Characteristics of and Public Health Emergency Responses to COVID-19 and H1N1 Outbreaks: A Case-Comparison Study

 ,
,
Abstract
1. Introduction
2. Methods
2.1. Data Collection
2.2. Comparison Content
3. Results
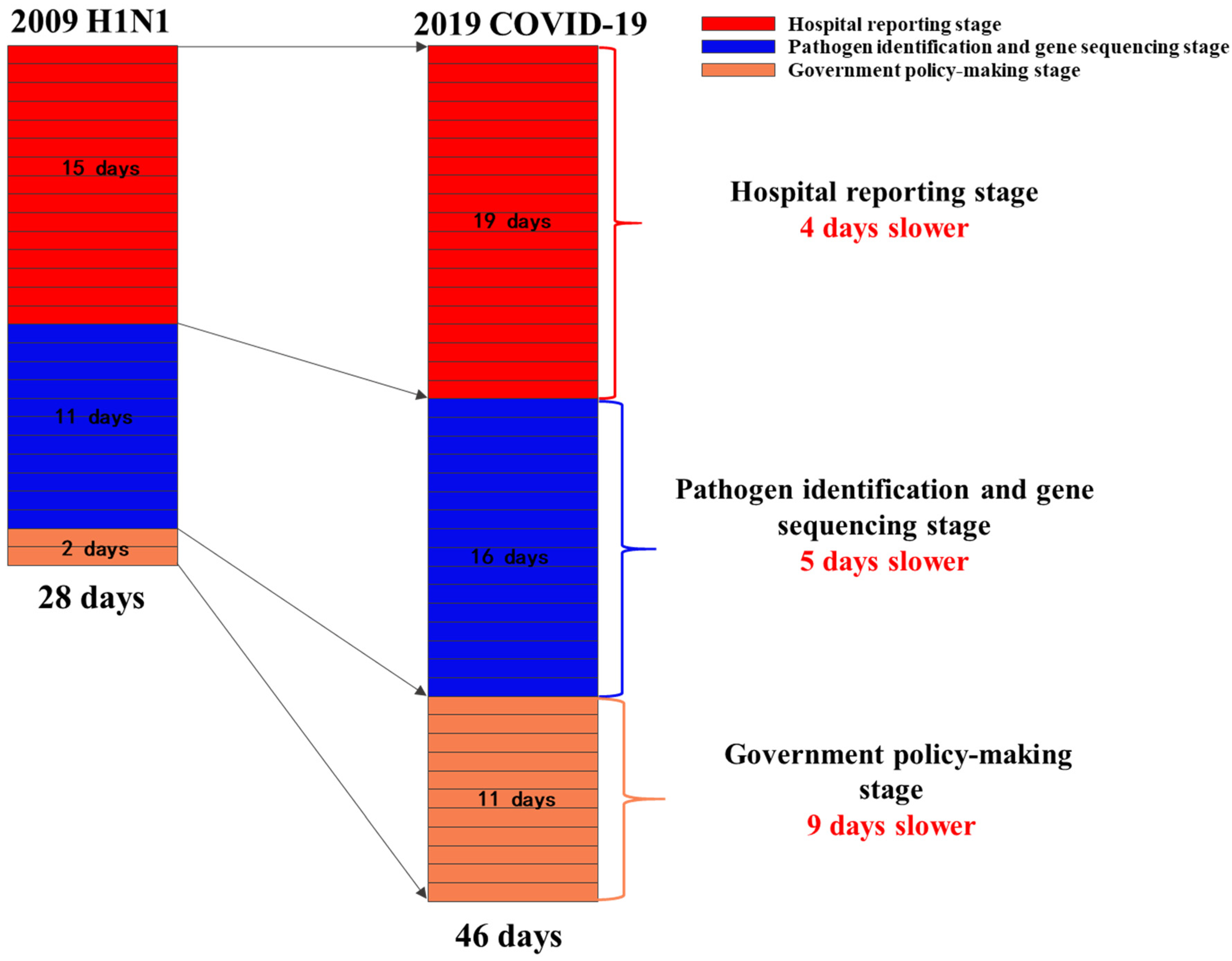
3.1. Hospital Reporting Stage
3.1.1. H1N1 Swine Influenza (2009)
3.1.2. COVID-19 (2019)
3.2. Pathogen Identification and Virus Gene Sequencing Stage
3.2.1. H1N1 Swine Influenza (2009)
3.2.2. COVID-19 (2019)
3.3. Government Policy-Making Stage
3.3.1. H1N1 Swine Influenza (2009)
3.3.2. COVID-19 (2019)
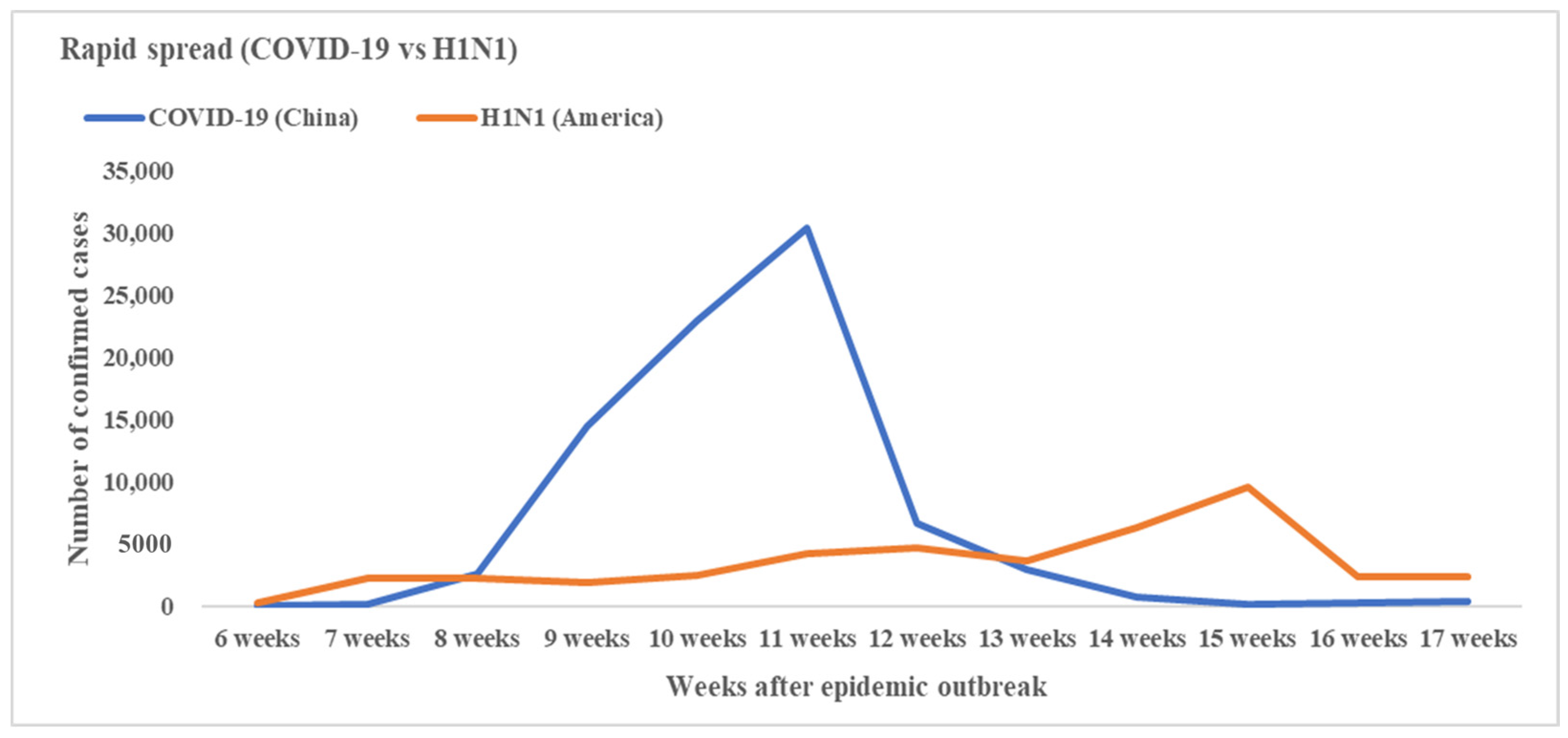
3.4. The Epidemic Spread Speed and Peak Time of COVID-19 and H1N1
3.4.1. H1N1 Swine Influenza (2009)
3.4.2. COVID-19 (2019)
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Callaway, E.; Cyranoski, D.; Mallapaty, S.; Stoye, E.; Tollefson, J. The coronavirus pandemic in five powerful charts. Nature 2020, 579, 482–483. [Google Scholar] [CrossRef] [PubMed]
- Wuhan Municipal Health Commission. Report of Clustering Pneumonia of Unknown Etiology in Wuhan City. Available online: http://wjw.wuhan.gov.cn/front/web/showDetail/20191231089892019 (accessed on 31 December 2019).
