Immediate Effects of Tibialis Anterior and Calf Muscle Taping on Center of Pressure Excursion in Chronic Stroke Patients: A Cross-Over Study


Abstract
1. Introduction
2. Materials and Methods
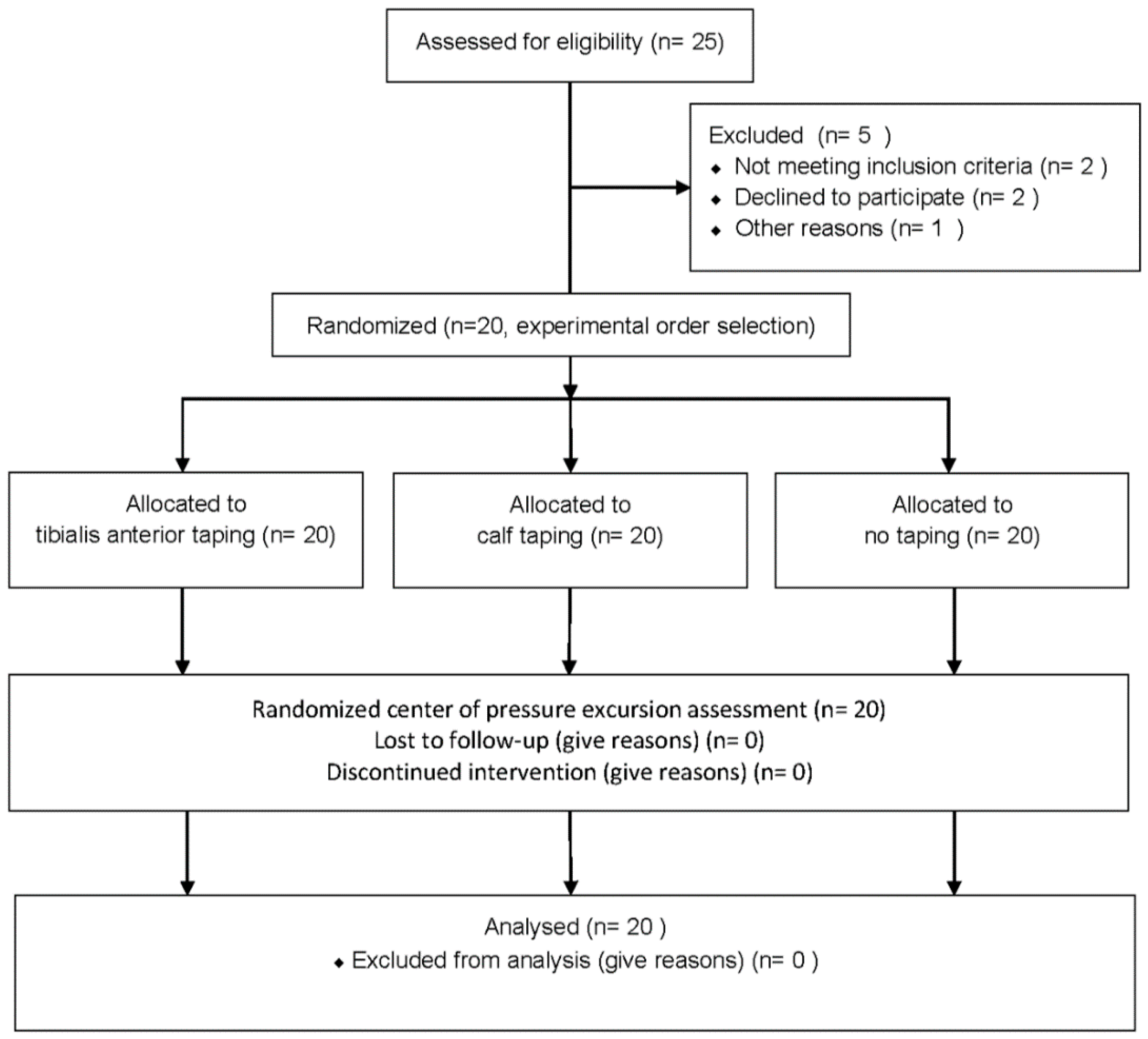
2.1. Participants
2.2. Sample Size Calculation
2.3. Study Design
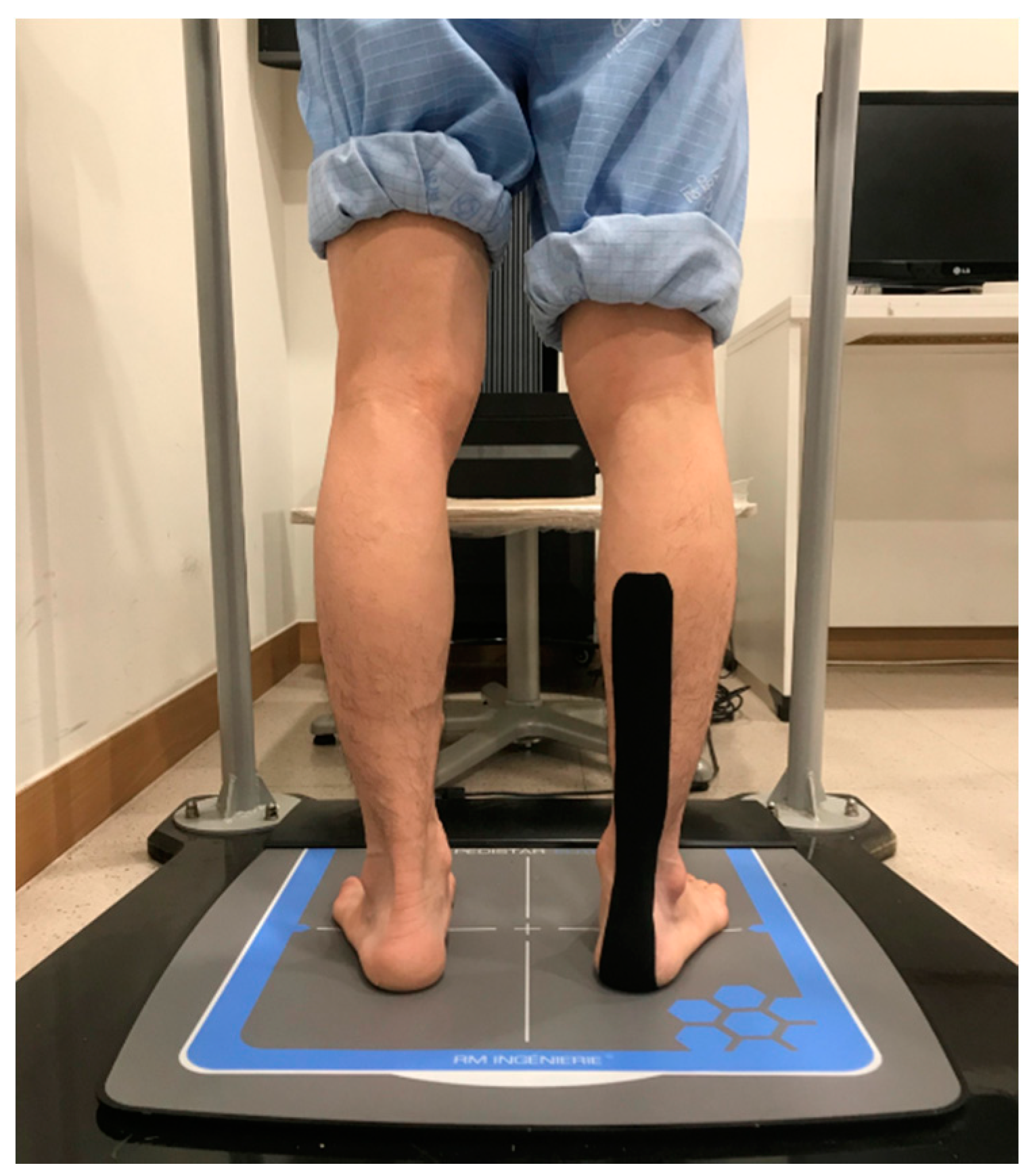
2.4. Taping Method
2.5. Tibial Muscle Taping
2.6. Calf Muscle Taping
2.7. Measurement Procedures
2.8. Measuring Changes in COP
2.9. Statistical Analysis
3. Result
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Wissel, J.; Verrier, M.; Simpson, D.M.; Charles, D.; Guinto, P.; Papapetropoulos, S.; Sunnerhagen, K.S. Post-stroke spasticity: Predictors of early development and considerations for therapeutic intervention. PM R 2015, 7, 60–67. [Google Scholar] [CrossRef] [PubMed]
- Gorst, T.; Rogers, A.; Morrison, S.C.; Cramp, M.; Paton, J.; Freeman, J.; Marsden, J. The prevalence, distribution, and functional importance of lower limb somatosensory impairments in chronic stroke survivors: A cross sectional observational study. Disabil. Rehabil. 2019, 41, 2443–2450. [Google Scholar] [CrossRef] [PubMed]
- Samuelsson, C.M.; Hansson, P.-O.; Persson, C.U. Early prediction of falls after stroke: A 12-month follow-up of 490 patients in The Fall Study of Gothenburg (FallsGOT). Clin. Rehabil. 2019, 33, 773–783. [Google Scholar] [CrossRef] [PubMed]
- De Oliveira, C.B.; de Medeiros, Í.R.T.; Ferreira, N.A.; Greters, M.E.; Conforto, A.B. Balance control in hemiparetic stroke patients: Main tools for evaluation. J. Rehabil. Res. Dev. 2008, 45, 1215–1226. [Google Scholar] [CrossRef] [PubMed]
