Hyperhomocysteinemia is Associated with Inflammation, Bone Resorption, Vitamin B12 and Folate Deficiency and MTHFR C677T Polymorphism in Postmenopausal Women with Decreased Bone Mineral Density



Abstract
1. Introduction
2. Materials and Methods
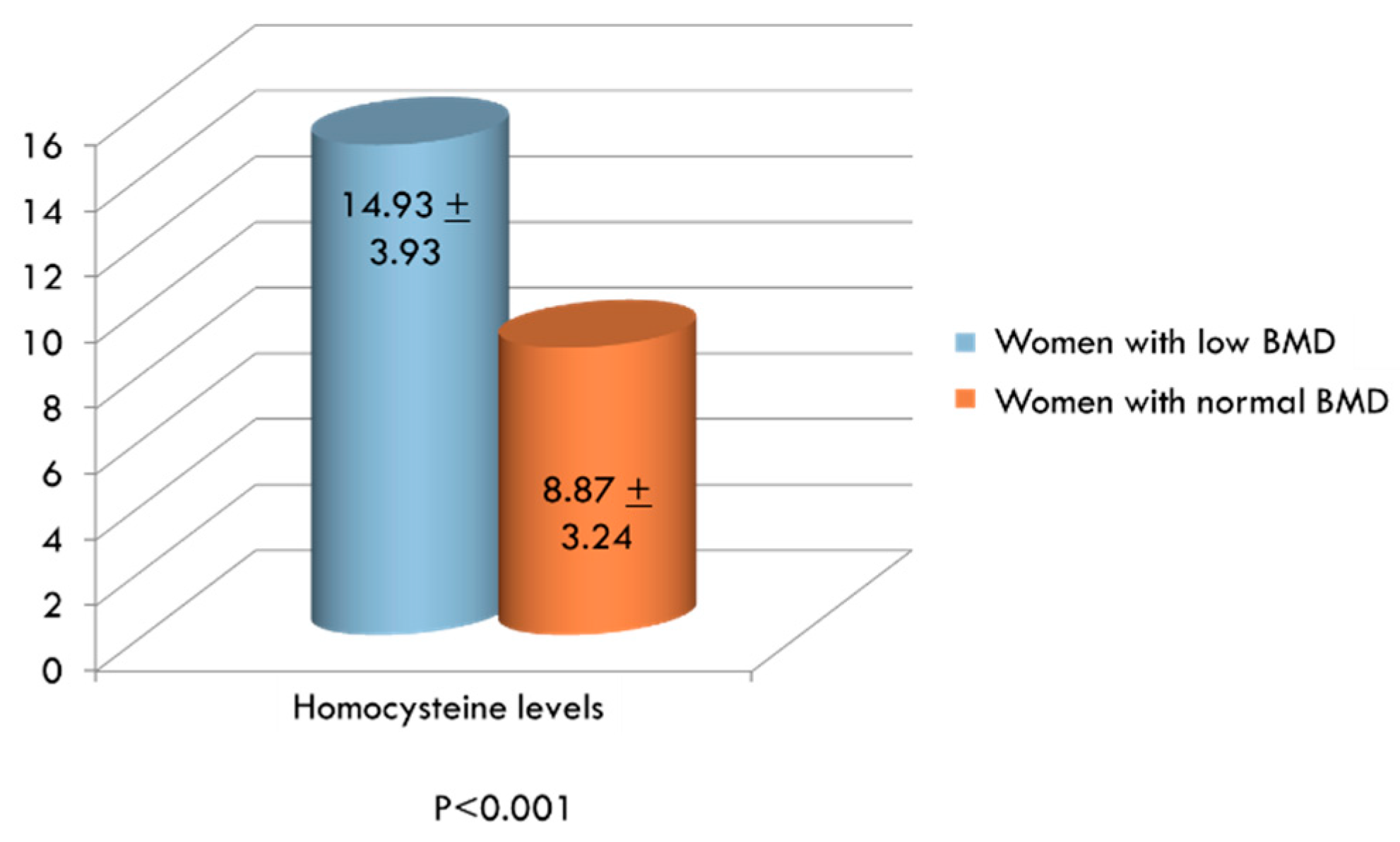
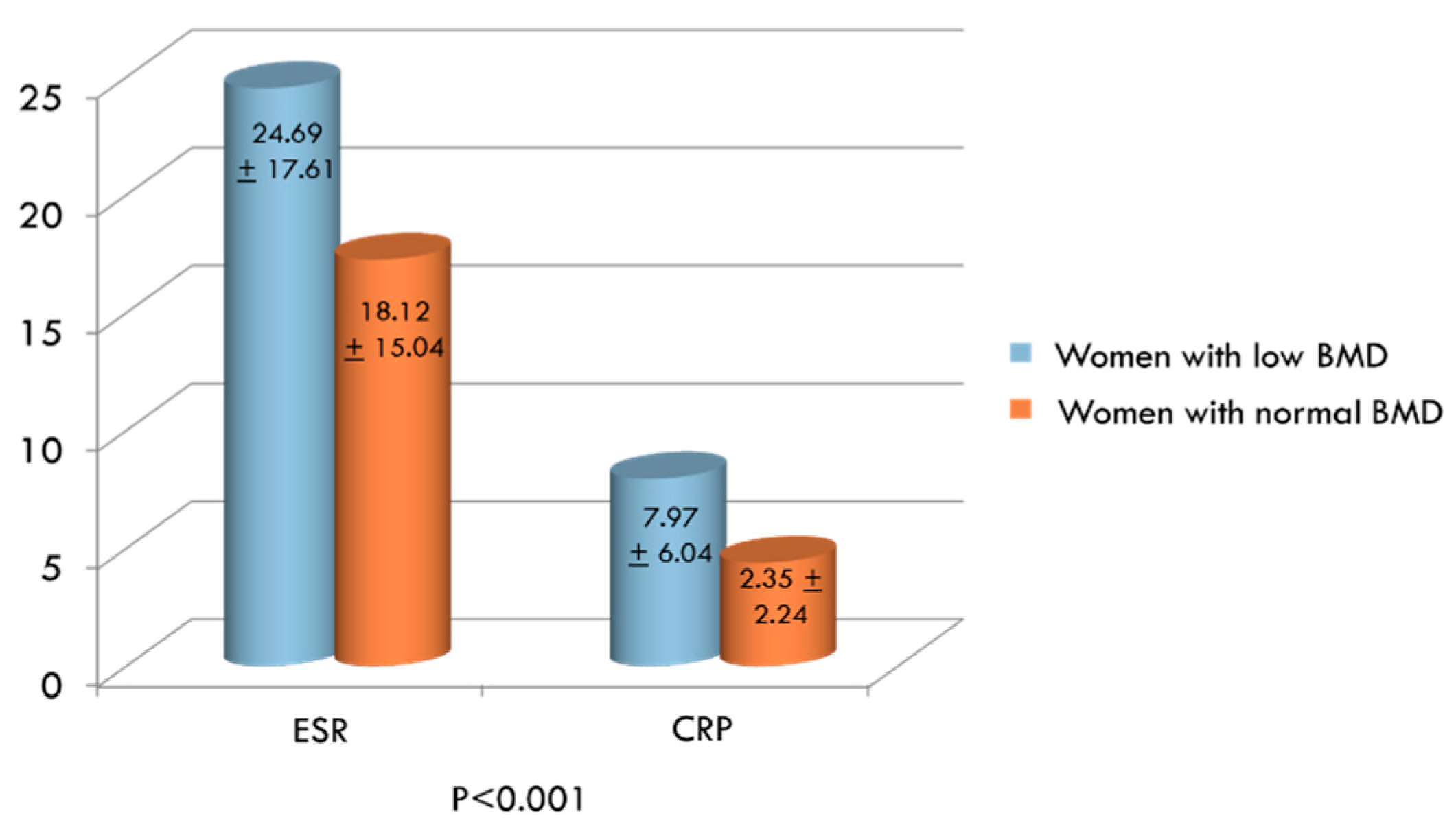
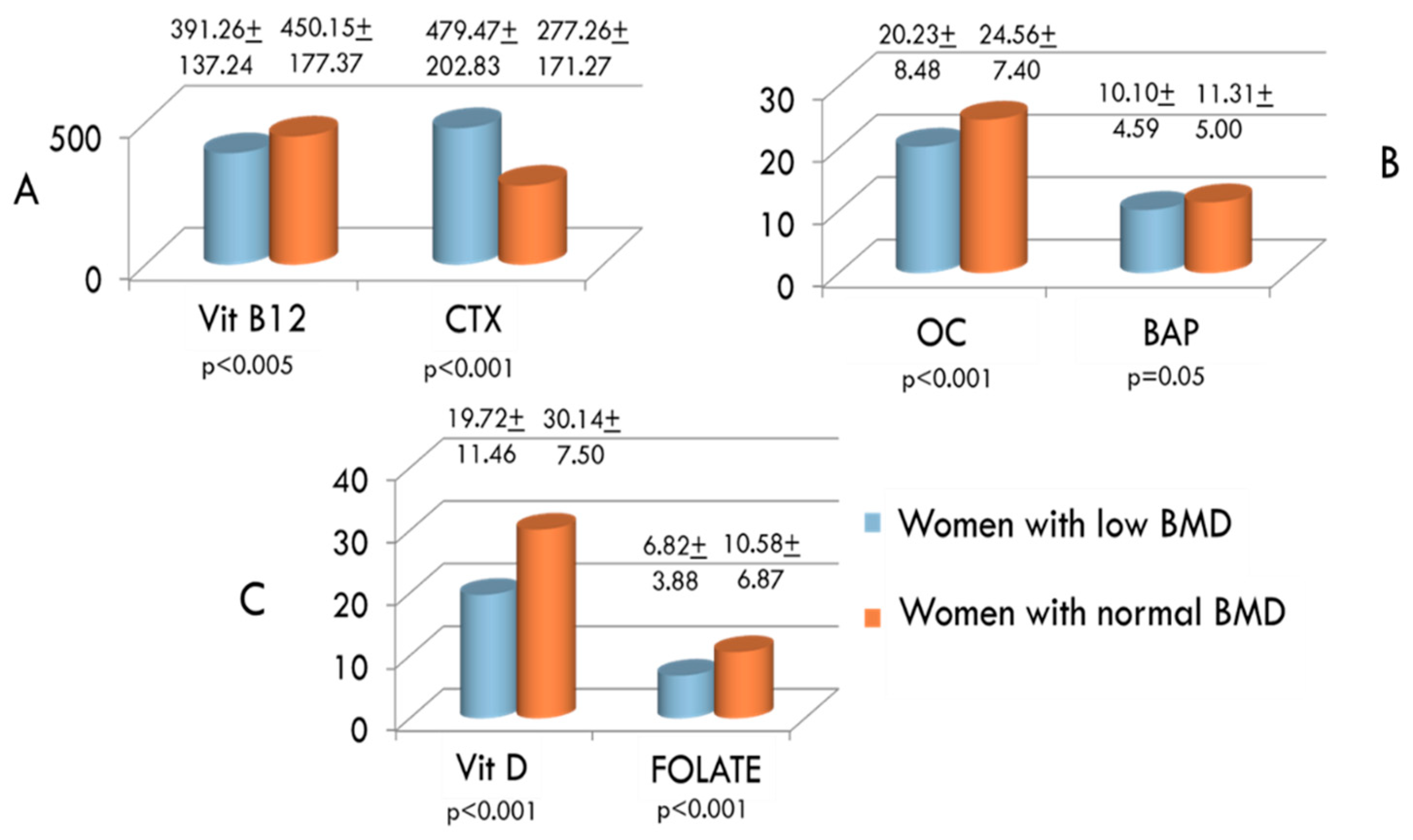
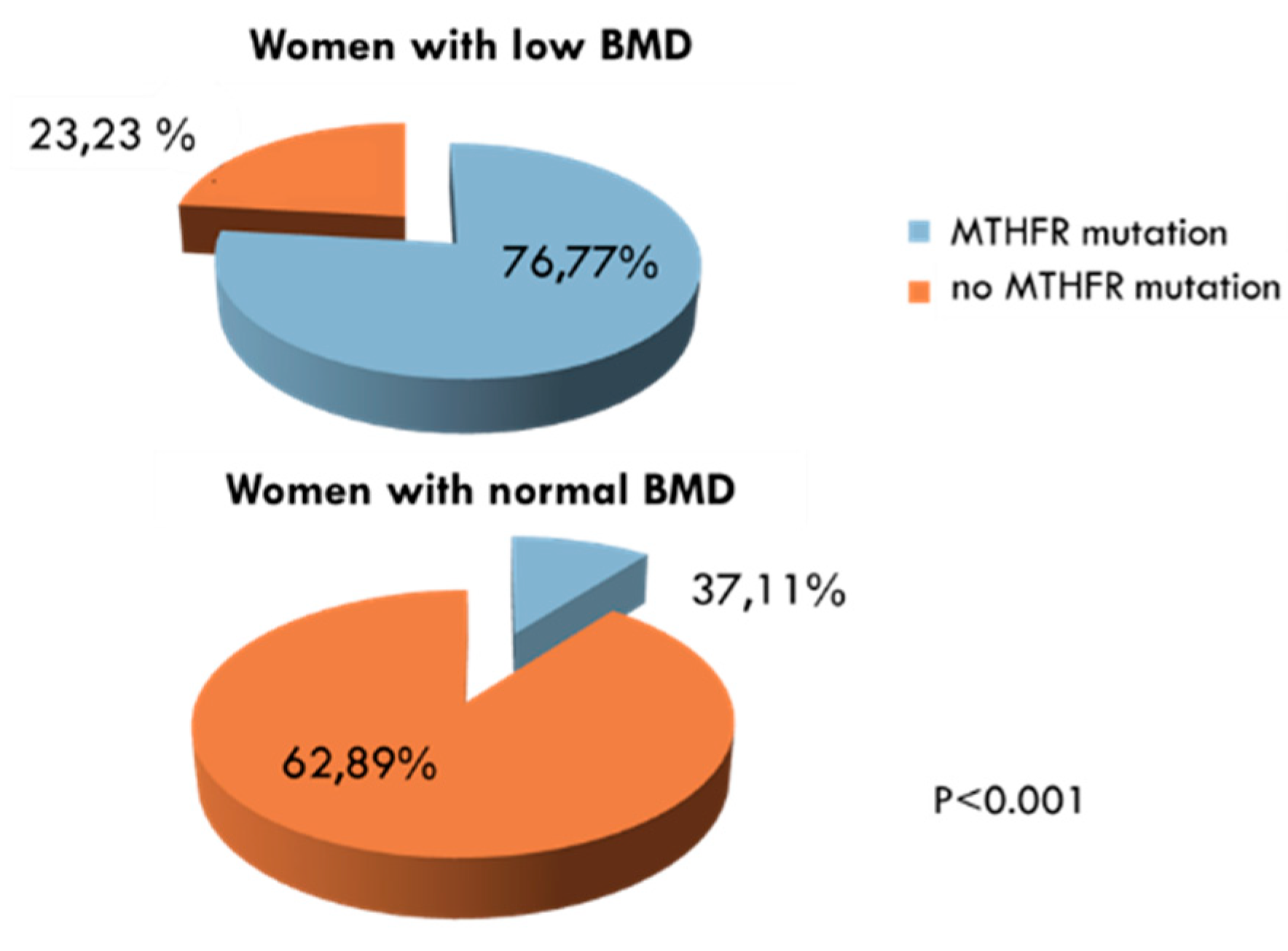
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Akkawi, I.; Zmerly, H. Osteoporosis: Current concepts. Joints 2018, 6, 122–127. [Google Scholar] [CrossRef] [PubMed]
- De Martinis, M.; Sirufo, M.M.; Ginaldi, L. Osteoporosis: Current and emerging therapies targeted to immunological checkpoints. Curr. Med. Chem. 2019. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.; Fortier, M.; Menopause and Osteoporosis Working Group; Fortier, M.; Reid, R.; Abramson, B.L.; Blake, J.; Desindes, S.; Dodin, S.; Graves, L.; et al. Osteoporosis in menopause. J. Obstet. Gynaecol. Can. 2014, 36, 839–843. [Google Scholar] [CrossRef]
- Sirufo, M.M.; Suppa, M.; Ginaldi, L.; De Martinis, M. Does allergy break bones? Osteoporosis and its connection to allergy. Int. J. Mol. Sci. 2020, 21, 712. [Google Scholar] [CrossRef]
- Irelli, A.; Sirufo, M.M.; .Scipioni, T.; De Pietro, F.; .Pancotti, A.; .Ginaldi, L.; De Martinis, M. mTOR links tumor immunity and bone metabolism: what are the clinical implications? Int. J. Mol. Sci. 2019, 20, 5841. [Google Scholar] [CrossRef]
- De Martinis, M.; Di Benedetto, M.; Mengoli, L.P.; Ginaldi, L. Senile osteoporosis: is it an immune-mediated disease? Inflamm. Res. 2006, 55, 399–404. [Google Scholar] [CrossRef]
- Massimini, M.; Palmieri, C.; De Maria, R.; Romanucci, M.; Malatesta, D.; De Martinis, M.; Maniscalco, L.; Ciccarelli, A.; Ginaldi, L.; Buracco, P.; et al. 17-AAG and apoptosis, autophagy, and mitophagy in canine osteosarcoma cell lines. Vet. Pathol. 2017, 54, 405–412. [Google Scholar] [CrossRef]
- Irelli, A.; Sirufo, M.M.; Scipioni, T.; De Pietro, F.; Pancotti, A.; Ginaldi, L.; De Martinis, M. Breast cancer patients receiving denosumab during adjuvant aromatase inhibitors treatment: who are the “inadequate responders” patients to denosumab? J. Buon 2020, 25, 648–654. [Google Scholar]
