Quality of Life in Liver Transplant Recipients: A Retrospective Study


 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
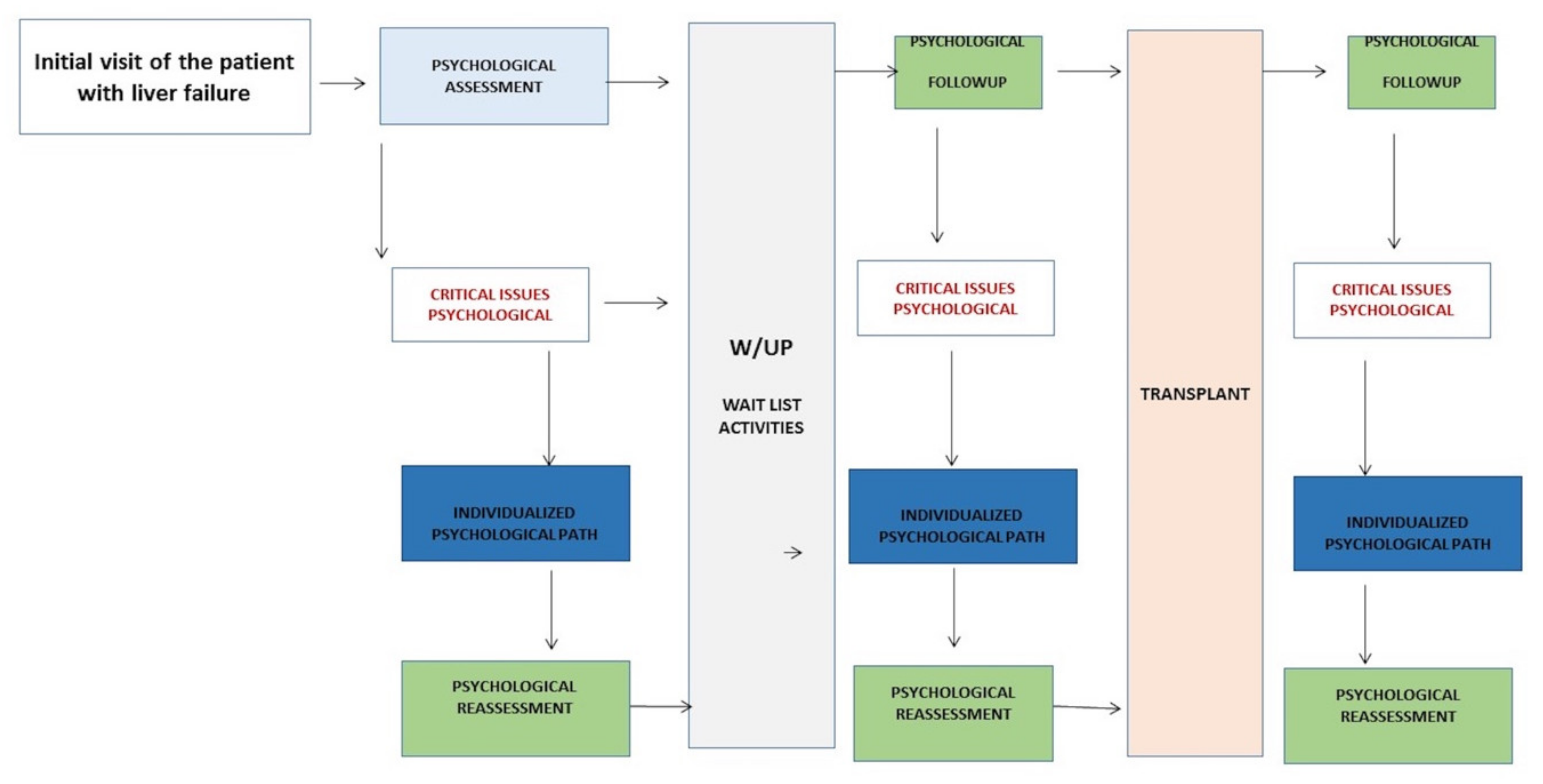
2.2. Psychology Pathway for Transplant Candidates
2.3. Tools
2.3.1. Quality of Life
2.3.2. Therapeutic Adherence
2.4. Statistical Analysis
3. Results
3.1. Analysis of Sociodemographic and Clinical Factors
3.2. Quality of Life
3.3. Compliance
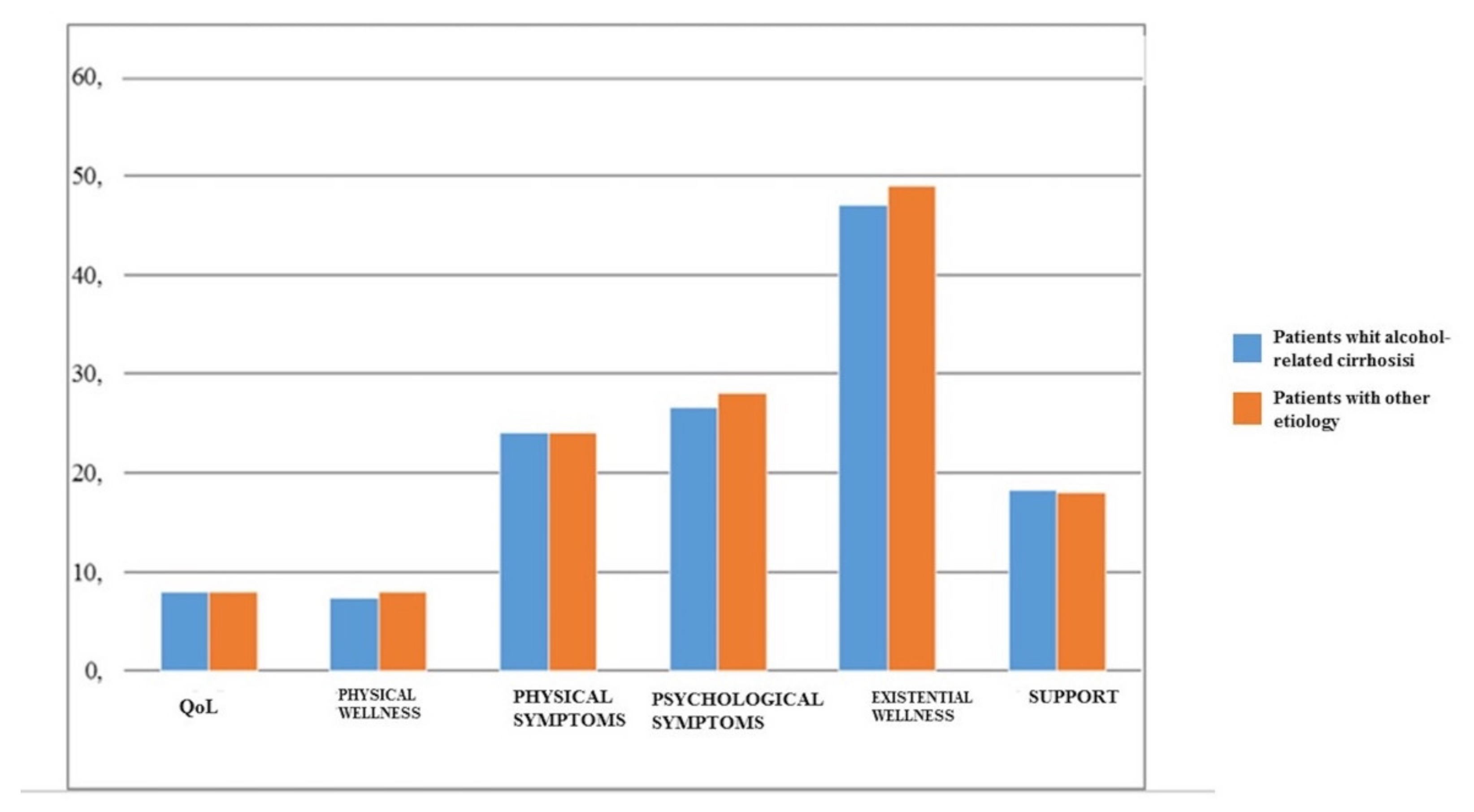
3.4. Alcohol-Related Cirrhosis
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Czyzewski, L.; Frelik, P.; Wyzgal, J.; Szarpak, L. Evaluation of Quality of Life and Severity of Depression, Anxiety, and Stress in Patients After Kidney Transplantation. Transplant. Proc. 2018, 50, 1733–1737. [Google Scholar] [CrossRef] [PubMed]
- Dabrowska-Bender, M.; Kozaczuk, A.; Paczek, L.; Milkiewicz, P.; Sloniewski, R.; Staniszewska, A. Patient Quality of Life After Liver Transplantation in Terms of Emotional Problems and the Impact of Sociodemographic Factors. Transplant. Proc. 2018, 50, 2031–2038. [Google Scholar] [CrossRef] [PubMed]
- Goetzmann, L.; Sarac, N.; Ambuhl, P.; Boehler, A.; Irani, S.; Msuellhaupt, B.; Noll, G.; Schleuniger, M.; Schwegler, K.; Buddeberg, C.; et al. Psychological Response and Quality of Life after Transplantation: A Comparison between Heart, Lung, Liver and Kidney Recipients. Swiss Med. Wkly. 2008, 138, 477–483. [Google Scholar] [CrossRef] [PubMed]
- Pinson, C.W.; Feurer, I.D.; Payne, J.L.; Wise, P.E.; Shockley, S.; Speroff, T. Health-related Quality of Life after Different Types of Solid Organ Transplantation. Ann. Surg. 2000, 232, 597–607. [Google Scholar] [CrossRef] [PubMed]
- Ortega, T.; Deulofeu, R.; Salamero, P.; Roman, A.; Masnou, N.; Rubio, S.; Garcia, O.; Casanovas, T.; Cofan, F.; Twose, J.; et al. Health-related Quality of Life before and after a Solid Organ Transplantation (Kidney, Liver, and Lung) of Four Catalonia Hospitals. Transplant. Proc. 2009, 41, 2265–2267. [Google Scholar] [CrossRef] [PubMed]
