Association between Gait Variability and Gait-Ability Decline in Elderly Women with Subthreshold Insomnia Stage






Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Instrumentation
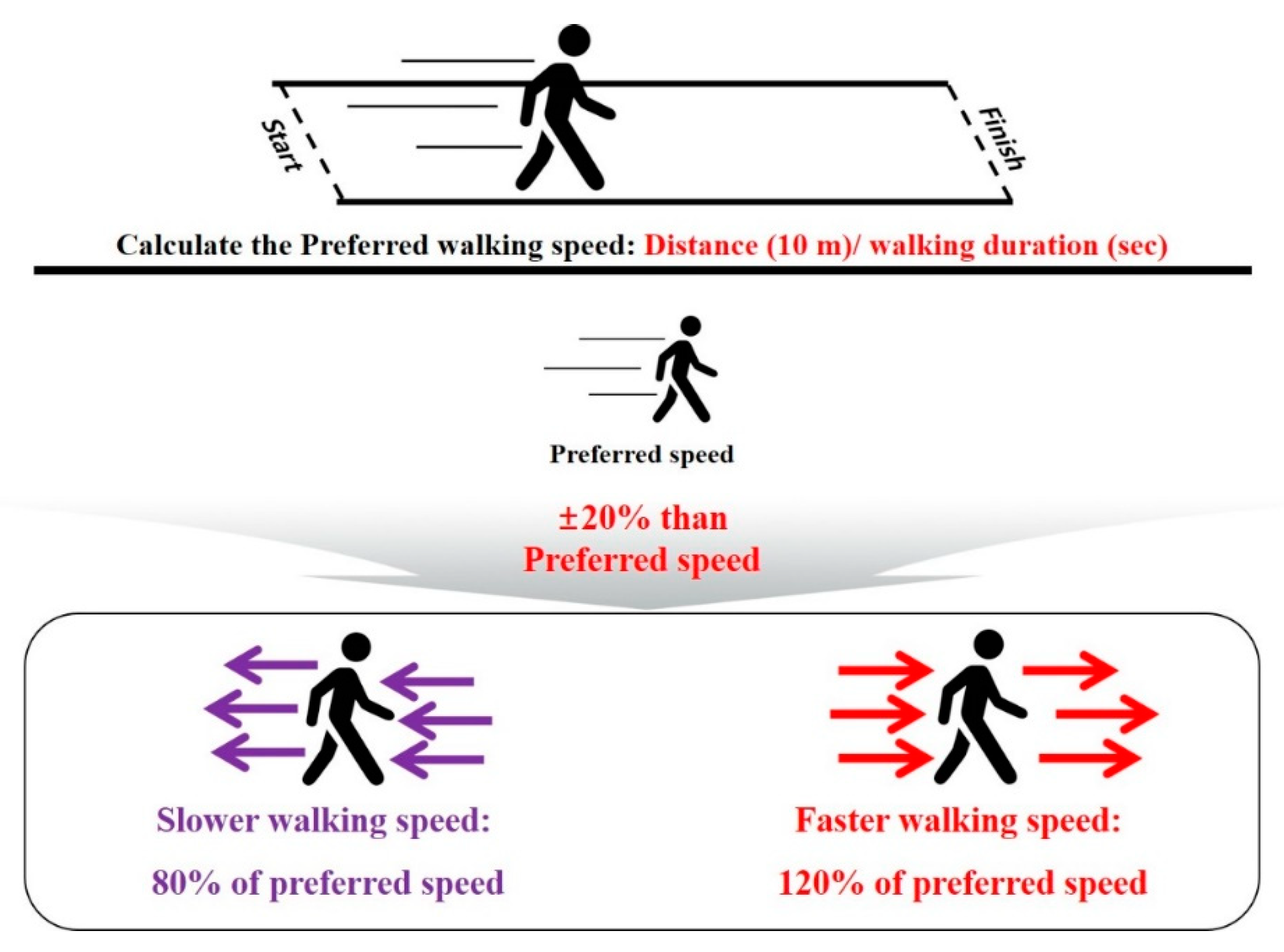
2.3. Test Procedure
2.4. Data Analyses
2.5. Statistical Analyses
3. Results
3.1. Group Differences: Insomnia vs. Control Group
3.2. Speed Differences: Slower, Preferred, and Faster Speed Condition Gait-Related Variables for All the Participants
3.3. Classifier Variables for the Insomnia and Control Groups
3.4. Relationship between the Total ISI Score and Functional Characteristics for the Global Cognitive Function, PA, and Stress Responses of All the Participants
3.5. Relationship Between the Total ISI Score and Gait-Related Variables of all the Participants
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Data Availability
References
- Perry, J.; Davids, J.R. Gait analysis: Normal and pathological function. J. Pediatr. Orthop. 1992, 12, 815. [Google Scholar] [CrossRef]
- Godfrey, A.; Del Din, S.; Barry, G.; Mathers, J.C.; Rochester, L. Instrumenting gait with an accelerometer: A system and algorithm examination. Med. Eng. Phys. 2015, 37, 400–407. [Google Scholar] [CrossRef] [PubMed]
- McKay, M.J.; Baldwin, J.N.; Ferreira, P.; Simic, M.; Vanicek, N.; Wojciechowski, E.; Mudge, A.; Burns, J. 1000 Norms Project Consortium, 2017. Spatiotemporal and plantar pressure patterns of 1000 healthy individuals aged 3–101 years. Gait Posture 2017, 58, 78–87. [Google Scholar] [CrossRef] [PubMed]
- Hollman, J.H.; McDade, E.M.; Petersen, R.C. Normative spatiotemporal gait parameters in older adults. Gait Posture 2011, 34, 111–118. [Google Scholar] [CrossRef]
- Herssens, N.; Verbecque, E.; Hallemans, A.; Vereeck, L.; Van Rompaey, V.; Saeys, W. Do spatiotemporal parameters and gait variability differ across the lifespan of healthy adults? A systematic review. Gait Posture 2018, 64, 181–190. [Google Scholar] [CrossRef]
- Aboutorabi, A.; Arazpour, M.; Bahramizadeh, M.; Hutchins, S.W.; Fadayevatan, R. The effect of aging on gait parameters in able-bodied older subjects: A literature review. Aging Clin. Exp. Res. 2016, 28, 393–405. [Google Scholar] [CrossRef]
- Almarwani, M.; VanSwearingen, J.M.; Perera, S.; Sparto, P.J.; Brach, J.S. Challenging the motor control of walking: Gait variability during slower and faster pace walking conditions in younger and older adults. Arch. Gerontol. Geriatr. 2016, 66, 54–61. [Google Scholar] [CrossRef]
- Rennie, L.; Löfgren, N.; Moe-Nilssen, R.; Opheim, A.; Dietrichs, E.; Franzén, E. The reliability of gait variability measures for individuals with Parkinson’s disease and healthy older adults—The effect of gait speed. Gait Posture 2018, 62, 505–509. [Google Scholar] [CrossRef]
