Geographic Inequalities in Breast Cancer in Italy: Trend Analysis of Mortality and Risk Factors

 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
Data Sources and Statistical Analyses
3. Results
3.1. Trend by Geographic Area and Age
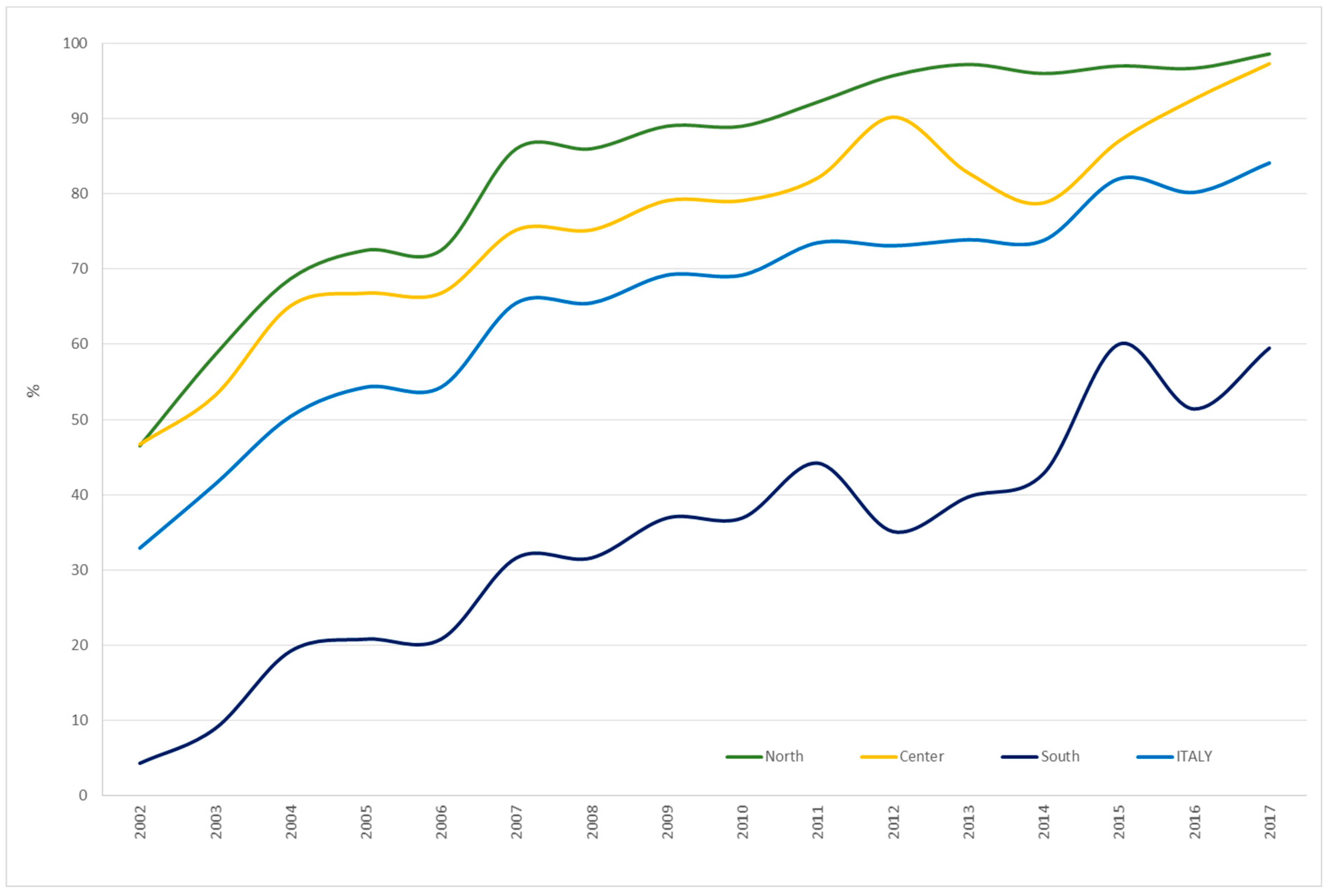
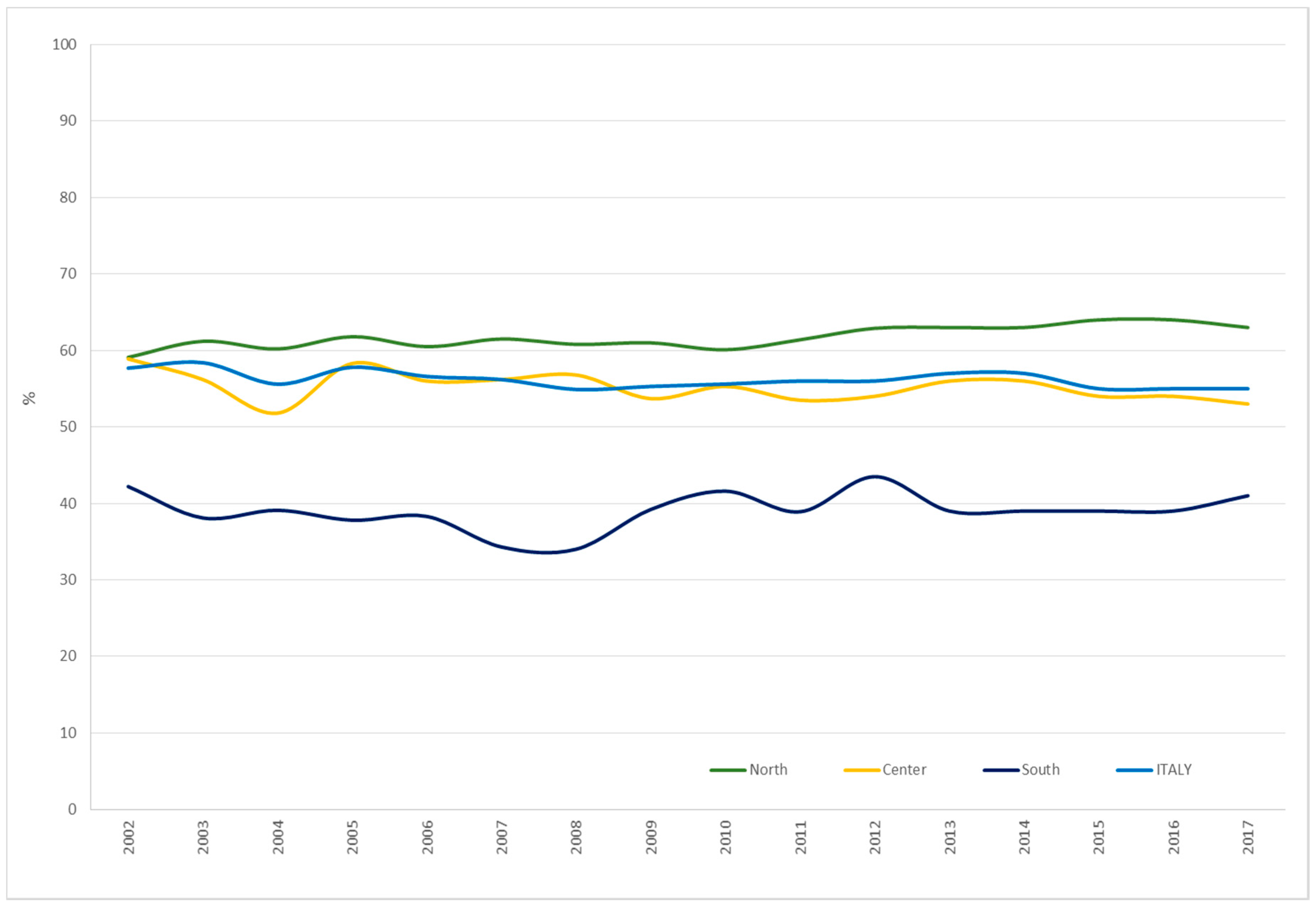
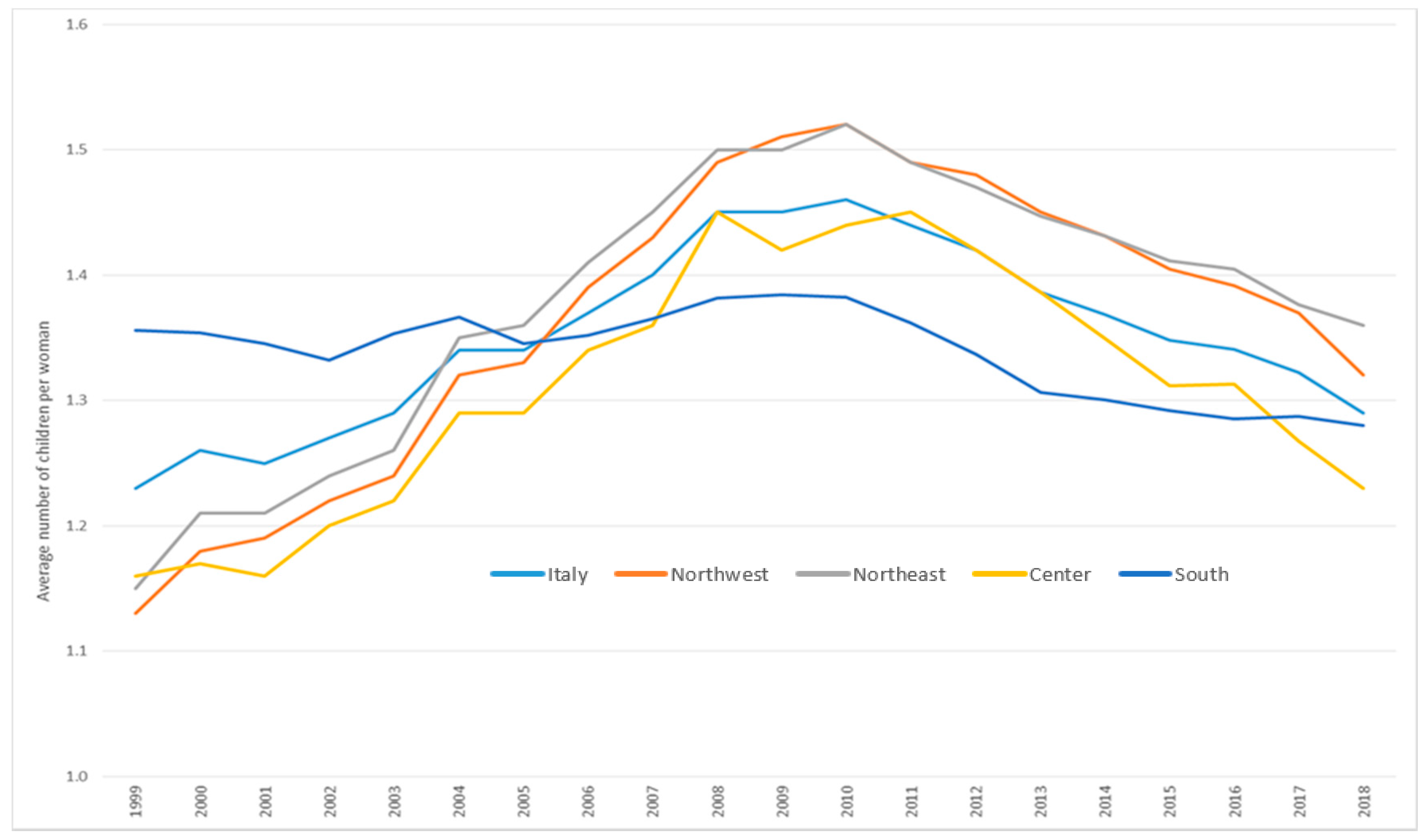
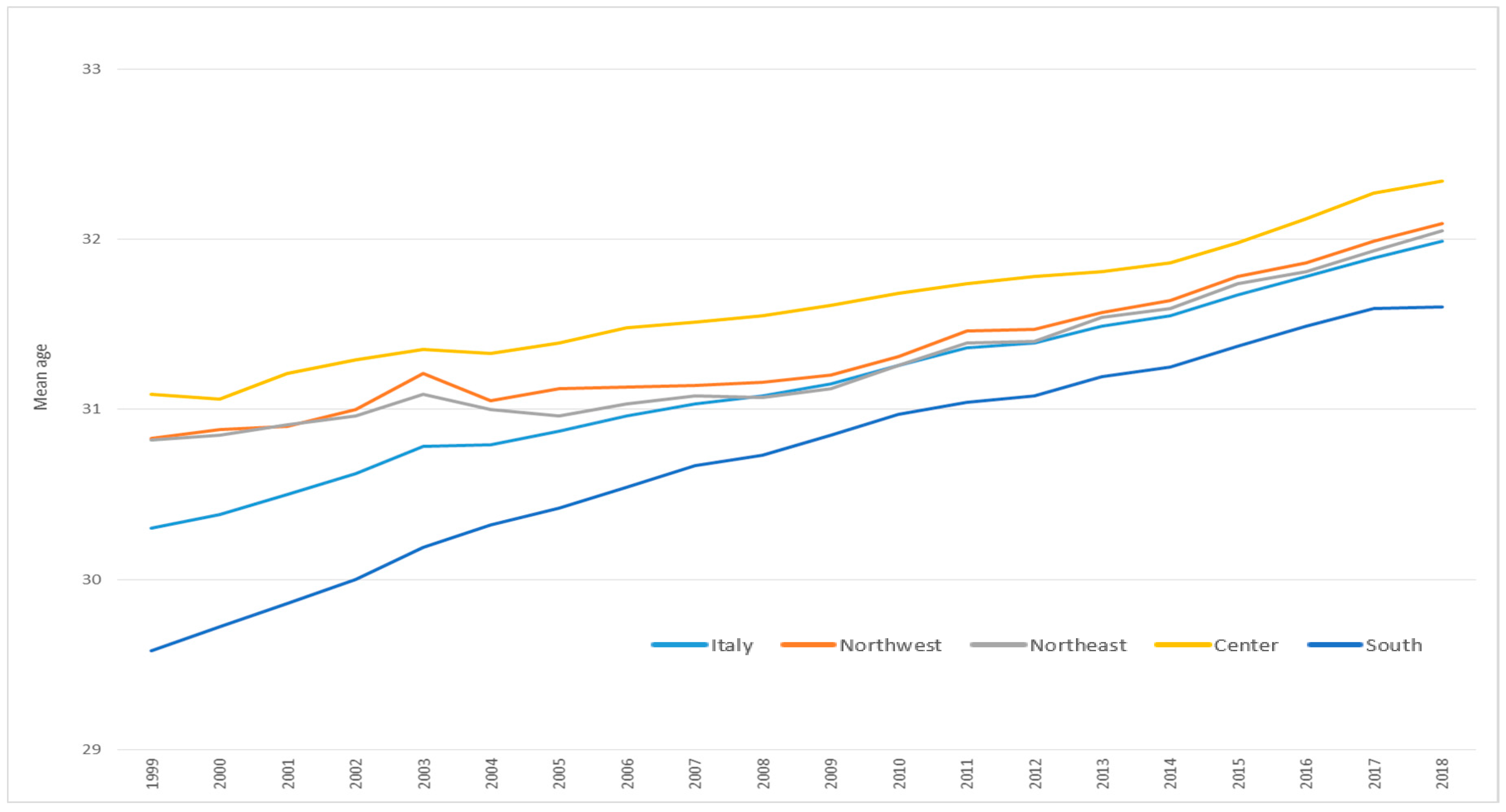
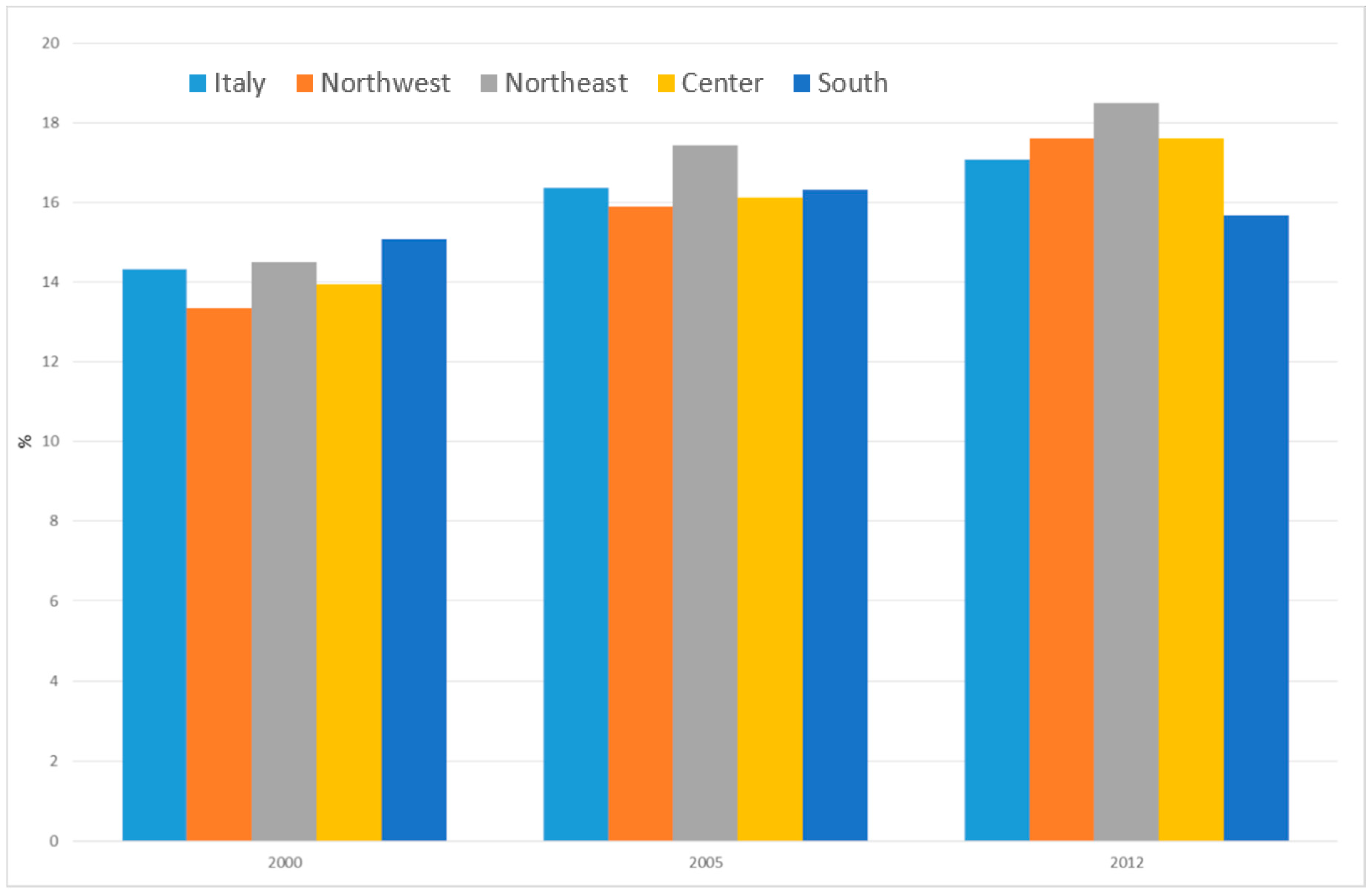
3.2. Risk Factors Trend by Geographic Area
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Mathers, C.; Parkin, D.M.; Piñeros, M.; Znaor, A.; Bray, F. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int. J. Cancer 2019, 144, 1941–1953. [Google Scholar] [CrossRef]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: Globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Morrison, A.S. Screening in Chronic Disease; Oxford University Press: New York, NY, USA, 1992; p. 254. [Google Scholar]
- Puliti, D.; Duffy, S.W.; Miccinesi, G.; de Koning, H.; Lynge, E.; Zappa, M.; Paci, E.; EUROSCREEN Working Group. Overdiagnosis in Mammographic Screening for Breast Cancer in Europe: A Literature Review. J. Med. Screen 2012, 19 (Suppl. 1), 42–56. [Google Scholar] [CrossRef]
- Biesheuvel, C.; Barratt, A.; Howard, K.; Houssami, N.; Irwig, L. Effects of study methods and biases on estimates of invasive breast cancer overdetection with mammography screening: A systematic review. Lancet Oncol. 2007, 8, 1129–1138. [Google Scholar] [CrossRef]
- Collaborative Group on Hormonal Factors in Breast Cancer. Type and timing of menopausal hormone therapy and breast cancer risk: Individual participant meta-analysis of the worldwide epidemiological evidence. Lancet 2019, 394, 1159–1168. [Google Scholar] [CrossRef]