- Irelli, A.; Sirufo, M.M.; Scipioni, T.; De Pietro, F.; Pancotti, A.; Ginaldi, L.; De Martinis, M. Denosumab in breast cancer patients receiving aromatase inhibitors: a single-center observational study of effectiveness in adjuvant setting. Indian J. Cancer 2020, in press. [Google Scholar]
- Irelli, A.; Sirufo, M.M.; D’Ugo, C.; Ginaldi, L.; De Martinis, M. Real-life use of denosumab 120 mg every 12 weeks in prolonged treatment over 2 years of patients with breast cancer bone metastases. J. Buon 2020, 25. in press. [Google Scholar]
- Behera, J.; Bala, J.; Nuru, M.; Tyagi, Sc.; Tyagi, N. Homocysteine as a pathological biomarker for bone disease. J. Cell Physiol. 2017, 232, 2704–2709. [Google Scholar] [CrossRef] [PubMed]
- Brustolin, S.; Giugliani, R.; Félix, T.M. Genetics of homocysteine metabolism and associated disorders. Braz. J. Med. Biol. Res. 2010, 43, 1–7. [Google Scholar] [CrossRef]
- Ohishi, T.; Fujita, T.; Nishida, T.; Asukai, M.; Suzuki, D.; Sugiura, K. Factors influencing serum homocysteine levels in postmenopausal osteoporotic females—comparison to urinary collagen crosslinks. Endocr. Res. 2019, 44, 117–125. [Google Scholar] [CrossRef]
- Liew, S.C.; Gupta, E.D. Methylene tetrahydrofolate reductase (MTHFR) C677T polymorphism: epidemiology, metabolism and the associated diseases. Eur. J. Med. Genet. 2015, 58, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Van Wijngaarden, J.P.; Swart, K.M.; Enneman, A.W.; Dhonukshe-Rutten, R.A.; van Dijk, S.C.; Ham, A.C.; Brouwer-Brolsma, E.M.; van der Zwaluw, N.L.; Sohl, E.; van Meurs, J.B.; et al. Effect of daily vitamin B-12 and folic acid supplementation on fracture incidence in elderly individuals with an elevated plasma homocysteine concentration: B-PROOF, a randomized controlled trial. Am. J. Clin. Nutr. 2014, 100, 1578–1586. [Google Scholar] [CrossRef] [PubMed]