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- HuiDS, E.I.A.; Madani, T.A.; Ntoumi, F.; Kock, R.; Dar, O. The continuing 2019-nCoV epidemic threat of novel coronaviruses to global health—The latest 2019 novel coronavirus outbreak in Wuhan, China. Int. J. Infect. Dis. 2020, 91, 264–266. [Google Scholar]
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19—11 March 2020. Available online: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-20202020 (accessed on 11 March 2020).
- DX Docor. COVID-19 Global Pandemic Real-Time Report. Available online: https://ncov.dxy.cn/ncovh5/view/en_pneumonia?from=dxy&source=&link=&share=2020 (accessed on 5 April 2020).
- World Health Organization. World Now at the Start of 2009 Influenza Pandemic. Available online: https://www.who.int/mediacentre/news/statements/2009/h1n1_pandemic_phase6_20090611/en/2009 (accessed on 11 June 2009).
- CDC. Outbreak of Swine-Origin Influenza A (H1N1) Virus Infection -Mexico, March–April 2009. Morb. Mortal. Wkly. Rep. 2009, 58, 467–470. [Google Scholar]
- CDC. Swine influenza A (H1N1) infection in two children—Southern California, March–April 2009. MMWR Morb. Mortal. Wkly. Rep. 2009, 58, 400–402. [Google Scholar]
- Brockmann, D.; Helbing, D. The hidden geometry of complex, network-driven contagion phenomena. Science 2013, 342, 1337–1342. [Google Scholar] [CrossRef] [PubMed]
