1. Introduction
Repeatability and precision are major factors which influence final implant treatment results. There is no doubt that clinicians should plan implant procedures based on careful clinical examination and analysis of CBCT (Cone beam computed tomography) scans to choose the best treatment option [
1].
However, in some cases, inaccuracies are introduced while transferring a virtual treatment plan to the patient’s mouth. Several different kinds of guide templates have been introduced to provide proper positioning and angulation of implants in the bone [
2]. Implant placement in respect of the prosthodontic plan plays a crucial role in the long-term predictability and success of implant prosthetics. Moreover, a prosthetically-driven implant placement accomplished with a surgical guide can decrease clinical and laboratory complications. Increase of demand for dental implants has resulted in the development of state-of-the-art techniques for the fabrication of these templates [
1].
A number of studies show that users of CAD/CAM (Computer-aided design/Computer-aided manufacturing) surgical guides may experience problems with accuracy and repeatability of dental implantation procedures [
2,
3,
4,
5,
6,
7,
8]. In the literature we can also find descriptions of a few problems with clinical application of guides (e.g., the guide fixation, its stability and limited mouth opening) [
9,
10]. Hence several surgical kits were introduced to help clinicians with proper implant positioning when a digital guide is not available.
The aim of this study was to evaluate the repeatability of freehand implant procedures assisted with special plastic sleeves which are placed on implant drills to assure the proper mesiodistal distance from patient teeth or anteriorly prepared implant sites.
2. Materials and Methods
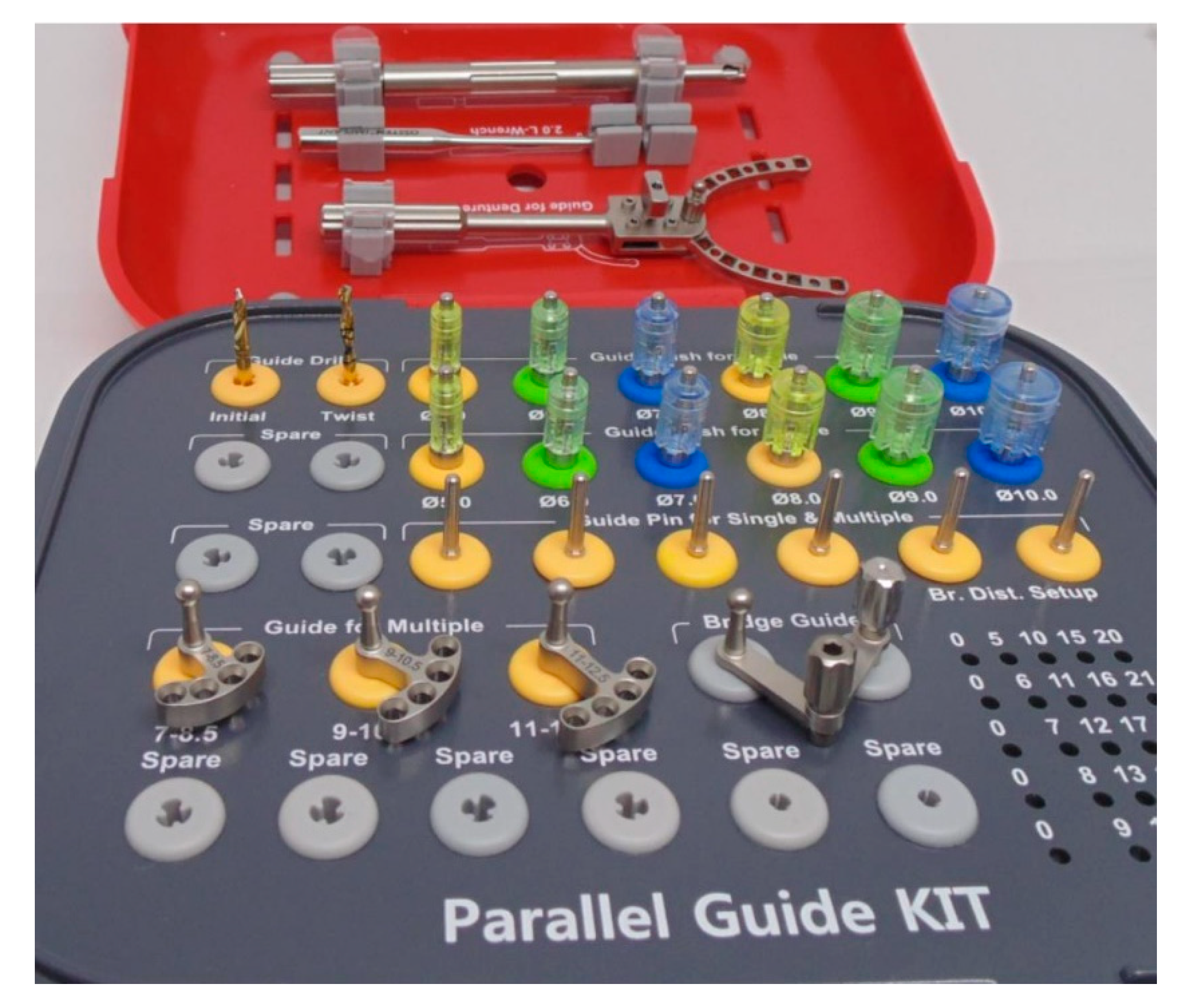
The following experiment was planned to check repeatability of implant procedures with a kit that includes plastic sleeves of different diameters corresponding to the mesiodistal dimensions of different teeth (Parallel Guide Kit, Osstem Implants, Seoul, Korea) (
Figure 1).
