Breast Cancer Primary Prevention and Diet: An Umbrella Review



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
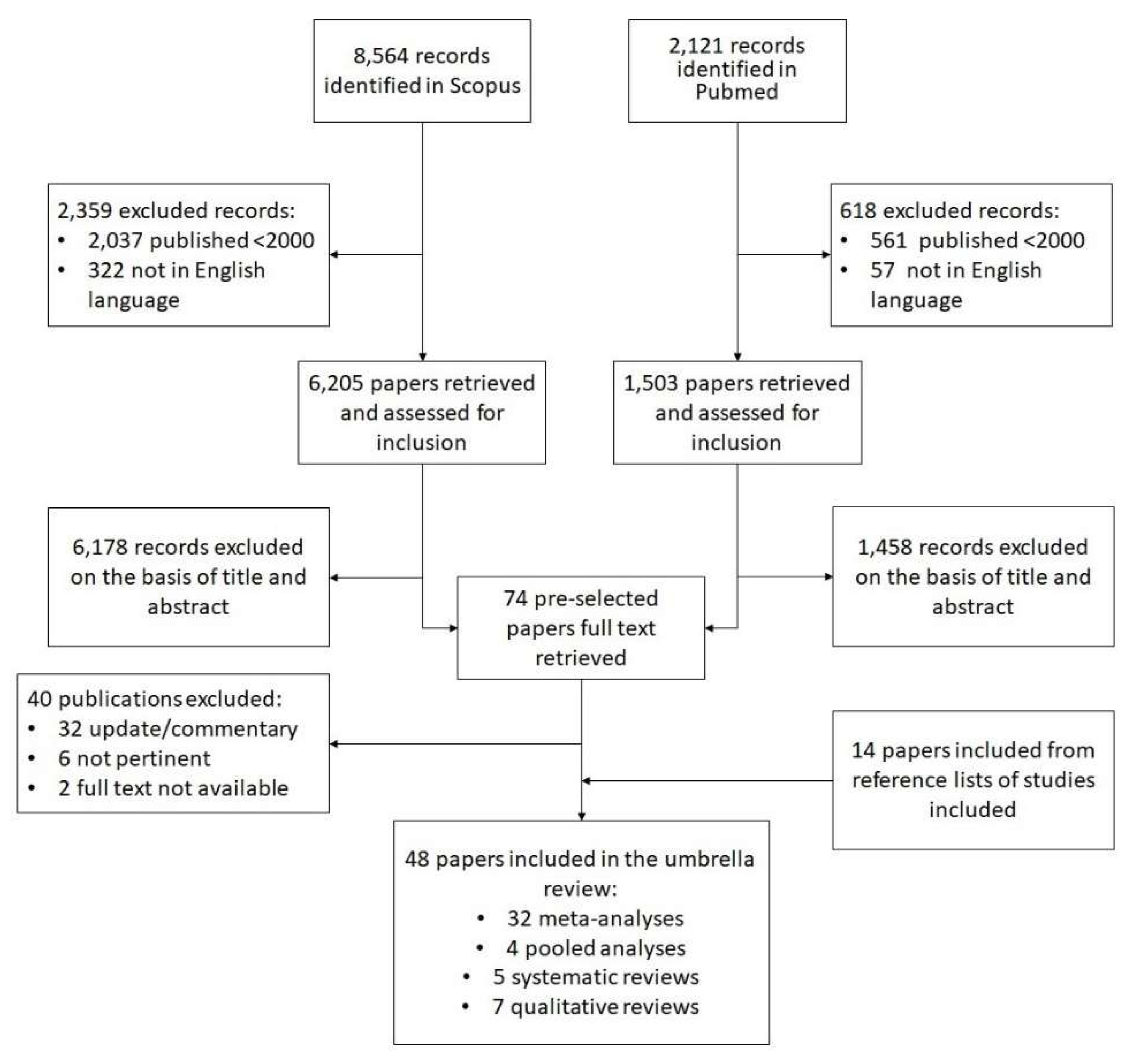
2.2. Sources
- General and descriptive reports, comments and updates without any reported association measures;
- Studies on populations or groups at increased risk;
- Analyses of dietary supplements or studies examining the combined effect of physical activity and diet;
- Studies involving BC recurrence;
- Studies written in languages other than Italian or English.
2.3. Data Extraction
2.4. Study Quality Assessment
3. Results
3.1. Dietary Patterns
3.2. Foods
3.3. Nutrients
4. Discussion
4.1. Dietary Patterns
4.2. Foods
4.3. Nutrients
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Tumore al Seno—Tumori AIRC. Available online: http://www.airc.it/tumori/tumore-al-seasp (accessed on 31 August 2017).
- Schütze, M.; Boeing, H.; Pischon, T.; Rehm, J.; Kehoe, T.; Gmel, G.; Olsen, A.; Tjønneland, A.M.; Dahm, C.C.; Overvad, K.; et al. Alcohol attributable burden of incidence of cancer in eight European countries based on results from prospective cohort study. BMJ 2011, 342, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Sieri, S.; Chiodini, P.; Agnoli, C.; Pala, V.; Berrino, F.; Trichopoulou, A.; Benetou, V.; Vasilopoulou, E.; Sánchez, M.J.; Chirlaque, M.; et al. Dietary fat intake and development of specific breast cancer subtypes. J. Natl. Cancer Inst. 2014, 106, 5. [Google Scholar] [CrossRef] [PubMed]
- Mattisson, E.; Wirfält, P.; Wallström, B.; Gullberg, H.O.L.; Berglund, G. High fat and alcohol intakes are risk factors of postmenopausal breast cancer: A prospective study from the Malmö diet and cancer cohort. Int. J. Cancer 2004, 110, 589–597. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.-X.; Ho, S.C.; Lin, F.-Y.; Chen, Y.-M.; Cheng, S.-Z.; Fu, J.-H. Dietary fat intake and risk of breast cancer: A case-control study in China. Eur. J. Cancer Prev. 2011, 20, 199–206. [Google Scholar] [CrossRef]
- Jansen, E.C.; Marin, C.; Mora-Plazas, M.; Villamor, E. Higher childhood red meat intake frequency is associated with earlier age at menarche. J. Nutr. 2016, 146, 792–798. [Google Scholar] [CrossRef]
- Varinska, L.; Gal, P.; Mojzisova, G.; Mirossay, L.; Mojzis, J. Soy and breast cancer: Focus on angiogenesis. Int. J. Mol. Sci. 2015, 16, 11728–11749. [Google Scholar] [CrossRef]
- Messina, M.; McCaskill-Stevens, W.; Lampe, J.W. Addressing the soy and breast cancer relationship: Review, commentary, and workshop proceedings. J. Natl. Cancer Inst. 2006, 98, 1275–1284. [Google Scholar] [CrossRef]
- Wu, H.; Yu, M.C.; Tseng, C.C.; Pike, M.C. Epidemiology of soy exposures and breast cancer risk. Br. J. Cancer 2008, 98, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Aromataris, E.; Fernandez, R.; Godfrey, C.M.; Holly, C.; Khalil, H.; Tungpunkom, P. Summarizing systematic reviews. Int. J. Evid. Based Healthc. 2015, 13, 132–140. [Google Scholar] [CrossRef]
- Aromataris, E.; Fernandez, R.; Godfrey, C.; Holly, C.; Khalil, H.; Tungpunkom, P. Methodology for JBI Umbrella Reviews. Joanna Briggs Inst. Rev. Man. 2014, 1–34. Available online: https://ro.uow.edu.au/cgi/viewcontent.cgi?article=4367&context=smhpapers (accessed on 29 June 2020).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D. PRISMA CHECKLIST. PLoS Med. 2009, 6, 7. [Google Scholar]
- Moher, D.; Altman, D.G.; Liberati, A.; Tetzlaff, J. PRISMA Statement. Epidemiology 2011, 22, 1. [Google Scholar] [CrossRef] [PubMed]
- Brennan, S.F.; Cantwell, M.M.; Cardwell, C.R.; Velentzis, L.S.; Woodside, J.V. Dietary patterns and breast cancer risk: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2010, 91, 1294–1302. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Hoffmann, G. Adherence to Mediterranean diet and risk of cancer: A systematic review and meta-analysis of observational studies. Int. J. Cancer 2014, 135, 1884–1897. [Google Scholar] [CrossRef]
- Männistö, S.; Dixon, L.B.; Balder, H.F.; Virtanen, M.J.; Krogh, V.; Khani, B.R.; Berrino, F.; van den Brandt, P.A.; Hartman, A.M.; Pietinen, P.; et al. Dietary patterns and breast cancer risk: Results from three cohort studies in the DIETSCAN project. Cancer Causes Control 2005, 16, 725–733. [Google Scholar] [CrossRef] [PubMed]
- Albuquerque, R.C.R.; Baltar, V.T.; Marchioni, D.M.L. Breast cancer and dietary patterns: A systematic review. Nutr. Rev. 2014, 72, 1–17. [Google Scholar] [CrossRef]
- Farsinejad-Marj, M.; Talebi, S.; Ghiyasvand, R.; Miraghajani, M. Adherence to Mediterranean diet and risk of breast cancer in premenopausal and postmenopausal women. Arch. Iran. Med. 2015, 18, 786–792. [Google Scholar]
- Guo, J.; Wei, W.; Zhan, L. Red and processed meat intake and risk of breast cancer: A meta-analysis of prospective studies. Breast Cancer Res. Treat. 2015, 151, 191–198. [Google Scholar] [CrossRef]
- Taylor, V.H.; Misra, M.; Mukherjee, S.D. Is red meat intake a risk factor for breast cancer among premenopausal women? Breast Cancer Res. Treat. 2009, 117, 1–8. [Google Scholar] [CrossRef]
- Mourouti, N.; Kontogianni, M.D.; Papavagelis, C.; Panagiotakos, D.B. Diet and breast cancer: A systematic review. Int. J. Food Sci. Nutr. 2015, 66, 1–42. [Google Scholar] [CrossRef]
- Missmer, S.A.; Smith-Warner, S.A.; Spiegelman, D.; Yaun, S.S.; Adami, H.O.; Beeson, W.L.; Van Den Brandt, P.A.; Fraser, G.E.; Freudenheim, J.L.; Goldbohm, R.A.; et al. Meat and dairy food consumption and breast cancer: A pooled analysis of cohort studies. Int. J. Epidemiol. 2002, 31, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Hanf, V.; Gonder, U. Nutrition and primary prevention of breast cancer: Foods, nutrients and breast cancer risk. Eur. J. Obstet. Gynecol. Reprod. Biol. 2005, 123, 139–149. [Google Scholar] [CrossRef] [PubMed]
- Gandini, S.; Merzenich, H.; Robertson, C.; Boyle, P. Meta-analysis of studies on breast cancer risk and diet: The role of fruit and vegetable consumption and the intake of associated micronutrients. Eur. J. Cancer 2000, 36, 636–646. [Google Scholar] [CrossRef]
- Si, R.; Qu, K.; Jiang, Z.; Yang, X.; Gao, P. Egg consumption and breast cancer risk: A meta-analysis. Breast Cancer 2014, 21, 251–261. [Google Scholar] [CrossRef]
- Dong, J.-Y.; Zhang, L.; He, K.; Qin, L.-Q. Dairy consumption and risk of breast cancer: A meta-analysis of prospective cohort studies. Breast Cancer Res. Treat. 2011, 127, 23–31. [Google Scholar] [CrossRef]
- Zang, J.; Shen, M.; Du, S.; Chen, T.; Zou, S. The association between dairy intake and breast cancer in western and Asian populations: A systematic review and meta-analysis. J. Breast Cancer 2015, 18, 313–322. [Google Scholar] [CrossRef]
- .Michels, K.B.; Mohllajee, P.A.; Roset-Bahmanyar, E.; Beehler, G.P.; Moysich, K.B. Diet and breast cancer: A review of the prospective observational studies. Cancer 2007, 109, 2712–2749. [Google Scholar] [CrossRef]
- Buck, K.; Zaineddin, A.K.; Vrieling, A.; Linseisen, J.; Chang-Claude, J. Meta-analyses of lignans and enterolignans in relation to breast cancer risk. Am. J. Clin. Nutr. 2010, 92, 141–153. [Google Scholar] [CrossRef]
- Dong, J.-Y.; Qin, L.-Q. Soy isoflavones consumption and risk of breast cancer incidence or recurrence: A meta-analysis of prospective studies. Breast Cancer Res. Treat. 2011, 125, 315–323. [Google Scholar] [CrossRef]
- Trock, B.J.; Leena, H.C.; Clarke, R. Meta-analysis of soy intake and breast cancer risk. J. Natl. Cancer Inst. 2006, 98, 459–471. [Google Scholar] [CrossRef]
- Velentzis, L.S.; Cantwell, M.M.; Cardwell, C.; Keshtgar, M.R.; Leathem, A.J.; Woodside, J.V. Lignans and breast cancer risk in pre- and post-menopausal women: Meta-analyses of observational studies. Br. J. Cancer 2009, 100, 1492–1498. [Google Scholar] [CrossRef]
- Wu, Y.-C.; Zheng, D.; Sun, J.-J.; Zou, Z.-K.; Ma, Z.-L. Meta-analysis of studies on breast cancer risk and diet in Chinese women. Int. J. Clin. Exp. Med. 2015, 8, 73–85. [Google Scholar] [PubMed]
- Mourouti, N.; Panagiotakos, D.B. Soy food consumption and breast cancer. Maturitas 2013, 76, 118–122. [Google Scholar] [CrossRef] [PubMed]
- Duffy, C.; Perez, K.; Partridge, A. Implications of phytoestrogen intake for breast cancer. Cancer J. Clin. 2007, 57, 60–277. [Google Scholar] [CrossRef] [PubMed]
- Lof, M.; Weiderpass, E. Epidemiologic evidence suggests that dietary phytoestrogen intake is associated with reduced risk of breast, endometrial, and prostate cancers. Nutr. Res. 2006, 26, 609–619. [Google Scholar] [CrossRef]
