Exposure to Nail and False Eyelash Glue: A Case Series Study

 ,
, 
Abstract
1. Introduction
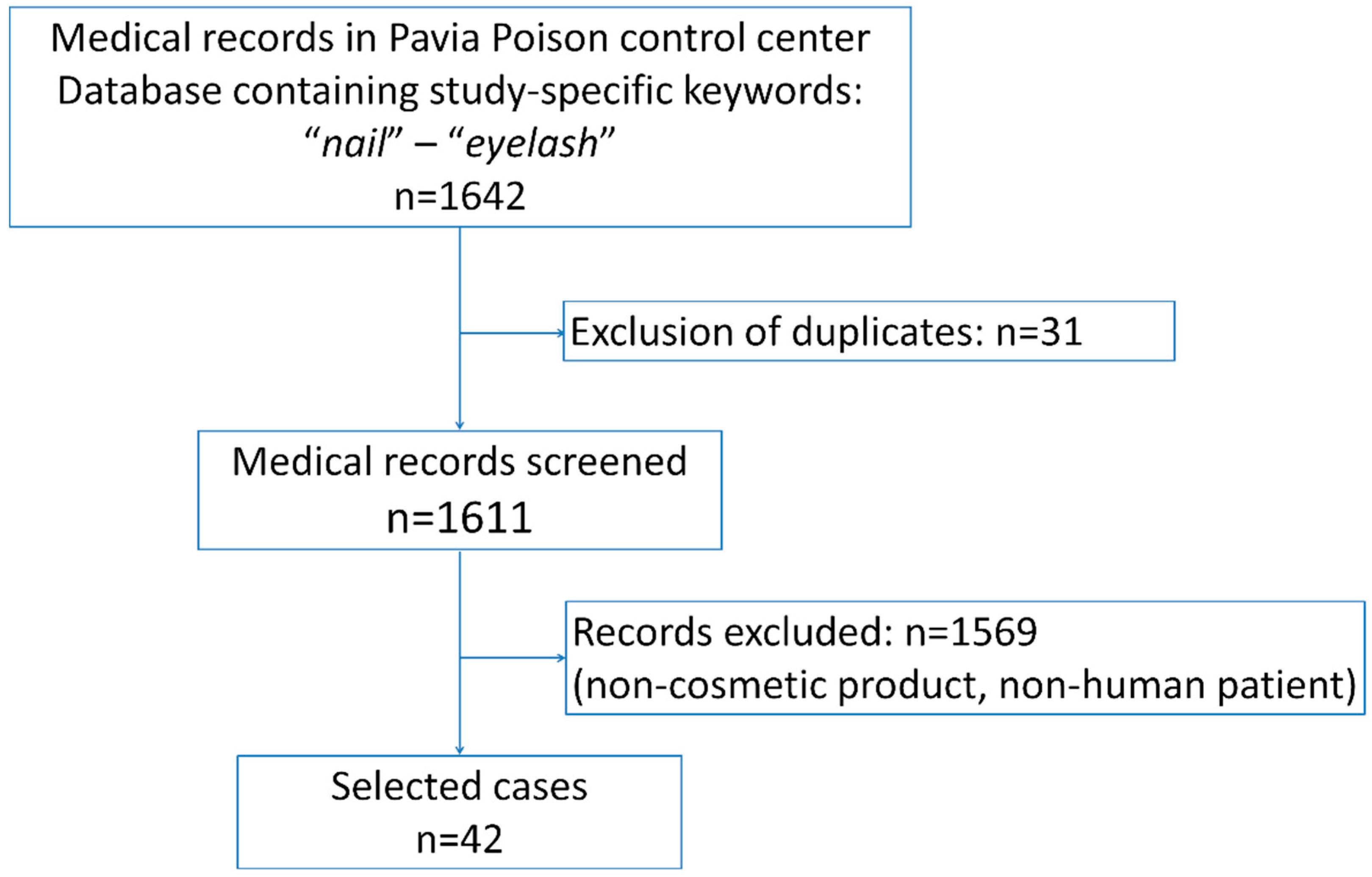
2. Materials and Methods
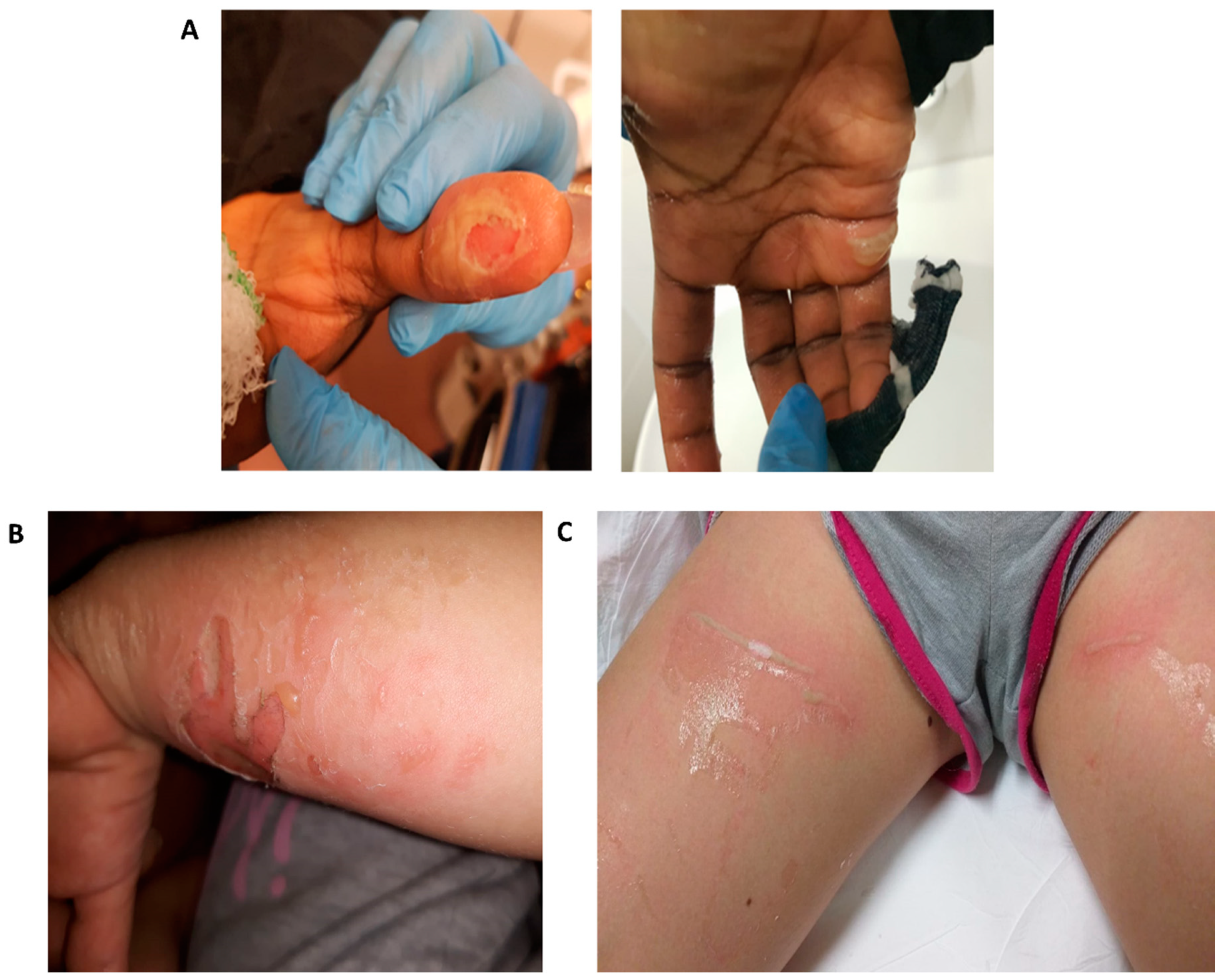
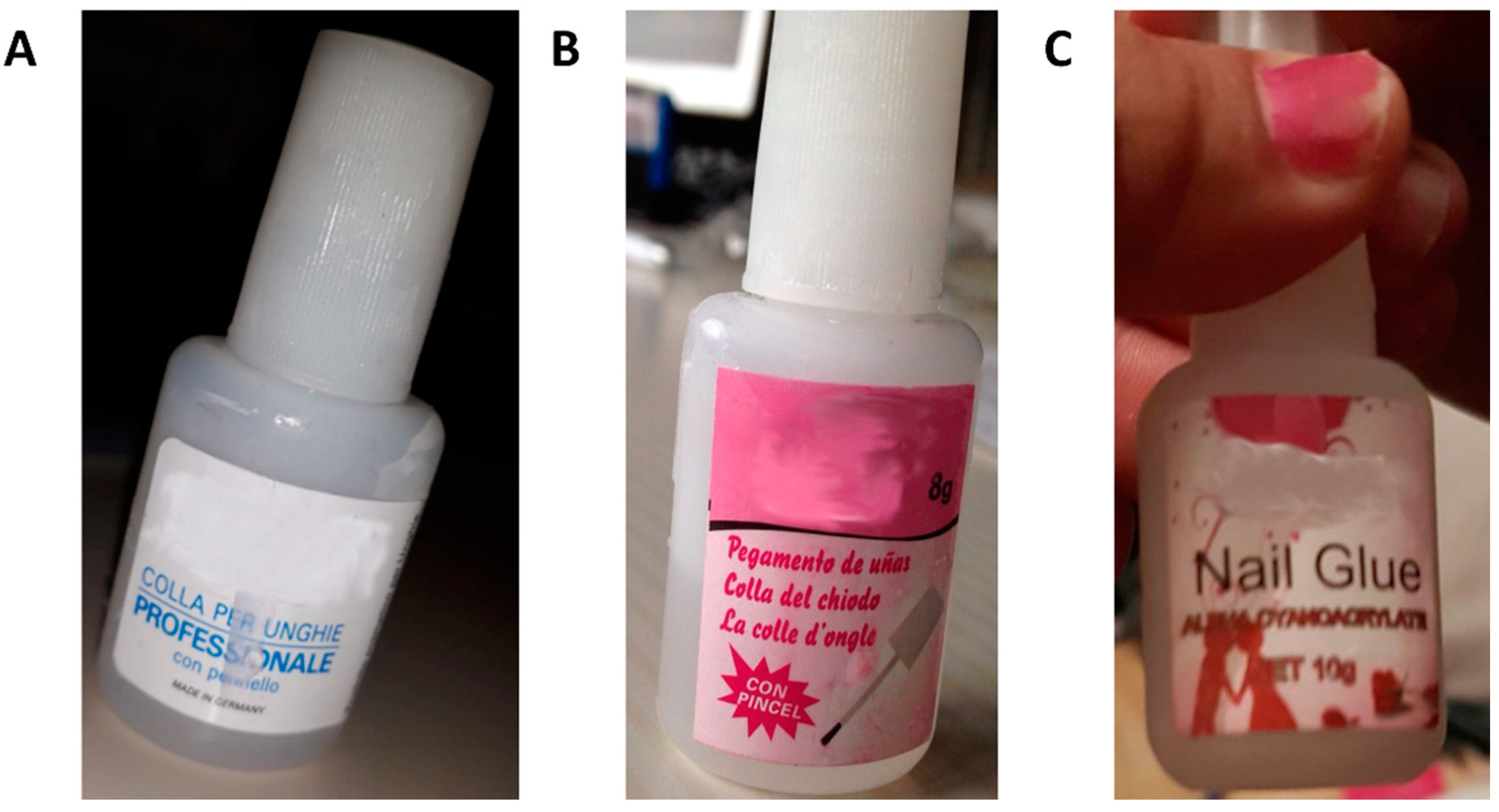
Case Series Presentation
3. Results
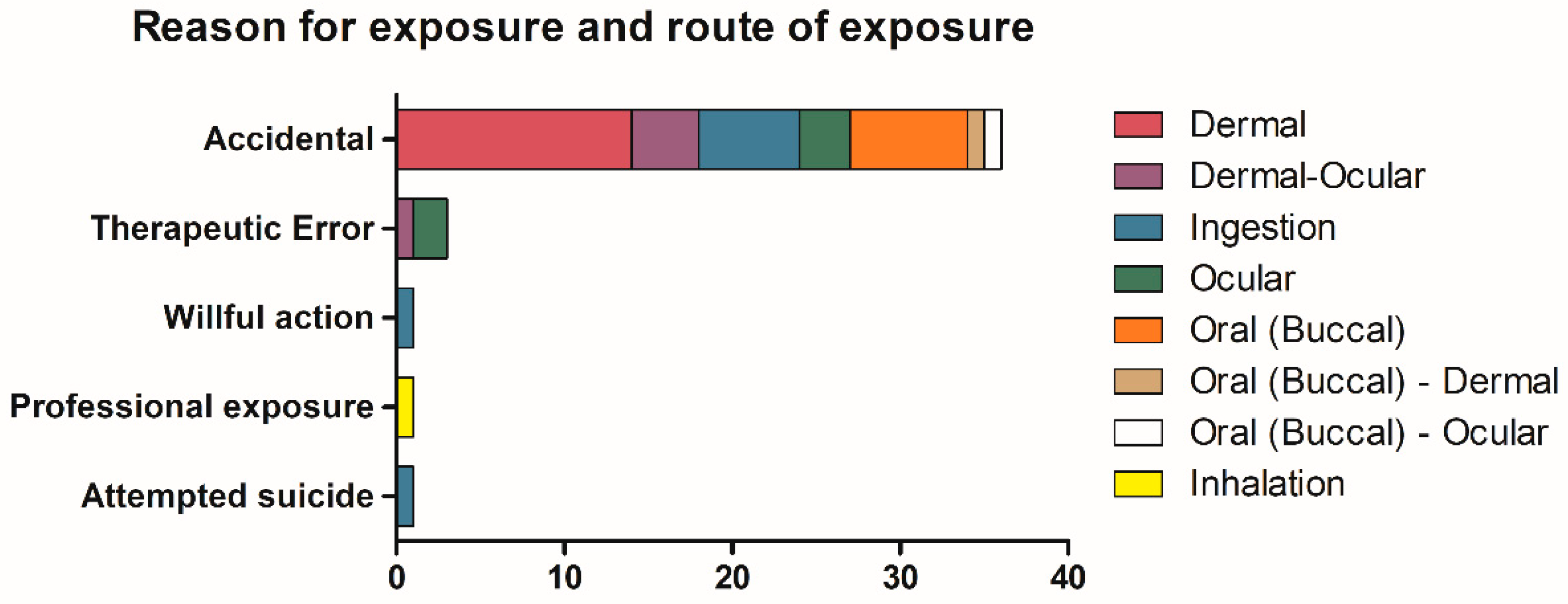
3.1. Patients Demographics, Route of Exposure, and Symptoms
3.2. Treatment Administered to Symptomatic Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kaličanin, B.; Velimirović, D. A Study of the Possible Harmful Effects of Cosmetic Beauty Products on Human Health. Biol. Trace Elem. Res. 2016, 170, 476–484. [Google Scholar] [PubMed]
- European Commission. Regulation (EC) No 1223/2009 of the European Parliament and Council of 30 November 2009 on cosmetic products. Off. J. Eur. Union 2009, 342, 59–209. [Google Scholar]
- Roda, E.; Butera, R.; Coccini, T.; Manzo, L. Safety assessment of cosmetic products containing nanomaterials. Current research trends and challenges. J. Appl. Cosmetol. 2011, 29, 27–39. [Google Scholar]
- Borowska, S.; Brzóska, M.M. Metals in cosmetics: Implications for human health. J. Appl. Toxicol. 2015, 35, 551–572. [Google Scholar] [CrossRef] [PubMed]
- Tang, C.L.; Larkin, G.; Kumiponjera, D.; Rao, G.S. Vanity burns: An unusual case of chemical burn caused by nail glue. Burns 2006, 32, 776–777. [Google Scholar] [CrossRef] [PubMed]
- Jamnadas-Khoda, B.; Khan, M.A.A.; Thomas, G.P.L.; Ghosh, S.J. Histoacryl glue: A burning issue. Burns 2011, 37, e1–e3. [Google Scholar] [CrossRef] [PubMed]
