Changes in the Type of Sports Activity Due to COVID-19: Hypochondriasis and the Intention of Continuous Participation in Sports

Abstract
1. Introduction
1.1. Background
1.2. Objectives
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Instruments
3. Results
3.1. Scale Validity and Reliability
3.2. Factorial Multivariate Analysis of Variance: Differences of Age and Type of Sport on Hypochondriasis and Intention of Continuous Participation
4. Discussion
5. Conclusions and Limitations
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Sato, M.; Jordan, J.S.; Funk, D.C. The role of physically active leisure for enhancing quality of life. Lei. Sci. 2014, 36, 293–313. [Google Scholar]
- Shin, D.; Enoh, J. Availability and use of work–life balance programs: Relationship with organizational profitability. Sustainability 2020, 12, 2965. [Google Scholar] [CrossRef]
- Brough, P.; Timms, C.; Chan, X.W.; Hawkes, A.; Rasmussen, L. Work–life balance: Definitions, causes, and consequences. In Handbook of Socioeconomic Determinants of Occupational Health; Theorell, T., Ed.; Springer: Cham, Switzerland, 2020. [Google Scholar]
- Cooper, S.L. Promoting physical activity for mental well-being. ACSM’s Health Fit. J. 2020, 24, 12–16. [Google Scholar] [CrossRef]
- Teychenne, M.; White, R.L.; Justin, R.; Schuh, F.B.; Rosenbaum, S.; Bennie, J.A. Do we need physical activity guidelines for mental health: What does the evidence tell us? Ment. Health Phys. Act. 2020, 18, 100315. [Google Scholar] [CrossRef]
- World Health Organization. Coronavirus Disease (COVID-19) Pandemic. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 2 April 2020).
- Centers for Disease Control and Prevention. How to Protect Yourself & Others. Available online: https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/prevention.html (accessed on 1 April 2020).
- Centers for Disease Control and Prevention. Symptoms of Coronavirus. Available online: https://www.cdc.gov/coronavirus/2019-ncov/symptoms-testing/sy mptoms.html (accessed on 22 March 2020).
- Korea Centers for Disease Control and Prevention. Information for COVID-19. Available online: http://ncov.mohw.go.kr/baroView.do?brdId=4&brdGubun=41 (accessed on 24 March 2020).
- BBC. Coronavirus Confirmed as Pandemic by World Health Organization. Available online: https://www.bbc.com/news/world-5183994 4 (accessed on 2 April 2020).
- BBC. Coronavirus: The World in Lockdown in Maps and Charts. Available online: https://www.bbc.com/news/world-52103747 (accessed on 1 April 2020).
- World Health Organization. Coronavirus Disease (COVID-19) Advice for the Public. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public (accessed on 4 April 2020).
- Holcombe, M. Long-Term Social Distancing May be Traumatic. Here is What to Expect and What to do. 2020. Available online: https://edition.cnn.com/2020/04/09/health/coronavirus-mental-health-long-term-wellness/index.html (accessed on 10 April 2020).
- Rachman, S. Health anxiety disorders: A cognitive construal. Behav. Res. Ther. 2012, 50, 502–512. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.S. The catastrophizing tendency of individuals with high health anxiety. Master’s Thesis, Seoul National University, Seoul, Korea, 2004. [Google Scholar]
- Creed, F.; Barsky, A.J. A systematic review of the epidemiology of somatisation disorder and hypochondriasis. J. Psychosom. Res. 2004, 56, 391–408. [Google Scholar] [CrossRef]
- Moon, H.J. The mediating effect of rumination on the relationship between mindfulness and hypochondriacal tendencies. Master’s Thesis, The Catholic University of Korea, Seoul, Korea, 2013. [Google Scholar]
- Martinsen, E.W. Physical activity in the prevention and treatment of anxiety and depression. Nord. J. Psychiatry 2007, 62, 25–29. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.S.; Won, Y.S.; Ko, D. Effects of participation motivation and participation satisfaction on exercise adherence intention of young-old age. J. Wellness 2017, 12, 261–271. [Google Scholar] [CrossRef]
- Craft, L.L.; Perna, F.M. The benefits of exercise for the clinically depressed. Prim. Care Companion J. Clin. Psychiatry 2004, 6, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Morgan, C.; Wang, A. Why South Korea’s Coronavirus Curve looks so Different from the United States. Available online: https://www.businessinsider.com/south-koreas-coronavirus-curve-timeline-2020-4 (accessed on 1 April 2020).