- Peeters, P.H.M.; Keinan-Boker, L.; van der Schouw, Y.T.; Grobbee, D.E. Phytoestrogens and breast cancer risk. Breast Cancer Res. Treat. 2003, 77, 71–183. [Google Scholar] [CrossRef]
- Aune, D.; Chan, D.S.; Greenwood, D.C.; Vieira, A.R.; Rosenblatt, D.A.; Vieira, R.; Norat, T. Dietary fiber and breast cancer risk: A systematic review and meta-analysis of prospective studies. Ann. Oncol. 2012, 23, 1394–1402. [Google Scholar] [CrossRef]
- Smith-Warner, S.A.; Spiegelman, D.; Yaun, S.S.; Adami, H.O.; Beeson, W.L.; van den Brandt, P.A.; Folsom, A.R.; Fraser, G.E.; Freudenheim, J.L.; Goldbohm, R.A.; et al. Intake of fruits and vegetables and risk of breast cancer a pooled analysis of cohort studies. J. Am. Med. Assoc. 2001, 285, 769–776. [Google Scholar] [CrossRef]
- Song, J.K.; Bae, J.M. Citrus fruit intake and breast cancer risk: A quantitative systematic review. J. Breast Cancer 2013, 16, 72–76. [Google Scholar] [CrossRef]
- Li, J.; Zou, L.; Chen, W.; Zhu, B.; Shen, N.; Ke, J.; Lou, J.; Song, R.; Zhong, R.; Miao, X. Dietary mushroom intake may reduce the risk of breast cancer: Evidence from a meta-analysis of observational studies. PLoS ONE 2014, 9, e93437. [Google Scholar] [CrossRef]
- Seely, D.; Mills, E.J.; Wu, P.; Verma, S.; Guyatt, G.H. The effects of green tea consumption on incidence of breast cancer and recurrence of breast cancer: A systematic review and meta-analysis. Integr. Cancer Ther. 2005, 4, 144–155. [Google Scholar] [CrossRef] [PubMed]
- Alexander, D.D.; Morimoto, L.M.; Mink, P.J.; Lowe, K.A. Summary and meta-analysis of prospective studies of animal fat intake and breast cancer. Nutr. Res. Rev. 2010, 23, 169–179. [Google Scholar] [CrossRef] [PubMed]
- Boyd, N.F.; Stone, J.; Vogt, K.N.; Connelly, B.S.; Martin, L.J.; Minkin, S. Dietary fat and breast cancer risk revisited: A meta-analysis of the published literature. Br. J. Cancer 2003, 89, 1672–1685. [Google Scholar] [CrossRef] [PubMed]
- Turner, L.B. A meta-analysis of fat intake, reproduction, and breast cancer risk: An evolutionary perspective. Am. J. Hum. Biol. 2011, 23, 601–608. [Google Scholar] [CrossRef] [PubMed]
- Smith-Warner, S.A.; Spiegelman, D.; Adami, H.O.; Beeson, W.L.; van den Brandt, P.A.; Folsom, A.R.; Fraser, G.E.; Freudenheim, J.L.; Goldbohm, R.A.; Graham, S.; et al. Types of dietary fat and breast cancer: A pooled analysis of cohort studies. Int. J. Cancer 2001, 92, 767–774. [Google Scholar] [CrossRef]
- Mulholland, H.G.; Murray, L.J.; Cardwell, C.R.; Cantwell, M.M. Dietary glycaemic index, glycaemic load and breast cancer risk: A systematic review and meta-analysis. Br. J. Cancer 2008, 99, 1170–1175. [Google Scholar] [CrossRef] [PubMed]
- Mullie, P.; Koechlin, A.; Boniol, M.; Autier, P.; Boyle, P. Critical reviews in food science and nutrition relation between breast cancer and high glycemic index or glycemic load: A meta-analysis of prospective cohort studies relation between breast cancer and high glycemic index or glycemic load. Crit. Rev. Food Sci. Nutr. 2016, 56, 152–159. [Google Scholar] [CrossRef] [PubMed]
- Yang, B.; Ren, X.-L.; Fu, Y.-Q.; Gao, J.-L.; Li, D. Ratio of n-3/n-6 PUFAs and risk of breast cancer: A meta-analysis of 274135 adult females from 11 independent prospective studies. BMC Cancer 2014, 14, 105. [Google Scholar] [CrossRef]
- Zheng, J.-S.; Hu, X.-J.; Zhao, Y.-M.; Yang, J.; Li, D. Intake of fish and marine n-3 polyunsaturated fatty acids and risk of breast cancer: Meta-analysis of data from 21 independent prospective cohort studies. BMJ 2013, 346, F3706. [Google Scholar] [CrossRef]
- Zhou, Y.; Wang, T.; Zhai, S.; Li, W.; Meng, Q. Linoleic acid and breast cancer risk: A meta-analysis. Public Health Nutr. 2015, 19, 1457–1463. [Google Scholar] [CrossRef]
- Chen, P.; Hu, P.; Xie, D.; Qin, Y.; Wang, F.; Wang, H. Meta-analysis of vitamin D, calcium and the prevention of breast cancer. Breast Cancer Res. Treat. 2010, 121, 469–477. [Google Scholar] [CrossRef] [PubMed]
- Gissel, T.; Rejnmark, L.; Mosekilde, L.; Vestergaard, P. Intake of vitamin D and risk of breast cancer—A. meta-analysis. J. Steroid Biochem. Mol. Biol. 2008, 111, 195–199. [Google Scholar] [CrossRef] [PubMed]
- Cui, Y.; Rohan, T.E. Vitamin D, calcium, and breast cancer risk: A review. Cancer Epidemiol. Biomark. Prev. 2006, 15, 1427–1437. [Google Scholar] [CrossRef]
- Chen, P.; Li, C.; Li, X.; Li, J.; Chu, R.; Wang, H. Higher dietary folate intake reduces the breast cancer risk: A systematic review and meta-analysis. Br. J. Cancer 2014, 110, 2327–2338. [Google Scholar] [CrossRef]
- Larsson, S.C.; Giovannucci, E.; Wolk, A. Folate and risk of breast cancer: A. meta-analysis. J. Natl. Cancer Inst. 2007, 99, 64–76. [Google Scholar] [CrossRef]
- Eichholzer, M.; Lüthy, J.; Moser, U.; Fowler, B. Folate and the risk of colorectal, breast and cervix cancer: The epidemiological evidence. Swiss Med. Wkly. 2001, 131, 539–549. [Google Scholar] [PubMed]
- Hui, C.; Qi, X.; Qianyong, Z.; Xiaoli, P.; Jundong, Z.; Mantian, M. Flavonoids, flavonoid subclasses and breast cancer risk: A meta-analysis of epidemiologic studies. PLoS ONE 2013, 8, e54318. [Google Scholar] [CrossRef]
- Hu, F.; Wang Yi, B.; Zhang, W.; Liang, J.; Lin, C.; Li, D.; Wang, F.; Pang, D.; Zhao, Y. Carotenoids and breast cancer risk: A meta-analysis and meta-regression. Breast Cancer Res. Treat. 2012, 131, 239–253. [Google Scholar] [CrossRef]
- Rossi, R.E.; Pericleous, M.; Mandair, D.; Whyand, T.; Caplin, M.E. The role of dietary factors in prevention and progression of breast cancer. Anticancer Res. 2014, 34, 6861–6875. [Google Scholar]
- van den Brandt, P.A.; Schulpen, M. Mediterranean diet adherence and risk of postmenopausal breast cancer: Results of a cohort study and meta-analysis. Int. J. Cancer 2017, 140, 2220–2231. [Google Scholar] [CrossRef]
- Campbell, K.L.; Foster-Schubert, K.E.; Alfano, C.M.; Wang, C.C.; Wang, C.Y.; Duggan, C.R.; Mason, C.; Imayama, I.; Kong, A.; Xiao, L. Reduced-calorie dietary weight loss, exercise, and sex hormones in postmenopausal women: Randomized controlled trial. J. Clin. Oncol. 2012, 30, 2314–2326. [Google Scholar] [CrossRef] [PubMed]
- Pasanisi, P.; Berrino, F.; de Petris, M.; Venturelli, E.; Mastroianni, A.; Panico, S. Metabolic syndrome as a prognostic factor for breast cancer recurrences. Int. J. Cancer 2006, 119, 236–238. [Google Scholar] [CrossRef] [PubMed]
- Frank, L.L.; Sorensen, B.E.; Yasui, Y.; Tworoger, S.S.; Schwartz, R.S.; Ulrich, C.M.; Irwin, M.L.; Rudolph, R.E.; Rajan, K.B.; Stanczyk, F.; et al. Effects of exercise on metabolic risk variables in overweight postmenopausal women: A randomized clinical trial. Obes. Res. 2005, 13, 615–625. [Google Scholar] [CrossRef] [PubMed]
- McTiernan, A.; Tworoger, S.S.; Ulrich, C.M.; Yasui, Y.; Irwin, M.L.; Rajan, K.B.; Sorensen, B.; Rudolph, R.E.; Bowen, D.; Stanczyk, F.Z. Effect of exercise on serum estrogens in postmenopausal women: A 12-month randomized clinical trial. Cancer Res. 2004, 64, 2923–2928. [Google Scholar] [CrossRef]
- Trichopoulou, C.; Bamia, P.L.; Trichopoulos, D. Conformity to traditional Mediterranean diet and breast cancer risk in the Greek EPIC (European Prospective Investigation into Cancer and Nutrition) cohort. Am. J. Clin. Nutr. 2010, 92, 620–625. [Google Scholar] [CrossRef]
- Sieri, S.; Krogh, V.; Pala, V.; Muti, P.; Micheli, A.; Evangelista, A.; Tagliabue, G.; Berrino, F. Dietary patterns and risk of breast cancer in the ORDET cohort. Cancer Epidemiol. Biomark. Prev. 2004, 13, 567–572. [Google Scholar]
- Murtaugh, M.A.; Sweeney, C.; Giuliano, A.R.; Herrick, J.S.; Hines, L.; Byers, T.; Baumgartner, K.B.; Slattery, M.L. Diet patterns and breast cancer risk in Hispanic and non-Hispanic white women: The Four-Corners Breast Cancer Study. Am. J. Clin. Nutr. 2008, 87, 978–984. [Google Scholar] [CrossRef]
- Wu, H.; Yu, M.C.; Tseng, C.-C.; Stanczyk, F.Z.; Pike, M.C. Dietary patterns and breast cancer risk in Asian American women. Am. J. Clin. Nutr. 2009, 89, 1145–1154. [Google Scholar] [CrossRef]
- Rose, D.P.; Goldman, M.; Connolly, J.M.; Strong, L.E. High-fiber diet reduces serum estrogen concentrations in premenopausal women. Am. J. Clin. Nutr. 1991, 54, 520–525. [Google Scholar] [CrossRef]
- Surh, Y.-J. Cancer chemoprevention with dietary phytochemicals. Nat. Rev. Cancer 2003, 3, 768–780. [Google Scholar] [CrossRef]
- Berrino, F. Il Cibo dell’Uomo. La Via della Salute tra Conoscenza Scientifica e Antiche Saggezze; Franco Angeli: Milan, Italy, 2015. [Google Scholar]