- Gennari, R.; Rotmensz, N.; Ballardini, B.; Scevola, S.; Perego, E.; Zanini, V.; Costa, A. A prospective, randomized, controlled clinical trial of tissue adhesive (2-octylcyanoacrylate) versus standard wound closure in breast surgery. Surgery 2004, 136, 593–599. [Google Scholar] [CrossRef] [PubMed]
- Yusuf, I.H.; Patel, C.K. A sticky sight: Cyanoacrylate ‘superglue’ injuries of the eye. BMJ Case Rep. 2010. [Google Scholar] [CrossRef] [PubMed]
- Eyth, C.P.; Echlin, K.; Jones, I. Cyanoacrylate Burn Injuries: Two Unusual Cases and a Review of the Literature. Wounds 2016, 28, E53–E59. [Google Scholar] [PubMed]
- Lazarov, A. Sensitization to acrylates is a common adverse reaction to artificial fingernails. J. Eur. Acad. Dermatol. Venereol. 2007, 21, 169–174. [Google Scholar] [CrossRef] [PubMed]
- Baran, R.; Goettmann, S.; André, J. Cosmetic nail products. Ann. Dermatol. Venereol. 2016, 143, 389–396. [Google Scholar] [CrossRef] [PubMed]
- Gagnier, J.J.; Kienle, G.; Altman, D.G.; Moher, D.; Sox, H.; Riley, D.; CARE Group. The CARE Guidelines: Consensus-based Clinical Case Reporting Guideline Development. Glob. Adv. Health Med. 2013, 2, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Clarke, T.F.E. Cyanoacrylate glue burn in a child–lessons to be learned. J. Plast. Reconstr. Aesthetic Surg. 2011, 64, e170–e173. [Google Scholar] [CrossRef] [PubMed]