- Esposito, K.; Chiodini, P.; Colao, A.; Lenzi, A.; Giugliano, D. Metabolic syndrome and risk of cancer: A systematic review and meta-analysis. Diabetes Care 2012, 35, 2402–2411. [Google Scholar] [CrossRef]
- Xia, X.; Chen, W.; Li, J.; Chen, X.; Rui, R.; Liu, C.; Sun, Y.; Liu, L.; Gong, J.; Yuan, P. Body Mass Index and Risk of Breast Cancer: A Nonlinear Dose-Response Meta-Analysis of Prospective Studies. Sci. Rep. 2014, 4, 1–5. [Google Scholar] [CrossRef]
- Ramteke, P.; Deb, A.; Shepal, V.; Bhat, M.K. Hyperglycemia Associated Metabolic and Molecular Alterations in Cancer Risk, Progression, Treatment, and Mortality. Cancers 2019, 11, 1402. [Google Scholar] [CrossRef]
- Scoccianti, C.; Key, T.J.; Anderson, A.S.; Armaroli, P.; Berrino, F.; Cecchini, M.; Boutron-Ruault, M.C.; Leitzmann, M.; Norat, T.; Powers, H.; et al. European Code against Cancer 4th Edition: Breastfeeding and cancer. Cancer Epidemiol. 2015, 39 (Suppl. 1), S101–S106. [Google Scholar] [CrossRef]
- Collaborative Group on Hormonal Factors in Breast Cancer. Breast cancer and breastfeeding: Collaborative reanalysis of individual data from 47 epidemiological studies in 30 countries, including 50302 women with breast cancer and 96973 women without the disease. Lancet 2002, 360, 187–195. [Google Scholar] [CrossRef]
- Zbuk, K.; Anand, S.S. Declining incidence of breast cancer after decreased use of hormone-replacement therapy: Magnitude and time lags in different countries. J. Epidemiol. Commun. Health 2012, 66, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Krieger, N.; Chen, J.T.; Waterman, P.D.; Soobader, M.J.; Subramanian, S.V.; Carson, R. Geocoding and monitoring of US socioeconomic inequalities in mortality and cancer incidence: Does the choice of area-based measure and geographic level matter?: The Public Health Disparities Geocoding Project. Am. J. Epidemiol. 2002, 156, 471–482. [Google Scholar] [CrossRef] [PubMed]
