A Systematic Review of the Health and Healthcare Inequalities for People with Intersex Variance


Abstract
1. Introduction
1.1. Intersex Variance
1.2. Intersex Healthcare
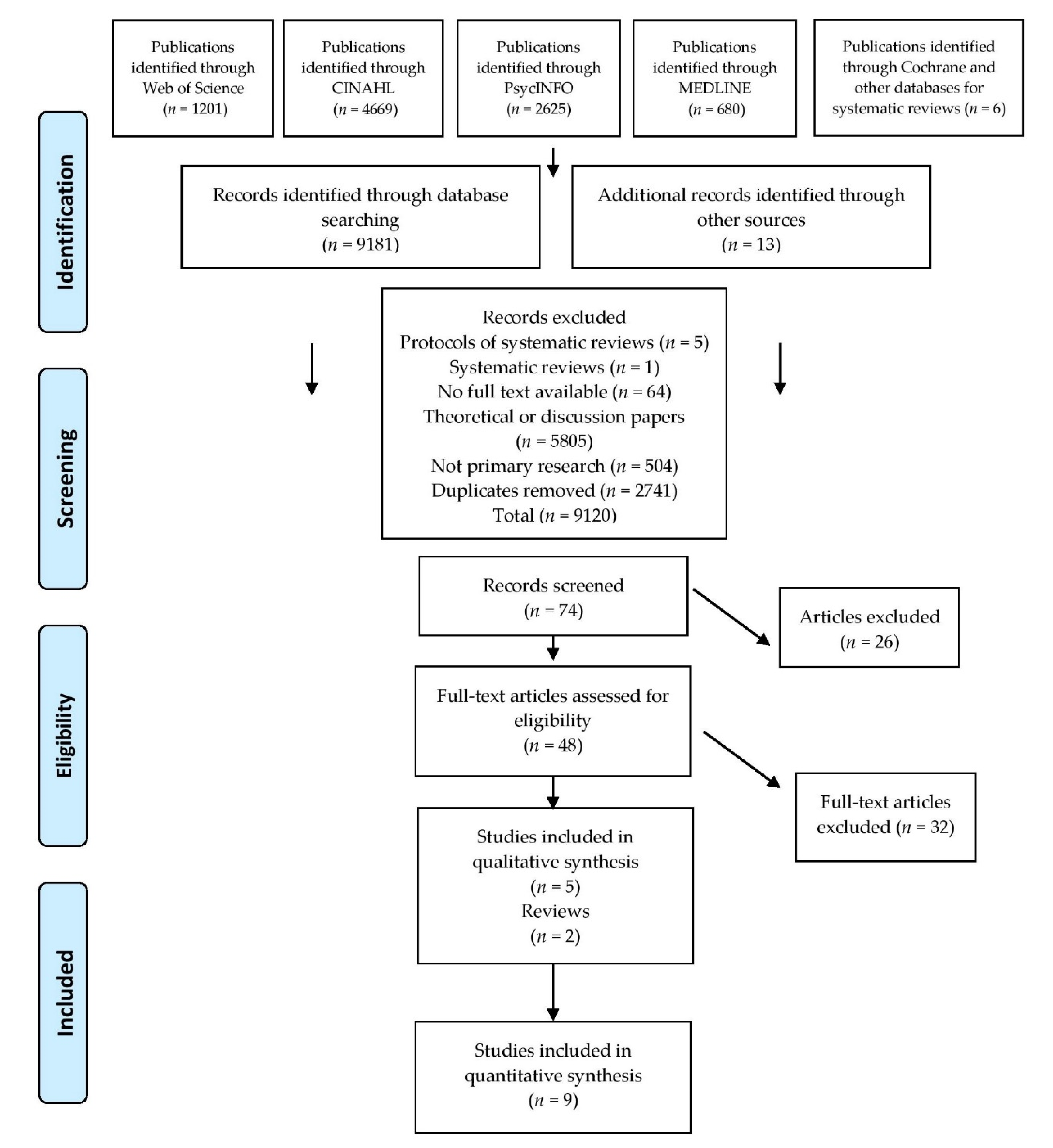
2. Methods
2.1. Search Strategy
2.2. Inclusion Criteria
2.3. Key Search Terms
2.4. Data Extraction
2.5. Synthesis
3. Results
3.1. Mental Health
3.2. Assigned Sex
3.3. Gender Identity
3.4. Healthcare
3.5. Surgery
3.6. Health Professionals
… nature has decided (tapping the table) that there should be a female and a male and when they are together then you can have a baby, yes? There is a God and he decided that it should be this way. With human beings and with all animals it’s the same: there are female and male animals.[42] (Prof. K., 29 October 2015 in Meoded Danon 2019 p. 150).