- Lin, P.-Y.; Yang, Y.-R.; Cheng, S.-J.; Wang, R.-Y. The relation between ankle impairments and gait velocity and symmetry in people with stroke. Arch. Phys. Med. Rehabil. 2006, 87, 562–568. [Google Scholar] [CrossRef] [PubMed]
- Chung, S.G.; Van Rey, E.; Bai, Z.; Roth, E.J.; Zhang, L.Q. Biomechanic changes in passive properties of hemiplegic ankles with spastic hypertonia. Arch. Phys. Med. Rehabil. 2004, 85, 1638–1646. [Google Scholar] [CrossRef] [PubMed]
- Horak, F.B.; Nashner, L.M. Central programming of postural movements: Adaptation to altered support-surface configurations. J. Neurophysiol. 1986, 55, 1369–1381. [Google Scholar] [CrossRef] [PubMed]
- Cheng, P.-T.; Chen, C.-L.; Wang, C.-M.; Hong, W.-H. Leg muscle activation patterns of sit-to-stand movement in stroke patients. Am. J. Phys. Med. Rehabil. 2004, 83, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Kligyte, I.; Lundy-Ekman, L.; Medeiros, J.M. Relationship between lower extremity muscle strength and dynamic balance in people post-stroke. Medicina 2003, 39, 122–128. [Google Scholar] [PubMed]
- Cortesi, M.; Cattaneo, D.; Jonsdottir, J. Effect of kinesio taping on standing balance in subjects with multiple sclerosis: A pilot study\m {1}. NeuroRehabilitation 2011, 28, 365–372. [Google Scholar] [CrossRef] [PubMed]
- Jaraczewska, E.; Long, C. Kinesio® taping in stroke: Improving functional use of the upper extremity in hemiplegia. Top. Stroke Rehabil. 2006, 13, 31–42. [Google Scholar] [CrossRef] [PubMed]