- Masala, G.; Assedi, M.; Bendinelli, B.; Ermini, I.; Sieri, S.; Grioni, S.; Sacerdote, C.; Ricceri, F.; Panico, S.; Mattiello, A.; et al. Fruit and vegetables consumption and breast cancer risk: The EPIC Italy study. Breast Cancer Res. Treat. 2012, 132, 1127–1136. [Google Scholar] [CrossRef]
- Ribaya-Mercado, J.D.; Blumberg, J.B. Lutein and zeaxanthin and their potential roles in disease prevention. J. Am. Coll. Nutr. 2004, 23, 567S–587S. [Google Scholar] [CrossRef] [PubMed]
- Allegro, G.; Villarini, A. Prevenire i Tumori Mangiando con Gusto; Sperling & Kupfer: Milan, Italy, 2013. [Google Scholar]
- Wasser, S. Medicinal mushrooms as a source of antitumor and immunomodulating polysaccharides. Appl. Microbiol. Biotechnol. 2003, 60, 258–274. [Google Scholar]
- Rohrmann, S.; Overvad, K.; Bueno-de-Mesquita, H.B.; Jakobsen, M.U.; Egeberg, R.; Tjønneland, A.; Nailler, L.; Boutron-Ruault, M.C.; Clavel-Chapelon, F.; Krogh, V.; et al. Meat consumption and mortality—Results from the European Prospective Investigation into Cancer and Nutrition. BMC Med. 2013, 11, 63. [Google Scholar] [CrossRef]
- Ferretti, G.; Bacchetti, T.; Nègre-Salvayre, A.; Salvayre, R.; Dousset, N.; Curatola, G. Structural modifications of HDL and functional consequences. Atherosclerosis 2006, 184, 1–7. [Google Scholar] [CrossRef]
- Aune, D.; De Stefani, E.; Ronco, A.L.; Boffetta, P.; Deneo-Pellegrini, H.; Acosta, G.; Mendilaharsu, M. Egg consumption and the risk of cancer: A multisite case-control study in Uruguay. Asian Pacific J. Cancer Prev. 2009, 10, 869–876. [Google Scholar]
- Li, F.; Zhou, Y.; Hu, R.T.; Hou, L.N.; Du, Y.J.; Zhang, X.J.; Olkkonen, V.M.; Tan, W.L. Egg consumption and risk of bladder cancer: A meta-analysis. Nutr. Cancer 2013, 65, 538–546. [Google Scholar] [CrossRef]
- Lu, L.J.; Anderson, K.E.; Grady, J.J.; Nagamani, M. Effects of soya consumption for one month on steroid hormones in premenopausal women: Implications for breast cancer risk reduction. Cancer Epidemiol. Prev. Biomark. 1996, 5, 63–70. [Google Scholar]
- Lu, L.-J.W.; Anderson, K.E.; Grady, J.J.; Kohen, F.; Nagamani, M. Decreased ovarian hormones during a soya diet: Implications for breast cancer prevention. Cancer Res. 2000, 60, 4112–4121. [Google Scholar]
- Bartolozzi, G. Fisiopatologia della vitamina D (seconda parte). Medico. E. Bambino. Pagine. Elettron. 2007, 10, 1–3. [Google Scholar]
- Pasanisi, P.; Bruno, E.; Venturelli, E.; Manoukian, S.; Barile, M.; Peissel, B.; De Giacomi, C.; Bonanni, B.; Berrino, J.; Berrino, F. Serum levels of IGF-I and BRCA penetrance: A case control study in breast cancer families. Fam. Cancer 2011, 10, 521–528. [Google Scholar] [CrossRef] [PubMed]
- Norat, T.; Dossus, L.; Rinaldi, S.; Overvad, K.; Grønbaek, H.; Tjønneland, A.; Olsen, A.; Clavel-Chapelon, F.; Boutron-Ruault, M.C.; Boeing, H. Diet, serum insulin-like growth factor-I and IGF-binding protein-3 in European women. Eur. J. Clin. Nutr. 2007, 61, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Qin, L.-Q.; He, K.; Xu, J.-Y. Milk consumption and circulating insulin-like growth factor-I level: A systematic literature review. Int. J. Food Sci. Nutr. 2009, 60, 330–340. [Google Scholar] [CrossRef] [PubMed]
- Silalahi, J. Anticancer and health protective properties of citrus fruit components. Asia Pac. J. Clin. Nutr. 2007, 11, 79–84. [Google Scholar] [CrossRef]
- Boeke, C.E.; Tamimi, R.M.; Berkey, C.S.; Colditz, G.A.; Eliassen, A.H.; Malspeis, S.; Willett, W.C.; Frazier, A.L. Adolescent carotenoid intake and benign breast disease. Pediatrics 2014, 133, 1–7. [Google Scholar] [CrossRef]
- Cui, Y.; Lu, Z.; Bai, L.; Shi, Z.; Zhao, W.e.; Zhao, B. β-Carotene induces apoptosis and up-regulates peroxisome proliferator-activated receptor γ expression and reactive oxygen species production in MCF-7 cancer cells. Eur. J. Cancer 2007, 43, 2590–2601. [Google Scholar] [CrossRef]
- Hui, C.; Yujie, F.; Lijia, Y.; Long, Y.; Hongxia, X.; Yong, Z.; Jundong, Z.; Qianyong, Z.; Mantian, M. MicroRNA-34a and microRNA-21 play roles in the chemopreventive effects of 3,6-dihydroxyflavone on 1-methyl-1-nitrosourea-induced breast carcinogenesis. Breast Cancer Res. 2012, 14, R80. [Google Scholar] [CrossRef]
- Zhang, S.; Yang, X.; Coburn, R.A.; Morris, M.E. Structure activity relationships and quantitative for the flavonoid-mediated inhibition of breast cancer resistance protein. Biochem. Pharmacol. 2005, 70, 627–639. [Google Scholar] [CrossRef]
- Neuhouser, M.L. Review. Dietary flavonoids and cancer risk: Evidence from human population studies. Nutr. Cancer 2004, 50, 16–22. [Google Scholar] [CrossRef]
- Ross, J.A.; Kasum, C.M. Dietary flavonoids: Bioavailability, metabolic effects, and safety. Annu. Rev. Nutr. 2002, 22, 19–34. [Google Scholar] [CrossRef]
- Papa, V.; Belfiore, A. Insulin receptors in breast cancer: Biological and clinical role. J. Endocrinol. Investig. 1994, 19, 324–333. [Google Scholar] [CrossRef] [PubMed]
- Laamiri, F.Z.; Otmani, A.; Ahid, S.; Barkat, A. Lipid profile among Moroccan overweight women and breast cancer: A case-control study. Int. J. Gen. Med. 2013, 6, 439–445. [Google Scholar]
- Sieri, S.; Krogh, V.; Ferrari, P.; Berrino, F.; Pala, V.; Thiébaut, A.C.; Tjønneland, A.; Olsen, A.; Overvad, K.; Jakobsen, M.U.; et al. Dietary fat and breast cancer risk in the European Prospective Investigation into Cancer and Nutrition. Am. J. Clin. Nutr. 2008, 88, 1304–1312. [Google Scholar] [PubMed]
- Armstrong, B.; Doll, R. Environmental factors and cancer incidence and mortality in different countries, with special reference to dietary practices. Int. J. Cancer 1975, 15, 617–631. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Obesity and Overweight. Global Strategy on Diet, Physical Activity and Health. Available online: https://www.who.int/dietphysicalactivity/publications/obesity/en/ (accessed on 29 June 2020).
- Golay, A.; Bobbioni, E. The role of dietary fat in obesity. Int. J. Obes. Relat. Metab. Disord. 1997, 21, S2–S11. [Google Scholar] [PubMed]
- Astrup, A.; Buemann, B.; Western, P.; Toubro, S.; Raben, A.; Christensen, N.J. Obesity as an adaptation to a high-fat diet: Evidence from a cross-sectional study. Am. J. Clin. Nutr. 1994, 59, 350–355. [Google Scholar] [CrossRef]
- Jequier, E. Pathways to obesity. Int. J. Obes. 2002, 26, S18–S27. [Google Scholar] [CrossRef] [PubMed]
- Hill, J.O.; Melanson, E.L.; Wyatt, H.T. Dietary fat intake and regulation of energy balance: Implications for obesity. J. Nutr. 2000, 130, 284S–288S. [Google Scholar] [CrossRef]
- Bray, G.A.; Popkin, B.M. Dietary fat intake does affect obesity! Am. J. Clin. Nutr. 1998, 68, 1157–1173. [Google Scholar] [CrossRef] [PubMed]
- Schrauwen, P.; Westerterp, K.R. The role of high-fat diets and physical activity in the regulation of body weight. Br. J. Nutr. 2000, 84, 417–427. [Google Scholar] [CrossRef] [PubMed]
- Larsson, S.C.; Wolk, A. Excess body fatness: An important cause of most cancers. Lancet 2008, 371, 536–537. [Google Scholar] [CrossRef]
- Dossus, L.; Kaaks, R. Nutrition, metabolic factors and cancer risk. Best Pract. Res. Clin. Endocrinol. Metab. 2008, 22, 551–571. [Google Scholar] [CrossRef]
- Key, T.J.; Allen, N.E.; Spencer, E.A.; Travis, R.C. Nutrition and breast cancer. The Breast 2003, 12, 412–416. [Google Scholar] [CrossRef]
- Lahmann, P.H.; Lissner, L.; Berglund, G. Breast cancer risk in overweight postmenopausal women. Cancer Epidemiol. Prev. Biomark. 2004, 13, 8. [Google Scholar]
- Murff, H.J.; Shu, X.O.; Li, H.; Yang, G.; Wu, X.; Cai, H.; Wen, W.; Gao, Y.T.; Zheng, W. Dietary polyunsaturated fatty acids and breast cancer risk in Chinese women: A prospective cohort study. Int. J. Cancer 2011, 128, 1434–1441. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Ma, D.W.L. The role of n-3 polyunsaturated fatty acids in the prevention and treatment of breast cancer. Nutrients 2014, 6, 5184–5223. [Google Scholar] [CrossRef]
- Corso, G.; Maisonneuve, P.; Massari, G.; Invento, A.; Pravettoni, G.; De Scalzi, A.; Intra, M.; Galimberti, V.; Morigi, C.; Lauretta, M.; et al. Validation of a Novel Nomogram for Prediction of Local Relapse after Surgery for Invasive Breast Carcinoma. Ann. Surg. Oncol. 2020, 27, 1864–1874. [Google Scholar] [CrossRef] [PubMed]
- World Cancer Research Fund/American Institute for Cancer Research. Diet, Nutrition, Physical Activity and Breast Cancer. Continuous Update Project Expert Report. 2018. Available online: https://www.wcrf.org/sites/default/files/Summary-of-Third-Expert-Report-2018.pdf (accessed on 29 June 2020).