- Goetzmann, L.; Ruegg, L.; Stamm, M.; Ambuhl, P.; Boehler, A.; Halter, J.; Muellhaupt, B.; Noll, G.; Schanz, U.; Wagner-Huber, R.; et al. Psychosocial Profiles after Transplantation: A 24-month Follow-up of Heart, Lung, Liver, Kidney and Allogeneic Bone-marrow Patients. Transplantation 2008, 86, 662–668. [Google Scholar] [CrossRef] [PubMed]
- Beilby, S.; Moss-Morris, R.; Painter, L. Quality of Life before and after Heart, Lung and Liver Transplantation. N. Z. Med. J. 2003, 116, U381. [Google Scholar]
- Burra, P.; Germani, G. Long-term Quality of Life for Transplant ecipients. Liver Transpl. 2013, 19 (Suppl. 2), S40–S43. [Google Scholar] [CrossRef]
- Caruso, S.; Cianci, S.; Vitale, S.G.; Fava, V.; Cutello, S.; Cianci, A. Sexual Function and Quality of Life of Women Adopting the Levonorgestrel-releasing Intrauterine ystem (LNG-IUS 13.5 mg) after Abortion for Unintended Pregnancy. Eur. J. Contracept. Reprod. Health Care 2018, 23, 24–31. [Google Scholar] [CrossRef]
- Vitale, S.G.; Caruso, S.; Rapisarda, A.M.C.; Cianci, S.; Cianci, A. Isoflavones, Calcium, Vitamin D and Inulin Improve Quality of Life, Sexual Function, Body Composition and Metabolic Parameters in Menopausal Women: Result from a Prospective, Randomized, Placebo-controlled, Parallel-group Study. Prz. Menopauzalny 2018, 17, 32–38. [Google Scholar] [CrossRef]
- Vitale, S.G.; Lagana, A.S.; Noventa, M.; Giampaolino, P.; Zizolfi, B.; Buttice, S.; La Rosa, V.L.; Gullo, G.; Rossetti, D. Transvaginal Bilateral Sacrospinous Fixation after Second Recurrence of Vaginal Vault Prolapse: Efficacy and Impact on Quality of Life and Sexuality. Biomed. Res. Int. 2018, 2018, 5727165. [Google Scholar] [CrossRef]
- Caruso, S.; Iraci, M.; Cianci, S.; Vitale, S.G.; Fava, V.; Cianci, A. Effects of Long-term Treatment with Dienogest on the Quality of Life and Sexual Function of Women Affected by Endometriosis-associated Pelvic Pain. J. Pain. Res. 2019, 12, 2371–2378. [Google Scholar] [CrossRef] [PubMed]
- Girgenti, R.; Lo Re, V.; Antonina Buttafarro, M. Resilienza E Resistenza Al Cambiamento: L’attività Psicoterapica Con Pazienti rapiantati. Riv. Di. Psicoter. Relaz. 2018, 47, 79–93. [Google Scholar] [CrossRef]