- Koseoglu, B.F.; Dogan, A.; Tatli, H.U.; Ozcan, D.S.; Polat, C.S. Can kinesio tape be used as an ankle training method in the rehabilitation of the stroke patients? Complementary Ther. Clin. Pract. 2017, 27, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Rojhani-Shirazi, Z.; Amirian, S.; Meftahi, N. Effects of ankle kinesio taping on postural control in stroke patients. J. Stroke Cerebrovasc. Dis. 2015, 24, 2565–2571. [Google Scholar] [CrossRef] [PubMed]
- Salvat, I.S.; Salvat, A.A. Efectos inmediatos del kinesio taping en la flexión lumbar. Fisioterapia 2010, 32, 57–65. [Google Scholar] [CrossRef]
- Tamburella, F.; Scivoletto, G.; Molinari, M. Somatosensory inputs by application of KinesioTaping: Effects on spasticity, balance, and gait in chronic spinal cord injury. Front. Hum. Neurosci. 2014, 8, 367. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.R.; Kim, J.I.; Kim, Y.Y.; Kang, K.Y.; Kim, B.K.; Park, J.H.; An, H.J.; Min, K.O. Effects of ankle joint taping on postural balance control in stroke patients. J. Int. Acad. Phys. Ther. Res. 2012, 3, 446–452. [Google Scholar] [CrossRef]
- Langendoen, J.; Sertel, K. Kinesiology Taping: The Essential Step-by-Step Guide: Taping for Sports, Fitness & Daily Life: 160 Conditions & Ailments; Robert Rose: New York, NY, USA, 2014. [Google Scholar]
- Shin, Y.J.; Lee, J.H.; Choe, Y.W.; Kim, M.K. Immediate effects of ankle eversion taping on gait ability of chronic stroke patients. J. Bodyw. Mov. Ther. 2019, 23, 671–677. [Google Scholar] [CrossRef] [PubMed]
- Nashner, L. Adapting reflexes controlling the human posture. Exp. Brain Res. 1976, 26, 59–72. [Google Scholar] [CrossRef] [PubMed]