- Plotnik, M.; Giladi, N.; Hausdorff, J.M. A new measure for quantifying the bilateral coordination of human gait: Effects of aging and Parkinson’s disease. Exp. Brain Res. 2007, 181, 561–570. [Google Scholar] [CrossRef]
- Nasirzade, A.; Sadeghi, H.; Mokhtarinia, H.R.; Rahimi, A. A review of selected factors affecting gait symmetry. Phys. Treat. Specif. Phys. Ther. J. 2017, 7, 3–12. [Google Scholar] [CrossRef]
- Patel, D.; Steinberg, J.; Patel, P. Insomnia in the elderly: A review. J. Clin. Sleep Med. 2018, 14, 1017–1024. [Google Scholar] [CrossRef] [PubMed]
- La, Y.K.; Choi, Y.H.; Chu, M.K.; Nam, J.M.; Choi, Y.C.; Kim, W.J. Gender differences influence over insomnia in Korean population: A cross-sectional study. PLoS ONE 2020, 15, e0227190. [Google Scholar] [CrossRef] [PubMed]
- Cao, X.L.; Wang, S.B.; Zhong, B.L.; Zhang, L.; Ungvari, G.S.; Ng, C.H.; Li, L.; Lok, G.K.I.; Lu, J.; Jia, F. The prevalence of insomnia in the general population in China: A meta-analysis. PLoS ONE 2017, 14, e0170772. [Google Scholar] [CrossRef]
- Crowley, K. Sleep and sleep disorders in older adults. Neuropsychol. Rev. 2011, 21, 41–53. [Google Scholar] [CrossRef] [PubMed]
- Ohayon, M.M. Epidemiology of insomnia: What we know and what we still need to learn. Sleep Med. Rev. 2002, 6, 97–111. [Google Scholar] [CrossRef] [PubMed]
- Yaffe, K.; Falvey, C.M.; Hoang, T. Connections between sleep and cognition in older adults. Lancet Neurol. 2014, 13, 1017–1028. [Google Scholar] [CrossRef]
- Spörndly-Nees, S.; Åsenlöf, P.; Lindberg, E. High or increasing levels of physical activity protect women from future insomnia. Sleep Med. 2017, 32, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Kredlow, M.A.; Capozzoli, M.C.; Hearon, B.A.; Calkins, A.W.; Otto, M.W. The effects of physical activity on sleep: A meta-analytic review. J. Behav. Med. 2015, 38, 427–449. [Google Scholar] [CrossRef] [PubMed]
- Bondarev, D.; Laakkonen, E.K.; Finni, T.; Kokko, K.; Kujala, U.M.; Aukee, P.; Kovanen, V.; Sipilä, S. Physical performance in relation to menopause status and physical activity. Menopause 2018, 25, 1432–1441. [Google Scholar] [CrossRef]
- Maltais, M.L.; Desroches, J.; Dionne, I.J. Changes in muscle mass and strength after menopause. J. Musculoskel. Neuron. Interact 2009, 9, 186–197. [Google Scholar]
- Chen, T.Y.; Lee, S.; Buxton, O.M. A greater extent of insomnia symptoms and physician-recommended sleep medication use predict fall risk in community-dwelling older adults. Sleep 2017, 40, 142. [Google Scholar] [CrossRef] [PubMed]