…First, when these children are born, they have genitalia that are neither male nor female, and society cannot accept this. This family seems bizarre to society. How will they put him in a kindergarten? Second, from a technical point of view, healing is faster, and there is a great advantage in doing these operations at a young age. Third, psychologically, a girl [in this case] also has to grow up knowing that she is more or less normal. She will grow up with female genitalia and not some intermediate thing that appears to be something more masculine. So, the goal is to fix these children between the age of six months and a year. This is the optimum age.(Prof B., 25 Oct 2015 in Meoded Danon [42] p. 156).
I say what I always say, which is ‘we are happy that your child is healthy. We don’t need to do anything. Everything is fine. Look at your beautiful child’. I will say this several times, so it is clear that there is no deal [no rush to do anything] now. So they will not do anything, I tell them what I think is most important so they can connect to their child.(Dr. E., 28 November 2015 in Meoded Danon [42], p. 155).
We really want to avoid early operations. We seriously spend a lot of time talking about the need to open our minds to the fact that we have more than two “drawers”, boys or girls, that it is a task for society to see the whole spectrum, that it is a challenge for the family to understand that this child is special and that we should wait until the child is able to express an opinion with his own voice. So regarding everything that has to do with correcting the genitalia we are very, very, very careful.(Dr. M., 8 April, 2016 in Meoded Danon [42], p. 155).
3.7. Accessing Healthcare
3.8. Parenting
3.9. Age
3.10. Social Factors
It’s hard for people like me to get a steady functional intimate relationship. Because if you think about it you’ve got your medical problems to explain for one and a lot of people these days are only out for one thing (sex) and you can’t just tell everyone that you can’t, things get round too fast. You have got to be careful. Everyone says you can have a decent life without a relationship, I don’t think that’s true. I’m sure there is, [someone like me] somewhere out there but I wouldn’t even speak to them about it all, because it’s just too awkward(a young woman in Sanders et al. [34], p. 1909).
4. Discussion
4.1. Summary of Findings
4.2. Strengths and Limitations of the Review
4.3. Implications for Research
- How meanings or understandings of intersex subjectivity and embodiment materialise as multi-layered forms of interdependence via health assemblages.
- How to achieve dynamic systems change via disruption of biomedical linguistic essentialism (as seen in ‘DSD’ diagnoses), whilst questioning sex and gender normativity in healthcare.
- What these forms of resistance might look like.
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Zeeman, L.; Sherriff, N.; Browne, K.; McGlynn, N.; Mirandola, M.; Gios, L.; Davis, R.; Sanchez-Lambert, J.; Aujean, S.; Pinto, N.; et al. A review of lesbian, gay, bisexual, trans and intersex (LGBTI) health and healthcare inequalities. Eur. J. Public Health 2019, 29, 974–980. [Google Scholar] [CrossRef] [PubMed]
- Sherriff, N.; Zeeman, L.; McGlynn, N.; Pinto, N.; Hugendubel, K.; Mirandola, M.; Gios, L.; Davis, R.; Donisi, V.; Farinella, F.; et al. Co-producing knowledge of lesbian, gay, bisexual, trans and intersex (LGBTI) health-care inequalities via rapid reviews of grey literature in 27 EU Member States. Health Expect. 2019, 22, 688–700. [Google Scholar] [CrossRef] [PubMed]
- Blondeel, K.; Say, L.; Chou, D.; Toskin, I.; Khosla, R.; Scolaro, E.; Temmerman, M. Evidence and knowledge gaps on the disease burden in sexual and gender minorities: A review of systematic reviews. Int. J. Equity Health 2016, 15, 1–9. [Google Scholar] [CrossRef]
- Jones, T. Intersex Studies: A systematic review of international health literature. SAGE Open 2018, 8, 2158244017745577. [Google Scholar] [CrossRef]
- Reisner, S.; Poteat, T.; Keatley, J.; Cabral, M.; Mothopeng, T.; Dunham, E.; Holland, C.; Max, R.; Baral, S. Global health burden and needs of transgender populations: A review. Lancet 2016, 388, 412–436. [Google Scholar] [CrossRef]
- Meads, C.; Hunt, R.; Martin, A.; Varney, J. A systematic review of sexual minority women’s experiences of health care in the UK. Int. J. Environ. Res. Public Health 2019, 16, 3032. [Google Scholar] [CrossRef]
- Fish, J.; Weis, C. All the lonely people, where do they all belong? An interpretive synthesis of loneliness and social support in older lesbian, gay and bisexual communities. Qual. Ageing Older Adults 2019, 20. [Google Scholar] [CrossRef]
- Zeeman, L.; Sherriff, N.S.; Browne, K.; McGlynn, N.; Aujean, S.; Pinto, N.; Davis, R.; Mirandola, M.; Gios, L.; Amaddeo, F.; et al. Scientific Review: A Review of Health Inequalities Experienced by LGBTI People and the Barriers Faced by Health Professionals in Providing Healthcare for LGBTI People; European Union: Luxembourg, 2017; Available online: https://ec.europa.eu/health/social_determinants/projects/ep_funded_projects_en#fragment2 (accessed on 18 July 2020).