- Butler, D. Portrait of a year-old pandemic. Nature 2010, 464, 1112–1113. [Google Scholar] [CrossRef] [PubMed]
- Fowlkes, A.L.; Arguin, P.; Biggerstaff, M.S. Epidemiology of 2009 Pandemic Influenza A (H1N1) Deaths in the United States, April-July 2009. Clin. Infect. Dis. 2010, 52, 60–68. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Ji-Eun Park, Y.R. Transmissibility and severity of influenza virus by subtype. Infect. Genet. Evol. 2018, 65, 288–292. [Google Scholar] [CrossRef] [PubMed]
- Sebastian, M.R.L.R.; Kabra, S.K. Swine origin influenza (swine flu). Indian J. Pediatr. 2009, 76, 833–841. [Google Scholar] [CrossRef] [PubMed]
- Epidemiology Working Group for Ncip Epidemic Response. [The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19) in China]. Zhonghua Liu Xing Bing Xue Za Zhi 2020, 41, 145–151. [Google Scholar]
- Verikios, G.S.M.; Stojanovski, P. Assessing Regional Risks from Pandemic Influenza: A Scenario Analysis. World Econ. 2016, 39, 1225–1255. [Google Scholar] [CrossRef]
- CDC. The 2009 H1N1 Pandemic: Summary Highlights, April 2009–April 2010. Available online: https://www.cdc.gov/h1n1flu/cdcresponse.htm2010 (accessed on 5 April 2020).