{kind=link}
| Author_ Year | Continent or Region, n. of Studies | Search Range Applied | Total n. of Studies Included in the Review | Total Sample Size of all Studies Included in the Review | Type of Study | Study Design | Association/s Examined |
|---|---|---|---|---|---|---|---|
| Characteristics of meta-analyses included in the umbrella review (32) | |||||||
| Alexander 2010 [43] | // | up to 2008 | 11 studies referring to 6 cohort studies | // | meta-analysis and review of epidemiological cohort studies | 6 cohort studies | animal fat intake and breast cancer (BC) |
| Aune 2012 [38] | 9 studies in America, 6 in Europe and 1 in Asia | from January 2006 to 31 August 2011 | 16 prospective studies (17 publications) | 26,523 cases among 999,271 participants | systematic review and meta-analysis | 16 cohort studies | high vs. low dietary fiber intake and BC risk |
| Boyd 2003 [44] | 22 studies in Europe (including Russia), 15 in North America, 5 in Asia, 2 in Australia and 1 in South America (Uruguay) | from January 1966 to July 2003 | 45 studies | 16,280 BC cases and 18,966 controls in case-control studies; 8735 BC cases out of 568,549 participants (total 25,015 BC cases and 580,000 controls) | meta-analysis of the published literature | 31 case-control studies and 14 prospective studies (cohort and nested case-control studies) | dietary fat and BC risk |
| Brennan 2010 [14] | 7 studies in North America, 5 in Europe, 2 in South America (Uruguay), 2 in Asia | up to November 2009 | 16 articles | 13,885 BC cases out of 465,891 participants in cohort studies; 10,746 BC cases and 34,311 controls in case-control studies | systematic review and meta-analysis | 8 case-control and 8 cohort studies | dietary patterns and BC risk |
| Buck 2010 [29] | 16 studies in Europe, 6 in North America 1 in Asia and 1 in Australia | from 1997 to August 2009 | 24 articles, including 21 studies (all on lignan exposures—9 studies on calculated dietary plant lignans) | 21,159 BC cases among 188,302 participants overall | meta-analysis | 11 cohort studies and 10 case-control studies | lignans and BC risk |
| Chen 2010 [52] | // | up to July 2009 | 11 studies on vitamin D intake and 15 on calcium intake (26 studies in all) | // | meta-analysis | 5 case-control and 6 cohort studies on vitamin D intake; 9 case-control and 6 cohort studies on calcium intake | vitamin D and calcium intake on BC risk |
| Chen 2014 [55] | 20 studies in North America,10 in Europe, 9 in Asia, 1 in Australia, 1 in China 1 in Brazil | up to January 2014 | 50 eligible studies, 42 of which reported on folate intake and breast cancer | 26,205 BC cases out of 744,068 participants in prospective studies; 16,826 BC cases and 21,820 controls in case-control studies | systematic review and meta-analysis | 16 prospective studies (14 cohort and 2 nested case-control) on folate intake; 26 case-control studies on folate intake (8 studies on blood folate levels) | folate intake and overall BC risk |
| Dong 2011 (a) [29] | 8 studies in Europe, 4 studies in Asia, 2 studies in USA | up to September 2010 | 14 studies on BC incidence | 369,934 participants and 5828 cases of BC | meta-analysis of prospective studies (nested case-control and cohort studies) | 6 nested case control studies and 8 cohort studies | soy isoflavone consumption and BC risk |
| Dong 2011 (b) [25] | 9 studies in USA, 8 in Europe, 1 in Japan | up to January 2011 | 18 studies | 24,187 BC cases and 1,063,471 participants | meta-analysis of prospective studies (nested case-control and cohort studies) | 18 cohort studies; 12 studies on total dairy food intake and 13 on milk intake | dairy product consumption and BC risk |
| Gandini 2000 [38] | 14 studies in Europe, 8 in North America, 3 in Asia, 1 in Australia | 1982–1999 | 26 studies focusing on vegetables (17), fruits (13), beta-carotene (11) and vitamin C (9) | 23,038 cases in all | meta-analysis | 5 cohort studies and 21 case-control studies | consumption of fruit and vegetables, and associated micronutrients, and risk of BC |
| Gissel 2008 [53] | // | up to June 2007 | 6 studies | 78,712 women | meta-analysis | epidemiological studies (cross-sectional, case-control, or cohort) and randomized controlled trials (RCTs) | vitamin D intake and BC |
| Guo 2015 [19] | 6 studies in the USA, 6 in Europe, 1 in North America and Western Europe, and 1 in Asia | up to October 2014 | 14 prospective studies | 1,588,890 participants and 31,552 BC cases | meta-analysis | 14 cohort/nested case-control studies | red meat and processed meat consumption and BC risk |
| Hu 2012 [59] | // | January 1982–May 2011 | 33 studies | // | meta-analysis and meta-regression | 24 case-control studies, 1 nested case-control study, 2 case-cohort studies and 6 cohort studies | carotenoids and BC risk |
| Hui 2013 [58] | 5 studies in Europe, 5 in North America (4 in the USA) and 2 in Asia (China) | up to July 2012 | 12 studies included | 9513 cases and 181,906 controls | meta-analysis of epidemiological studies | 6 cohort studies, 6 case-control studies | flavonoids, flavonoid subclasses and BC risk |
| Larsson 2007 [56] | 12 studies in North America (10 in the USA), 7 in Europe, 2 in Asia, 1 in South America (Uruguay) and 1 in Australia | from January 1966 to November 2006 | 23 studies (21 assessing dietary folate intake) | 8367 BC cases out of 302,959 participants in cohort studies; 8558 BC cases and 10,812 control subjects in case-control studies | meta-analysis | 9 cohort studies and 14 case-control studies | dietary folate intake and BC risk |
| Li 2014 [41] | 8 case-control studies in Asia, 2 cohort studies in Europe | up to 2013 | 7 articles including 10 studies | 2313 BC cases and 2387 controls in case-control studies; 4577 cases among 1,748,623 follow-up person/years | meta-analysis | 2 cohort and 8 case-control studies | dietary mushroom intake and BC risk |
| Mulholland 2008 [47] | 8 studies in North-Central America, 5 in Europe and 1 Australia | up to May 2008 | 14 studies | 17,673 BC cases out of 492,011 participants | systematic review and meta-analysis | 10 cohort, 4 case-control studies | dietary glycemic index, glycemic load and BC risk |
| Mullie 2016 [48] | 6 studies in North America, 4 in Europe, 1 in Australia and 1 in China | up to December 2011 | 12 studies | 20,973 BC cases out of 773,971 subjects | meta-analysis of prospective cohort studies | 12 cohort studies | high glycemic index, glycemic load and BC risk |
| Schwingshackl 2014 [15] | 7 studies in Europe, 4 in North America | up to January 2014 | 11 studies on BC risk | 489,109 participants in cohort studies; 4990 BC cases and 5446 controls in case-control studies | systematic review and meta-analysis | 5 case-control and 6 cohort studies | Mediterranean diet and BC risk |
| Seely 2005 [42] | 4 studies in Asian populations (Japanese, Chinese or Filipino) in Asia, 1 in Asian populations of the USA | from 1966 to November 2004 | 7 studies (5 prevention studies examining risk of primary BC and green tea consumption) | 857 primary BC cases and 1519 controls in case-control studies; 115,601 participants in cohort studies | systematic review and meta-analysis | 3 cohort studies and 2 case-control studies | green tea consumption and BC risk |
| Si 2014 [25] | 5 studies in Asia, 4 in Europe, 2 in the USA, 1 in South America and 1 in both Europe and America | up to February 2013 | 13 studies | 19,280 BC cases among 811,555 participants in cohort studies; 13,949 cases and 37,883 controls in case-control studies | meta-analysis | 5 cohort studies and 8 case-control studies | egg consumption and BC risk |
| Song 2013 [40] | 3 studies in China, 2 in the USA, 1 in Australia | up to January 2012 | 6 studies | 8393 participants: 3789 cases and 4705 controls | quantitative systematic review and meta-analysis | 6 case-control studies | association between citrus fruit intake and BC risk |
| Taylor 2009 [20] | 5 studies in North America, 2 in Europe, 2 in Asia and 1 in South America | from 1966 to 2009 | 10 studies | 1842 BC cases and 2124 controls in case-control studies; 2024 BC cases among 192,627 participants in cohort studies | meta-analysis | 6 case-control studies, 1 nested case-control and 3 cohort studies | red meat intake and BC risk |
| Trock 2006 [31] | 8 studies in Asian populations and 10 in Western populations | from 1978 to 2004 | 18 studies | 9182 BC cases | meta-analysis | 12 case-control and 6 cohort or nested case-control studies | soy intake and BC risk |
| Turner 2011 [45] | 25 studies in North America (USA), 18 in Europe, 2 in South America (Uruguay), 6 in Asia, and 1 in Australia | up to May 2010 | 52 studies | 44,070 BC cases among 1,659,913 participants/controls | meta-analysis | 25 cohort studies and 27 case-control studies | fat intake and BC risk |
| Velentzis 2009 [32] | 6 studies conducted in North America, 6 in Europe | up to September 2008 | 23 studies, 12 of them on plant lignan intake | 12,430 BC cases among 258,984 participants | meta-analyses | 5 cohort and 7 case-control studies | lignans and BC risk |
| Wu 2008 [9] | 8 studies in Asia and Asian Americans, 11 in Western populations | // | 19 studies | // | meta-analysis | 14 case-control studies and 5 cohort/nested case-control studies | soy exposure and BC risk |
| Wu 2015 [33] | All studies on Chinese populations | up to June 2013 | 22 studies | 23,201 subjects: 10,566 in the experimental group (cases) and 12,635 controls | systematic review and meta-analysis | 21 case-control studies and 1 cohort study | dietary factors and BC risk |
| Yang 2014 [49] | 4 studies in the USA, 5 in Europe and 2 in Asia | up to April 2013 | 11 prospective studies | 8331 BC events among 274,135 adult women | meta-analysis | 6 nested case-control studies and 5 cohort studies | n-3/n-6 PUFAs and risk of BC |
| Zang 2015 [27] | 11 cohort studies in the USA, 10 in Europe, 1 in Japan; 5 case-control studies in Asia | up to January 2014 | 27 studies | 37,925 BC cases among 1,566,940 participants in cohort studies and 7418 incident BC cases among 33,372 participants in case-control studies | systematic review and meta-analysis | 22 cohort studies and 5 case-control studies | dairy intake and BC |
| Zheng 2013 [50] | 11 studies in USA, 11 in Europe and 4 in Asia | up to December 2012 | 26 publications on 21 prospective studies: (14 on fish intake and 19 on marine n-3 PUFA) | 20,905 BC cases and 883,585 participants | meta-analysis | 26 cohort studies (8 nested case-control and 2 case-cohort studies) | intake of fish and marine omega-3 polyunsaturated fatty acids (n-3 PUFA)and risk of BC |
| Zhou 2015 [51] | 6 studies in Europe, 5 in the USA and 1 in Asia (China) | up to November 2014 | 12 studies, 2 of which reported two separate outcomes (pre- and post-menopausal), for a total of 14 outcomes included in the meta-analysis | 10,410 BC events among 358,955 adult females | meta-analysis | 8 cohort studies and 4 nested case-control studies | linoleic acid and BC risk |
| Characteristics of pooled analyses included in the umbrella review (4) | |||||||
| Mannisto 2005 [16] | // | 3 cohort studies | 77,037 participants and 3271 BC cases | pooled analysis | 3 cohort studies in the DIETSCAN project: Netherlands Cohort Study on diet and cancer (NCLS), the Italian “Ormoni e Dieta nella Eziologia dei Tumori”(ORDET) and the Swedish Mammography Cohort (SMC) | dietary pattern and BC risk | |
| Missmer 2002 [22] | North America and Western Europe | // | 8 studies | 7379 BC cases out of 351,041 women | pooled analysis | 8 cohort studies | meat and dairy food consumption and risk of BC |
| Smith-Warner 2001 (a) [46] | 7 studies in North America, 2 in Europe | up to 2001 | 8 studies (9 in all, because the Nurse’s Health Study was divided in two) | 7329 BC cases out of 351,821 participants | pooled analysis of cohort studies | pooling project: 9 prospective studies (8 analyzed as nested case-control studies, 1 used a case-cohort design) | types of dietary fat and BC risk |
| Smith-Warner 2001 (b) [39] | 7 studies in North America, 2 in Europe | up to 2001 | 8 studies (9 in all, because the Nurse’s Health Study was divided in two) | 7377 incident BC cases among 351,825 participants | pooled analysis of cohort studies | pooling project: 9 prospective studies (8 analyzed as nested case-control studies, 1 used a case-cohort design) | intake of fruits and vegetables and BC risk |
| Characteristics of systematic reviews included in the umbrella review (5) | |||||||
| Albuquerque 2013 [17] | 8 studies in Europe, 9 in North America, 5 in Asia, 4 in South America, 1 in Africa, and 1 in Oceania | up December 2012 | 26 articles | 584,437 women and 28,962 incident cases of BC | systematic review | 11 cohort studies and 15 case-control studies | dietary patterns and BC risk |
| Farsinejad-Marj 2015 [18] | 7 studies in Europe, 1 in America | up to April 2015 | 8 studies | 502,253 participants | systematic review | 5 cohort studies; 3 case-control studies | Mediterranean diet and BC risk |
| Michels 2007 [28] | not clearly defined | January 1950–May 2005 | 21 studies on fat intake, 8 on fruit and vegetables, 11 on carbohydrates, 11 on antioxidants, 12 on dairy products, 2 on vitamin D, 5 on soy, 6 on green tea, 1 on heterocyclic amines, 2 on adolescent diet | not clearly defined | systematic review | 73 cohort studies, 3 meta-analyses, 3 pooled analyses | diet and BC |
| Mourouti 2013 [34] | // | from January 2000 to April 2013 | 29 studies, 12 on populations with a high consumption of soy | // | systematic review | 10 cohort, 3 nested case-control and 16 case-control studies | soy food consumption and BC risk |
| Mourouti 2015 [21] | // | from January 2002 to August 2012 | 95 studies on: fruit and vegetable (11), meat (14), soy (24), dietary fiber (9), dietary carbohydrates (16), dietary lipids (21) | fruit and veg: 16,110 cases among 122,933 participants meat: 31,918 cases among 813.021 participants soy: 9064 cases among 324,345 participants dietary fiber: 15,880 cases among 641,322 participants fat: 24,788 cases among 951,479 participants diet carbohydrates (studies showing a positive association): 4332 cases among 146,692 participants | systematic review | 42 case-control studies, 51 cohort studies and 2 dietary intervention RCTs | diet and BC |
| Characteristics of not systematic reviews included in the umbrella review (7) | |||||||