- McGlynn, N.; Browne, K.; Sherriff, N.; Zeeman, L.; Mirandola, M.; Gios, L.; Davis, R.; Donisi, V.; Farinella, F.; Rosińska, M.; et al. Healthcare professionals’ assumptions as barriers to LGBTI healthcare. Cult. Health Sex. 2020, 22, 954–970. [Google Scholar] [CrossRef]
- Fish, J.; Williamson, I. Exploring lesbian, gay and bisexual patients’ accounts of their experiences of cancer care in the UK. Eur. J. Cancer Care 2016, 10, 1–13. [Google Scholar] [CrossRef]
- Whitehead, J.; Shaver, J.; Stephenson, R. Outness, Stigma, and Primary Health Care Utilization among Rural LGBT Populations. PLoS ONE 2016, 11, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Budge, S.L.; Adelson, J.L.; Howard, K.A.S. Anxiety and depression in transgender individuals: The roles of transition status, loss, social support, and coping. J. Consult. Clin. Psychol. 2013, 81, 545–557. [Google Scholar] [CrossRef]
- Jones, T. Improving Services for Transgender and Gender Variant Youth: Research, Policy and Practice for Health and Social Care Professionals; Jessica Kingsley Publishers: London, UK, 2019. [Google Scholar]
- Zeeman, L.; Sherriff, N.S.; Aujean, S.; Pinto, N.; Browne, K.; McGlynn, N.; Davis, R.; Mirandola, M.; Gios, L.; Amaddeo, F.; et al. Comprehensive Scoping Report: A Review of the European Grey Literature on Health Inequalities Experienced by LGBTI People and the Barriers Faced by Health Professionals in Providing Healthcare for LGBTI People; European Union: Luxembourg, 2017; Available online: https://ec.europa.eu/health/social_determinants/projects/ep_funded_projects_en#fragment2 (accessed on 13 July 2020).