- Tariq, S.; Lone, K.P. Interplay of Vitamin D, Vitamin B 12, homocysteine and bone mineral density in postmenopausal females. Health Care Women Int. 2018, 39, 1340–1349. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.I.; Moon, J.H.; Hye Won Chung, H.W.; Kong, M.H.; Kim, H.J. Association between homocysteine and bone mineral density according to age and sex in healthy adults. J. Bone Metab. 2016, 23, 129–134. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Zaric, B.L.; Obradovic, M.; Bajic, V.; Haidara, M.A.; Jovanovic, M.; Isenovic, E.R. Homocysteine and Hyperhomocysteinaemia. Curr. Med. Chem. 2019, 26. [Google Scholar] [CrossRef]
- Ginaldi, L.; De Martinis, M. Osteoimmunology and beyond. Curr. Med. Chem. 2016, 23, 3754–3774. [Google Scholar] [CrossRef]
- Weber, D.R.; Coughlin, C.; Brodsky, J.L.; Lindstrom, K.; Ficicioglu, C.; Kaplan, P.; Freehauf, C.L.; Levine, M.A. Low bone mineral density is a common finding in patients with homocystinuria. Mol. Genet. Metab. 2016, 117, 351–354. [Google Scholar] [CrossRef][Green Version]
- Bucciarelli, P.; Martini, G.; Martinelli, I.; Ceccarelli, E.; Gennari, L.; Bader, R.; Valenti, R.; Franci, B.; Nuti, R.; Mannucci, P.M. The relationship between plasma homocysteine levels and bone mineral density in post-menopausal women. Eur. J. Intern. Med. 2010, 21, 1–305. [Google Scholar] [CrossRef] [PubMed]
- Bailey, R.L.; van Wijngaarden, J.P. The role of B-vitamins in bone health and disease in older adults. Curr. Osteoporos. Rep. 2015, 13, 256–261. [Google Scholar] [CrossRef]
- Rumbak, I.; Zižić, V.; Sokolić, L.; Cvijetić, S.; Kajfež, R.; Barić, I.C. Bone mineral density is not associated with homocysteine level, folate and vitamin B12 status. Arch. Gynecol. Obstet. 2012, 285, 991–1000. [Google Scholar] [CrossRef]
- Ahn, T.K.; Kim, J.O.; An, H.J.; Park, H.S.; Choi, U.Y.; Sohn, S.; Kim, K.T.; Kim, N.K.; Han, I.B. 3’-UTR Polymorphisms of Vitamin B-Related Genes Are Associated with Osteoporosis and Osteoporotic Vertebral Compression Fractures (OVCFs) in Postmenopausal Women. Genes 2020, 11, 612. [Google Scholar] [CrossRef]