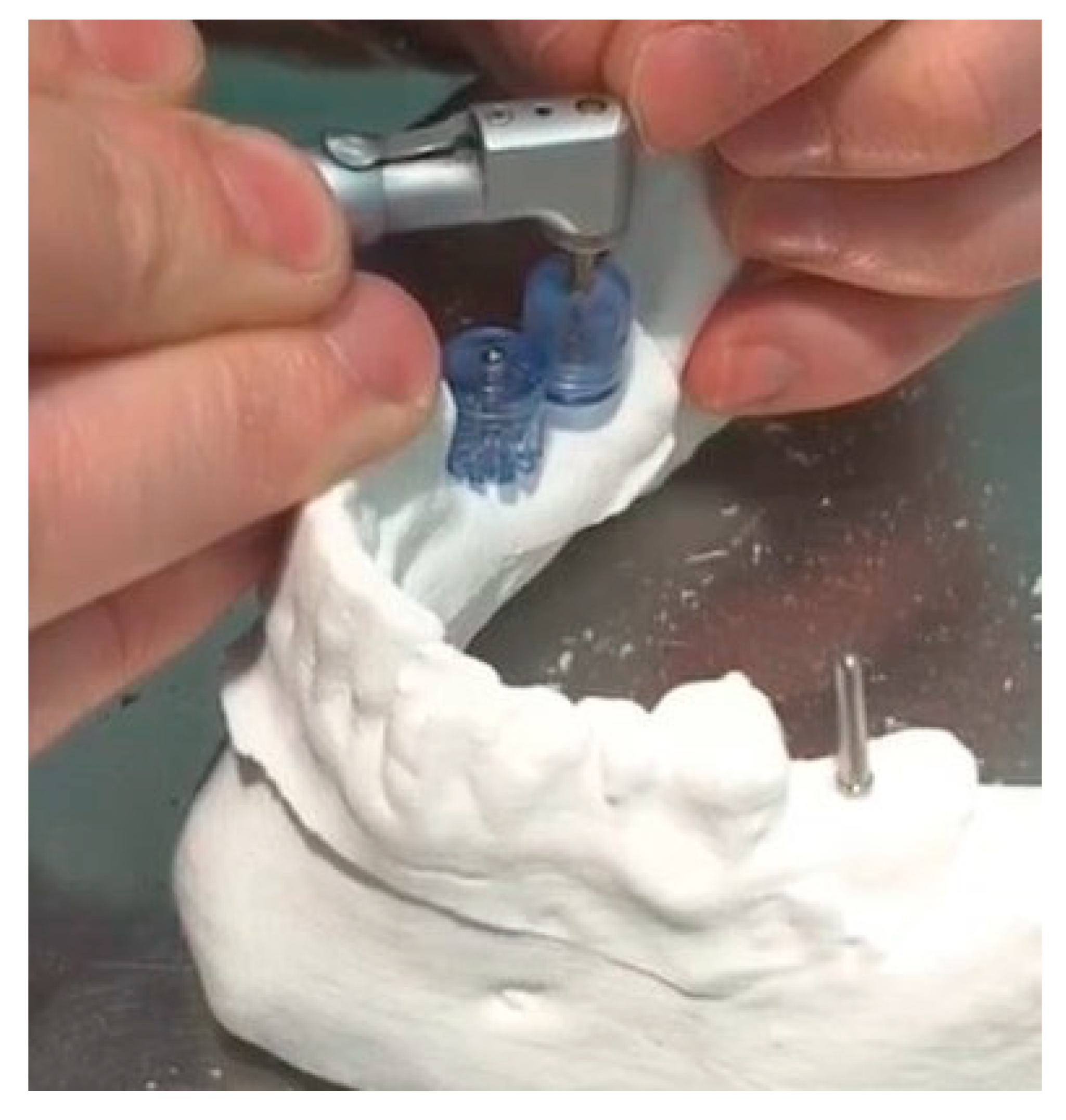
Patient data required for implant treatment, like an image of the mandible from a CBCT scan and a virtual model of soft tissues and teeth, were used to prepare a complete virtual model of patients’ clinical conditions. For this purpose, DDS-Pro software (JST, Częstochowa, Poland) for virtual treatment planning was used. The same software was used for supporting the diagnosis process and for choosing the best place for implantation. The model was saved as an STL file and 3D printed in five copies in a SONDASYS SL01 device using Selective Laser Sintering (SLS) technology (material: polyamide powder with aluminum nanofiller and fiberglass, Sondasys, Ogrodzieniec, Poland). Drilling procedures were done with a Parallel Guide Kit. Positions of implants were chosen to be placed with the use of 10 mm diameter sleeves for each implant. The sleeves touched the distal surface of tooth 36 at position 37, the distal surface of tooth 45 at position 46, and the 10 mm sleeve already placed on a guide pin at tooth 46 in position 47.