- Alexander, C.M.; McMullan, M.; Harrison, P.J. What is the effect of taping along or across a muscle on motoneurone excitability? A study using triceps surae. Man. Ther. 2008, 13, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, A.; Kahanov, L. The effect of kinesio taping on lower trunk range of motions. Res. Sports Med. 2007, 15, 103–112. [Google Scholar] [CrossRef] [PubMed]
- Chern, J.-S.; Chang, H.-S.; Lung, C.-W.; Wu, C.-Y.; Tang, S.F. Static ankle-foot orthosis improves static balance and gait functions in hemiplegic patients after stroke. In Proceedings of the 2013 35th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Osaka, Japan, 3–7 July 2013; pp. 5009–5012. [Google Scholar]
- Cikajlo, I.; Osrečki, K.; Burger, H. The effects of different types of ankle-foot orthoses on postural responses in individuals with walking impairments. Int. J. Rehabil. Res. 2016, 39, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Keklicek, H.; Uygur, F.; Yakut, Y. Effects of taping the hand in children with cerebral palsy. J. Hand Ther. 2015, 28, 27–33. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Subjects (n = 20) |
|---|---|
| Sex (male/female) | 14/6 |
| Paretic side (left/right) | 9/11 |
| Etiology (infarction/hemorrhage) | 13/7 |
| Age (years) | 58.95 ± 11.27 |
| Height (cm) | 163.30 ± 7.28 |
| Weight (kg) | 66.05 ± 6.36 |
| Disease duration (month) | 12.35 ± 2.56 |
| K–MMSE (point) | 27.60 ± 0.10 |
| K–NIHSS score | 9.65 ± 3.25 |
| Variable | Before Tape | TA Taping | Calf Taping | F | p |
|---|---|---|---|---|---|
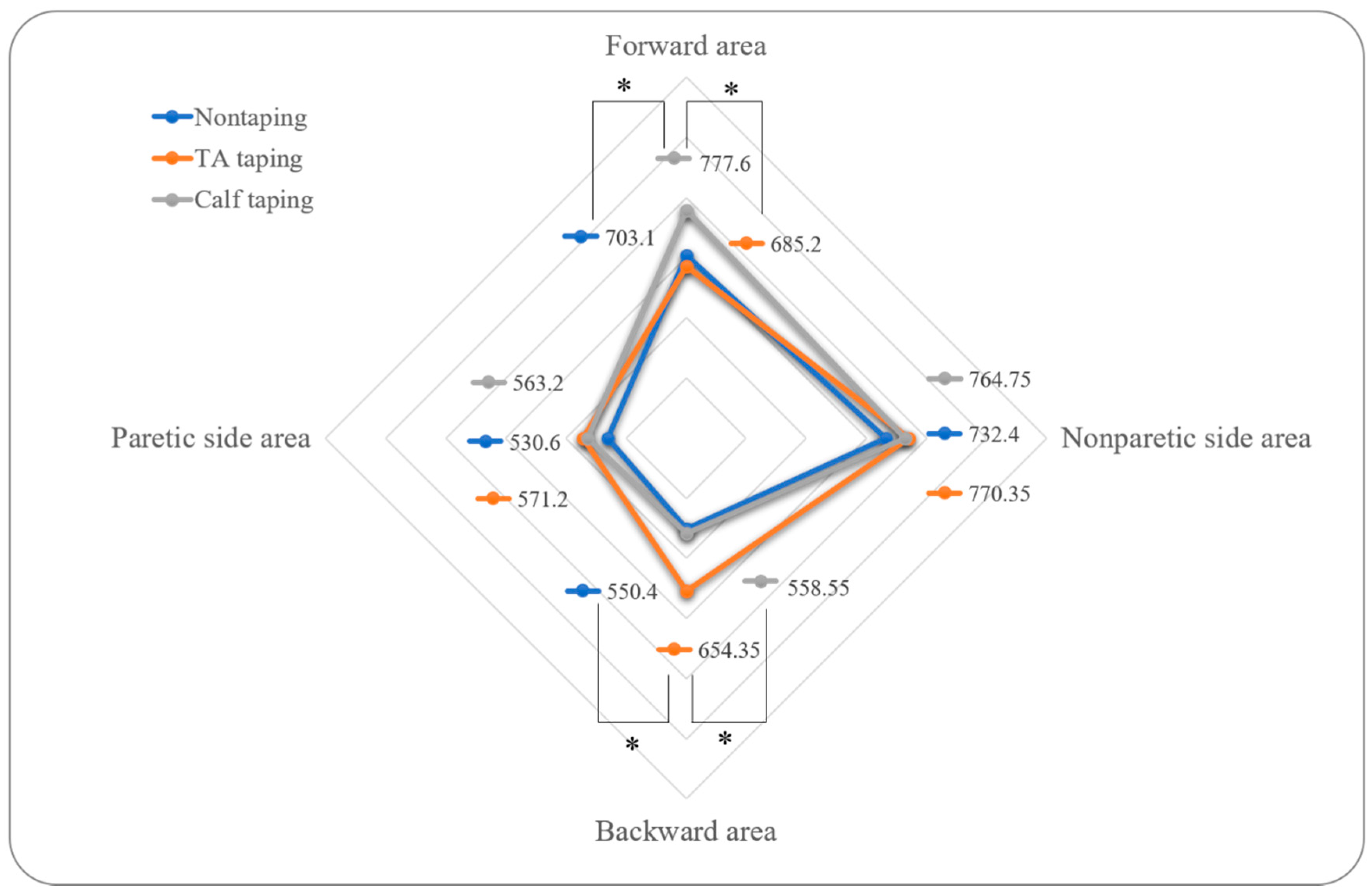