- Enneman, A.W.; Swart, K.M.A.; van Wijngaarden, J.P.; van Dijk, S.C.; Ham, A.C.; Brouwer-Brolsma, E.M.; van der Zwaluw, N.L.; Dhonukshe-Rutten, R.A.M.; van der Cammen, T.J.M.; de Groot, L.C.P.G.M.; et al. Effect of vitamin B12 and folic acid supplementation on bone mineral density and quantitative ultrasound parameters in older people with an elevated plasma homocysteine level: B-PROOF, a Randomized Controlled Trial. Calcif. Tissue Int. 2015, 96, 401–4090. [Google Scholar] [CrossRef]
- Álvarez-Sánchez, N.; Álvarez-Ríos, A.I.; Guerrero, J.M.; García-García, F.J.; Rodríguez-Mañas, L.; Cruz-Chamorro, I.; Lardone, P.J.; Carrillo-Vico, A. Homocysteine levels are associated with bone resorption in pre-frail and frail Spanish women: The Toledo Study for Healthy Aging. Exp. Gerontol. 2018, 108, 201–208. [Google Scholar] [CrossRef]
- Ginaldi, L.; De Martinis, M.; Ciccarelli, F.; Saitta, S.; Imbesi, S.; Mannucci, C.; Gangemi, S. Increased levels of interleukin 31 (IL-31) in osteoporosis. BMC Immunol. 2015, 16, 60. [Google Scholar] [CrossRef]
- Ginaldi, L.; De Martinis, M.; Saitta, S.; Sirufo, M.M.; Mannucci, C.; Casciaro, M.; Ciccarelli, F.; Gangemi, S. Interleukin-33 serum levels in postmenopausal women with osteoporosis. Sci. Rep. 2019, 9, 3786. [Google Scholar] [CrossRef]
- Ciccarelli, F.; De Martinis, M.; Ginaldi, L. Glucocorticoids in patients with rheumatic diseases: friends or enemies of bone? Curr. Med. Chem. 2015, 22, 596–603. [Google Scholar] [CrossRef] [PubMed]
- Sözen, T.; Özışık, L.; Başaran, N.Ç. An overview and management of osteoporosis. Eur. J. Rheumatol. 2017, 4, 46–56. [Google Scholar] [CrossRef] [PubMed]
- De Martinis, M.; Sirufo, M.M.; Polsinelli, M.; Placidi, G.; Di Silvestre, D.; Ginaldi, L. Gender differences in osteoporosis: A single-center observational study. WJMH 2020. submitted. [Google Scholar]
- Donnelly, J.G.; Pronovost, C. Evaluation of the Abbott IMx fluorescence polarization immunoassay and the bio-rad enzyme immunoassay for homocysteine: Comparison with high-performance liquid chromatography. Ann. Clin. Biochem. 2000, 37, 194–198. [Google Scholar] [CrossRef] [PubMed]
- Yadav, U.; Kumar, P.; Gupta, S.; Rai, V. Distribution of MTHFR C677T gene polymorphism in healthy North Indian population and an updated meta-analysis. Ind. J. Clin. Biochem. 2017, 32, 399–410. [Google Scholar] [CrossRef] [PubMed]