- Vitale, S.G.; Caruso, S.; Rapisarda, A.M.C.; Valenti, G.; Rossetti, D.; Cianci, S.; Cianci, A. Biocompatible Porcine Dermis Graft to Treat Severe Cystocele: Impact on Quality of Life and Sexuality. Arch. Gynecol. Obs. 2016, 293, 125–131. [Google Scholar] [CrossRef]
- Vitale, S.G.; Ferrero, S.; Ciebiera, M.; Barra, F.; Torok, P.; Tesarik, J.; Vilos, G.A.; Cianci, A. Hysteroscopic Endometrial Resection Vs. Hysterectomy for Abnormal Uterine Bleeding: Impact on Quality of Life and Sexuality. Evidence from A Systematic Review of Randomized Controlled Trials. Curr. Opin. Obs. Gynecol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Vitale, S.G.; La Rosa, V.L.; Rapisarda, A.M.C.; Lagana, A.S. Impact of Endometriosis on Quality of Life and Psychological Well-being. J. Psychosom. Obs. Gynaecol. 2017, 38, 317–319. [Google Scholar] [CrossRef]
- Bravata, D.M.; Olkin, I.; Barnato, A.E.; Keeffe, E.B.; Owens, D.K. Health-related Quality of Life after Liver Transplantation: A Meta-analysis. Liver Transpl. Surg. 1999, 5, 318–331. [Google Scholar] [CrossRef]
- Duffy, J.P.; Kao, K.; Ko, C.Y.; Farmer, D.G.; McDiarmid, S.V.; Hong, J.C.; Venick, R.S.; Feist, S.; Goldstein, L.; Saab, S.; et al. Long-term Patient Outcome and Quality of Life after Liver Transplantation: Analysis of 20-year Survivors. Ann. Surg. 2010, 252, 652–661. [Google Scholar] [CrossRef]
- Masala, D.; Mannocci, A.; Unim, B.; Del Cimmuto, A.; Turchetta, F.; Gatto, G.; Santoro, R.; Ettorre, G.M.; Boccia, A.; La Torre, G. Quality of Life and Physical Activity in Liver Transplantation Patients: Results of a Case-control Study in Italy. Transplant. Proc. 2012, 44, 1346–1350. [Google Scholar] [CrossRef]
- Wang, G.S.; Yang, Y.; Li, H.; Jiang, N.; Fu, B.S.; Jin, H.; Yang, J.X.; Chen, G.H. Health-related Quality of Life after Liver Transplantation: The Experience from a Single Chinese Center. Hepatobiliary Pancreat. Dis. Int. HBPD INT. 2012, 11, 262–266. [Google Scholar] [CrossRef]
- Telles-Correia, D.; Barbosa, A.; Mega, I.; Mateus, E.; Monteiro, E. When does Quality of Life Improve after Liver Transplantation? A longitudinal Prospective Study. Transplant. Proc. 2009, 41, 904–905. [Google Scholar] [CrossRef] [PubMed]