- Robert, S.A.; Strombom, I.; Trentham-Dietz, A.; Hampton, J.M.; McElroy, J.A.; Newcomb, P.A.; Remington, P.L. Socioeconomic risk factors for breast cancer: Distinguishing individual- and community-level effects. Epidemiology 2004, 15, 442–450. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.; Thomson, K.; Bambra, C.; Todd, A. The breast cancer paradox: A systematic review of the association between area-level deprivation and breast cancer screening uptake in Europe. Cancer Epidemiol. 2019, 60, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Palència, L.; Espelt, A.; Rodríguez-Sanz, M.; Puigpinós, R.; Pons-Vigués, M.; Pasarín, M.I.; Spadea, T.; Kunst, A.E.; Borrell, C. Socio-economic inequalities in breast and cervical cancer screening practices in Europe: Influence of the type of screening program. Int. J. Epidemiol. 2010, 39, 757–765. [Google Scholar] [CrossRef] [PubMed]
- Dialla, P.O.; Arveux, P.; Ouedraogo, S.; Pornet, C.; Bertaut, A.; Roignot, P.; Janoray, P.; Poillot, M.L.; Quipourt, V.; Dabakuyo-Yonli, T.S. Age-related socio-economic and geographic disparities in breast cancer stage at diagnosis: A population-based study. Eur. J. Public Health 2015, 25, 966–972. [Google Scholar] [CrossRef]
- Flores, Y.N.; Davidson, P.L.; Nakazono, T.T.; Carreon, D.C.; Mojica, C.M.; Bastani, R. Neighborhood socio-economic disadvantage and race/ethnicity as predictors of breast cancer stage at diagnosis. BMC Public Health 2013, 13, 1061. [Google Scholar] [CrossRef]
- Pacelli, B.; Carretta, E.; Spadea, T.; Caranci, N.; Di Felice, E.; Stivanello, E.; Cavuto, S.; Cisbani, L.; Candela, S.; De Palma, R.; et al. Does breast cancer screening level health inequalities out? A population-based study in an Italian region. Eur. J. Public Health 2014, 24, 280–285. [Google Scholar] [CrossRef][Green Version]