| Paretic side area | 530.60 ± 284.53 | 571.20 ± 271.40 | 563.20 ± 272.85 | 2.065 | 0.156 |
| Nonparetic side area | 732.40 ± 407.92 | 770.35 ± 443.29 | 764.75 ± 419.97 | 1.963 | 0.154 |
| Forward area | 703.10 ± 394.27 | 685.20 ± 392.86 | 777.60 ± 386.02 a | 5.596 | 0.013 * |
| Backward area | 550.40 ± 290.83 | 654.35 ± 328.69 b | 558.55 ± 305.57 | 9.289 | 0.001 * |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, S.J.; Kim, T.-H.; Oh, S. Immediate Effects of Tibialis Anterior and Calf Muscle Taping on Center of Pressure Excursion in Chronic Stroke Patients: A Cross-Over Study. Int. J. Environ. Res. Public Health 2020, 17, 4109. https://doi.org/10.3390/ijerph17114109
Park SJ, Kim T-H, Oh S. Immediate Effects of Tibialis Anterior and Calf Muscle Taping on Center of Pressure Excursion in Chronic Stroke Patients: A Cross-Over Study. International Journal of Environmental Research and Public Health. 2020; 17(11):4109. https://doi.org/10.3390/ijerph17114109
Chicago/Turabian StylePark, Shin Jun, Tae-Hyun Kim, and Seunghue Oh. 2020. "Immediate Effects of Tibialis Anterior and Calf Muscle Taping on Center of Pressure Excursion in Chronic Stroke Patients: A Cross-Over Study" International Journal of Environmental Research and Public Health 17, no. 11: 4109. https://doi.org/10.3390/ijerph17114109
APA StylePark, S. J., Kim, T.-H., & Oh, S. (2020). Immediate Effects of Tibialis Anterior and Calf Muscle Taping on Center of Pressure Excursion in Chronic Stroke Patients: A Cross-Over Study. International Journal of Environmental Research and Public Health, 17(11), 4109. https://doi.org/10.3390/ijerph17114109