- Onghena, L.; Develtere, W.; Poppe, C.; Geerts, A.; Troisi, R.; Vanlander, A.; Berrevoet, F.; Rogiers, X.; Van Vlierberghe, H.; Verhelst, X. Quality of Life after Liver Transplantation: State of the Art. World J. Hepatol. 2016, 8, 749–756. [Google Scholar] [CrossRef] [PubMed]
- Painter, P.; Krasnoff, J.; Paul, S.M.; Ascher, N.L. Physical Activity and Health-related Quality of Life in Liver Transplant Recipients. Liver Transpl. 2001, 7, 213–219. [Google Scholar] [CrossRef]
- Yang, L.S.; Shan, L.L.; Saxena, A.; Morris, D.L. Liver Transplantation: A Systematic Review of Long-term Quality of Life. Liver Int. Off. J. Int. Assoc. Study Liver 2014, 34, 1298–1313. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.R.; Mount, B.M.; Strobel, M.G.; Bui, F. The McGill Quality of Life Questionnaire: A Measure of Quality of Life Appropriate for People with Advanced Disease. A Preliminary Study of Validity and Acceptability. Palliat. Med. 1995, 9, 207–219. [Google Scholar] [CrossRef]
- Morisky, D.E.; Ang, A.; Krousel-Wood, M.; Ward, H.J. Predictive Validity of a Medication Adherence Measure in an Outpatient Setting. J. Clin. Hypertens. Greenwich Conn 2008, 10, 348–354. [Google Scholar] [CrossRef]
- De Las Cuevas, C.; Penate, W. Psychometric Properties of the Eight-item Morisky Medication Adherence Scale (MMAS-8) in a Psychiatric Outpatient Setting. Int. J. Clin. Health Psychol. 2015, 15, 121–129. [Google Scholar] [CrossRef]
- Berlakovich, G.A. Challenges in Transplantation for Alcoholic Liver Disease. World J. Gastroenterol. 2014, 20, 8033–8039. [Google Scholar] [CrossRef]
- Vassallo, G.A.; Tarli, C.; Rando, M.M.; Mosoni, C.; Mirijello, A.; Agyei-Nkansah, A.; Antonelli, M.; Sestito, L.; Perotti, G.; Di Giuda, D.; et al. Liver Transplantation in Patients with Alcoholic Liver Disease: A Retrospective Study. Alcohol 2018, 53, 151–156. [Google Scholar] [CrossRef]
- Lim, J.; Curry, M.P.; Sundaram, V. Risk Factors and Outcomes Associated with Alcohol Relapse after Liver Transplantation. World J. Hepatol. 2017, 9, 771–780. [Google Scholar] [CrossRef]