- Dreyer, M.S.; Nattinger, A.B.; McGinley, E.L.; Pezzin, L.E. Socioeconomic status and breast cancer treatment. Breast Cancer Res. Treat. 2018, 167, 1–8. [Google Scholar] [CrossRef]
- Richardson, L.C. Treatment of breast cancer in medically underserved women: A review. Breast J. 2004, 10, 2–5. [Google Scholar] [CrossRef]
- Petrelli, A.; Giorgi Rossi, P.; Francovich, L.; Giordani, B.; Di Napoli, A.; Zappa, M.; Mirisola, C.; Gargiulo, L. Geographical and socioeconomic differences in uptake of Pap test and mammography in Italy: Results from the National Health Interview Survey. BMJ Open 2018, 8, e021653. [Google Scholar] [CrossRef]
- Petrelli, A.; Di Napoli, A.; Sebastiani, G.; Rossi, A.; Giorgi Rossi, P.; Demuru, E.; Costa, G.; Zengarini, N.; Alicandro, G.; Marchetti, S.; et al. Italian Atlas of mortality inequalities by education level. Epidemiol. Prev. 2019, 43, 1–120. [Google Scholar]
- Martin, A.M.; Weber, B.L. Genetic and hormonal risk factors in breast cancer. J. Natl. Cancer Inst. 2000, 92, 1126–1135. [Google Scholar] [CrossRef]
- Michailidou, K.; Beesley, J.; Lindstrom, S.; Canisius, S.; Dennis, J.; Lush, M.J.; Maranian, M.J.; Bolla, M.K.; Wang, Q.; Shah, M.; et al. Genome-wide association analysis of more than 120,000 individuals identifies 15 new susceptibility loci for breast cancer. Nat. Genet. 2015, 47, 373–380. [Google Scholar] [CrossRef]
- Feinberg, A.P.; Koldobskiy, M.A.; Göndör, A. Epigenetic modulators, modifiers and mediators in cancer aetiology and progression. Nat. Rev. Genet. 2016, 17, 284–299. [Google Scholar] [CrossRef]
