI [kg/m2] | 27.31(2.59) | 26.01(3.41) | 1.21 | 0.23 |
| PA [cals used/wk] | 21918.94 (2962.42) | 19694.56 (4178.72) | 1.74 | 0.09 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cyma-Wejchenig, M.; Maciaszek, J.; Marciniak, K.; Stemplewski, R. The Effects of Cognitive Task and Change of Height on Postural Stability and Cardiovascular Stress in Workers Working at Height. Int. J. Environ. Res. Public Health 2020, 17, 6541. https://doi.org/10.3390/ijerph17186541
Cyma-Wejchenig M, Maciaszek J, Marciniak K, Stemplewski R. The Effects of Cognitive Task and Change of Height on Postural Stability and Cardiovascular Stress in Workers Working at Height. International Journal of Environmental Research and Public Health. 2020; 17(18):6541. https://doi.org/10.3390/ijerph17186541
Chicago/Turabian StyleCyma-Wejchenig, Magdalena, Janusz Maciaszek, Katarzyna Marciniak, and Rafał Stemplewski. 2020. "The Effects of Cognitive Task and Change of Height on Postural Stability and Cardiovascular Stress in Workers Working at Height" International Journal of Environmental Research and Public Health 17, no. 18: 6541. https://doi.org/10.3390/ijerph17186541
APA StyleCyma-Wejchenig, M., Maciaszek, J., Marciniak, K., & Stemplewski, R. (2020). The Effects of Cognitive Task and Change of Height on Postural Stability and Cardiovascular Stress in Workers Working at Height. International Journal of Environmental Research and Public Health, 17(18), 6541. https://doi.org/10.3390/ijerph17186541