- Zappacosta, B.; Romano, L.; Persichilli, S.; Cutrone, L.A.; Graziano, M.; Vitrani, A.; Di Castelnuovo, A.; Giardina, B.; Musumeci, S.; Mastroiacovo, P. Genotype prevalence and allele frequencies of 5,10-methylenetetrahydrofolate reductase (MTHFR) C677T and A1298C polymorphisms in Italian newborns. Lab. Med. 2009, 40, 732–736. [Google Scholar] [CrossRef]
- Ye, Z.; Zhang, Q.; Li, Y.; Wang, C.; Zhang, J.; Ma, X.; Peng, H.; Lou, T. High prevalence of hyperhomocysteinemia and its association with target organ damage in Chinese patients with chronic kidney disease. Nutrients 2016, 8, 645. [Google Scholar] [CrossRef] [PubMed]
- Yang, B.; Fan, S.; Zhi, X.; Wang, Y.; Wang, W.; Zheng, Q.; Sun, G. Prevalence of hyperhomocysteinemia in China: A systematic review and meta-analysis. Nutrients 2015, 7, 74–90. [Google Scholar] [CrossRef]
- Zhang, H.; Tao, X.; Wu, J. Association of homocysteine, vitamin B12, and folate with bone mineral density in postmenopausal women: A meta-analysis. Arch. Gynecol. Obstet. 2014, 289, 1003–1009. [Google Scholar] [CrossRef]
- Pandey, S.K.; Singh, A.; Polipalli, S.K.; Gupta, S.; Kapoor, S. Association of methylene tetrahydrofolate reductase polymorphism with BMD and homocysteine in premenopausal north Indian women. J. Clin. Diagn. Res. 2013, 7, 2908–2911. [Google Scholar] [CrossRef]
- Vacek, T.P.; Kalani, A.; Voor, M.J.; Tyagi, S.C.; Tyagi, N. The role of Hcy in bone remodeling. Clin. Chem. Lab. Med. 2013, 51, 579–590. [Google Scholar] [CrossRef]
- Zhu, Y.; Shen, J.; Cheng, Q.; Fan, Y.; Lin, W. Plasma homocysteine level is a risk factor for osteoporotic fractures in elderly patients. Clin. Interv. Aging 2016, 11, 1117–1121. [Google Scholar] [CrossRef]
- Kuroda, T.; Tanaka, S.; Saito, M.; Shiraki, Y.; Shiraki, M. Plasma level of homocysteine associated with severe vertebral fracture in postmenopausal women. Calcif. Tissue Int. 2013, 93, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Bhupathiraju, S.N.; Alekel, D.L.; Stewart, J.W.; Hanson, L.N.; Shedd, K.M.; Reddy, M.B.; Hanson, K.B.; Van Loan, M.D.; Genschel, U.; Koehler, K.J. Relationship of circulating total homocysteine and C-reactive protein to trabecular bone in postmenopausal women. J. Clin. Densitom. 2007, 10, 395–403. [Google Scholar] [CrossRef]