After preparing osteotomies, guide pins were placed and each model was scanned with an optical scanner (Cs3600, Carestream, Atlanta, GA, USA) to create a 3D model in the STL file. Each one of 5 STL files was then compared with four others using free software HP 3D Scan 5 (HP, Palo Alto, CA, USA). The method of measurement is shown in
Figure 1.
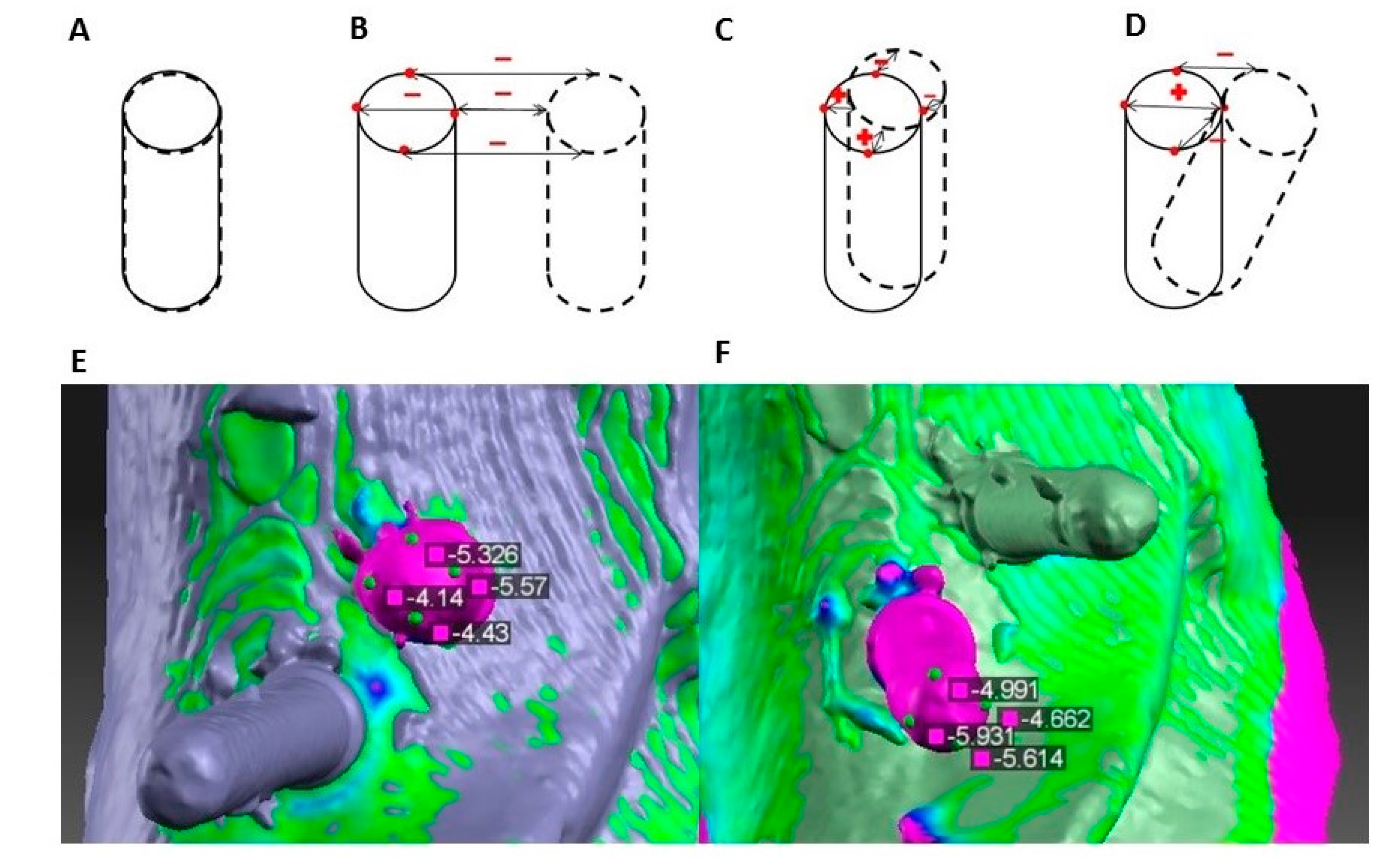
After preparing the implant sites, guide pins were placed and each model was scanned with an optical scanner (Cs3600, Carestream) to create a 3D model as an STL file. Each one of 5 STL files was then compared with four others using HP 3D Scan 5 software (HP, Palo Alto, CA, USA). The method of measurement is shown in
Figure 2.
STL files show the object surface as a set of triangles. Surfaces of all five models were almost the same outside of the place of the guide pins. Because of this, it was possible to align scans with each other. On the model which served as a reference in this measurement, four reference points were marked on each of the guide pin tops based on their geometric structure. After