| Cui 2006 [54] | vitamin D: 7 studies in North America (6 in USA), 1 in Europe (Switzerland) Calcium: 9 studies in Europe, 2 in North America, and 1 in Asia (China) | not defined | 20 studies (8 on dietary vitamin D and 12 on calcium intake) | vitamin D: 7947 BC cases out of 218,776 subjects; calcium: 11,378 BC cases out of 16,764 subjects | not-systematic review | vitamin D: 5 prospective studies (4 cohort and 1 nested case-control) and 3 case control studies; calcium: 3 cohort and 9 case-control studies | association between vitamin D and calcium and BC risk |
| Duffy 2007 [35] | 5 studies in Europe, 8 in Asia, 6 North America | // | 21 studies | 12,472 BC cases and 35,513 controls in case-control studies; 1799 BC cases among 206,030 participants in cohort studies | not-systematic review | 6 cohort studies and 15 case-control studies | phytoestrogen intake and BC risk |
| Eichholzer 2001 [57] | 6 studies in North America, 1 in South America, and 1 in Europe | // | 8 studies | 9420 BC cases | not-systematic review | 5 case control studies and 3 nested case-control studies | folate intake and BC risk |
| Hanf 2005 [23] | // | // | 13 prospective studies on fat intake; 10 prospective studies on meat consumption | // | not-systematic review | cohort studies and interventional trials | foods, nutrients and BC risk |
| Lof 2006 [36] | 5 studies in North America, 3 in Europe (1 of them on an Asian population) | from 1966 to September 2006 | 7 studies | 4741 BC cases among 134,100 participants | not-systematic review | 5 case-control studies and 2 cohort studies | dietary phytoestrogens intake and BC risk |
| Peeters 2003 [37] | 2 studies in North America and 11 on Asian populations | up to November 2011 | 13 studies on dietary phytoestrogens | 5954 BC cases out of 27,162 participants | not-systematic review | 9 case-control studies and 4 cohort studies | phytoestrogens and BC risk |
| Rossi 2014 [60] | // | 1975–2013 | 175 pertinent articles: 18 for proteins, 18 for carbohydrates, 18 for dietary fat, 33 for polyphenols and phytoestrogen, 18 for fruit and vegetables, 11 for lycopene, 44 for vitamins and oligo elements, 8 for alcohol | // | not-systematic review | // | impact of dietary factors in BC risk |
| Author_ Year | Menopausal Status | Exposure Measure | Overall Results of Review | Statistical Method | Summary Estimates and Related 95% CI | p-value |
| Results of meta-analysis included in the umbrella review (32) | ||||||
| Alexander 2010 [43] | pre- and post-menopause | animal fat intake (highest vs. lowest categories) | no statistically significant association was found between animal fat intake (comparing highest vs. lowest category) and BC risk. | random effect model | summary relative risk (RR) estimates: 1.11 (0.91–1.36) | // |
| Aune 2012 [38] | pre- and post-menopause | dietary fiber, fruit fiber, vegetable fiber, cereal fiber, soluble and insoluble fiber | an inverse association was found between dietary fiber intake and BC risk; the association appeared to be most pronounced in studies with high levels (>25 vs. <25 g/day) or large ranges (>13 vs. <13 g/day) of fiber intake. | random effects model was used to calculate summary RRs and 95% CIs | summary RR (high vs. low intake): | // |
| - dietary fiber 0.93 (0.89–0.98) | ||||||
| - fruit fiber 0.95 (0.86–1.06) | ||||||
| - vegetable fiber 0.99 (0.92–1.07) | ||||||
| - cereal fiber 0.96 (0.90–1.02) | ||||||
| - soluble and insoluble fiber 0.91 (0.84–0.99) | ||||||
| Boyd 2003 [44] | // | dietary fat: total fat, saturated fat and monounsaturated fat; foods containing animal fat: meat, milk and cheese | a higher fat intake is associated with a higher risk of BC, with a significant positive association confirmed for total fat and saturated fat; meat and cheese consumption was also associated with a statistically significant increase in BC risk. | random effects model | summary RR (highest vs. lowest categories of intake) for all studies combined | // |
| - total fat 1.13 (1.03–1.25) | ||||||
| - saturated fat 1.19 (1.06–1.35) | ||||||
| - monounsaturated fat 1.11 (0.96–1.28) | ||||||
| -polyunsaturated fat 0.94 (0.80–1.10) | ||||||
| - meat consumption 1.17 (1.06–1.29) | ||||||
| - milk consumption 1.12 (0.88–1.43) | ||||||
| - cheese consumption 1.26 (0.96–1.66) | ||||||
| Brennan 2010 [14] | // | dietary patterns (DP): “prudent/healthy” vs. “Western/unhealthy” | no overall association was found for Western/unhealthy DP and BC risk; results of combined case-control studies showed that Western DP was positively associated with BC risk (highest vs. lowest category of intake); there was evidence of a lower risk of BC (highest vs. lowest category of intake) associated with a prudent/healthy DP in all studies and in pooled cohort studies. | random effects model | summary RR estimates (highest vs. lowest categories of intake): | |
| Western/unhealthy diet overall 1.09 (0.98–1.22); | 0.11 | |||||
| - case-control combined 1.31 (1.04–1.63); | 0.02 | |||||
| - cohort combined 0.99 (0.90–1.08) | 0.82 | |||||
| Prudent/healthy diet overall 0.89 (0.82–0.99); | 0.02 | |||||
| - case-control combined 0.84 (0.67–1.04); | 0.12 | |||||
| - cohort combined 0.93 (0.88–0.98) | 0.01 | |||||
| Buck 2010 [29] | pre- and post-menopause | lignan exposure, plant lignan intake | lignan exposure was not associated with a significantly lower risk of BC; but a high lignan intake in postmenopausal women was associated with a significant reduction in risk of BC. | random effects model and fixed effects model | pooled estimate (highest vs. lowest quantile) | // |
| overall 0.92 (0.81–1.02) | ||||||
| - premenopause 0.87 (0.66–1.08) | ||||||
| - postmenopause 0.86 (0.78–0.94) | ||||||
| dietary plant lignans 0.94 (0.82–1.05) | ||||||
| - premenopause 1.01 (0.87–1.15) | ||||||
| - postmenopause 0.86 (0.77–0.94) | ||||||
| Chen 2010 [52] | pre- and post-menopause | dietary calcium and vitamin D intake | a statistically significant overall inverse association was found between dietary vitamin D intake and BC risk; high vitamin D intake was associated with a 17% decrease in BC risk in premenopausal women; a statistically significant overall inverse association was found between dietary calcium intake and BC risk. | a random effects model if there was significant heterogeneity among studies; if not, a fixed effects model was acceptable | summary RRs (highest vs. lowest category): | // |
| - vitamin D intake overall 0.91 (0.83–1.00) | ||||||
| premenopause 0.83 (0.73–0.95) | ||||||
| postmenopause 0.94 (0.83–1.07) | ||||||
| - calcium intake overall 0.81 (0.72–0.90) | ||||||
| premenopause 0.72 (0.55–0.95) | ||||||
| postmenopause 0.95 (0.79–1.14) | ||||||
| Chen 2014 [55] | pre- and post-menopause | total folate intake, dietary folate intake and folate supplement intake | no significant association between dietary folate intake and BC risk in meta-analysis of prospective studies, but a significantly negative correlation emerged from the case control studies, particularly for postmenopausal women; more dietary folate may reduce the BC risk in populations of Europe, Australia or Asia (not in the USA). | inverse variance weighting method; random effects model | summary RRs (highest vs. lowest category) in prospective studies: | // |
| total folate 0.97 (0.87–1.08); | ||||||
| dietary folate (DF) 0.95 (0.87–1.03) | ||||||
| - DF premenopause 1.02 (0.62–1.67) | ||||||
| - DF postmenopause 0.94 (0.81–1.08) | ||||||
| OR (highest vs. lowest category) in case-control studies: | ||||||
| total folate 0.87 (0.61–1.23) | ||||||
| dietary folate (DF) 0.79 (0.67–0.92) | ||||||
| DF premenopause 0.78 (0.53–1.14) | ||||||
| DF postmenopause 0.73 (0.59–0.92) | ||||||
| Dong 2011 (a) [30] | pre- and post-menopause | dietary soy isoflavone intake | soy isoflavone intake was associated with a significantly reduced risk of BC in Asian populations, but not in Western populations; a significant inverse association between soy isoflavone intake and risk of BC emerged in postmenopausal but not in premenopausal women. | random or fixed effects model | summary RR: | // |
| all women 0.89 (0.79–0.99) | ||||||
| Asian countries 0.76 (0.65–0.86) | ||||||
| Western countries 0.97 (0.87–1.06) | ||||||
| premenopause 0.90 (0.64–1.15) | ||||||
| postmenopause 0.78 (0.63–0.93) | ||||||
| Dong 2011 (b) [26] | pre- and post-menopause | total dairy food defined as skimmed/low-fat milk, whole/high-fat milk, yogurt, cottage cheese, butter, and other dairy products | for total dairy food consumption, a significantly inverse association with BC risk was confirmed, and was stronger for low-fat dairy food and for premenopausal women; for milk consumption only low-fat milk was significantly associated with a lower BC risk; no association in postmenopausal women. | random effects model | summary RR (highest vs. lowest intake) | // |
| total dairy food 0.85 (0.76–0.95) | ||||||
| milk 0.90 (0.80–1.02) | ||||||
| total dairy food | ||||||
| - premenopause 0.79 (0.63) | ||||||
| - postmenopause 0.92 (0.83–1.01) | ||||||
| total milk | ||||||
| - premenopause 0.79 (0.60–1.02) | ||||||
| - postmenopause 1.01 (0.94–1.09) | ||||||
| Gandini 2000 [38] | // | vegetable and fruit consumption, and 2 related micronutrients: vitamin C and beta-carotene | high vegetable consumption, and high vitamin C and beta-carotene intake had a significant protective effect against BC; pooled estimates for fruit intake indicated that this food group may have a protective effect, but without statistical significance. | random effects model fixed effects model | summary RR (high vs. low consumption) | // |
| - vegetables 0.75 (0.66–0.85) | ||||||
| - fruits 0.94 (0.79–1.11) | ||||||
| - vitamin C 0.80 (0.68–0.95) | ||||||
| - beta-carotene 0.82 (0.76–0.91) | ||||||
| Gissel 2008 [53] | pre- and post-menopause | vitamin D consumption | no association between vitamin D levels and BC risk. | random effects model | summary RR: 0.98 (0.93–1.03) analysis restricted to intake <400 International Units (IU)/day vs. lower intake: | // |
| RR 0.92 (0.87–0.97) | ||||||
| Guo 2015 [19] | pre- and post-menopause | red and processed meat consumption | higher red and processed meat intake was associated with higher risk of BC. | random effects model | summary RR of BC (highest vs. lowest consumer categories) were: 1.10 (95% confidence interval (CI), 1.02–1.19) for red meat, and 1.08 (95% CI, 1.01–1.15) for processed meat intake; estimated summary RR were 1.11 (1.05–1.16) for an increase of 120 g/day of red meat, and 1.09 (1.03–1.16) for an increase of 50 g/day of processed meat | // |
| Hu 2012 [59] | pre- and post-menopause | dietary α-carotene; dietary β-carotene; β-cryptoxanthin; lutein+ zeaxanthin; lycopene | a significant inverse association between α-carotene consumption and BC risk, in both cohort and case-control studies; a trend towards a protective effect of β-carotene; no significant association between β-cryptoxanthin, lutein+zeaxanthin and BC risk; lycopene may have a protective effect against BC (significant inverse association in case-control studies). | random effects model | summary RR among cohort studies: | |
| α-carotene 0.91 (0.85–0.98) | 0.01 | |||||
| β-carotene 0.94 (0.88–1.00) | 0.05 | |||||
| β-cryptoxanthin 1.03 (0.96–1.11) | 0.39 | |||||
| lutein+zeaxanthin 0.94 (0.87–1.02) | 0.13 | |||||
| lycopene 0.99 (0.93–1.06) | 0.77 | |||||
| summary OR among case-control studies: | ||||||
| α-carotene 0.82 (0.70–0.97) | 0.02 | |||||
| β-carotene 0.75 (0.67–0.85) | <0.01 | |||||
| β-cryptoxanthin 0.95 (0.80–1.13) | 0.54 | |||||
| lutein+zeaxanthin 0.79 (0.66–0.94) | 0.01 | |||||
| lycopene 0.71 (0.56–0.92) | 0.01 | |||||
| Hui 2013 [58] | pre- and post-menopause | flavonoid subclasses: flavonols (onions, broccoli, tea, fruit); flavones (herbs, parsley, chamomile); flavonones (citrus fruits, oranges, grapefruit); flavan-3-ols (dark chocolate, apples, grapes, red wine, green tea); anthocyanidins (berries, cranberries, black currants, blueberries); isoflavones (soy and soy products) | BC risk significantly lower in women with high intake of flavonols and flavones; no significant association with flavan-3-ols, flavonones, anthocyanins or total flavonoids. Summary RRs of studies stratified by menopausal status suggest that flavonols, flavones and flavan-3-ols are associated with a significantly lower risk of BC in postmenopausal, but not in premenopausal women. | random and fixed effects model | summary RR (highest vs. lowest consumption): | // |
| flavonols 0.88 (0.80–0.96) | ||||||
| - postmenopause 0.92 (0.85–0.99) | ||||||
| flavones 0.83 (0.76–0.91) | ||||||
| - postmenopause 0.86 (0.77–0.94) | ||||||
| flavan-3-ols 0.93 (0.84–1.02) | ||||||
| - postmenopause 0.90 (0.83–0.98) | ||||||
| flavonones 0.95 (0.88–1.03) | ||||||
| anthocyanidins 0.97 (0.87–1.08) | ||||||
| Larsson 2007 [56] | pre- and post-menopause | dietary folate intake | no significant association between dietary folate intake and BC risk in prospective studies; in case-control studies, high vs. low dietary folate intake was associated with a significantly different risk of BC (lower in the former). | random effects model | summary estimates (highest vs. lowest dietary folate intake categories): | // |
| cohort studies: RR 0.96 (0.87–1.05) | ||||||
| case-control studies: Odds Ratio (OR) 0.73 (0.64–0.83) | ||||||
| Li 2014 [41] | pre- and post-menopause | dietary mushroom intake | a significant inverse association between mushroom consumption and BC risk | random and fixed effects model | summary RR (highest vs. lowest dietary mushroom intake categories): | // |
| premenopause 0.96 (0.91–1.00) | ||||||
| postmenopause 0.94 (0.91–0.97) | ||||||
| overall: 0.97 (0.96–0.99) | ||||||
| Mulholland 2008 [47] | pre- and post-menopause | glycemic index (GI) and glycemic load (GL) | no strong associations between high vs. low GI and BC risk; a positive association emerged once analysis was restricted to more robust measures of dietary intake, for both premenopausal and postmenopausal women. | // | summary RR in cohort studies (high vs. low GI) | // |
| premenopause RR 1.20 (1.01–1.43) | ||||||
| postmenopause RR 1.10 (1.02–1.19) | ||||||
| Mullie 2016 [48] | pre- and post-menopause | dietary pattern with high GI or GL | women with high GI or GL had a small, 5–6% increase in BC risk. | random effects model | summary RR (high vs. low) for GI 1.05 (1.00–1.11) | // |
| - premenopause 1.04 (0.86–1.27) | ||||||