- Tinelli, C.; Di Pino, A.; Ficulle, E.; Marcelli, S.; Feligioni, M. Hyperhomocysteinemia as a risk factor and potential nutraceutical target for certain pathologies. Front. Nutr. 2019, 6, 49. [Google Scholar] [CrossRef] [PubMed]
- Lazzerini, P.E.; Capecchi, P.L.; Selvi, E.; Lorenzini, S.; Bisogno, S.; Galeazzi, S.; LaghiPasini, F. Hyperhomocysteinemia, inflammation and autoimmunity. Autoimmun. Rev. 2007, 6, 503. [Google Scholar] [CrossRef] [PubMed]
- De Martinis, M.; Sirufo, M.M.; Suppa, M.; Ginaldi, L. IL-33/IL-31 Axis in osteoporosis. Int. J. Mol. Sci. 2020, 21, 1239. [Google Scholar] [CrossRef] [PubMed]
- Ginaldi, L.; Di Benedetto, M.C.; De Martinis, M. Osteoporosis, inflammation and ageing. Immun. Ageing 2005, 2, 14. [Google Scholar] [CrossRef] [PubMed]
- Kamen, D.L.; Tangpricha, V. Vitamin D and molecular actions on the immune system: modulation of innate and autoimmunity. J. Mol. Med. 2010, 88, 441–450. [Google Scholar] [CrossRef]
- Sirufo, M.M.; Ginaldi, L.; Irelli, A.; De Martinis, M. Effectiveness of restoring vitamin B12 levels in the resolution of a case of erythema nodosum. Dermatol. Sin. 2020, 38. in press. [Google Scholar]
- Clarke, M.; Ward, M.; Strain, J.J.; Hoey, L.; Dickey, W.; McNulty, H. B-vitamins and bone in health and disease: The current evidence. Proc. Nutr. Soc. 2014, 73, 330–339. [Google Scholar] [CrossRef]
- Gommans, J.; Yi, Q.; Eikelboom, J.W.; Hankey, G.J.; Chen, C.; Rodgers, H.; VITATOPS trial study group. The effect of homocysteine-lowering with B-vitamins on osteoporotic fractures in patients with cerebrovascular disease: substudy of VITATOPS, a randomised placebo-controlled trial. BMC Geriatr. 2013, 13, 88. [Google Scholar] [CrossRef]
- Fratoni, V.; Brandi, M.L. B vitamins, homocysteine and bone health. Nutrients 2015, 7, 2176–2192. [Google Scholar] [CrossRef]
- Saito, M.; Marumo, K. The Effects of Homocysteine on the Skeleton. Curr. Osteoporos. Rep. 2018, 16, 554–560. [Google Scholar] [CrossRef] [PubMed]