- Sirard, J.R.; Pate, R.R. Physical Activity Assessment in Children and Adolescents. Sports Med. 2001, 31, 439–454. [Google Scholar] [CrossRef] [PubMed]
- Petry, N. A Comparison of Young, Middle-Aged, and Older Adult Treatment-Seeking Pathological Gamblers. Geronotologist 2002, 42, 92–99. [Google Scholar] [CrossRef] [PubMed]
- Kellner, R.; Abbott, P.; Winslow, W.; Pathak, D. Fear, beliefs and attitudes in DSM III hypochondriasis. J. Nerv. Ment. Dis. 1987, 175, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Yi, I. Factor structure of the Illness Attitudes Scale (IAS) in a Korean College Sample. Korean J. Health Psychol. 2004, 9, 203–218. [Google Scholar]
- Courneya, K.K.; McAuley, E. Predicting physical activity from intention: Conceptual and methodological issues. J. Sport Exerc. Psychol. 1993, 5, 50–62. [Google Scholar] [CrossRef]
- Poff, R.A. Understanding the relationship between involvement, commitment and future behavior intentions of kayakers and canoeists using structural equation modeling. Ph.D. Thesis, Unpublished dissertation. Indiana University, Boomington, IN, USA, 2001. [Google Scholar]
- Jeon, B.E.; Lee, S.Y.; Kim, J.Y. The relationship among participation motivation, life satisfaction, and continuous participation intention of triathlon enthusiasts. Korean J. Phys. Educ. 2014, 53, 309–320. [Google Scholar]
- Nunnally, J.C.; Berstein, I.H. Psychometric Theory, 3rd ed.; McGraw-Hill: New York, NY, USA, 1994. [Google Scholar]
- Lewis, S. Thousands Flock to Florida Beaches, Ignoring Coronavirus Concerns. Available online: https://www.cbsnews.com/news/coronavirus-florida-beaches-ignore-social-distancing/ (accessed on 1 May 2020).
- Centers for Disease Control and Prevention. Coping with Stress. Available online: https://www.cdc.gov/coronavirus/2019-ncov/daily-life-coping/managing-stress-anxiety.html (accessed on 1 May 2020).