- Carroll, L. Intersex. In Youth, Education and Sexualities: An International Encyclopedia; Sears, J.T., Ed.; Greenwood Press: Westport, CT, USA, 2005; Volume 1, pp. 440–444. [Google Scholar]
- Fausto-Sterling, A. Sexing the Body: Gender Politics and the Construction of Sexuality; Basic Books: New York, NY, USA, 2000. [Google Scholar]
- Fausto-Sterling, A. The five sexes: Why male and female are not enough. Sciences 1993, 33, 20–24. [Google Scholar] [CrossRef]
- Köhler, B.; Kleinemeier, E.; Lux, A.; Hiort, O.; Grüters, A.; Thyen, U. Satisfaction with genital surgery and sexual life of adults with XY disorders of sex development: Results from the German clinical evaluation study. J. Clin. Endocrinol. Metab. 2012, 97, 577–588. [Google Scholar] [CrossRef] [PubMed]
- Ainsworth, C. Sex redefined. Nature 2015, 518, 288–291. [Google Scholar] [CrossRef] [PubMed]
- Thyen, U.; Lux, A.; Jürgensen, M.; Hiort, O.; Köhler, B. Utilization of health care services and satisfaction with care in adults affected by disorders of sex development (DSD). J. Gen. Intern. Med. 2014, 29, 752–759. [Google Scholar] [CrossRef] [PubMed]
- Roen, K. Intersex or Diverse Sex Development: Critical Review of Psychosocial Health Care Research and Indications for Practice. J. Sex. Res. 2019, 56, 511–528. [Google Scholar] [CrossRef]
- Malatino, H. Queer Embodiment: Monstrosity, Medical Violence and Intersex Experience; University of Nebraska Press: Lincoln, NE, USA, 2019. [Google Scholar]
- Warne, G.; Raza, J. Disorders of sex development (DSDs), their presentation and management in different cultures. Rev. Endocr. Metab. Disord. 2008, 9, 227–236. [Google Scholar] [CrossRef]
- Holmes, M. Critical Intersex; Routledge: London, UK, 2009. [Google Scholar]
- Pagonis, P. The son they never had. Narrat. Inq. Bioeth. 2015, 5, 103–106. [Google Scholar] [CrossRef] [PubMed]
- Hughes, I.A. Disorders of sex development: A new definition and classification. Best Pract. Res. Clin. Endocrinol. Metab. 2008, 22, 119–134. [Google Scholar] [CrossRef]
- Davis, G. The power in a name: Diagnostic terminology and diverse experiences. Psychol. Sex. 2014, 5, 15–27. [Google Scholar] [CrossRef]
- Rubin, D.A. Provincializing Intersex: US Intersex Activism, Human Rights, and Transnational Body Politics. Front. A J. Women Stud. 2015, 36, 51–83. [Google Scholar] [CrossRef]
- Rubin, D.A. “An Unnamed Blank That Craved a Name”: A Genealogy of Intersex as Gender. Signs 2012, 37, 883–908. [Google Scholar] [CrossRef]
- United Nations. Born Free and Equal: Sexual Orientation and Gender Identity in International Human Rights Law; United Nations Human Rights Office of the High Commissioner: Geneva, Switzerland, 2012; Available online: https://www.ohchr.org/Documents/Publications/BornFreeAndEqualLowRes.pdf (accessed on 14 August 2020).
- Meoded Danon, L. Time matters for intersex bodies: Between socio-medical time and somatic time. Soc. Sci. Med. 2018, 208, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Jones, T. The needs of students with intersex variations. Sex Educ. 2016, 16, 602–618. [Google Scholar] [CrossRef]
- Ojanen, T.T.; Burford, J.; Juntrasook, A.; Kongsup, A.; Assatarakul, T.; Chaiyajit, N. Intersections of lgbti exclusion and discrimination in Thailand: The role of socio-economic status. Sex. Res. Soc. Policy 2019, 16, 529–542. [Google Scholar] [CrossRef]
- Sanders, C.; Carter, B.; Lwin, R. Young women with a disorder of sex development: Learning to share information with health professionals, friends and intimate partners about bodily differences and infertility. J. Adv. Nurs. 2015, 71, 1904–1913. [Google Scholar] [CrossRef]
- Bennecke, E.; Werner-Rosen, K.; Thyen, U.; Kleinemeier, E.; Lux, A.; Jurgensen, M.; Gruters, A.; Kohler, B. Subjective need for psychological support (PsySupp) in parents of children and adolescents with disorders of sex development (dsd). Eur. J. Pediatri. 2015, 174, 1287–1297. [Google Scholar] [CrossRef]
- Berglund, A.; Johannsen, T.H.; Stochholm, K.; Viuff, M.H.; Fedder, J.; Main, K.M.; Gravholt, C.H. Morbidity, mortality, and socioeconomics in females with 46,XY disorders of sex development: A Nationwide Study. J. Clin. Endocrinol. Metab. 2018, 103, 1418–1428. [Google Scholar] [CrossRef]
- D’Alberton, F.; Assante, M.T.; Foresti, M.; Balsamo, A.; Bertelloni, S.; Dati, E.; Nardi, L.; Bacchi, M.L.; Mazzanti, L. Quality of Life and Psychological Adjustment of Women Living with 46,XY Differences of Sex Development. J. Sex. Med. 2015, 12, 1440–1449. [Google Scholar] [CrossRef]