- Hill, E.L.; Cumming, R.G.; Lewis, R.; Carrington, S.; Couteur, D.G.L. Sleep disturbances and falls in older people. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2007, 62, 62–66. [Google Scholar] [CrossRef] [PubMed]
- Daley, M.; Morin, C.M.; LeBlanc, M.; Grégoire, J.P.; Savard, J. The economic burden of insomnia: Direct and indirect costs for individuals with insomnia syndrome, insomnia symptoms, and good sleepers. Sleep 2009, 32, 55–64. [Google Scholar] [PubMed]
- Agmon, M.; Shochat, T.; Kizony, R. Sleep quality is associated with walking under dual-task, but not single-task performance. Gait Posture 2016, 49, 127–131. [Google Scholar] [CrossRef]
- Hartmann, A.; Luzi, S.; Murer, K.; de Bie, R.A.; de Bruin, E.D. Concurrent validity of a trunk tri-axial accelerometer system for gait analysis in older adults. Gait Posture 2009, 29, 444–448. [Google Scholar] [CrossRef]
- Han, S.H.; Kim, C.O.; Kim, K.J.; Jeon, J.; Chang, H.; Kim, E.S.; Park, H. Quantitative analysis of the bilateral coordination and gait asymmetry using inertial measurement unit-based gait analysis. PLoS ONE 2019, 14, e0222913. [Google Scholar] [CrossRef]
- Noh, B.; Youm, C.; Lee, M.; Park, H. Age-specific differences in gait domains and global cognitive function in older women: Gait characteristics based on gait speed modification. PeerJ 2020, 8, e8820. [Google Scholar] [CrossRef]
- Lee, M.; Youm, C.; Noh, B.; Park, H.; Cheon, S.M. Gait characteristics under imposed challenge speed conditions in patients with Parkinson’s disease during overground walking. Sensors 2020, 20, 2132. [Google Scholar] [CrossRef]
- Bastien, C.H.; Vallières, A.; Morin, C.M. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001, 2, 297–307. [Google Scholar] [CrossRef]
- Gerber, M.; Lang, C.; Lemola, S.; Colledge, F.; Kalak, N.; Holsboer-Trachsler, E.; Pühse, U.; Brand, S. Validation of the German version of the insomnia severity index in adolescents, young adults and adult workers: Results from three cross-sectional studies. BMC Psychiatry 2016, 16, 1–14. [Google Scholar] [CrossRef]
- Morin, C.M. Insomnia: Psychological Assessment and Management; Guilford press: New York, NY, USA, 1993. [Google Scholar]
- Joo, J.Y.; Kim, Y.K.; Park, J.Y. Reliability of 3D-inertia measurement unit based shoes in gait analysis. Korean J. Sport Biomech. 2015, 25, 123–130. [Google Scholar] [CrossRef][Green Version]