comparing, surface software showed values of deviation in each point: pm—mesial point, pd—distal point, pl—lingual point, pb—buccal point. In each of the series of measurements these points were marked only once, so when test models were changed, they stayed in exactly the same place on the reference model. Thus, benchmarks for assessing similarity of particular samples were the same.
Sixty measurements were made in all—each of the five models with 3 guide pins was both a test and a reference.
Figure 2 also shows how the deviation values changed depending on which model was the reference one.
Values of deviation on all points were recorded for each guide pin for each measurement. All data was reported as the mean ± standard deviation. Correlations between implant placement and level of average deviation on guide pins were analyzed by chi square test. Statistical analyses were performed using Microsoft Office Excel for Windows (Microsoft 2018, Redmond, WA, USA). A p-palue < 0.01 was considered significant.
3. Results
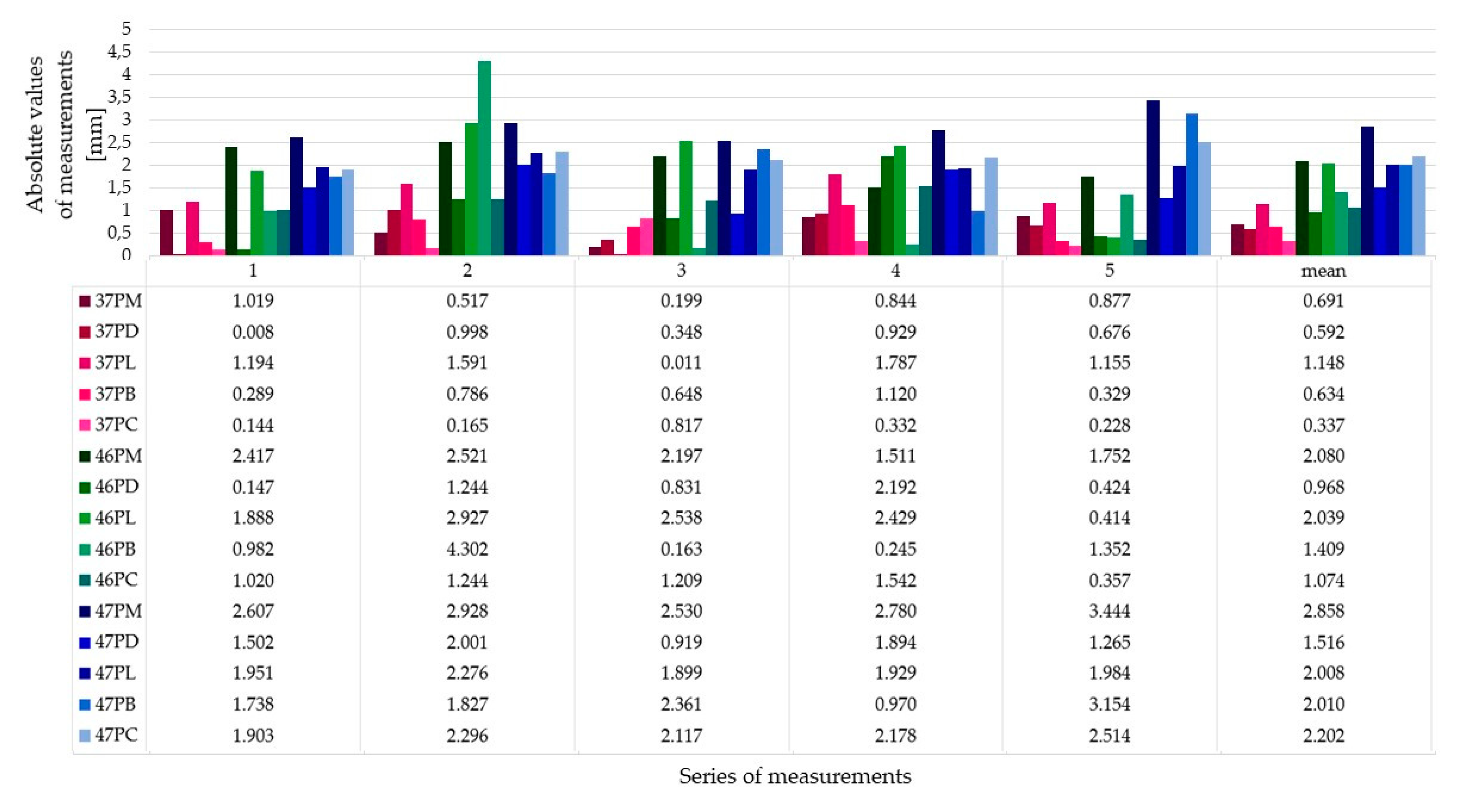
Figure 3 shows the absolute values of measurements (mm) in each of the measurement series. This figure is an overview of our results.
The average deviation was −1.38 ± 1.4 mm. The differentiation of deviation values depended on implant placement. The standard deviation value indicated that the differentiation of samples was high, despite the fact that average deviation was low. This observation suggested that there is a correlation between the benchmark for implantation and its repeatability. Average deviation on the guide pin placed at position 37 was −0.46 ± 0.59 mm, and at position 46 it was −1.46 ± 0.88 mm. During implantation of these 10 implants, the plastic sleeve touched the previous tooth. Implant sites at position 47 were prepared with another 10mm sleeve touching the 10 mm sleeve on the pin guide at position 46. The average deviation in this group of five guide pins was the highest: −2.69 ± 1.62 mm. Analyzing the results one has to consider that the crest of the ridge in areas 46 and 47 was tilted buccally compared to the more even and flat crest at site 36 (
Figure 4 and
Figure 5).