| - postmenopause 1.05 (0.98–1.13) | ||||||
| for GL 1.06 (1.00–1.13) | ||||||
| - premenopause 1.23 (0.75–2.00) | ||||||
| - postmenopause 1.05 (0.97–1.13) | ||||||
| Schwingshackl 2014 [15] | // | Mediterranean diet (MD; fruits, vegetables, legumes, olive oil, nuts, plant protein and whole grains, fish; moderate red wine consumption and low amounts of red meat, poultry and dairy products) | case-control studies showed a significant association between greater adherence to MD and lower BC risk; cohort studies showed no significant association between BC risk and MD. Overall, MD was not associated with a significant reduction in BC risk. | random effects model | pooled RR (highest vs. lowest adherence to MD category): | |
| total 0.95 (0.84–1.06) | 0.35 | |||||
| cohort 1.01 (0.88–1.16) | 0.89 | |||||
| case-control 0.82 (0.69–0.97) | 0.02 | |||||
| Seely 2005 [42] | // | green tea (dried leaves of Camellia sinensis with minimal oxidation of herbs, polyphenols and catechins) | random effects model revealed no significant association between green tea consumption and BC risk; fixed effects model in case-control studies showed a significant inverse association. | random effects model fixed effects model | pooled RR (highest vs. lowest consumption) | |
| cohort studies 0.89 (0.71–1.10) | 0.28 | |||||
| case-control studies 0.44 (0.14–1.31) | 0.14 | |||||
| case-control studies 0.57 (0.38–0.86) | 0.007 | |||||
| Si 2014 [25] | pre- and post-menopause | egg consumption quartiles: 1 a week (reference) ≥1, <2 a week ≥2, ≤5 a week > 5 a week | higher egg consumption was associated with higher BC risk; subgroup analyses showed this association in cohort studies, among Europeans, Asian populations, postmenopausal women, and consumers of ≥2 and ≤5 eggs/week. | random effects model | pooled adjusted RR | |
| overall 1.04 (1.01–1.08) | 0.02 | |||||
| case control 1.06 (0.97–1.15) | 0.21 | |||||
| cohort 1.04 (1.00–1.08) | 0.05 | |||||
| postmenopause 1.06 (1.02–1.10) | 0.01 | |||||
| premenopause 1.04 (0.98–1.11) | 0.2 | |||||
| ≥2 and ≤5/week (ref. <1/week) | ||||||
| RR 1.10 (1.02–1.17) | 0.01 | |||||
| Song 2013 [40] | not stated | citrus fruit intake, yellow and orange fruit, oranges or tangerines | a higher intake of citrus fruit may reduce BC risk. | fixed effects model | summary OR (highest vs. lowest intake group): 0.90 (0.85–0.96) | // |
| Taylor 2009 [20] | premenopause | red meat consumption | a significant positive association was found overall between high of red meat intake and BC risk among premenopausal women; case-control studies confirmed a strong association between red meat and BC risk, while cohort studies found no statistically significant association between them. | // | summary RR (highest vs. lowest red meat intake): | // |
| overall 1.24 (1.08–1.42) | ||||||
| cohort studies 1.11 (0.94–1.31) | ||||||
| case-control studies 1.57 (1.23–1.99) | ||||||
| Trock 2006 [31] | pre- and post-menopause | soy protein (grams of soy protein consumed daily) | among all women, high soy intake was modestly associated with a lower BC risk; the association was not significant for Asian women; among 10 studies stratified by menopausal status, the inverse association between soy exposure and BC risk was stronger premenopause than postmenopause. | random effects model and fixed effects model (in premenopausal women) | pooled OR (high vs. low soy intake) | // |
| all women 0.86 (0.75–0.99) | ||||||
| premenopause 0.70 (0.58–0.85) | ||||||
| postmenopause 0.77 (0.60–0.98) | ||||||
| Turner 2011 [45] | premenopause (7), postmenopause (20), and both (25) | total fat, saturated fat (SAT), monounsaturated fat (MUFA), polyunsaturated fat (PUFA) | cohort studies found significant summary RR between PUFA and BC; case-control studies found no association between fat and BC; postmenopausal women had a significant association between total fat, PUFA intake and BC; an inverse association between total intake of all fats and BC was seen in premenopausal women, but was not significant. | random effects model | pooled RR (highest vs. lowest quartile of consumption) | |
| total fat 1.01 (0.99–1.03) | non-significant (NS) | |||||
| SAT 1.00 (0.95–1.05) | NS | |||||
| MUFA 0.99 (0.95–1.05) | NS | |||||
| PUFA 1.06 (1.01–1.14) | 0.03 | |||||
| premenopause 0.97 (0.94–1.01) | NS | |||||
| postmenopause 1.04 (1.01–1.07) | 0.004 | |||||
| Velentzis 2009 [32] | pre- and post-menopause | plant lignan intake | no significant association between plant lignan intake and BC risk, despite a slight protective effect; when menopausal status was considered, a statistically significant risk reduction was seen for the highest plant lignan intake in postmenopausal women. | random effects model | combined OR (highest vs. lowest plant lignan intake) | |
| overall 0.93 (0.83–1.03) | 0.15 | |||||
| postmenopause 0.85 (0.78–0.93) | < 0.001 | |||||
| Wu 2008 [9] | pre- and post-menopause | soy intake - isoflavone Asian (highest >20 mg/day - lowest <5 mg/day) Western (highest >0.8 mg/day - lowest <0.15 mg/day) | a statistically significant 29% reduction in BC risk associated with high soy intake in Asian populations (high consumers); both premenopausal and postmenopausal Asian women consuming large amounts of soy had a lower BC risk; no significant association was found in Western countries. | random effects model | pooled OR (highest vs. lowest soy intake) | // |
| Asian 0.71 (0.60–0.85) | ||||||
| - premenopause 0.65 (0.50–0.85) | ||||||
| - postmenopause 0.63 (0.46–0.85) | ||||||
| Western 1.04 (0.97–1.11) | ||||||
| Wu 2015 [33] | // | dietary factors: vegetables, fruits, soy food, or dietary fat | high consumption of fruits, vegetables and soy foods was significantly inversely associated with a lower BC risk in Chinese women; higher fatty food consumption appeared to be related to higher risk of BC in Chinese women. | random effects model | combined OR (high vs. low intake) | |
| vegetables 0.77 (0.62–0.96) | 0.02 | |||||
| fruit 0.68 (0.49–0.93) | 0.02 | |||||
| soy food 0.68 (0.50–0.93) | 0.02 | |||||
| fat 1.15 (1.01–1.30) | 0.03 | |||||
| Yang 2014 [49] | pre- and post-menopause | dietary polyunsaturated fatty acid intake (n-3/n-6 PUFA) | intake ratio of n-3/n-6 PUFA was inversely associated with BC risk for the highest vs. lowest quantiles of the study population. | random effects model | pooled RR (highest quantile vs. lowest) | // |
| overall diet 0.90 (0.82–0.99) | ||||||
| premenopause 0.80 (0.43–1.48) | ||||||
| postmenopause 0.85 (0.75–0.97) | ||||||
| Zang 2015 [27] | pre- and post-menopause | dairy food consumption: high (>600 g/day) modest (400–600 g/day) low (<400 g/day) dairy food items (milk, cheese, butter) converted into grams of protein per day | higher dairy food consumption was associated with a statistically significant lower risk of BC, in both cohort and case-control studies; there was a marginally lower BC risk in premenopausal women. | random effects model | combined estimates (highest dairy consumption vs. lowest) | // |
| cohort RR 0.90 (0.83–0.98) | ||||||
| - premenopause 0.88 (0.77–1.00) | ||||||
| - postmenopause 0.94 (0.86–1.02) | ||||||
| case-control OR 0.74 (0.62–0.88) | ||||||
| Zheng 2013 [50] | pre- and post-menopause | dietary intake of marine n-3 polyunsaturated fatty acids (PUFA) | greater marine n-3 PUFA intake was associated with a 14% reduction in BC risk; no significant association for fish intake or exposure to alpha-linoleic acid. | random effects model | fish intake (highest vs. lowest category) | // |
| overall 1.03 (0.93–1.14) | ||||||
| - premenopause 1.04 (0.91–1.20) | ||||||
| - postmenopause 1.08 (0.92–1.27) | ||||||
| marine n-3 PUFA (highest vs. lowest) | ||||||
| overall 0.86 (0.78–0.94) | ||||||
| - premenopause 0.96 (0.78–1.18) | ||||||
| - postmenopause 0.88 (0.76–1.00) | ||||||
| Zhou 2015 [51] | pre- and post-menopause | linoleic acid | both dietary linoleic acid and overall linoleic acid level were associated with a lower risk of BC, but none of the associations were statistically significant. | random and fixed effects model | exposure assessment (highest vs. lowest category of linoleic acid) | // |
| overall 0.98 (0.93–1.04) | ||||||
| dietary linoleic acid 0.96 (0.92–1.01) | ||||||
| premenopause 0.64 (0.20–2.09) | ||||||
| postmenopause 1.01 (0.94–1.08) | ||||||
| Results of pooled analyses included in the umbrella review (4) | ||||||
| Mannisto 2005 [16] | // | 2 dietary patterns with a high intake of: VEG = vegetables, legumes, fruit, pasta fish and oil; PPP = pork, processed meat, potatoes, beef, rice, poultry, liver, butter/low-fat margarine, pasta and coffee | no significant association between VEG pattern and BC risk in any of the cohorts included in the analysis; in the multivariate model PPP was not significantly associated with BC risk in two cohorts (ORDET, SMC), while in the NLCS (Netherlands) cohort there was a significantly inverse association between PPP intake and BC risk (RR 0.90_0.81–0.99). | // | // | // |
| Missmer 2002 [22] | pre- and post-menopause | total meat, red and white meat, dairy fluids and solids | no significant association between total meat, red meat, white meat, total dairy fluids or solids and BC risk. | random effects model | pooled RR (highest vs. lowest quartile) | |
| total meat 1.08 (0.98–1.19) | 0.13 | |||||
| red meat 0.94 (0.87–1.02) | 0.13 | |||||
| white meat 1.02 (0.91–1.13) | 0.21 | |||||
| dairy fluids 0.93 (0.84–1.03) | 0.09 | |||||
| dairy solids 1.01 (0.93–1.09) | 0.94 | |||||
| Smith-Warner 2001 (a) [46] | pre- and post-menopause | saturated, monounsaturated, polyunsaturated, animal, vegetable and total fat intake | no statistically significant association between intake of fat subtypes and BC risk; no associations for animal or vegetable fat intake; these associations were unaffected by menopausal status. | random effects model | pooled adjusted RR (5% energy increases from specific fat subtypes): | |
| saturated fat 1.09 (1.00–1.19) | ||||||
| - premenopause 1.10 (0.91–1.35) | 0.61 | |||||
| - postmenopause 1.07 (0.93–1.24) | 0.61 | |||||
| monounsaturated fat 0.93 (0.84–1.03) | ||||||
| - premenopause 0.87 (0.63–1.19) | 0.46 | |||||
| - postmenopause 0.81 (0.65–1.03) | 0.46 | |||||
| polyunsaturated fat 1.05 (0.96–1.16) | ||||||
| - premenopause 1.12 (0.88–1.41) | 0.72 | |||||
| - postmenopause 1.28 (0.96–1.69) | 0.72 | |||||
| animal fat 1.01 (0.96–1.06) | ||||||
| - premenopause 1.01 (0.91–1.12) | 0.93 | |||||
| - postmenopause 0.99 (0.95–1.03) | 0.93 | |||||
| vegetable fat 1.01 (0.98–1.04) | ||||||
| - premenopause 1.03 (0.93–1.13) | 0.54 | |||||
| - postmenopause 0.99 (0.94–1.04) | 0.54 | |||||
| Smith-Warner 2001 (b) [39] | pre- and post-menopause | total fruits, fruit juice, total vegetables, total fruit and vegetables | weak, insignificant associations for total fruits, total vegetables, and total fruit and vegetables; no associations for green leafy vegetables, 8 botanical groups, and 17 specific fruits and vegetables; these associations were not influenced by menopausal status. | random effects model | pooled adjusted RR (highest vs. lowest quartile of intake): | |
| total fruits 0.93 (0.86–1.00) | 0.08 | |||||
| total vegetables 0.96 (0.89–1.04) | 0.54 | |||||
| total fruits and vegetables 0.93 (0.86–1.00) | 0.12 | |||||
| Author_year | Menopausal status | Exposure measure | Overall results of review | |||
| Results of systematic reviews included in the umbrella review (5) | ||||||
| Albuquerque 2013 [17] | // | dietary patterns (DP): - “Healthy/prudent”(fruits, vegetables, whole grains and cereals, fish and soy) -”Mediterranean”(fruit, raw and cooked vegetables, fish and crustaceans, olive and sunflower oil) - “Western” (red and processed meats, refined grains, potatoes and starches, snacks, sweets, fried food and soft drinks) | 23 studies on the association of Healthy DP and BC risk (highest vs. lowest level of consumption): | |||
| - 12 studies found a significant inverse association with BC; | ||||||
| - 9 studies reported no statistically significant association; | ||||||
| - 2 case-control studies found a positive association. | ||||||
| 3 studies assessed the Mediterranean DP (highest vs. lowest level of consumption): | ||||||
| - 2 studies found a significant inverse association with BC; | ||||||
| - 1 study report no statistically significant association. | ||||||
| 24 studies examined the association of Western DP and BC risk (highest vs. lowest level of consumption): | ||||||
| - 9 studies found a positive association with BC; | ||||||
| - 14 studies reported no statistically significant association; | ||||||
| - 1 studies found a significant inverse association with BC. | ||||||
| Farsinejad-Marj 2015 [18] | pre- and post-menopause for six studies; postmenopause for two studies | Mediterranean diet | 4 studies considered the association between MD and BC risk in both pre- and post-menopausal women:
| |||
| Michels 2007 [28] | pre- and post-menopause | dietary exposures: fat intake, fruit and vegetables consumption, antioxidants, vitamins (A, C, E, β-carotene), carbohydrates, glycemic index (GI) and glycemic load (GL), dairy food consumption (including vitamin D), soy and isoflavones, green tea, heterocyclic amines, adolescent diet | overall fat intake was unrelated to the incidence of BC; 2 cohorts showed a significant positive association between high fat intake and BC risk (ORDET cohort: RR 3.47_1.43–8.44); | |||
| fruit and vegetable consumption may prevent BC: only one significant association (Nurses’ Health Study) reported an inverse association for 5 or more vegetables/day; | ||||||
| vitamins A,C,E, beta-carotene: no consistent association (except for vitamin E intake in postmenopausal women); | ||||||
| carbohydrates, GI and GL: no significant association; | ||||||
| results for vitamin D, dairy and soy products were inconsistent. | ||||||
| Mourouti 2013 [34] | // | soy consumption (isoflavones and lignans) | 13 out of 16 case-control studies, 3 out of 3 nested case-control studies, and 3 out of 10 cohort studies demonstrated an inverse association between soy food, soy product or isoflavone intake and BC risk; some studies, 3 out of 16 case-control studies and 6 out of 10 cohort studies found no association between soy or isoflavone intake and BC risk; only 1 of 29 studies revealed a possible association between phytoestrogen dietary intake and BC risk. | |||