- Kelemen, N.; Karagergou, E.; Jones, S.L.; Morritt, A.N. Full thickness burns caused by cyanoacrylate nail glue: A case series. Burns 2016, 42, e51–e54. [Google Scholar] [CrossRef] [PubMed]
- Coles, C.; Javed, M.U.; Hemington Gorse, S.; Nguyen, D. Paediatric burns secondary to nail adhesives: A case series. Burns Trauma 2016, 4, 17. [Google Scholar] [CrossRef] [PubMed]
- Spencer, T.J.; Clark, B. Self-inflicted Superglue Injuries. Med. J. Aust. 2004, 181, 341. [Google Scholar] [CrossRef] [PubMed]
- Needham, A.D.; Natha, S.; Kaye, S. Similarities in the packaging of cyanoacrylate nail glue and ophthalmic preparations: An ongoing problem. Br. J. Ophthalmol. 2001, 85, 496–497. [Google Scholar] [CrossRef] [PubMed][Green Version]
- DeRespinis, P.A. Cyanoacrylate Nail Glue Mistaken for Eye Drops. JAMA 1990, 263, 2301. [Google Scholar] [CrossRef] [PubMed]
- Morgan, S.J.; Astbury, N.J. Inadvertent self administration of superglue: A consumer hazard. Br. Med. J. Clin. Res. 1984, 289, 226–227. [Google Scholar] [CrossRef] [PubMed]
- Woolf, A.; Shaw, J. Childhood Injuries from Artificial Nail Primer Cosmetic Products. Arch. Pediatr. Adolesc. Med. 1998, 152, 41–46. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case Number | Age | Clinical Effects | Route of Exposure | Way of Exposure 1 | Score | Product | Component 1 | Component 2 | Component 3 |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Adult | Damaged skin | Dermal | A | 1 | Nail glue | Poly methyl methacrylate | ||
| 2 | Adult | Finger’s oedema | Dermal | A | 1 | Nail glue | - | ||