- Lee, M.; Youm, C.; Jeon, J.; Cheon, S.M.; Park, H. Validity of shoe-type inertial measurement units for Parkinson’s disease patients during treadmill walking. J. Neuroeng. Rehabil. 2018, 15, 38. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. Mini-mental state: A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Oyeyemi, A.L.; Umar, M.; Oguche, F.; Aliyu, S.U.; Oyeyemi, A.Y. Accelerometer-determined physical activity and its comparison with the international physical activity questionnaire in a sample of Nigerian adults. PLoS ONE 2014, 9, e87233. [Google Scholar] [CrossRef]
- Choi, S.M.; Kang, T.Y.; Woo, J.M. Development and validation of a modified form of the stress response inventory for workers. J. Korean Neuropsychiatr. Assoc. 2006, 45, 541–553. [Google Scholar]
- Koh, K.B.; Park, J.K.; Kim, C.H.; Cho, S. Development of the stress response inventory and its application in clinical practice. Psychosom. Med. 2001, 63, 668–678. [Google Scholar] [CrossRef]
- Lee, M.; Youm, C.; Noh, B.; Park, H. Gait characteristics based on shoe-type inertial measurement units in healthy young adults during treadmill walking. Sensors 2020, 20, 2095. [Google Scholar] [CrossRef]
- Kim, Y.K.; Joo, J.Y.; Jeong, S.H.; Jeon, J.H.; Jung, D.Y. Effects of walking speed and age on the directional stride regularity and gait variability in treadmill walking. J. Mech. Sci. Technol. 2016, 30, 2899–2906. [Google Scholar] [CrossRef]
- Lord, S.; Galna, B.; Verghese, J.; Coleman, S.; Burn, D.; Rochester, L. Independent domains of gait in older adults and associated motor and nonmotor attributes: Validation of a factor analysis approach. J. Gerontol. Ser. A 2012, 68, 820–827. [Google Scholar] [CrossRef]
- Verlinden, V.J.; van der Geest, J.N.; Hofman, A.; Ikram, M.A. Cognition and gait show a distinct pattern of association in the general population. Alzheimer Dement. 2014, 10, 328–335. [Google Scholar] [CrossRef]
- Plotnik, M.; Bartsch, R.P.; Zeev, A.; Giladi, N.; Hausdorff, J.M. Effects of walking speed on asymmetry and bilateral coordination of gait. Gait Posture 2013, 38, 864–869. [Google Scholar] [CrossRef] [PubMed]
- Oh-Park, M.; Holtzer, R.; Mahoney, J.; Wang, C.; Verghese, J. Effect of treadmill training on specific gait parameters in older adults with frailty: Case series. J. Geriatr. Phys. Ther. 2011, 34, 184–188. [Google Scholar] [CrossRef] [PubMed]
- Pau, M.; Leban, B.; Collu, G.; Migliaccio, G.M. Effect of light and vigorous physical activity on balance and gait of older adults. Arch. Gerontol. Geriatr. 2014, 59, 568–573. [Google Scholar] [CrossRef]
- Persch, L.N.; Ugrinowitsch, C.; Pereira, G.; Rodacki, A.L. Strength training improves fall-related gait kinematics in the elderly: A randomized controlled trial. Clin. Biomech. 2009, 24, 819–825. [Google Scholar] [CrossRef] [PubMed]
- Schneider, W.; Chein, J.M. Controlled & automatic processing: Behavior, theory, and biological mechanisms. Cogn. Sci. 2003, 27, 525–559. [Google Scholar]