- Lee, B.P.; Mehta, N.; Platt, L.; Gurakar, A.; Rice, J.P.; Lucey, M.R.; Im, G.Y.; Therapondos, G.; Han, H.; Victor, D.W.; et al. Outcomes of Early Liver Transplantation for Patients With Severe Alcoholic Hepatitis. Gastroenterology 2018, 155, 422–430. [Google Scholar] [CrossRef] [PubMed]
- Marroni, C.A.; Fleck, A.M., Jr.; Fernandes, S.A.; Galant, L.H.; Mucenic, M.; de Mattos Meine, M.H.; Mariante-Neto, G.; Brandao, A.B.M. Liver Transplantation and Alcoholic Liver Disease: History, Controversies, and Considerations. World J. Gastroenterol. 2018, 24, 2785–2805. [Google Scholar] [CrossRef] [PubMed]
- Szabo, G.; Kamath, P.S.; Shah, V.H.; Thursz, M.; Mathurin, P.; Meeting, E.-A. Alcohol-Related Liver Disease: Areas of Consensus, Unmet Needs and Opportunities for Further Study. Hepatology 2019, 69, 2271–2283. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| N = 82 | ||
|---|---|---|
| Age, years | 56 ± 9 | |
| Male | 62 (76%) | |
| Female | 20 (24%) | |
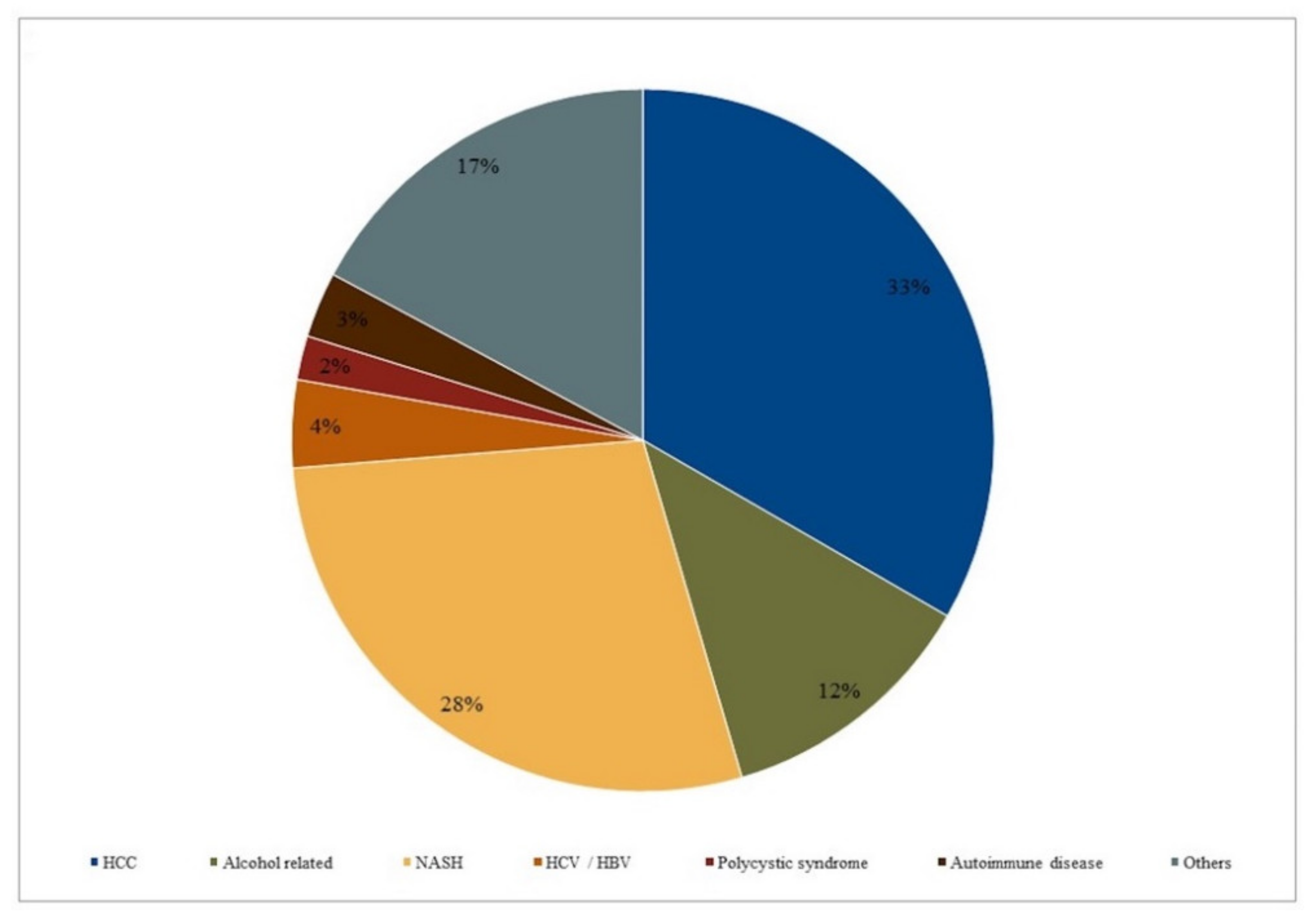
| Main Etiology | HCC (33%) | |
| Transplant date | 2017–2019 | |
| MELD | Score 1 | ISO > 30 = 11 |
| Score 2 | 20 < ISO < 30 = 53 | |
| Score 3 | ISO < 20 = 15 | |
| Total Patients | Transplant Recipients Since over Two Years | Transplant Recipients Since Less than Two Years | |
|---|---|---|---|
| (n = 34) | (n = 46) | ||
| Total QOL | 8/10 | 8 | 7 |
| (excellent) | |||
| Physical well-being | 8/10 | 8 | 7 |
| (excellent) | |||
| Physical symptoms | 24/30 | 25 | 24 |
| (no problem) | |||
| Psychological symptoms | 28/40 | 28 | 28 |
| (no problem) | |||
| Existential well-being | 49/60 | 51 | 46 |
| (excellent) | |||
| Support | 18/20 | 18 | 18 |
| (excellent) |
| Main Physical Symptoms Reported | N Reported Cases |
|---|---|
| Abdominal hernia | 7 |
| Fatigue | 6 |
| Mucositis | 1 |
| Insomnia | 1 |
| Joint rigidity | 2 |
| Pain | 3 |
| Hcc recurrence | 3 |
| Reference | Title | Study Design | Population (n) | Instruments Used to Assess QOL | Main Conclusions |
|---|---|---|---|---|---|
| Bravata, Olkin, Barnato, Keeffe, Owens (1999) [12] | Health-related quality of life after liver transplantation: a meta analysis | Meta-analysis | N/A | N/A | Transplant recipients reported large gains in those aspects of QOL most affected by physical health and smaller improvements in areas affected by psychological functioning. |