| 3 | Infant | Second-degree burns on hand and thigh | Dermal | A | 1 | Nail glue | Cyanoacrylate | ||
| 4 | Adult | First-degree burns on thigh | Dermal | A | 1 | Nail glue | Methacrylic acid | Butyl acetate | Butyl methacrylate |
| 5 | Adult | Cutaneous hyperaemia and erithema on hand | Dermal | A | 1 | Nail glue | Cyanoacrylate | ||
| 6 | Adolescent | Cutaneous hyperaemia and blister | Dermal | A | 1 | Nail glue | Cyanoacrylate | Poly | |
| 7 | Child | Damaged skin | Dermal | A | 1 | Nail glue | Ethyl cyanoacrylate | Poly | |
| 8 | Infant | First-degree burns and residues of glue | Dermal | A | 1 | Nail glue | - | ||
| 9 | Infant | Second-degree burns on thigh, perilesional oedema | Dermal | A | 2 | Nail glue | - | ||
| 10 | Adolescent | Second-degree burns on thigh | Dermal | A | 2 | Nail glue | - | ||
| 11 | Adult | First- and second-degree burns on hand | Dermal | A | 2 | Nail glue | - | ||
| 12 | Infant | Second-degree burns on forearm, palm and thigh | Dermal | A | 2 | Nail glue | Cyanoacrylate | Isopropyl alcohol | Ethanol |
| 13 | Infant | Second-degree burns on thigh and thorax | Dermal | A | 2 | Nail glue | - | ||
| 14 | Adolescent | First- and second-degree burns on both thighs | Dermal | A | 2 | Nail glue | - | ||
| 15 | Adolescent | Glued eyelids | Dermal-Ocular | A | 1 | Nail glue | Cyanoacrylate | ||
| 16 | Adult | Conjunctival hyperemia, cutaneous erythema | Dermal-Ocular | A | 1 | Nail glue | - | ||
| 17 | Adolescent | Glued eyelashes | Dermal-Ocular | A | 1 | Nail glue | Ethyl cyanoacrylate | ||