- Ruffieux, J.; Keller, M.; Lauber, B.; Taube, W. Changes in standing and walking performance under dual-task conditions across the lifespan. Sports Med. 2015, 45, 1739–1758. [Google Scholar] [CrossRef]
- Clark, D.J. Automaticity of walking: Functional significance, mechanisms, measurement and rehabilitation strategies. Front. Hum. Neurosci. 2015, 9, 246. [Google Scholar] [CrossRef]
- Cricco, M.; Simonsick, E.M.; Foley, D.J. The impact of insomnia on cognitive functioning in older adults. J. Am. Geriatr. Soc. 2001, 49, 1185–1189. [Google Scholar] [CrossRef]
- Sexton, C.E.; Storsve, A.B.; Walhovd, K.B.; Johansen-Berg, H.; Fjell, A.M. Poor sleep quality is associated with increased cortical atrophy in community-dwelling adults. Neurology 2014, 83, 967–973. [Google Scholar] [CrossRef]
- Lewis, S.J. Neurological update: Emerging issues in gait disorders. J. Neurol. 2015, 262, 1590–1595. [Google Scholar] [CrossRef]
- Holt, K.G.; Jeng, S.F.; Ratcliffe, R.; Hamill, J. Energetic cost and stability during human walking at the preferred stride frequency. J. Motor Behav. 1995, 27, 164–178. [Google Scholar] [CrossRef] [PubMed]
- Gabell, A.; Nayak, U.S.L. The effect of age on variability in gait. J. Gerontol. 1984, 39, 662–666. [Google Scholar] [CrossRef]
- Nutt, J.G.; Marsden, C.D.; Thompson, P.D. Human walking and higher-level gait disorders, particularly in the elderly. Neurology 1993, 43, 268. [Google Scholar] [CrossRef] [PubMed]
- Hausdorff, J.M.; Rios, D.A.; Edelberg, H.K. Gait variability and fall risk in community-living older adults: A 1-year prospective study. Arch. Phys. Med. Rehabil. 2001, 82, 1050–1056. [Google Scholar] [CrossRef]
- Hausdorff, J.M. Stride variability: Beyond length and frequency. Gait Posture 2004, 20, 304. [Google Scholar] [CrossRef] [PubMed]
- Hausdorff, J.M.; Yogev, G.; Springer, S.; Simon, E.S.; Giladi, N. Walking is more like catching than tapping: Gait in the elderly as a complex cognitive task. Exp. Brain Res. 2005, 164, 541–548. [Google Scholar] [CrossRef] [PubMed]
- Hollman, J.H.; Watkins, M.K.; Imhoff, A.C.; Braun, C.E.; Akervik, K.A.; Ness, D.K. A comparison of variability in spatiotemporal gait parameters between treadmill and overground walking conditions. Gait Posture 2016, 43, 204–209. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Insomnia (n = 202) (min to max, 95% CI) | Controls (n = 190) (min to max, 95% CI) | T-Test p-Value | Cohen’s d |
|---|---|---|---|---|
| Age (years) | 71.3 ± 4.6 (70.7 to 72.0) | 71.4 ± 4.9 (70.7 to 72.1) | 0.876 | 0.016 |
| Height (cm) | 155.5 ± 5.3 (154.7 to 156.2) | 154.9 ± 5.9 (154.1 to 155.8) | 0.330 | 0.098 |