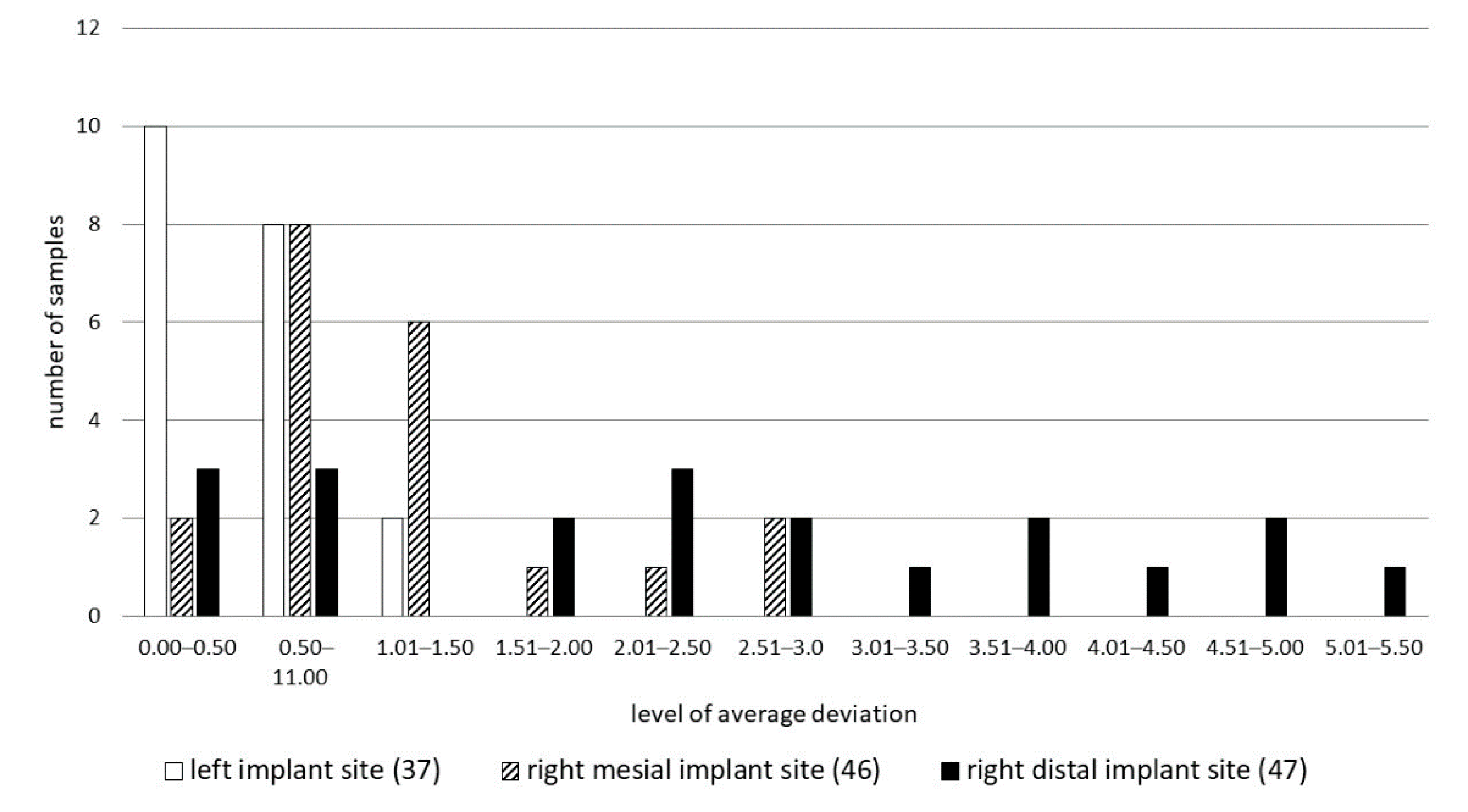
Figure 6 presents the results of a chi square test. All twenty samples are matched to one of the levels of possible average deviation. The results of the chi square test allow us to reject the hypothesis about quality independence. As we can see on the bar chart only right mesial implants have the highest levels of average deviation. This group was also characterized by the highest differentiation.
4. Discussion
In vitro studies provide stable conditions during series of procedures. Three-dimensional printed models properly represent the shape of the alveolar bone. The authors must mention that a limitation of this study is that the material which was used for model manufacturing was harder than bone, which caused initial difficulties with drilling. The material which was cut during implant site preparation was depositing on the drill, making it difficult to perform full-depth insertion. However, these models and digital methods of sample comparison contribute to eliminating invasive procedures and increasing objectivity and precision of measurements.
The main purpose of this examination was to evaluate repeatability of freehand implant procedures assisted with special plastic sleeves. The results of this study show that using such support could help improve the precision of freehand implant surgery in the case of replacing a single missing tooth but is not as good as using individual implant guides.
In the research by Vermeulen et al., where the accuracy of implant placement with and without using implant guide templates was examined, it was shown that average deviation for placement with a guide was 0.42 ± 0.52 mm and without a guide was 1.27 ± 1.28 mm [
11]. As we can see, the average deviation of freehand implant placement without any assistance is even slightly lower than with the support of plastic sleeves. This incoherence could be caused by different methods of measurement and sample size.
The meta-analysis of Tahmaseb et al., based on 20 clinical studies including placing 2238 implants using static guides in 471 patients, revealed a total mean error of 1.2 mm (1.04 mm to 1.44 mm) at the entry point, 1.4 mm (1.28 mm to 1.58 mm) at the apical point and deviation of 3.5° (3.0° to 3.96°). This meta-analysis, as well as the present study, both emphasize statistical significance differences in accuracy in favor of partial edentulous compared to full edentulous cases [
12].