| 18 | Adult | Glued eyelids | Dermal-Ocular | Th. E | 1 | Nail glue | Cyanoacrylate | ||
| 19 | Infant | Eyelid and cheek oedema, glued eyelid | Dermal-Ocular | A | 2 | Nail glue | Cyanoacrylate | Methacrylate | |
| 20 | Infant | Asymptomatic | Ingestion | A | 0 | Nail glue | - | ||
| 21 | Infant | Asymptomatic | Ingestion | A | 0 | Nail glue | Cyanoacrylate | ||
| 22 | Adolescent | Asymptomatic | Ingestion | W | 0 | Nail glue | Cyanoacrylate | ||
| 23 | Adult | Asymptomatic | Ingestion | A | 0 | False eyelashes glue | Cellulose | Dodecyl benzene sulfonate | Ammonium hydroxide |
| 24 | Adolescent | Asymptomatic | Ingestion | A | 0 | Nail glue | - | ||
| 25 | Infant | Asymptomatic | Ingestion | A | 0 | Nail glue | Ethyl cyanoacrylate | ||
| 26 | Adult | Pharyngodynia, glottis oedema, hyperaemia | Ingestion | A | 1 | Nail glue | - | ||
| 27 | Adult | Epigastralgia | Ingestion | S | 1 | Nail glue | - | ||
| 28 | Adult | Cough and chronic irritation | Inhalation | Pr | 1 | Nail glue | Cyanoacrylate | ||
| 29 | Adult | Slight ocular discomfort | Ocular | A | 1 | Nail glue | Cyanoacrylate | ||
| 30 | Child | Oculodynia, conjunctival hyperemia | Ocular | A | 1 | Nail glue | Ethyl cyanoacrylate | ||
| 31 | Adolescent | Oculodynia | Ocular | Th. E | 1 | Nail glue | - | ||
| 32 | Child | Conjunctival hyperemia, oedema and burning eyelids | Ocular | A | 1 | Tip glue | Ethyl cyanoacrylate | Methyl methacrylate | BHA |
| 33 | Infant | Glued eyelid and eyelashes | Ocular | Th. E | 2 | Nail glue | - | ||