| Body weight (kg) | 58.8 ± 7.3 (57.8 to 59.8) | 59.4 ± 7.9 (58.3 to 60.5) | 0.438 | 0.078 |
| BMI (kg/m2) | 24.3 ± 2.9 (23.9 to 24.7) | 24.8 ± 3.1 (24.3 to 25.2) | 0.150 | 0.147 |
| Body fat percentage (%) | 32.9 ± 5.9 (32.1 to 33.7) | 33.0 ± 6.6 (32.0 to 33.9) | 0.878 | 0.016 |
| ISI (score) | 10.9 ± 2.4 (10.5 to 11.2) | 2.0 ± 2.5 (1.6 to 2.3) | <0.001 | 3.639 |
| MMSE (score) | 27.4 ± 2.6 (27.0 to 27.8) | 27.9 ± 2.1 (27.6 to 28.2) | 0.022 | 0.233 |
| SRI-MF (score) | 5.3 ± 6.3 (4.4 to6.2) | 3.1 ± 4.9 (2.4 to 3.8) | <0.001 | 0.396 |
| Vigorous PAs (Mets/week) | 997.8 ± 1385.7 (805.6 to 1190.1) | 1118.5 ± 1696.8 (875.7 to 1361.3) | 0.440 | 0.078 |
| Moderate PAs (Mets/week) | 618.9 ± 743.1 (515.8 to 722.0) | 817.7 ± 951.3 (681.5 to 953.8) | 0.021 | 0.232 |
| Walking PAs (Mets/week) | 787.8 ± 927.5 (659.1 to 916.5) | 997.7 ± 977.76 (857.8 to 1137.7) | 0.030 | 0.220 |
| Total PAs (Mets/week) | 2404.5 ± 2304.1 (2084.8 to 2724.2) | 2933.9 ± 2487.9 (2577.9 to 3290.0) | 0.029 | 0.213 |
| Variables | Definition |
|---|---|
| Pace parameters | |
| Walking speed (m/s) | Performed treadmill walking speed |
| Stride length (m) | Distance between the first contact of one foot to the first contact of the following ipsilateral foot, measured parallel to the direction of progression |
| Step length (m) | Distance between the successive heel points of opposite feet, measured parallel to the direction of progression |
| Rhythm parameters | |
| Cadence (beats/min) | Total number of steps during 1 min |
| Stride time (s) | Time taken between the first contact of one foot to the first contact of the following ipsilateral foot |
| Step time (s) | Time taken between the first contact of one foot to the first contact of the following contralateral foot |
| Phase parameters | |
| Single support phase (%) | Time when one foot is in contact with the ground during one stride cycle |
| Double support phase (%) | Time when both feet is in contact with the ground during one stride cycle |
| Stance phase (%) | Time when foot is in contact with the ground during one stride cycle |
| Gait variability | |
| Parameters for pace, rhythm, and phase (%) | Coefficient of variance ((standard deviation/mean) × 100) for stride length, step length, stride time, step time, single support phase, double support phase, and stance phase |
| Bilateral coordination [9] | |
| GA (%) | Temporal symmetry between the left and right foot during walking |
| PCI (%) | Coordination between the left and right foot during walking |
| Variables | Slower Speed | Preferred Speed | Faster Speed | Group Significance | Speed Significance | ||||