- Teschendorff, A.E.; Gao, Y.; Jones, A.; Ruebner, M.; Beckmann, M.W.; Wachter, D.L.; Fasching, P.A.; Widschwendter, M. DNA methylation outliers in normal breast tissue identify field defects that are enriched in cancer. Nat. Commun. 2016, 7, 10478. [Google Scholar] [CrossRef]
- Grimm, E.R.; Steinle, N.I. Genetics of eating behavior: Established and emerging concepts. Nutr. Rev. 2011, 69, 52–60. [Google Scholar] [CrossRef]
- Herceg, Z.; Boffetta, P. Epigenetic changes in cancer: Role of environment. In Environmental Factors, Genes, and the Development of Human Cancers; Roy, D., Dorak, M., Eds.; Springer: New York, NY, USA, 2010; pp. 153–196. [Google Scholar]
- Fortner, R.T.; Sisti, J.; Chai, B.; Collins, L.C.; Rosner, B.; Hankinson, S.E.; Tamimi, R.M.; Eliassen, A.H. Parity, breastfeeding, and breast cancer risk by hormone receptor status and molecular phenotype: Results from the Nurses’ Health Studies. Breast Cancer Res. 2019, 21, 40. [Google Scholar] [CrossRef]
- Anderson, A.S.; Key, T.J.; Norat, T.; Scoccianti, C.; Cecchini, M.; Berrino, F.; Boutron-Ruault, M.C.; Espina, C.; Leitzmann, M.; Powers, H.; et al. European Code against Cancer 4th Edition: Obesity, body fatness and cancer. Cancer Epidemiol. 2015, 39 (Suppl. 1), S34–S45. [Google Scholar] [CrossRef]
- Segnan, N. Socioeconomic status and cancer screening. IARC Sci. Publ. 1997, 138, 369–376. [Google Scholar]
- Hastert, T.A.; Ruterbusch, J.J.; Beresford, S.A.; Sheppard, L.; White, E. Contribution of health behaviors to the association between area-level socioeconomic status and cancer mortality. Soc. Sci. Med. 2016, 148, 52–58. [Google Scholar] [CrossRef] [PubMed]
- Parida, S.; Sharma, D. The Microbiome-Estrogen Connection and Breast Cancer Risk. Cells 2019, 8, 1642. [Google Scholar] [CrossRef] [PubMed]