| Mourouti 2014 [21] | pre- and post-menopause | intake of fruit and vegetables, meat, soy products and isoflavones, dietary fiber, dietary carbohydrates, dietary lipids | for fruit and vegetable consumption, most studies found a significant inverse association with BC risk; | |||
| for meat intake, 7 studies found a significantly higher risk and 7 found no association; most case-control studies on soy consumption found an inverse association; | ||||||
| most studies on dietary fiber found no association; | ||||||
| 3 cohort and 2 case-control studies on dietary carbohydrates found a higher BC risk for higher GI and GL, while the other 11 studies found no association; | ||||||
| 6 out of 10 case-control studies found a positive association with high fat intake, but most cohort studies found no significant association. | ||||||
| Results of qualitative reviews included in the umbrella review (7) | ||||||
| Cui 2006 [54] | pre- and post-menopause | dietary and supplemental vitamin D intake; dietary and supplemental calcium intake | 7 studies (5 on pre- and post-menopausal women, 1 on postmenopausal women, 1 on premenopausal women) of the 12 studies considered found a statistically significant inverse association (highest vs. lowest category of intake) between calcium intake and BC risk; this study showed no association between dietary and supplemental vitamin D intake and BC; only one cohort study found a protective effect among premenopausal women. | |||
| Duffy 2007 [35] | pre- and post-menopause | phytoestrogen intake | 10 case-control studies showed a significant inverse association between phytoestrogen/isoflavone/lignin intake and BC risk, while 5 revealed no such association; only 1 of 6 cohort studies found a protective effect of high isoflavone intake. | |||
| Eichholzer 2001 [57] | pre- and post-menopause | dietary folate intake | epidemiological studies suggested an inverse association between folate intake and BC among female regular alcohol consumers; no significant association between folate intake and BC risk in the overall population. | |||
| Hanf 2005 [23] | // | fat intake; meat and fish consumption; fruit and vegetable consumption, fiber consumption | 12 studies tested total fat intake as a risk factor for BC, and only one showed a statistically significant reduced RR with a higher total fat intake; animal fat was not found associated with BC; no significant association emerged for saturated, monounsaturated and polyunsaturated fatty acids: 4/10 prospective studies found a positive correlation between high levels of meat consumption and BC risk; no association between fish intake and BC; no significant correlation between BC and high consumption of fruit and vegetables; no overall association between fiber intake and BC risk: only 1 of 5 studies suggested an effect of fiber. | |||
| Lof 2006 [36] | pre- and post-menopause | dietary lignan intake | 4 of 5 case-control studies showed a protective effect of dietary lignans against BC, especially in premenopausal women; 2 prospective studies did not confirm any protective effect of dietary lignans. | |||
| Peeters 2003 [37] | pre- and post-menopause | phytoestrogens (soybeans, soy products, miso, tofu, soy protein, isoflavones) | overall, results showed no protective effect of dietary intake of soy products against BC, except for women who consumed phytoestrogens in adolescence or in very high doses. | |||
| Rossi 2014 [60] | // | proteins, carbohydrates and glycemic index (GI), dietary fat, polyphenols and phytoestrogens, fruits and vegetables, lycopene, vitamins and oligo elements, alcohol | consumption of well- or over-cooked red meat was associated with a higher risk of BC; n-3 PUFA may protect against BC; a lower GI seems associated with a lower risk of BC; high-fat diet, and high total cholesterol and triglyceride levels are associated with a higher risk of BC; evidence supports a protective role of lycopene, polyphenols, fruit and vegetables against BC; there was evidence of vitamin D reducing the BC risk; and of zinc and, to a lesser extent, vitamins E and B reducing the BC risk thanks to their antioxidant properties. | |||
| Author_ Year | Limitations | Recommendations/Conclusions | Quality Assessment Tool | Quality Assessment |
|---|---|---|---|---|
| Conclusion and quality assessment of meta-analysis included in the umbrella review (32) | ||||
| Alexander 2010 [43] | Meta-analysis limited to analysis of results reported across publications. Many studies on fat intake and BC probably did not examine fat from animal sources alone. Differential reporting of dietary factors may influence summary associations across the literature. The association between dietary fat and BC subgroups is also incomplete. | The available epidemiological evidence from prospective studies does not support an independent association between animal fat intake and BC risk. Better dietary assessments and methods in cohort studies, also examining dietary fat and BC in randomized clinical trials, may help to clarify any possible relationships. | // | // |
| Aune 2012 [38] | Potential unmeasured or residual confounders; a higher fiber intake is often associated with other lifestyle factors (higher levels of physical activity, lower prevalence of obesity, lower intake of alcohol and dietary fat); measurement errors in dietary intake assessments are known to bias effect estimates. | Diet with a high intake of plant-based foods rich in fiber could have an impact in the prevention of BC; this review suggests that diets rich in fiber are associated with a lower BC risk. | // | // |
| Boyd 2003 [44] | Measurement error in the food frequency questionnaires (FFQs) used in most studies may lead to overestimation of the range of intakes, and may also lead to attenuation of risk. | Combined risk estimates of for total and saturated fat intake, and for meat intake, all indicated an association between higher intakes and an increased risk of BC. Case-control and cohort studies gave similar results. | Quality of studies scored using preset methodological standards | Twenty-six studies defined as “higher-quality” |
| Brennan 2010 [14] | Possible recall bias in case-control combined analysis; possible weakness in design of the studies (different response rates and inconsistent adjustment for potential confounders). Possible misclassification within the two dietary patterns. | This review provided evidence of a small inverse association between a healthy diet and a positive trend between Western diet and BC risk. The results of this meta-analysis highlight the need for more carefully designed observational and intervention studies to clarify the influence of diet on BC risk. | // | // |
| Buck 2010 [29] | Potential measurement errors due to recall bias or shortcomings in food composition database. | High lignan exposure may be associated with a reduced risk of BC in postmenopausal women. Additional work is warranted to confirm this association. | // | // |
| Chen 2010 [52] | Not reported. | From the meta-analysis, there was a significant inverse association between vitamin D and calcium intake and BC risk; these findings support the use of vitamin D and calcium as chemopreventive agents against BC. Better designed clinical trials are needed to ascertain the protective effect and optimize the doses of these nutrients. | // | // |
| Chen 2014 [55] | The BC prevention effect of folate may be conferred by other nutrients in foods (leafy vegetables, legumes, egg yolk, baker’s yeast); dose–effect relationships for dietary folate intake level and BC risk differed between prospective and case-control studies; changing dietary habits during the follow-up in prospective studies was not assessed; differences in sample size, study region, study design and assessment methods may cause heterogeneity and prompt differences in the stratification analysis. | The findings revealed a potential non-linear dose effect for dietary folate levels against BC risk, and modest folate intake may reduce BC risk. Given the complexity of folate metabolism and uses, the dose and timing of folate intake should be considered. More prospective studies are necessary. | Newcastle–Ottawa Scale (NOS) | Thirty studies classified as “higher-quality” (≥5 points (pt)), twelve as “lower-quality” (<5 pt) |
| Dong 2011 (a) [30] | Strong degree of heterogeneity made results difficult to interpret. Changes in soy consumption during the long follow-up may have weakened the associations observed. | A statistically significant inverse association was confirmed between soy isoflavone intake and BC risk. The protective effect of soy against BC may be due to other, associated healthy lifestyle factors (high vegetable and fruit intake, more physical activity). | // | // |
| Dong 2011 (b) [26] | Consumption of dairy food, especially low-fat products, is probably associated with a healthy lifestyle; the likelihood of inadequate control for confounding factors may bias the findings; dietary assessments suffer from measurement error; possible misclassification bias; substantial heterogeneity across studies. | Findings indicate that a higher consumption of total dairy products may be associated with a reduced BC risk: menopausal status may influence this effect. | // | // |
| Gandini 2000 [24] | Possibility of publication bias (due to studies not being published if findings are not significant); heterogeneous intake categories. | This analysis confirmed the association between vegetable and, to a lesser extent, fruit intake and BC risk. Increasing vegetable consumption, and the intake of associated micronutrients (vitamin C and b-carotene) might reduce the risk of BC. | // | // |
| Gissel 2008 [53] | Few studies and low vitamin D intake reported in most trials; possible bias from diet reporting. | Increasing the intake of vitamin D above 400 IU/day may help to prevent BC; but more research is needed. | // | // |
| Guo 2015 [19] | The residual confounders in the studies are a problem in the meta-analysis of observational studies; these findings are probably affected by the misclassification of meat; the intake and consumption levels in the highest and lowest categories varied across studies; possibility of publication bias. | A high intake of red and/or processed meat was associated with an increased risk of BC. Additional cohort or interventional studies will be needed to confirm the association. | // | // |
| Hu 2012 [59] | Socio-economic position may influence the intake of carotenoids; the lack of original data in the studies limited the assessment of potential interactions; no cohort study in Asia focused on the associations between carotenoids and BC. This analysis did not assess the quality of all the studies included. | Total α-carotene intake could reduce the BC risk. The relationship between β-carotene intake and BC needs to be confirmed. No significant associations emerged between dietary β-cryptoxanthin, lutein+zeaxanthin, lycopene and BC. | // | // |
| Hui 2013 [58] | // | The study suggested that the intake of flavonols and flavones, but not of other flavonoid subclasses, is associated with a decreased risk of BC, especially after menopause. | // | // |
| Larsson 2007 [56] | Potential bias due to confounders inherent in the original studies; potential recall, interviewer or selection bias in case-control studies; heterogeneity due to methodological differences among the studies. | No clear support for an overall relationship between folate intake and BC risk. Adequate folate intake may have a protective effect against BC. | // | // |
| Li 2014 [41] | Relatively small number of eligible studies included in the analysis, and only two prospective studies; limited information extracted from the original studies; different types of mushroom. | The findings suggested that a higher edible mushroom consumption may be associated with a lower risk of BC; large-scale prospective studies are needed to confirm as much. | Newcastle–Ottawa Scale (NOS)—9 pt scoring system | Four studies classified as “higher-quality” (≥7 pt) three as “lower-quality” (<7 pt) |
| Mulholland 2008 [47] | Study results inconsistently adjusted for potential confounders might result in residual confounding elements; a relatively small number of studies included in the analysis, making it difficult to estimate publication bias and heterogeneity. | High dietary GI and GL do not appear to be of etiological importance in BC development. | Newcastle–Ottawa quality assessment Scale (NOS) —9 pt scoring system | Fourteen “higher-quality” studies |
| Mullie 2016 [48] | Not all studies reported women’s menopausal status. Lack of RR unadjusted and adjusted for adiposity. | The evidence supports a modest association between a dietary pattern with high GI/GL and the risk of BC. | // | // |
| Schwingshackl 2014 [15] | Relationship between diet and cancer is complex (multiple confounding variables); Mediterranean diet (MD) was not homogenous (heterogeneity on score items); possible measurement errors and recall/selection bias in the studies included. | No significant changes in risk reduction for BC by adherence to MD. | Newcastle–Ottawa quality assessment Scale (NOS)—9 pt scoring system | Eight “higher-quality” (≥7 pt) and three “lower-quality” studies (<7 pt) |
| Seely 2005 [42] | Small number of observational studies and no RCTs; marked variability among questionnaire response rates in cohort studies; unadjusted analysis for potential confounding factors; possible selection bias that could distort the findings; case-control studies produced weaker evidence than cohort studies. | This systematic review and meta-analysis found no significant effect of green tea on BC prevention. Green tea consumption may be associated with a reduced risk of BC recurrences. | // | // |
| Si 2014 [25] | Only articles written in English were included in the meta-analysis; possible selection bias; categorical standards for egg consumption were confused, making it difficult to them among the studies; cooking methods were not ascertained. | Pooled results of cohort studies and combined results showed that higher egg consumption was associated with a higher BC risk, especially for European and postmenopausal populations. More studies should be conducted using a well-recognize categorical standard for egg consumption. Egg consumption should be reduced to reduce BC risk. | // | // |