- Hughes, M. Health and well being of lesbian, gay, bisexual, transgender and intersex people aged 50 years and over. Aust. Health Rev. 2018, 42, 146–151. [Google Scholar] [CrossRef]
- Jürgensen, M.; Kleinemeier, E.; Lux, A.; Steensma, T.D.; Cohen-Kettenis, P.T.; Hiort, O.; Thyen, U.; Köhler, B. Psychosexual development in adolescents and adults with disorders of sex development-results from the German clinical evaluation dtudy: Psychosexual Development in Adolescents and Adults with DSD. J. Sex. Med. 2013, 10, 2703–2714. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Tian, Q. The Investigation of Quality of Life in 87 Chinese Patients with Disorders of Sex Development. BioMed. Res. Int. 2015, 2015, 342420. [Google Scholar] [CrossRef] [PubMed]
- Schweizer, K.; Brunner, F.; Handford, C.; Richter-Appelt, H. Gender experience and satisfaction with gender allocation in adults with diverse intersex conditions (divergences of sex development, DSD). Psychol. Sex. 2014, 5, 56–82. [Google Scholar] [CrossRef]
- Meoded Danon, L. Comparing contemporary medical treatment practices aimed at intersex/DSD bodies in Israel and Germany. Sociol. Health Illn. 2019, 41, 143–164. [Google Scholar] [CrossRef]
- Jürgensen, M.; Lux, A.; Wien, S.B.; Kleinemeier, E.; Hiort, O.; Thyen, U. Health-related quality of life in children with disorders of sex development (DSD). Eur. J. Pediatr. 2014, 173, 893–903. [Google Scholar] [CrossRef]
- Tinney, J.; Dow, B.; Maude, P.; Purchase, R.; Whyte, C.; Barrett, C. Mental health issues and discrimination among older LGBTI people. Int. Psychogeriatr. 2015, 27, 1411–1416. [Google Scholar] [CrossRef]
- Westwood, S.; Willis, P.; Fish, J.; Hafford-Letchfield, T.; Semlyen, J.; King, A.; Beach, B.; Almack, K.; Kneale, D.; Toze, M.; et al. Older LGBT+ health inequalities in the UK: Setting a research agenda. J. Epidemiol. Community Health 2020, 74, 408–411. [Google Scholar] [CrossRef]
- Andrews, G.J.; Duff, C. Matter Beginning to Matter: On Posthumanist Understandings of the Vital Emergence of Health. Soc. Sci. Med. 2019, 226, 123–134. [Google Scholar] [CrossRef]
- NIHR INVOLVE. Guidance on Co-Producing a Research Project. 2018. Available online: www.involve.nihr.ac.uk (accessed on 14 August 2020).
- Palmer, V.; Weavell, W.; Callander, R.; Piper, D.; Maher, R.; Boyd, H.; Herrman, H.; Furler, J.; Gunn, J.; Iedema, R. The participatory zeitgeist: An explanatory theoretical model of change in an era of coproduction and codesign in healthcare improvement. Med. Humanit. 2019, 45, 247–257. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Authors, Year | Country | Design | Population | Participant Numbers | Outcome of Interest |
|---|---|---|---|---|---|
| Bennecke et al., 2015 | Germany, Austria and Switzerland | Multicentre clinical evaluation with ‘dsd’ questionnaire and SPSS statistical analysis | Young people diagnosed with ‘dsd-XX or XY without (c) or with partial (p) androgen effects, and female (f) or male (m) sex of rearing: dsd-XX-p-f, dsd- XY-p-f, dsd-XY-p-m and dsd-XY-c-f. | children and adolescents (n = 329) and parents (n = 110) | (1) Parents of children with ‘dsd’ have a significant need for psychological support. (2) Half of parents did not receive support. (3) Support should be part of multidisciplinary care of parents to reduce their fears of stigmatisation and to discuss gender issues, hormonal treatment and surgery of their child. |
| Berglund et al., 2018 | Denmark | Nationwide registry study with random selection of participants and a control cohort with statistical analysis | 46,XY females with Androgen insensitivity (AIS), GD, 17α -OHD, 17beta-HSD, WT-1 and Star mutation | XY females (n = 123), with a control cohort of females (n = 12,300) and males (n = 12,300) from the general population | (1) Mortality and education were similar to controls. (2) Cohabitation and motherhood were reduced for XY females compared to the controls. (3) Income and performance in the labour market were higher amongst in XY females later in life compared to the general population. |
| D’Alberton et al., 2015 | Italian | Cross-sectional study with standardised (ABCL, WHOQOL) questionnaires | 46,XY females with ‘dsd’ with AIS, Gonadal dysgenesis, 5α -reductase deficiency, Leydig cell hypoplasia | (n = 43) aged 18–57 years | (1) Statistically higher scores than the comparison group for depression, anxiety, internalising and externalising problems. (2) Younger people were more likely to access psychological support. (3) Lower psychological distress in younger women could indicate positive outcomes of changes in management. |