- Armaroli, P.; Villain, P.; Suonio, E.; Almonte, M.; Anttila, A.; Atkin, W.S.; Dean, P.B.; de Koning, H.J.; Dillner, L.; Herrero, R.; et al. European Code against Cancer, 4th Edition: Cancer screening. Cancer Epidemiol. 2015, 39 (Suppl. 1), S139–S152. [Google Scholar] [CrossRef]
- Nelson, H.D.; Fu, R.; Cantor, A.; Pappas, M.; Daeges, M.; Humphrey, L. Effectiveness of Breast Cancer Screening: Systematic Review and Meta-analysis to Update the 2009 U.S. Preventive Services Task Force Recommendation. Ann. Intern. Med. 2016, 164, 244–255. [Google Scholar] [CrossRef]
- Moss, S.M.; Nyström, L.; Jonsson, H.; Paci, E.; Lynge, E.; Njor, S.; Broeders, M.; Euroscreen Working Group. The impact of mammographic screening on breast cancer mortality in Europe: A review of trend studies. J. Med. Screen 2012, 19 (Suppl. 1), 26–32. [Google Scholar] [CrossRef]
- Giorgi Rossi, P.; Federici, A.; Farchi, S.; Chini, F.; Barca, A.; Guasticchi, G.; Borgia, P. The effect of screening programmes on the treatment of benign breast neoplasms: Observations from current practice in Italy. J. Med. Screen 2006, 13, 123–128. [Google Scholar] [CrossRef]
- Istat. Analisi del bridge coding Icd-9—Icd-10 per le statistiche di mortalità per causa in Italia, Metodi e Norme; Istat: Rome, Italy, 2011; p. 50. [Google Scholar]
- Giorgi Rossi, P.; Carrozzi, G.; Federici, A.; Mancuso, P.; Sampaolo, L.; Zappa, M. Invitation coverage and participation in Italian cervical, breast and colorectal cancer screening programmes. J. Med. Screen 2018, 25, 17–23. [Google Scholar] [CrossRef]
- Coviello, V.; Buzzoni, C.; Fusco, M.; Barchielli, A.; Cuccaro, F.; De Angelis, R.; Giacomin, A.; Luminari, S.; Randi, G.; Mangone, L.; et al. Survival of cancer patients in Italy. Epidemiol. Prev. 2017, 41 (Suppl. 1), 1–244. [Google Scholar]