- Hubei Provincial Government. Circular of Hubei Provincial People’s Government on Strengthening Pneumonia Prevention and Control of New Coronavirus Infection. Available online: http://www.hubei.gov.cn/xxgk/gsgg/202001/t20200122_2013895.shtml2020 (accessed on 22 January 2020).
- Wuhan Municipal Health Commission. Experts Interpret the Latest Notice of Viral Pneumonia of Unknown Causes. Available online: http://wjw.wuhan.gov.cn/front/web/showDetail/20200111090362020 (accessed on 11 January 2020).
- National Health Commission of the People’s Republic of China. Available online: http://www.nhc.gov.cn/ (accessed on 5 April 2020).
- CCTV. Novel Coronavirus! Preliminary Determination of the “Culprit” of Unexplained Pneumonia in Wuhan. Available online: http://m.news.cctv.com/2020/01/09/ARTI9Vp9Lra4Tvltz3r7es96200109.shtml2020 (accessed on 9 January 2020).
- YiMagazine. Wuhan Epidemic Core Timeline. Available online: https://j-x.gitee.io/home/nCovTimeline2020 (accessed on 9 February 2020).
- CDC. H1N1 Flu (Swine Flu): Past Situation Updates. Available online: https://www.cdc.gov/h1n1flu/updates/ (accessed on 5 April 2020).
- CDC. Update: Swine influenza A (H1N1) infections—California and Texas, April 2009. MMWR Morb. Mortal. Wkly. Rep. 2009, 58, 435–437. [Google Scholar]
- World Health Organization. Influenza A (H1N1)—Update 23. Available online: https://www.who.int/csr/don/2009_05_09/en/2009 (accessed on 5 April 2020).
- Nature, After the pandemic. Nature 2010, 466, 903. Available online: https://www.nature.com/articles/466903b#citeas (accessed on 5 April 2020). [CrossRef] [PubMed][Green Version]
- World Health Organization. H1N1 in Post-Pandemic Period. Available online: https://www.who.int/mediacentre/news/statements/2010/h1n1_vpc_20100810/en/2010 (accessed on 5 April 2020).
- Ding, L.; Cai, W.; Ding, J.Q. An interim review of lessons from the Novel Coronavirus (SARS-CoV-2) outbreak in China. Sci. Sin. Vitae 2020, 50, 247–257. [Google Scholar]
- Vincent, A.L.; Ma, W.; Lager, K.M.; Janke, B.H.; Richt, J.A. Swine influenza viruses a North American perspective. Adv. Virus Res. 2008, 72, 127–154. [Google Scholar] [PubMed]