| Song 2013 [40] | Diversity of study design; the apparent association of these pooled results is restricted to the case-control study (overestimating the exposure effect due to recall and selection bias); measurement error in the FFQs; cut-off points for citrus fruit intake vary across studies, so there is uncertainty about the optimal citrus fruit intake for the prevention of BC. | Pooled results from observational studies showed an inverse association between citrus fruit intake and the risk of BC. This study underscores the need for well-designed prospective observational and intervention studies to clarify the influence of citrus fruit on BC. | // | // |
| Taylor 2009 [20] | Bias involving the use of FFQs in all studies (self-report measures to assess consumption can lead to misclassification of intake); recall bias in case-control studies may affect observed associations between dietary intake and cancer risk (tendency to over-report among cases and under-report among controls). | Red meat may be a source of heterocyclic amines and heme-iron, a highly bioavailable form of iron which has been shown to enhance estrogen-induced tumor formation. This quantitative summary of published literature indicates that red meat may contribute to BC risk in premenopausal women. | // | // |
| Trock 2006 [31] | Possible measurement errors among the studies; potential selection bias; different levels of soy consumption among the studies; potentially uncontrolled confounders among the studies. | Soy intake may be associated with a small reduction in BC risk. This result should be interpreted with caution, however, due to potential exposure misclassification, confounders, or lack of a dose-response effect. | // | // |
| Turner 2011 [45] | Small sample size in premenopausal studies; association between BC risk and PUFA subtypes not examined separately. | High-fat diet may increase estrogen levels and therefore increase BC risk. Higher risk of BC in postmenopausal women consuming large amounts of total fat and PUFA. Conversely, dietary fat may have some BC prevention effects in premenopausal women. | // | // |
| Velentzis 2009 [32] | Over- or under-estimation of food content; some food composition databases are incomplete; the amount of lignans in food can differ depending on crop variety, location, year of harvest and processing; possible dietary measurement errors associated with FFQs; possibility of residual confounding factors. | Plant lignans may be associated with a small (15%) reduction in postmenopausal BC risk, but further studies are needed to confirm these results. | // | // |
| Wu 2008 [9] | Not reported | Overall, data based on Asian women showed a dose-dependent statistically significant association between soy food intake and BC risk reduction; soy intake was unrelated to BC risk in studies conducted on Western populations. | // | // |
| Wu 2015 [33] | Different units used to assess food intakes among the studies; dose-response analysis was not conducted; possible measurement errors and analysis unadjusted for potential confounding factors. | High fruit and vegetable consumption, as a protective measure, can reduce the incidence of BC in Chinese women. High fruit consumption protects against BC (higher soy food consumption induces a 69% reduction in BC risk). High-fat food consumption may increase BC risk. | Newcastle–Ottawa quality assessment Scale (NOS)—9 pt scoring system | Eleven studies were “higher-quality” (≥7 pt) and eleven were “lower-quality” (<7 pt) |
| Yang 2014 [49] | Potential publication bias (small studies with null results tend not to be published); any measurement error and resulting misclassification would most likely lead to an attenuation of the true association; dietary questionnaires are liable to measurement errors (reporting bias or inaccurate databases); potential residual confounding factors not excluded. | Findings provide conclusive evidence to support increasing n-3/n-6 PUFA intake for BC prevention. For every 1/10 increment in n-3/n-6 PUFA there was a 6% reduction in BC risk; importance of promoting nutritional education (increasing the consumption of marine foods). | Newcastle–Ottawa quality assessment Scale (NOS)—9 pt scoring system | Six studies were classified as “high-quality” (≥8 pt), five as “moderate-quality” (<8 pt) |
| Zang 2015 [27] | Potential confounding factors inherent in the original study design; misclassification of dairy food consumption (self-reporting system) may cause incorrect estimates; potential methodological differences between studies; use of case-control studies may provide a lower level of evidence. | Dairy food consumption was inversely associated with BC risk; possible association between high dairy food consumption and beneficial environmental factors (economic status, physical activity, healthier lifestyle). | Newcastle–Ottawa quality assessment Scale (NOS)—9 pt scoring system | Twelve studies scored 8 pts, nine scored 7 pts, and six scored 6 pts |
| Zheng 2013 [50] | Different assessment methods; limited data available on individual n-3 PUFA; potential residual confounders not analyzed; possible language bias. | This meta-analysis provided strong and solid evidence of marine n-3 PUFA intake being inversely associated with risk of BC. | Newcastle–Ottawa quality assessment Scale (NOS)—9 pt scoring system | Studies were of “moderate-quality“ (5–7 pt) and “higher-quality” (>7 pt) |
| Zhou 2015 [51] | Selection bias might be unavoidable; relatively limited amount of data included in the meta-analysis; potential measurement errors and misclassification; unmeasured or residual confounders might affect the association between linoleic acid and BC risk | This meta-analysis suggested that linoleic acid is associated with a lower risk of BC, but none of the associations were statistically significant. | Newcastle–Ottawa quality assessment Scale (NOS)—9 pt scoring system | Four studies scored 6/9 pts, ten studies scored 7/9 pts |
| Conclusion and quality assessment of pooled analysis included in the umbrella review (4) | ||||
| Mannisto 2005 [16] | // | The results supported the suggestion deriving from relatively recent epidemiological research that diet may not have an important role in the etiology of BC. The possible protective effect of “Pork, Processed Meat, Potatoes” dietary pattern in the NLCS cohort could be explained by a difference in that pattern for NLCS (type of food included in the FFQs). | // | // |
| Missmer 2002 [22] | Inability to assess the effect of how food was cooked and for how long (data not collected); possible measurement errors not collected. | This large study does not provide evidence of a diet rich in meat and dairy products increasing the risk of BC. | // | // |
| Smith-Warner 2001 (a) [46] | Possible errors in estimates of consumption (over- or under-estimation); possible methodological errors in study design. | The pooled analysis suggested only a weak positive association for replacing saturated fat consumption with carbohydrate consumption; none of the other types of fat examined were associated with BC risk; these results, though not significant, are compatible with a lower BC risk observed for higher intakes of olive oil (rich source of monounsaturated fat) in studies conducted in Mediterranean countries. | // | // |
| Smith-Warner 2001 (b) [39] | Differences in study design; numerous fruit and vegetable categories reported in the studies; possible publication bias. | The results suggest that fruit and vegetable consumption in adulthood is not significantly associated with BC risk (BC risk only 3% to 9% lower in women in the highest decile of fruit or vegetable consumption). No specific fruits or vegetables had strong and significant association with BC risk. | // | // |
| Conclusion and quality assessment of systematic reviews included in the umbrella review (5) | ||||
| Albuquerque 2013 [17] | No summary estimate measure was produced; instruments used to collect dietary information differed among the studies; FFQs, used in most cases, are liable to measurement error and might not detect a significant association; great variability among the studies; possibility of recall or selection bias. | The results suggest that a dietary pattern characterized by vegetables, fruit, fish and soy (healthy), or the Mediterranean diet reduces the risk of BC. A positive association was observed for the Western dietary pattern, but most of these results were not statistically significant. Efforts are expected to aid future research. | Strobe Checklist | // |
| Farsinejad-Marj 2015 [18] | Scarcity of studies, no assessment of factors hypothesized to relate to BC (breastfeeding, adiposity, physical activity, genetic background, insulin resistance, and chronic inflammation). Few studies separately investigated risk of BC in pre- and post-menopausal women. Different components of the MD can act synergistically in reducing BC risk so it is important to consider all components of the MD in studies. | Case-cohort studies found an inverse association between the MD and BC risk in pre- and post-menopausal women, but cohort studies reported controversial results. It seems that there are insufficient data to reach a conclusion about the effect of MD on BC risk before and after menopause, but there is some evidence to suggest a protective association. More cohort studies need to be conducted in different parts of the world to confirm these results. | // | // |
| Michels 2007 [28] | Possible measurement error (FFQs); great heterogeneity in dietary patterns among different countries; timing in diet; possible inadequate follow-up in studies. | There was no consistent strong and statistically significant association between diet and BC risk. | // | // |
| Mourouti 2013 [34] | Possible recall bias; variation in exposure measures used in the studies; variation in the amount and type of soy consumed and in the sample size may have over- or under- estimated the true effect sizes measured. Potential dietary measurement error may mask the true relationship. | The majority of the studies (66%) revealed a statistically significant inverse association between soy and isoflavones consumption and BC risk. Limitations in the study design may mask the real associations. | // | // |
| Mourouti 2014 [21] | Differences in experimental design and habits among study populations; lack of sufficient follow-up in the studies; methodological problems with the assessment tools used in each study. | No consistent and statistically strong association emerged between BC incidence and dietary factors; soy food and isoflavone intake seemed to protect against BC, mainly in Asian populations; no association reported for the consumption of dietary carbohydrates, GI or GL, dietary fiber intake and the risk of BC. The consumption of dietary fat probably raises the risk of BC. The studies that examined the role of fruit, vegetable and meat intake provide inconsistent results. | // | // |
| Conclusion and quality assessment of qualitative reviews included in the umbrella review (7) | ||||
| Cui 2006 [54] | Possible selection bias due to case-control study design; shortcomings in methodology and summary estimate measures. | Despite inconsistent results from the epidemiological studies, some evidence indicates that vitamin D and calcium might have a protective role against BC. Experimental evidence suggests that the association between vitamin D intake and BC may be stronger for premenopausal than for postmenopausal women. Further analyses are required to assess this interaction. | // | // |
| Duffy 2007 [35] | Not reported | Early exposure in childhood or adolescence may have a protective effect against BC. | // | // |
| Eichholzer 2001 [57] | Not reported | High folate intake may be associated with a lower risk of BC in women at high risk (alcohol users). | // | // |
| Hanf 2005 [23] | Not reported | Regional differences in BC incidence are probably partially attributable to lifelong dietary habits. | // | // |
| Lof 2006 [36] | Potential misclassification of phytoestrogen intake due to measurement associated with dietary assessment; potential recall bias in retrospective studies. | Epidemiological data seem to support a small protective effect of isoflavones against BC; as for lignans and BC, the results are somewhat inconsistent, but the protective effect might be limited to premenopausal women. | // | // |
| Peeters 2003 [37] | None of the studies considered age at time of consumption, which seems to be important in BC development; methodological differences between the studies are too large to estimate any summary effect; limited number of epidemiological studies on phytoestrogens and BC. | None of the studies found evidence for an increased risk of BC with an increased phytoestrogen intake. | // | // |
| Rossi 2014 [60] | Limitations due to study design (methodological shortcomings and lack of association measures). | Nutritional factors might have a role in the development of BC; red meat intake and dietary sugar should be reduced, whereas increased fish intake appears to be protective; fruit and vegetables, including polyphenols, have shown promising results. Prospective randomized trials are needed to develop population-based prevention strategies for BC. | // | // |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buja, A.; Pierbon, M.; Lago, L.; Grotto, G.; Baldo, V. Breast Cancer Primary Prevention and Diet: An Umbrella Review. Int. J. Environ. Res. Public Health 2020, 17, 4731. https://doi.org/10.3390/ijerph17134731
Buja A, Pierbon M, Lago L, Grotto G, Baldo V. Breast Cancer Primary Prevention and Diet: An Umbrella Review. International Journal of Environmental Research and Public Health. 2020; 17(13):4731. https://doi.org/10.3390/ijerph17134731
Chicago/Turabian StyleBuja, Alessandra, Marco Pierbon, Laura Lago, Giulia Grotto, and Vincenzo Baldo. 2020. "Breast Cancer Primary Prevention and Diet: An Umbrella Review" International Journal of Environmental Research and Public Health 17, no. 13: 4731. https://doi.org/10.3390/ijerph17134731
APA StyleBuja, A., Pierbon, M., Lago, L., Grotto, G., & Baldo, V. (2020). Breast Cancer Primary Prevention and Diet: An Umbrella Review. International Journal of Environmental Research and Public Health, 17(13), 4731. https://doi.org/10.3390/ijerph17134731