- Vijayan, V.; Khandelwal, M.; Manglani, K.; Singh, R.R.; Gupta, S.; Surolia, A. Homocysteine alters the osteoprotegerin/RANKL system in the osteoblast to promote bone loss: pivotal role of the redox regulator forkhead O1. Free Radic. Biol. Med. 2013, 61, 72–84. [Google Scholar] [CrossRef]
- De Martinis, M.; Ginaldi, L.; Sirufo, M.M.; Pioggia, G.; Calapai, G.; Gangemi, S.; Mannucci, C. Alarmins in Osteoporosis, RAGE, IL-1, and IL-33 Pathways: A Literature Review. Medicina 2020, 56, 138. [Google Scholar] [CrossRef] [PubMed]
- Thaler, R.; Zwerina, J.; Rumpler, M.; Spitzer, S.; Gamsjaeger, S.; Paschalis, E.P.; Klaushofer, K.; Varga, F. Homocysteine induces serum amyloid A3 in osteoblasts via unlocking RGD-motifs in collagen. FASEB J. 2013, 27, 446–463. [Google Scholar] [CrossRef] [PubMed]
- Tyagi, N.; Kandel, M.; Munjal, C.; Qipshidze, N.; Vacek, J.C.; Pushpakumar, S.B.; Metreveli, N.; Tyagi, S.C. Homocysteine mediated decrease in bone blood flow and remodeling: role of folic acid. J. Orthop. Res. 2011, 29, 1511–1516. [Google Scholar] [CrossRef]
- Blouin, S.; Thaler, H.W.; Korninger, C.; Schmid, R.; Hofstaetter, J.G.; Zoehrer, R.; Phipps, R.; Klaushofer, K.; Roschger, P.; Paschalis, E.P. Bone matrix quality and plasma homocysteine levels. Bone 2009, 44, 959–964. [Google Scholar] [CrossRef] [PubMed]
- Thaler, R.; Agsten, M.; Spitzer, S.; Paschalis, E.P.; Karlic, H.; Klaushofer, K.; Varga, F. Homocysteine suppresses the expression of the collagen cross-linker lysyl oxidase involving IL-6, Fli1, and epigenetic DNA methylation. J. Biol. Chem. 2011, 286, 5578–5588. [Google Scholar] [CrossRef]
- Sirufo, M.M.; De Pietro, F.; Bassino, E.M.; Ginaldi, L.; De Martinis, M. Osteoporosis in skin diseases. Int. J. Mol. Sci. 2020. submitted. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Laboratory findings | Women with Serum HcyConcentration > 12 μmol/L (n. 147) | Women with Serum HcyConcentration < 12 μmol/L (n. 105) | |
|---|---|---|---|
| Means ± Standard Deviations | p values | ||
| ESR | 23.54 mm/h ± 13.77 | 16.65 mm/h ± 9.78 | p < 0.001 |