{kind=link}
{kind=link}
| Young | Middle-Aged | Older | ||||
|---|---|---|---|---|---|---|
| Individual | Group | Individual | Group | Individual | Group | |
| Gender | ||||||
| Male | 30 (66.7%) | 11 (40.7%) | 27 (55.1%) | 25 (62.5%) | 26 (59.1%) | 12 (50.0%) |
| Female | 15 (33.3%) | 16 (59.3%) | 22 (44.9%) | 15 (37.5%) | 18 (40.9%) | 12 (50.0%) |
| Type of Sport | ||||||
| Home training | 13 (28.9%) | - | 9 (18.4%) | - | 8 (18.2%) | - |
| Walking | 8 (17.8%) | - | 10 (20.4%) | - | 9 (20.5%) | - |
| Running | 9 (20.0%) | - | 8 (16.3%) | - | 8 (18.2%) | - |
| Tracking | 13 (28.9%) | - | 13 (26.5%) | - | 8 (18.2%) | - |
| Cycling | 2 (4.4%) | - | 9 (18.4%) | - | 11 (25.0%) | - |
| Golf | - | 5 (18.5%) | - | 10 (25.0%) | - | 6 (25.0%) |
| Gym | - | 5 (18.5%) | - | 10 (25.0%) | - | 6 (25.0%) |
| Basketball | - | 5 (18.5%) | - | 8 (20.0%) | - | 4 (16.7%) |
| Baseball | - | 9 (33.3%) | - | 10 (25.0%)- | 4 (16.7%) | |
| Swimming | - | 1 (3.7%) | - | 4 (10.0%) | - | 5 (20.8%) |
| Frequency of playing | ||||||
| Rarely | 10 (22.2%) | 3 (11.1%) | 9 (18.4%) | 6 (15.0%) | 12 (27.3%) | 2 (8.3%) |
| Sometimes | 8 (17.8%) | 8 (29.6%) | 9 (18.4%) | 15 (37.5%) | 9 (20.5%) | 6 (25.0%) |
| Often | 10 (22.2%) | 6(22.2%) | 13 (26.5%) | 5 (12.5%) | 8 (18.2%) | 4 (16.7%) |
| Very Often | 13 (28.9%) | 7 (25.9%) | 14 (28.6%) | 10 (25.0%) | 9 (20.5%) | 6 (25.0%) |
| Always | 4 (8.9%) | 3 (11.1%) | 4 (8.2%) | 4 (10.0%) | 6 (13.6%) | 6 (25.0%) |
| Total | 45 (100%) | 27 (100%) | 49 (100%) | 40 (100%) | 44 (100%) | 24 (100%) |
| Items | 1 | 2 | 3 | 4 |