- Giorgi Rossi, P.; Camilloni, L.; Mantellini, P.; Barile, V.; Borgia, P.; Federici, A.; Mangia, M.; Paci, E.; Vella, A.; Zappa, M. Breast cancer diagnostic methods: Screen-detected and clinical cases. An Italian survey of women’s experiences. Tumori J. 2007, 93, 452–460. [Google Scholar] [CrossRef]
- Plevritis, S.K.; Munoz, D.; Kurian, A.W.; Stout, N.K.; Alagoz, O.; Near, A.M.; Lee, S.J.; van den Broek, J.J.; Huang, X.; Schechter, C.B.; et al. Association of Screening and Treatment With Breast Cancer Mortality by Molecular Subtype in US Women, 2000–2012. JAMA 2018, 319, 154–164, Erratum in 2018, 319, 724. [Google Scholar] [CrossRef]
- Saadatmand, S.; Bretveld, R.; Siesling, S.; Tilanus-Linthorst, M.M. Influence of tumour stage at breast cancer detection on survival in modern times: Population based study in 173797 patients. BMJ 2015, 351, h4901. [Google Scholar] [CrossRef]
- Giordano, L.; Castagno, R.; Giorgi, D.; Piccinelli, C.; Ventura, L.; Segnan, N.; Zappa, M. Breast cancer screening in Italy: Evaluating key performance indicators for time trends and activity volumes. Epidemiol. Prev. 2015, 39 (3 Suppl. 1), 30–39. [Google Scholar]
- Sinopoli, A.; Saulle, R.; Guarino, A.; Cereda, D.; Giorgi Rossi, P.; Serantoni, G.; Giordano, L.; De Belvis, A.G.; Marino, M.; Bellentani, D.; et al. Experimenting an instrument for cancer screening programming in Italy. Ig Sanita Pubbl. 2017, 73, 303–309. (In Italian) [Google Scholar]
- Giorgi Rossi, P.; Petrelli, A.; Rossi, A.; Francovich, L.; Zappa, M.; Gargiulo, L. The inappropriateness in the use of female cancer screening tests in Italy: Over- and under-utilization determinants. Epidemiol. Prev. 2019, 43, 35–47. (In Italian) [Google Scholar]