| 34 | Infant | Asymptomatic | Oral (Buccal) | A | 0 | Nail glue | - | ||
| 35 | Infant | Asymptomatic | Oral (Buccal) | A | 0 | Nail glue | - | ||
| 36 | Infant | Asymptomatic | Oral (Buccal) | A | 0 | Nail glue | - | ||
| 37 | Infant | Asymptomatic | Oral (Buccal) | A | 0 | Nail glue | - | ||
| 38 | Infant | Glue attached to palate and teeth | Oral (Buccal) | A | 1 | Nail glue | Ethyl cyanoacrylate | Poly methyl methacrylate | BHA |
| 39 | Adult | Pharyngodynia | Oral (Buccal) | A | 1 | Nail glue | - | ||
| 40 | Infant | Solid and dry residues of glue on mouth | Oral (Buccal) | A | 1 | Nail glue | - | ||
| 41 | Adult | Cutaneous burns, dysphonia, pharyngodynia | Oral (Buccal)-Dermal | A | 2 | Nail glue | Ethyl cyanoacrylate | ||
| 42 | Infant | Glued tongue and eyelids | Oral (Buccal)-Ocular | A | 1 | Nail glue | Cyanoacrylate |
| Glue Composition | PubChem® CID 1 | Score 0 | Score 1 | Score 2 | Total |
|---|---|---|---|---|---|
| Cyanoacrylate | 81530 | 2 | 7 | 0 | 9 |
| 90% Cyanoacrylate, 10% Poly | 81530–6658 | 0 | 1 | 0 | 1 |
| Cyanoacrylate, Methacrylate | 81530–6658 | 0 | 1 | 0 | 1 |
| Cyanoacrylate, Isopropyl alcohol, Ethanol | 81530–3776–702 | 0 | 0 | 1 | 1 |
| Ethyl cyanoacrylate | 81530 | 1 | 2 | 1 | 4 |
| Ethyl cyanoacrylate, Poly | 81530–6658 | 0 | 1 | 0 | 1 |
| Ethyl cyanoacrylate, Methyl methacrylate, BHA | 81530–6658–24667 | 0 | 1 | 0 | 1 |
| Ethyl cyanoacrylate, Poly methyl methacrylate, BHA | 81530–6658–24667 | 0 | 1 | 0 | 1 |