|---|---|---|---|---|
| I fear when I hear news that reminds me of death. | 0.913 | 0.126 | 0.045 | 0.034 |
| Thinking about death makes me feel afraid. | 0.857 | 0.019 | 0.013 | −0.004 |
| I fear that I might die. | 0.788 | −0.067 | 0.066 | −0.153 |
| I worry about health. | 0.084 | 0.882 | 0.202 | 0.060 |
| I worry about becoming seriously ill in the future. | −0.003 | 0.837 | −0.016 | 0.003 |
| I am scared when I think about serious diseases. | −0.004 | 0.808 | 0.215 | 0.101 |
| I fear that I may contract COVID-19. | 0.073 | 0.123 | 0.892 | 0.038 |
| I fear that I may become seriously ill. | 0.156 | 0.077 | 0.838 | 0.011 |
| When I read an article about virus, I feel similar symptoms. | −0.088 | 0.152 | 0.737 | 0.033 |
| When a symptom persists, I believe I have a serious illness. | −0.123 | 0.023 | 0.004 | 0.895 |
| If I detect a symptom, I can’t think anything else because of it. | 0.030 | 0.079 | −0.096 | 0.836 |
| If I feel unusual symptoms in my body, I worry about them. | −0.035 | 0.046 | 0.180 | 0.770 |
| Eigenvalues | 2.992 | 2.411 | 1.816 | 1.548 |
| Variance (%) | 24.935 | 20.095 | 15.136 | 12.899 |
| Source | Dependent Variables | df | F | p | Mean | ||
|---|---|---|---|---|---|---|---|
| Age | Hypochondriasis | G1 | G2 | G3 | |||
| Worry about Illness | 2 | 25.522 | 0.000 * | 2.491 | 3.254 | 3.126 | |
| Disease Phobia | 2 | 12.868 | 0.000 * | 2.676 | 3.390 | 3.202 | |
| Thanatophobia | 2 | 8.016 | 0.000 * | 2.713 | 2.856 | 3.488 | |
| Symptom Preoccupation | 2 | 0.490 | 0.613 | 3.153 | 3.167 | 3.005 | |