| Davis 2014 | USA | In-depth individual interviews standpoint feminist analysis | Individuals with intersex traits | (n = 37) | (1) ‘dsd’ terminology is received and utilised in different ways, embraced by some and refuted by other participants. (2) Self-understanding might conflict with the ‘dsd’ terminology ascribed in the 1990s. |
| Meoded Danon 2018 | Israel and Germany | Narrative interviews | People with intersex variations, medical professionals, parents | Total (n = 62) German adults with intersex variations (n = 4), parents (n = 4), professionals (n = 18); and Israeli adults with intersex variations (n = 15), professionals (n = 34), parents (n = 11) | (1) Health professional expressed range of views regarding people with intersex variance, sex as a spectrum, treatment options and whether intervention is needed or not. (2) The importance of intersex children meeting each other for support. (3) Legal reform can help prevent unnecessary surgery on minors with intersex variance. |
| Hughes 2018 | Australia | Survey (SF12 and with a Likert scale and Kessler 10) with statistical and bivariate analysis | LGBTI older people | LGBT people (n-312), older adult with intersex variance (n = 1) | (1) Though many older LGBTI people are well, both physically and mentally, they do appear to face increased risk of certain health issues compared with the general population such as loneliness and psychological distress. (2) Participants with intersex variation were underrepresented in the sample. |
| Jones 2016 | Australian | Survey with a descriptive comparative statistical analysis | People with intersex variations | People with intersex variance (n = 272) aged 16 to 87 years | (1) 42% of participants thought about self-harm on the basis of issues related to having an intersex variation (2) 26% had engaged in self-harm on the basis of having an intersex variation. (3) 60% had thought about suicide, and 19% had attempted suicide compared to under 3% for the general Australian population. |
| Jones 2018 | International | Systematic review of health literature via theoretical lenses | People with intersex variations | Studies published in 2015–2016 (n = 61) | (1) studies framing medical interventions as problematic (n = 27). (2) studies using a bioethical/narrative inquiry frame (n = 26). (3) Studies with clinical medical theoretical lens (n = 24). (4) Studies with a critical LGBTI liberationist theoretical lens (n = 4). |
| Jurgensen et al., 2013 | Germany, Austria, Switzerland | Questionnaire via interviews with statistical analysis | People with ‘dsd’ | Adolescents (n = 66) and adults (n = 110) | (1) Partnership and sexuality were identified as challenging areas of life. (2) Fewer experiences of peer, romantic or sexual relationships were reported compared to the general population. (3) 25% of adults with ‘dsd’ never had a love relationship and will benefit from support and counselling. |
| Köhler et al., 2012 | Germany, Austria, Switzerland | Evaluation via questionnaire with statistical analysis | Individuals with ‘46,XY,dsd’ | People with intersex variance (n = 57) aged 18–62 | (1) Constructive genital surgery should be minimised and only undertaken with informed consent mainly in adolescence or adulthood. (2) Multidisciplinary care and psychological support should include parents, peers and patient groups. |
| Ojanen et al., 2018 | Thailand | Life story interviews with thematic analysis | LGBTI people | A person with intersex variance (n = 1) | (1) Transgender and intersex participants reported more discrimination and exclusion compared to LGB people. (2) Lower socio-economic status of LGBTI people results in vulnerability. |
| Thyen et al., 2014 | Germany, Austria, Switzerland | Clinical evaluation via cross-sectional assessment with statistical analysis in SPSS | People with intersex variations | Adults with ‘dsd’ (n = 110) | (1) People with intersex variance should have access to mental health services as part of interdisciplinary care. (2) long-term follow-up should include measures of satisfaction with care and subjective psychosexual, emotional, and social well-being. |