| Duffy, Kao, Ko, Farmer, McDiarmid, Hong et al. (2010) [13] | When does quality of life improve after liver transplantation? A longitudinal prospective study | Prospective, cross-sectional study | 168 | SF-36 | More than 50% of LT recipients survive 20 years, achieve important socioeconomic milestones, and report quality of life superior to patients with liver disease or other chronic conditions. |
| Masala, Mannocci, Unim, Cimmuto, Turchetta, Gatto et al. (2012) [14] | Quality of life and physical activity in liver transplantation patients: Results of a case-control study in Italy | Case-control | 45 transplant patients, 108 controls | SF-36 | Transplant recipients are more subject to low physical functions and to psychological/emotional distress compared to the general population. |
| IPAQ | |||||
| Wang, Yang, Li, Jiang, Fu, Jin et al. (2012) [15] | Health-related quality of life after liver transplantation: The experience from a single Chinese center | Case-control | 60 post-LT, 55 benign end-stage liver disease, 50 controls | SF-36 | In transplant recipients QOL remains to be improved, but generally they have a good QOL. |
| Sirivatanauksorn, Dumronggittigule, Limsrichamrern, Iramaneerat, Kolladarungkri, Kositamongkol et al. (2012) [16] | Quality of life among liver transplantation patients | Case-control | 57 pre-LT 95 post-LT | SF-36 | Liver transplant recipients and also their caregivers have a good QOL. |
| CLDQ | |||||
| Ridolfi, Nanni Costa, Martinelli, Donati, Morselli Labate, Venturoli. [17] | Qualità di Vita ed Integrazione Sociale delle Persone Sottoposte a Trapianto dell’Organo Salvavita: Fegato | Cohort study | 365 | SF-36 | QOL in transplant recipients returns to excellent levels, similarly to a control group population. The progressive improvement in time of the physical role and state score demonstrated that regaining social “normality” is in any case possible for most of these individuals. |
| Q-Qsex | |||||