Analysis of in vitro studies and systematic review, as well as multicenter clinical trials and randomized controlled trials, lead to the conclusion that using individual guides may be the best way to achieve elevated accuracy and remain in line with the treatment plan [
7,
8,
10,
11,
12,
13,
14]. However, limited surgical access especially in the distal area of the alveolar ridge with surgical guides intraorally, may be one of the most common challenges in using surgical guides [
4,
14]. Tallarico et al. found that even if the accuracy of guided surgeries in the anterior region was more than good, accuracy dropped in the distal area where some guide movement may occur, or open sleeve design has to be applied. However, the same author in another study comparing guided and freehand approaches achieved successful results over the five-year follow-up period for both techniques. Clinically we have to evaluate all advantages and limitations of guided implant surgeries, such as surgical time, level of post-operative pain and swelling, and overall costs and time required to perform a fully guided surgery [
2,
14,
15]. Proper and careful diagnosis is the basis of present-day implantology. The whole process of preparing digital implant templates forces clinicians to carefully analyze CBCT scans as well as intraoral scans, or stone or virtual models and leads to careful planning of each specific case [
16]. Considering individuals’ needs as well as clinical limitations including surgical access and guide fixation, as well as costs required to produce the guide, clinicians may decide to use simpler and less expensive tools to transfer the digital plan to the patient’s mouth.
5. Conclusions
Within the limitations of this in vitro study, the following conclusion was drawn: using universal plastic sleeves could improve implant procedure precision over a freehand approach especially in the case of partially edentulous patients. The authors believe that clinical scientific research should focus more in identifying which clinical situations can get the greatest benefits from implant guided surgery and which interventions may be performed successfully, faster or more cheaply with the use of different tools, e.g., the kit used in this study.
Regarding further studies by means of 3D printed models, there is a need to analyze which 3D printing material will be most appropriate in terms of consistency, strength and hardness. Furthermore, there is still a need for more studies such as randomized controlled trials that comprehensively assess the advantages and disadvantages of fully digital surgical protocols in specific clinical situations.
Author Contributions
Conceptualization, Ł.Z.; methodology, Ł.Z.; software, M.C.; validation, Ł.Z., M.C., L.W.; formal analysis, M.C., L.W.; investigation, Ł.Z., M.C., L.W.; resources, Ł.Z.; data curation, Ł.Z.; writing—original draft preparation, M.C.; writing—review and editing, Ł.Z., L.W., E.M.; visualization, M.C.; supervision, E.M.; project administration, Ł.Z., L.W.; funding acquisition, Ł.Z. All authors have read and agreed to the published version of the manuscript.
Funding
The study was carried out as a part of a project in the field of scientific developmental research aimed at the development of young scientists and participants of PhD studies, financed within the scientific activity of the Medical University of Warsaw, Poland.
Acknowledgments
The study was done under a statutory grant for Department of Dental Propaedeutics and Prophylaxis Medical University of Warsaw, Poland. We appreciate the help from SondaSYS Company (Poland) for printing models by SLS technology and Optident Company (Poland) for 3D scanning. All the authors would like to thank them for their time and commitment.
Conflicts of Interest
All authors declare that they have no competing interests connected with this study. Łukasz Zadrożny is a consultant for Osstem AIC, but the study fully belongs to the authors and was prepared as a scientific activity of the Medical University of Warsaw. No company has influenced the design or results of this study.