| CRP | 7.46 mg/L ± 7.44 | 3.09 mg/L ± 2.98 | p < 0.001 |
| OC | 20.80ng/mL ± 8.01 | 25.13 ng/mL ± 7.54 | p < 0.001 |
| CTX | 451.64 pg/mL ± 237.05 | 317.77 pg/mL ± 190.67 | p < 0.001 |
| BAP | 11.20 µg/L ± 4.74 | 11.78 µg/L ± 5.56 | ns |
| VIT B 12 | 376.16 pg/mL ± 147.20 | 455.79 pg/mL ± 167.50 | p < 0.001 |
| FOLATE | 5.69 ng/mL ± 3.13 | 9.16 ng/mL ± 4.34 | p < 0.001 |
| VIT D | 22.03 ng/mL ± 9.56 | 27.84 ng/mL ± 10.95 | p < 0.001 |
| MTHFR C677T | 57.14% | 33% | p < 0.001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Martinis, M.; Sirufo, M.M.; Nocelli, C.; Fontanella, L.; Ginaldi, L. Hyperhomocysteinemia is Associated with Inflammation, Bone Resorption, Vitamin B12 and Folate Deficiency and MTHFR C677T Polymorphism in Postmenopausal Women with Decreased Bone Mineral Density. Int. J. Environ. Res. Public Health 2020, 17, 4260. https://doi.org/10.3390/ijerph17124260
De Martinis M, Sirufo MM, Nocelli C, Fontanella L, Ginaldi L. Hyperhomocysteinemia is Associated with Inflammation, Bone Resorption, Vitamin B12 and Folate Deficiency and MTHFR C677T Polymorphism in Postmenopausal Women with Decreased Bone Mineral Density. International Journal of Environmental Research and Public Health. 2020; 17(12):4260. https://doi.org/10.3390/ijerph17124260
Chicago/Turabian StyleDe Martinis, Massimo, Maria Maddalena Sirufo, Cristina Nocelli, Lara Fontanella, and Lia Ginaldi. 2020. "Hyperhomocysteinemia is Associated with Inflammation, Bone Resorption, Vitamin B12 and Folate Deficiency and MTHFR C677T Polymorphism in Postmenopausal Women with Decreased Bone Mineral Density" International Journal of Environmental Research and Public Health 17, no. 12: 4260. https://doi.org/10.3390/ijerph17124260
APA StyleDe Martinis, M., Sirufo, M. M., Nocelli, C., Fontanella, L., & Ginaldi, L. (2020). Hyperhomocysteinemia is Associated with Inflammation, Bone Resorption, Vitamin B12 and Folate Deficiency and MTHFR C677T Polymorphism in Postmenopausal Women with Decreased Bone Mineral Density. International Journal of Environmental Research and Public Health, 17(12), 4260. https://doi.org/10.3390/ijerph17124260