| Telles-Correia, Barbosa, Mega, Mateus, Monteiro (2009) [18] | When does quality of life improve after liver transplantation? A longitudinal prospective study | Cohort study | 60 | SF-36 | QOL improved early after liver transplantation (1 month), mostly with a significant improvement in the physical quality of life. |
| Onghena, Develtere, Poppe, Geerts, Troisi, Vanlander (2016) [19] | Quality of life after liver transplantation: State of the art | Review | N/A | N/A | During the first year there is a significant improvement in QOL, which remains stable thereafter. |
| Painter, Krasnoff, Paul, Ascher (2001) [20] | Physical Activity and Health-Related Quality of Life in Liver Transplant Recipients | Cohort study | 180 | SF-36 | This study indicates that physical activity is related to QOL after liver transplantation independent of other coexisting medical conditions. |
| Yang, Shan, Saxena, Morris (2014) [21] | Liver transplantation: a systematic review of long-term quality of life | Review | N/A | N/A | Liver transplantation confers specific long-term QOL and functional benefits when compared to preoperative status. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Girgenti, R.; Tropea, A.; Buttafarro, M.A.; Ragusa, R.; Ammirata, M. Quality of Life in Liver Transplant Recipients: A Retrospective Study. Int. J. Environ. Res. Public Health 2020, 17, 3809. https://doi.org/10.3390/ijerph17113809
Girgenti R, Tropea A, Buttafarro MA, Ragusa R, Ammirata M. Quality of Life in Liver Transplant Recipients: A Retrospective Study. International Journal of Environmental Research and Public Health. 2020; 17(11):3809. https://doi.org/10.3390/ijerph17113809
Chicago/Turabian StyleGirgenti, Rosario, Alessandro Tropea, Maria Antonina Buttafarro, Rosalia Ragusa, and Martina Ammirata. 2020. "Quality of Life in Liver Transplant Recipients: A Retrospective Study" International Journal of Environmental Research and Public Health 17, no. 11: 3809. https://doi.org/10.3390/ijerph17113809
APA StyleGirgenti, R., Tropea, A., Buttafarro, M. A., Ragusa, R., & Ammirata, M. (2020). Quality of Life in Liver Transplant Recipients: A Retrospective Study. International Journal of Environmental Research and Public Health, 17(11), 3809. https://doi.org/10.3390/ijerph17113809