References
- Ganz, S.D. Presurgical planning with CT-derived fabrication of surgical guides. J. Oral Maxillofac. Surg. 2005, 63 (Suppl. S2), 59–71. [Google Scholar] [CrossRef] [PubMed]
- Mouhyi, J.; Salama, M.A.; Mangano, F.G.; Mangano, C.; Margiani, B.; Admakin, O. A novel guided surgery system with a sleeveless open frame structure: A retrospective clinical study on 38 partially edentulous patients with 1 year of follow-up. BMC Oral Health 2019, 19, 253. [Google Scholar] [CrossRef] [PubMed]
- Schnutenhaus, S.; von Koenigsmarck, V.; Blender, S.; Ambrosius, L.; Luthardt, R.G.; Rudolph, H. Precision of sleeveless 3D drill guides for insertion of one-piece ceramic implants: A prospective clinical trial. Int. J. Comput. Dent. 2018, 21, 97–105. [Google Scholar] [PubMed]
- Zweifel, D.; Bredell, M.G.; Lanzer, M.; Rostetter, C.; Rücker, M.; Studer, S. Precision of simultaneous guided dental implantation in microvascular fibular flap reconstructions with and without additional guiding splints. J. Oral Maxillofac. Surg. 2019, 5, 971–976. [Google Scholar] [CrossRef] [PubMed]
- Park, C.; Raigrodski, A.J.; Rosen, J.; Spiekerman, C.; London, R.M. Accuracy of implant placement using precision surgical guides with varying occlusogingival heights: An in vitro study. J. Prosthet. Dent. 2009, 101, 372–381. [Google Scholar] [CrossRef]
- Nickenig, H.J.; Eitner, S.; Rothamel, D.; Wichmann, M.; Zöller, J.E. Possibilities and limitations of implant placement by virtual planning data and surgical guide templates. Int. J. Comput. Dent. 2012, 15, 9–21. [Google Scholar] [PubMed]
- Nickenig, H.J.; Wichmann, M.; Hamel, J.; Schlegel, K.A.; Eitner, S. Evaluation of the difference in accuracy between implant placement by virtual planning data and surgical guide templates versus the conventional free-hand method—A combined in vivo—In vitro technique using cone-beam CT (Part II). J. Cranio Maxillofac. Surg. 2010, 38, 488–493. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.H.; An, S.Y.; Hong, M.H.; Jeon, K.B.; Lee, K.B. Accuracy of a direct drill-guiding system with minimal tolerance of surgical instruments used for implant surgery: A prospective clinical study. J. Adv. Prosthodont. 2016, 8, 207–213. [Google Scholar] [CrossRef] [PubMed]
- Mai, H.N.; Choi, S.Y.; Lee, S.T.; Lee, D.H. Optimizing accuracy in computer-guided implant surgery with a superimposition-anchor microscrew system: A clinical report. J. Prosthet. Dent. 2018, 120, 789.e1–789.e5. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.D.; Mai, H.N.; Mai, H.Y.; Ha, J.H.; Li, L.J.; Lee, D.H. The Effects of Distribution of Image Matched Fiducial Markers on Accuracy of Computer-Guided Implant Surgery. J. Prosthodont. 2020. [Google Scholar] [CrossRef] [PubMed]
- Vermeulen, J. The Accuracy of Implant Placement by Experienced Surgeons: Guided vs. Freehand Approach in a Simulated Plastic Model. Int. J. Oral Maxillofac. Implant. 2017, 32, 617–624. [Google Scholar] [CrossRef] [PubMed]
- Tahmaseb, A.; Wu, V.; Wismeijer, D.; Coucke, W.; Evans, C. The accuracy of static computer-aided implant surgery: A systematic review and meta-analysis. Clin. Oral Implant. Res. 2018, 29 (Suppl. S16), 416–435. [Google Scholar] [CrossRef] [PubMed]
- Tallarico, M.; Kim, Y.J.; Cocchi, F.; Martinolli, M.; Meloni, S.M. Accuracy of newly developed sleeve-designed templates for insertion of dental implants: A prospective multicenters clinical trial. Clin. Implant Dent. Relat. Res. 2019, 21, 108–113. [Google Scholar] [CrossRef] [PubMed]
- Tallarico, M.; Esposito, M.; Xhanari, E.; Caneva, M.; Meloni, S.M. Computer-guided vs. freehand placement of immediately loaded dental implants: 5-year postloading results of a randomised controlled trial. Eur. J. Oral Implantol. 2018, 11, 203–213. [Google Scholar] [PubMed]
- Colombo, M.; Mangano, C.; Mijiritsky, E.; Krebs, M.; Hauschild, U.; Fortin, T. Clinical applications and effectiveness of guided implant surgery: A critical review based on randomized controlled trials. BMC Oral Health 2017, 17, 150. [Google Scholar] [CrossRef] [PubMed]
- Mangano, F.G.; Veronesi, G.; Hauschild, U.; Mijiritsky, E.; Mangano, C. Trueness and Precision of Four Intraoral Scanners in Oral Implantology: A Comparative in Vitro Study. PLoS ONE 2016, 11, e0163107. [Google Scholar] [CrossRef] [PubMed]
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}