|---|---|---|---|---|---|---|---|---|---|
| Insomnia | Controls | Insomnia | Controls | Insomnia | Controls | Insomnia | Controls | ||
| Pace parameters | |||||||||
| Walking speed (m/s) | 0.67 ± 0.15 | 0.74 ± 0.13 | 0.84 ± 0.19 | 0.92 ± 0.16 | 1.01 ± 0.23 | 1.10 ± 0.19 | A, B, C | d, e, f | d, e, f |
| Stride length (m) | 0.90 ± 0.24 | 0.96 ± 0.18 | 0.99 ± 0.26 | 1.07 ± 0.19 | 1.10 ± 0.26 | 1.18 ± 0.19 | A, B, C | d, e, f | d, e, f |
| Step length (m) | 0.45 ± 0.12 | 0.48 ± 0.09 | 0.49 ± 0.13 | 0.53 ± 0.10 | 0.55 ± 0.13 | 0.59 ± 0.09 | A, B, C | d, e, f | d, e, f |
| Rhythm parameters | |||||||||
| Cadence (beats/min) | 92.50 ± 17.10 | 92.78 ± 14.72 | 103.49 ± 15.41 | 104.15 ± 14.62 | 110.66 ± 14.20 | 111.79 ± 12.97 | N/S | d, e, f | d, e, f |
| Stride time (s) | 1.33 ± 0.24 | 1.32 ± 0.21 | 1.18 ± 0.18 | 1.17 ± 0.17 | 1.10 ± 0.14 | 1.08 ± 0.13 | N/S | d, e, f | d, e, f |
| Step time (s) | 0.67 ± 0.12 | 0.66 ± 0.10 | 0.59 ± 0.09 | 0.58 ± 0.08 | 0.55 ± 0.07 | 0.54 ± 0.06 | N/S | d, e, f | d, e, f |
| Phase parameters | |||||||||
| Single support phase (%) | 35.17 ± 2.61 | 35.51 ± 2.12 | 36.48 ± 2.20 | 36.85 ± 1.64 | 37.43 ± 2.03 | 37.86 ± 1.57 | C | d, e, f | d, e, f |
| Double support phase (%) | 29.46 ± 4.79 | 29.05 ± 4.16 | 27.09 ± 3.57 | 26.29 ± 3.10 | 25.14 ± 3.32 | 24.32 ± 2.90 | B, C | d, e, f | d, e, f |
| Stance phase (%) | 64.63 ± 2.61 | 64.56 ± 2.37 | 63.57 ± 1.86 | 63.14 ± 1.80 | 62.57 ± 1.65 | 62.18 ± 1.58 | B, C | d, e, f | d, e, f |
| Gait variability | |||||||||
| CV of stride length (%) | 3.45 ± 2.12 | 3.20 ± 1.74 | 3.24 ± 2.24 | 2.53 ± 1.45 | 2.39 ± 1.79 | 1.79 ± 1.04 | B, C | e, f | d, e, f |
| CV of step length (%) | 2.19 ± 1.54 | 2.06 ± 1.09 | 1.94 ± 1.47 | 1.42 ± 0.76 | 1.30 ± 1.02 | 0.95 ± 0.47 | B, C | d, e, f | d, e, f |
| CV of stride time (%) | 3.45 ± 2.12 | 3.20 ± 1.74 | 3.24 ± 2.24 | 2.53 ± 1.45 | 2.39 ± 1.79 | 1.79 ± 1.04 | B, C | e, f | d, e, f |
| CV of step time (%) | 3.31 ± 2.07 | 3.17 ± 1.72 | 3.28 ± 2.27 | 2.45 ± 1.32 | 2.38 ± 1.90 | 1.77 ± 0.83 | B, C | e, f | d, e, f |
| CV of single support phase (%) | 7.32 ± 3.92 | 6.55 ± 2.70 | 5.38 ± 3.22 | 4.42 ± 1.73 | 4.06 ± 3.41 | 3.05 ± 1.19 | A, B, C | d, e, f | d, e, f |
| CV of double support phase (%) | 12.35 ± 8.02 | 10.71 ± 4.85 | 10.59 ± 7.76 | 7.80 ± 3.69 | 8.20 ± 8.06 | 5.71 ± 2.90 | A, B, C | d, e, f | d, e, f |
| CV of stance phase (%) | 5.69 ± 3.67 | 5.01 ± 2.47 | 4.63 ± 3.39 | 3.46 ± 1.87 | 3.16 ± 2.31 | 2.28 ± 1.22 | A, B, C | d, e, f | d, e, f |
| Bilateral coordination | |||||||||
| GA (%) | 4.57 ± 3.76 | 3.67 ± 3.15 | 3.88 ± 3.65 | 2.87 ± 2.82 | 3.19 ± 2.92 | 2.41 ± 2.16 | A, B, C | d, e, f | d, e, f |