| Intention of Continuous Participation | 2 | 54.736 | 0.000 * | 3.656 | 2.901 | 2.116 |
| Worry about Illness | Disease Phobia | Thanatophobia | Symptom Preoccupation | Intention of Continuous Participation | ||
|---|---|---|---|---|---|---|
| G1 | G2 | 0.000 * | 0.000 * | 0.563 | 0.995 | 0.000 * |
| G3 | 0.000 * | 0.002 * | 0.000 * | 0.606 | 0.000 * | |
| G2 | G1 | 0.000 * | 0.000 * | 0.563 | 0.995 | 0.000 * |
| G3 | 0.454 | 0.418 | 0.000 * | 0.518 | 0.000 * | |
| G3 | G1 | 0.000 * | 0.002 * | 0.000 * | 0.606 | 0.000 * |
| G2 | 0.000 * | 0.418 | 0.000 * | 0.518 | 0.000 * |
| Source | Dependent Variables | df | F | p | Mean | |
|---|---|---|---|---|---|---|
| Type of Sport | Hypochondriasis | G1 | G2 | |||
| Worry about Illness | 1 | 183.419 | 0.000 * | 2.473 | 3.736 | |
| Disease Phobia | 1 | 8.399 | 0.004 * | 2.930 | 3.381 | |
| Thanatophobia | 1 | 0.159 | 0.690 | 2.976 | 3.040 | |
| Symptom Preoccupation | 1 | 12.680 | 1.000 * | 2.944 | 3.370 | |
| Intention of Continuous Participation | 1 | 26.822 | 0.000 * | 3.127 | 2.560 | |
| Source | Dependent Variables | df | F | p |
|---|---|---|---|---|
| Age * Type of Sport | Hypochondriasis | |||
| Worry about Illness | 2 | 1.106 | 0.333 | |
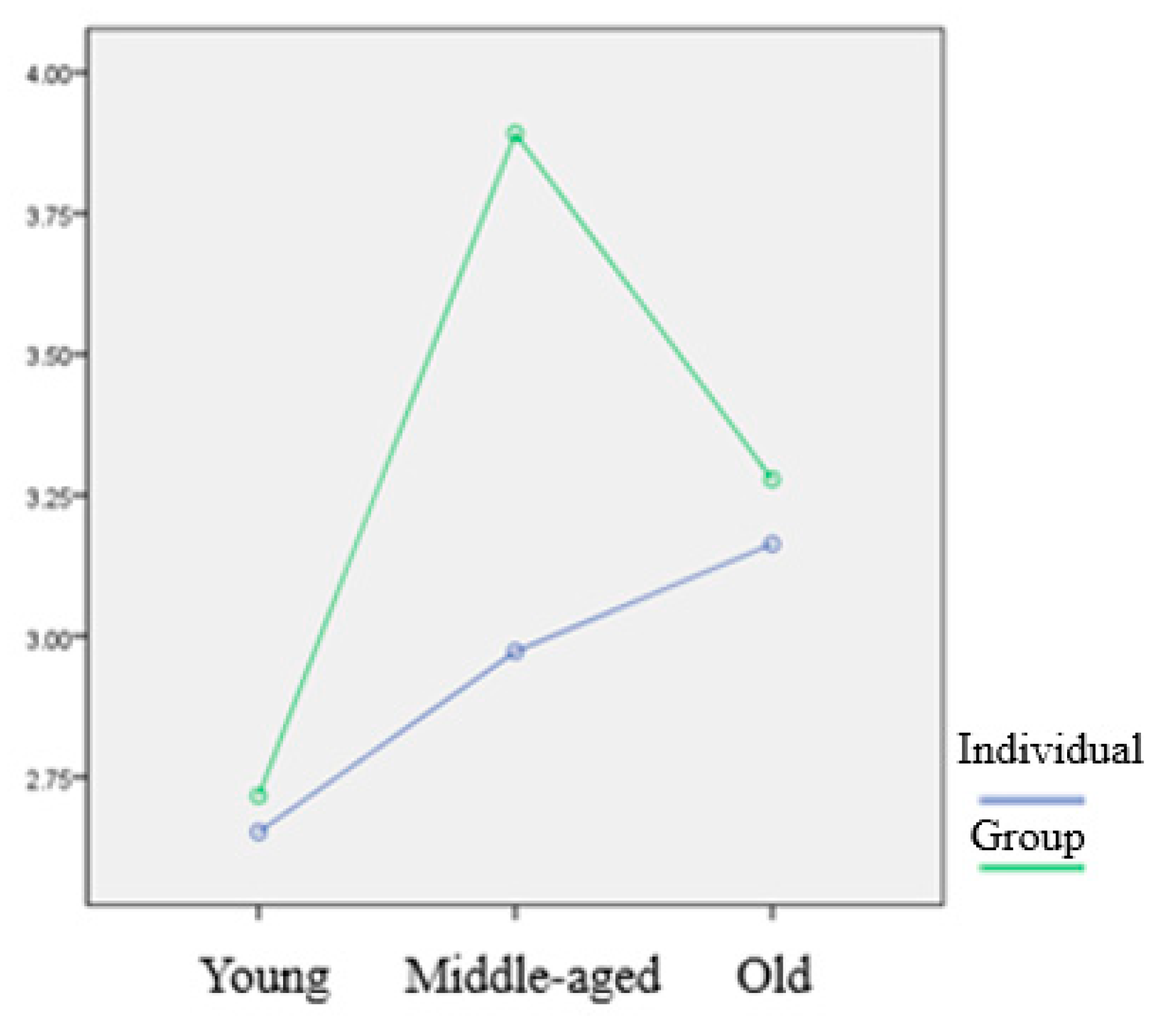
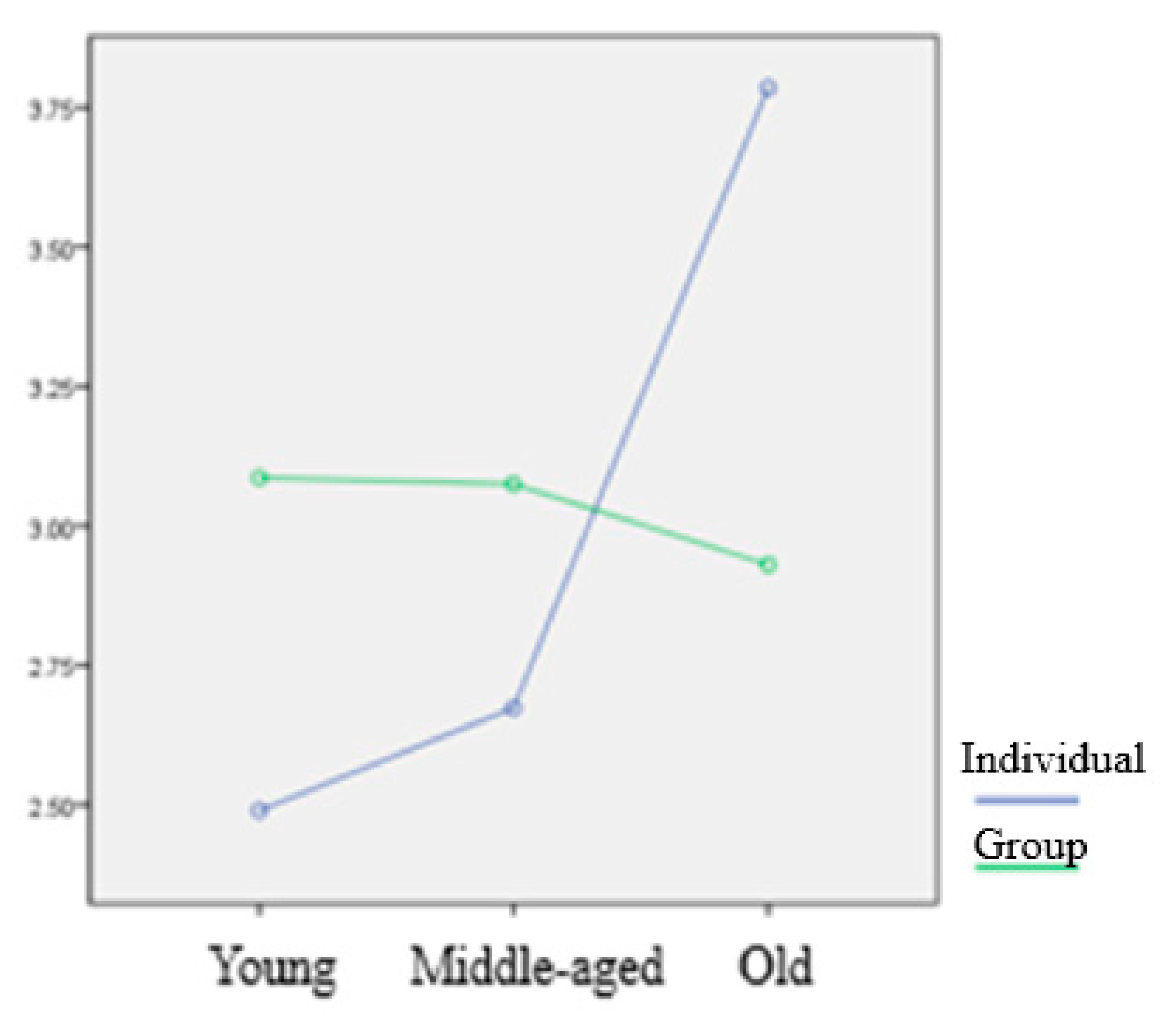
| Disease Phobia | 2 | 5.314 | 0.006 * | |
| Thanatophobia | 2 | 13.200 | 0.000 * | |
| Symptom Preoccupation | 2 | 1.901 | 0.152 | |
| Intention of Continuous Participation | 2 | 0.033 | 0.968 |
| Age | Type of Sport | WI | DP | TH | SP | ICP |