- Vincent, A.L.; Swenson, S.L.; Lager, K.M.; Gauger, P.C.; Loiacono, C.; Zhang, Y. Characterization of an influenza A virus isolated from pigs during an outbreak of respiratory disease in swine and people during a county fair in the United States. Vet. Microbiol. 2009, 137, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Newman, A.P.; Reisdorf, E.; Beinemann, J.; Uyeki, T.M.; Balish, A.; Shu, B. Human case of swine influenza A (H1N1) triple reassortant virus infection, Wisconsin. Emerg. Infect. Dis. 2008, 14, 1470–1472. [Google Scholar] [CrossRef] [PubMed]
- Anderson, R.M.; Heesterbeek, H.; Klinkenberg, D.; Hollingsworth, T.D. How will country-based mitigation measures influence the course of the COVID-19 epidemic? Lancet 2020, 395, 931–934. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | H1N1 | COVID-19 |
|---|---|---|
| Susceptible population | People younger than 30 | People aged 30–79 years old |
| Main route of transmission | Droplets or fomites | Droplets or fomites, contact |
| Common clinical symptoms | Fever, cough, sore throat and myalgia | Fever, cough, short of breath |
| Seasonality | Yes | Unknown |
| Diagnosis | RT-PCR | RT-PCR |
| Human-to-human transmission | Yes | Yes |
| Vaccine | Lack | Lack |
| Timeline | Three Crucial Stages | H1N1 Swine Influenza (2009) | COVID-19 (2019) | ||
|---|---|---|---|---|---|
| Dates and Events | Accumulated Days | Dates and Events | Accumulated Days | ||
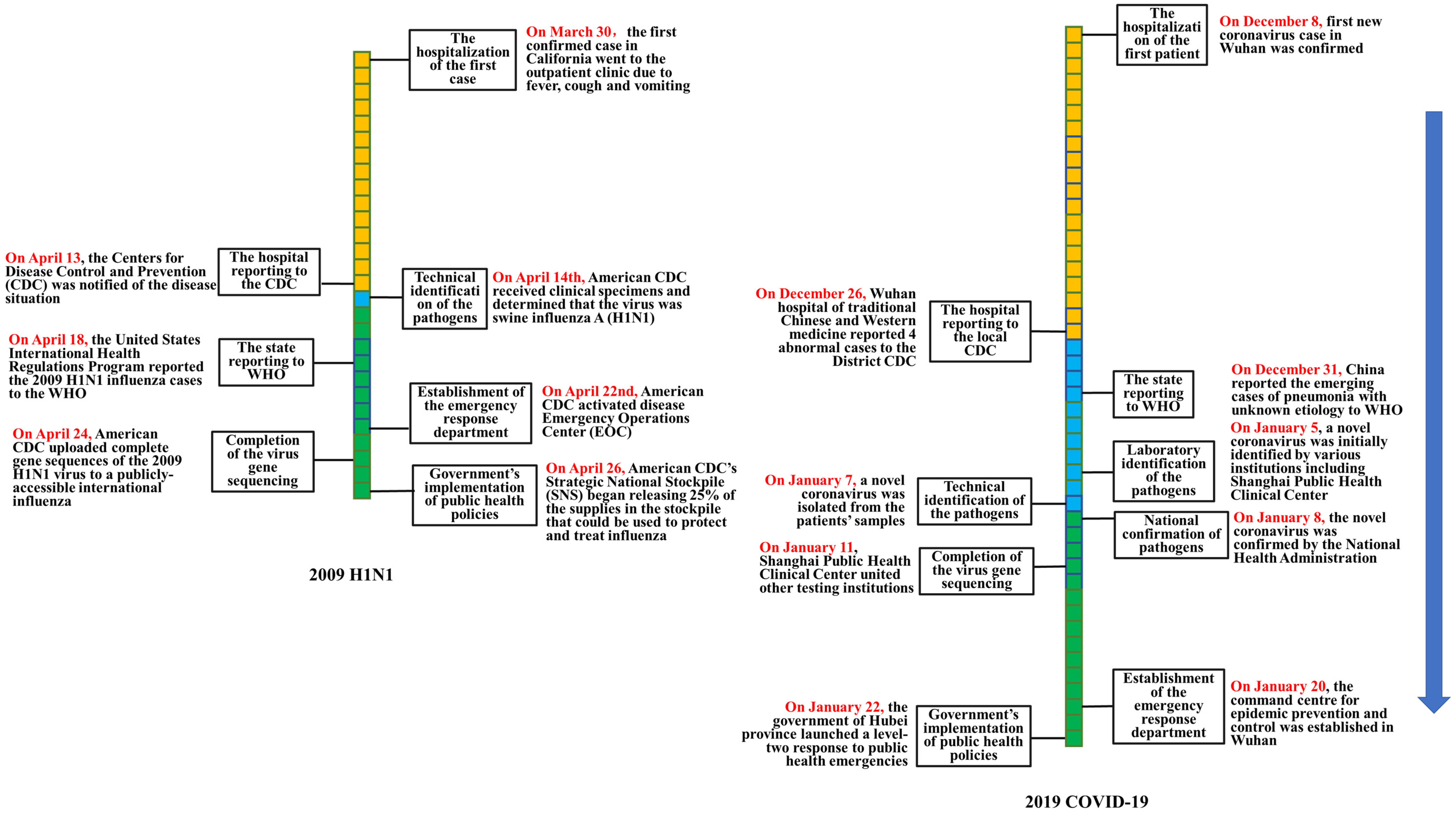
| The hospitalization of the first case | Hospital reporting stage | On 30 March, the first confirmed case in California went to the outpatient clinic due to fever, cough and vomiting. | 1 | On 8 December, the first novel coronavirus case in Wuhan was confirmed. | 1 |
| The hospital reporting to the CDC | After receiving the patients, the clinic reported the cases to the San Diego Health Bureau, but the specific time was not reported. On 13 April, American CDC was notified of the disease situation. | 15 | On 26 December, the Wuhan hospital of traditional Chinese and Western medicine reported four abnormal cases to the District CDC. | 19 | |
| Technical identification of the pathogens | Pathogen identification and virus gene sequencing stage | On 14 April, American CDC received clinical specimens and determined that the virus was swine influenza A (H1N1). | 16 | On 7 January, Chinese CDC isolated a new type of coronavirus from samples collected from patients. | 31 |