| PCI (%) | 5.92 ± 4.32 | 5.05 ± 2.21 | 5.35 ± 4.75 | 4.14 ± 2.50 | 4.72 ± 5.26 | 3.26 ± 1.85 | A, B, C | d, e, f | d, e, f |
| Variables | Estimate | SE | OR | 95% CI for the OR | p-Value |
|---|---|---|---|---|---|
| Slower speed | |||||
| Walking speed | −3.740 | 0.824 | 0.024 | 0.005–0.119 | <0.001 |
| Preferred speed | |||||
| Walking speed | −2.086 | 0.716 | 0.124 | 0.030–0.505 | 0.004 |
| CV of double support phase | 0.068 | 0.025 | 1.070 | 1.019–1.123 | 0.006 |
| Faster speed | |||||
| Walking speed | −1.567 | 0.638 | 0.209 | 0.060–0.729 | 0.014 |
| CV of stance phase | 0.207 | 0.084 | 1.229 | 1.042–1.451 | 0.014 |
| Gait Parameters | Variables | ISI Score | ||
|---|---|---|---|---|
| Slower | Preferred | Faster | ||
| Pace | Walking speed | −0.184 * | −0.186 * | −0.185 * |
| Stride length | −0.114 * | −0.163 * | −0.165 * | |
| Step length | −0.116 * | −0.162 * | −0.164 * | |
| Phases | Double support phase | - | - | 0.110 * |
| Stance phase | - | - | 0.105 * | |
| GV: Pace | CV of stride length | - | 0.190 * | 0.156 * |
| CV of step length | - | 0.192 * | 0.140 * | |
| GV: Phases | CV of single support phase | - | 0.116 * | 0.112 * |
| CV of double support phase | - | 0.206 * | 0.153 * | |
| CV of stance phase | - | 0.197 * | 0.185 * | |
| GV: Rhythms | CV of stride time | - | 0.190 * | 0.156 * |
| CV of step time | - | 0.201 * | 0.138 * | |
| Bilateral coordination | GA | 0.157 * | 0.191 * | 0.138 * |
| PCI | - | 0.146 * | 0.164 * | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, T.; Lee, M.; Youm, C.; Noh, B.; Park, H. Association between Gait Variability and Gait-Ability Decline in Elderly Women with Subthreshold Insomnia Stage. Int. J. Environ. Res. Public Health 2020, 17, 5181. https://doi.org/10.3390/ijerph17145181
Lee T, Lee M, Youm C, Noh B, Park H. Association between Gait Variability and Gait-Ability Decline in Elderly Women with Subthreshold Insomnia Stage. International Journal of Environmental Research and Public Health. 2020; 17(14):5181. https://doi.org/10.3390/ijerph17145181
Chicago/Turabian StyleLee, Taesang, Myeounggon Lee, Changhong Youm, Byungjoo Noh, and Hwayoung Park. 2020. "Association between Gait Variability and Gait-Ability Decline in Elderly Women with Subthreshold Insomnia Stage" International Journal of Environmental Research and Public Health 17, no. 14: 5181. https://doi.org/10.3390/ijerph17145181
APA StyleLee, T., Lee, M., Youm, C., Noh, B., & Park, H. (2020). Association between Gait Variability and Gait-Ability Decline in Elderly Women with Subthreshold Insomnia Stage. International Journal of Environmental Research and Public Health, 17(14), 5181. https://doi.org/10.3390/ijerph17145181