| Sanders et al., 2015 | UK | Interpretive phenomenological analysis | Young people with intersex variations | Young women with ‘dsd’ aged 14–19 (n = 13) | (1) Young women may fear sharing personal information (2) Physical intimacy may require planning which has an impact on their perceived expectation of sexual spontaneity in a relationship. (3) For those who can’t have children meaning given to fertility change over time. |
| Schweizer et al., 2014 | Germany | Questionnaire, standardised scales, qualitative content and statistical analysis | People with intersex variations | Young people and adults with ‘dsd’ (n = 78) | (1) 24% of participants reported an inclusive two-gender/mixed identity and 3% neither male nor female gender identity. (2) Uncertainty of belonging to the female or male gender category as well as non-binary identifications highlight the need for alternative gender categories. |
| Wang and Tian 2015 | China | Case-control with SPSS statistical analysis | Patients with ‘dsd’ | People with ‘dsd’ (n = 87) aged 13–38 | (1) Only 13.7% of participants partook in sexual activity. (2) Quality of life of ‘dsd’ patients are not significantly lower compared to the urban Chinese population. |
| Zeeman et al., 2018 | International | Narrative synthesis of systematic reviews, meta-synthesis and primary research | LGBTI people | Studies of people with intersex variations (n = 8) published 2010–2016 | (1) A significant lack of research exists on the general health profile and healthcare experiences of intersex people. (2) Unessential corrective surgery on intersex minors to align their bodies to the male/female binary should only occur when the young person can provide informed consent. (3) Intersex variations are diagnosed biomedically which unnecessarily medicalises intersex people. (4) Male/female binary categories for sex markers and gender identify are not helpful as intersex bodies can be ‘trapped’ in these limiting categories. |
| No | Study | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Davis 2014 [27] | y | y | y | y | y | y | y | y | ct | y |
| 2 | Meoded Danon 2018 [31] | y | y | y | y | y | y | y | y | ct | y |
| 3 | Jones 2016 [32] | y | y | y | y | y | ct | y | y | y | y |
| 4 | Ojanen et al., 2019 [33] | y | y | y | y | y | y | y | y | y | y |
| 5 | Sanders et al., 2015 [34] | y | y | y | y | y | ct | y | y | y | y |
| No | Study | 1 | 2 | 3 | 4 | 5a | 5b | 6a | 6b | 9 | 10 | 11 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Bennecke et al., 2015 [35] | y | y | y | y | ct | ct | y | ct | y | y | y |
| 2 | Berglund et al., 2018 [36] | y | y | y | y | ct | ct | y | y | y | y | y |
| 3 | D’Alberton [37] | y | y | y | y | ct | ct | y | y | y | y | y |
| 4 | Hughes 2018 [38] | y | ct | ct | ct | y | y | ct | ct | y | ct | y |
| 5 | Jürgensen et al., 2013 [39] | y | y | y | y | y | y | ct | n/a | y | y | y |
| 6 | Köhler et al., 2012 [18] | y | y | y | y | y | y | ct | ct | y | y | y |
| 7 | Thyen et al., 2014 [20] | y | y | y | y | y | y | y | y | y | y | y |
| 8 | Wang and Tian 2015 [40] | y | y | y | y | y | y | ct | ct | ct | ct | ct |
| 9 | Schweizer 2014 [41] | y | y | y | y | y | y | ct | y | y | y | y |
| No | Study | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Jones 2018 [4] | y | y | ct | n/a | n/a | n/a | ct | y | y | n/a |
| 2 | Zeeman et al., 2018 [1] | y | y | y | n/a | y | y | y | y | y | n/a |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zeeman, L.; Aranda, K. A Systematic Review of the Health and Healthcare Inequalities for People with Intersex Variance. Int. J. Environ. Res. Public Health 2020, 17, 6533. https://doi.org/10.3390/ijerph17186533
Zeeman L, Aranda K. A Systematic Review of the Health and Healthcare Inequalities for People with Intersex Variance. International Journal of Environmental Research and Public Health. 2020; 17(18):6533. https://doi.org/10.3390/ijerph17186533
Chicago/Turabian StyleZeeman, Laetitia, and Kay Aranda. 2020. "A Systematic Review of the Health and Healthcare Inequalities for People with Intersex Variance" International Journal of Environmental Research and Public Health 17, no. 18: 6533. https://doi.org/10.3390/ijerph17186533
APA StyleZeeman, L., & Aranda, K. (2020). A Systematic Review of the Health and Healthcare Inequalities for People with Intersex Variance. International Journal of Environmental Research and Public Health, 17(18), 6533. https://doi.org/10.3390/ijerph17186533