|---|---|---|---|---|---|---|
| Young | Individual | 2.096 | 2.652 | 2.489 | 2.889 | 3.889 |
| Group | 3.148 | 2.716 | 3.086 | 3.593 | 3.269 | |
| Middle-aged | Individual | 2.632 | 2.972 | 2.674 | 3.104 | 3.156 |
| Group | 4.000 | 3.892 | 3.075 | 3.242 | 2.594 | |
| Older | Individual | 2.682 | 3.163 | 3.785 | 2.830 | 2.333 |
| Group | 3.959 | 3.278 | 2.931 | 3.333 | 1.708 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, C.; Bum, C.-H. Changes in the Type of Sports Activity Due to COVID-19: Hypochondriasis and the Intention of Continuous Participation in Sports. Int. J. Environ. Res. Public Health 2020, 17, 4871. https://doi.org/10.3390/ijerph17134871
Choi C, Bum C-H. Changes in the Type of Sports Activity Due to COVID-19: Hypochondriasis and the Intention of Continuous Participation in Sports. International Journal of Environmental Research and Public Health. 2020; 17(13):4871. https://doi.org/10.3390/ijerph17134871
Chicago/Turabian StyleChoi, Chulhwan, and Chul-Ho Bum. 2020. "Changes in the Type of Sports Activity Due to COVID-19: Hypochondriasis and the Intention of Continuous Participation in Sports" International Journal of Environmental Research and Public Health 17, no. 13: 4871. https://doi.org/10.3390/ijerph17134871
APA StyleChoi, C., & Bum, C.-H. (2020). Changes in the Type of Sports Activity Due to COVID-19: Hypochondriasis and the Intention of Continuous Participation in Sports. International Journal of Environmental Research and Public Health, 17(13), 4871. https://doi.org/10.3390/ijerph17134871