| Poly methyl methacrylate | 6658 | 0 | 1 | 0 | 1 |
| Methacrylic acid, Butyl acetate, Butyl methacrylate | 4093–31272–7354 | 0 | 1 | 0 | 1 |
| Cellulose, Dodecyl benzene sulfonate, Ammonium hydroxide | 14055602–15900–12896473 | 1 | 0 | 0 | 1 |
| Unknown composition | - | 6 | 7 | 7 | 20 |
| Total | 42 | ||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brambilla, E.; Crevani, M.; Petrolini, V.M.; Scaravaggi, G.; Di Primo, M.; Roda, E.; Locatelli, C.A. Exposure to Nail and False Eyelash Glue: A Case Series Study. Int. J. Environ. Res. Public Health 2020, 17, 4283. https://doi.org/10.3390/ijerph17124283
Brambilla E, Crevani M, Petrolini VM, Scaravaggi G, Di Primo M, Roda E, Locatelli CA. Exposure to Nail and False Eyelash Glue: A Case Series Study. International Journal of Environmental Research and Public Health. 2020; 17(12):4283. https://doi.org/10.3390/ijerph17124283
Chicago/Turabian StyleBrambilla, Elena, Marta Crevani, Valeria M. Petrolini, Giulia Scaravaggi, Maria Di Primo, Elisa Roda, and Carlo A. Locatelli. 2020. "Exposure to Nail and False Eyelash Glue: A Case Series Study" International Journal of Environmental Research and Public Health 17, no. 12: 4283. https://doi.org/10.3390/ijerph17124283
APA StyleBrambilla, E., Crevani, M., Petrolini, V. M., Scaravaggi, G., Di Primo, M., Roda, E., & Locatelli, C. A. (2020). Exposure to Nail and False Eyelash Glue: A Case Series Study. International Journal of Environmental Research and Public Health, 17(12), 4283. https://doi.org/10.3390/ijerph17124283