| Completion of the virus gene sequencing | On 24 April, American CDC uploaded the complete gene sequences of the 2009 H1N1 virus to a publicly accessible international influenza database. | 26 | On 11 January, Shanghai Public Health Clinical Center united other testing institutions to decipher the virus genome. | 35 | |
| Establishment of the emergency response department | Government policy-making stage | On 22 April, American CDC activated the disease Emergency Operations Center (EOC). | 24 | On 20 January 2020, the command center for epidemic prevention and control was established in Wuhan. | 44 |
| Government’s implementation of public health policies | On 26 April, American CDC’s Strategic National Stockpile (SNS) began releasing 25% of the supplies in the stockpile that could be used to protect and treat influenza. | 28 | On 22 January, the government launched a level-two response to public health emergencies. | 46 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Q.; Zhang, T.; Zhu, H.; Wang, Y.; Liu, X.; Bai, G.; Dai, R.; Zhou, P.; Luo, L. Characteristics of and Public Health Emergency Responses to COVID-19 and H1N1 Outbreaks: A Case-Comparison Study. Int. J. Environ. Res. Public Health 2020, 17, 4409. https://doi.org/10.3390/ijerph17124409
Wang Q, Zhang T, Zhu H, Wang Y, Liu X, Bai G, Dai R, Zhou P, Luo L. Characteristics of and Public Health Emergency Responses to COVID-19 and H1N1 Outbreaks: A Case-Comparison Study. International Journal of Environmental Research and Public Health. 2020; 17(12):4409. https://doi.org/10.3390/ijerph17124409
Chicago/Turabian StyleWang, Qian, Tiantian Zhang, Huanhuan Zhu, Ying Wang, Xin Liu, Ge Bai, Ruiming Dai, Ping Zhou, and Li Luo. 2020. "Characteristics of and Public Health Emergency Responses to COVID-19 and H1N1 Outbreaks: A Case-Comparison Study" International Journal of Environmental Research and Public Health 17, no. 12: 4409. https://doi.org/10.3390/ijerph17124409
APA StyleWang, Q., Zhang, T., Zhu, H., Wang, Y., Liu, X., Bai, G., Dai, R., Zhou, P., & Luo, L. (2020). Characteristics of and Public Health Emergency Responses to COVID-19 and H1N1 Outbreaks: A Case-Comparison Study. International Journal of Environmental Research and Public Health, 17(12), 4409. https://doi.org/10.3390/ijerph17124409