- Njor, S.; Nyström, L.; Moss, S.; Paci, E.; Broeders, M.; Segnan, N.; Lynge, E.; Euroscreen Working Group. Breast cancer mortality in mammographic screening in Europe: A review of incidence-based mortality studies. J. Med. Screen 2012, 19 (Suppl. 1), 33–41. [Google Scholar]
- United Nations, Department of Economic and Social Affairs, Population Division. World Fertility Patterns 2015—Data Booklet. 2015. Available online: https://zimbra.ausl.re.it/service/home/~/?auth=co&loc=it&id=10573&part=3 (accessed on 21 May 2020).









© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giorgi Rossi, P.; Djuric, O.; Navarra, S.; Rossi, A.; Di Napoli, A.; Frova, L.; Petrelli, A. Geographic Inequalities in Breast Cancer in Italy: Trend Analysis of Mortality and Risk Factors. Int. J. Environ. Res. Public Health 2020, 17, 4165. https://doi.org/10.3390/ijerph17114165
Giorgi Rossi P, Djuric O, Navarra S, Rossi A, Di Napoli A, Frova L, Petrelli A. Geographic Inequalities in Breast Cancer in Italy: Trend Analysis of Mortality and Risk Factors. International Journal of Environmental Research and Public Health. 2020; 17(11):4165. https://doi.org/10.3390/ijerph17114165
Chicago/Turabian StyleGiorgi Rossi, Paolo, Olivera Djuric, Simone Navarra, Alessandra Rossi, Anteo Di Napoli, Luisa Frova, and Alessio Petrelli. 2020. "Geographic Inequalities in Breast Cancer in Italy: Trend Analysis of Mortality and Risk Factors" International Journal of Environmental Research and Public Health 17, no. 11: 4165. https://doi.org/10.3390/ijerph17114165
APA StyleGiorgi Rossi, P., Djuric, O., Navarra, S., Rossi, A., Di Napoli, A., Frova, L., & Petrelli, A. (2020). Geographic Inequalities in Breast Cancer in Italy: Trend Analysis of Mortality and Risk Factors. International Journal of Environmental Research and Public Health, 17(11), 4165. https://doi.org/10.3390/ijerph17114165