Effects of the Use of Air Purifier on Indoor Environment and Respiratory System among Healthy Adults


 and
and
Abstract
1. Introduction
2. Materials and Methods
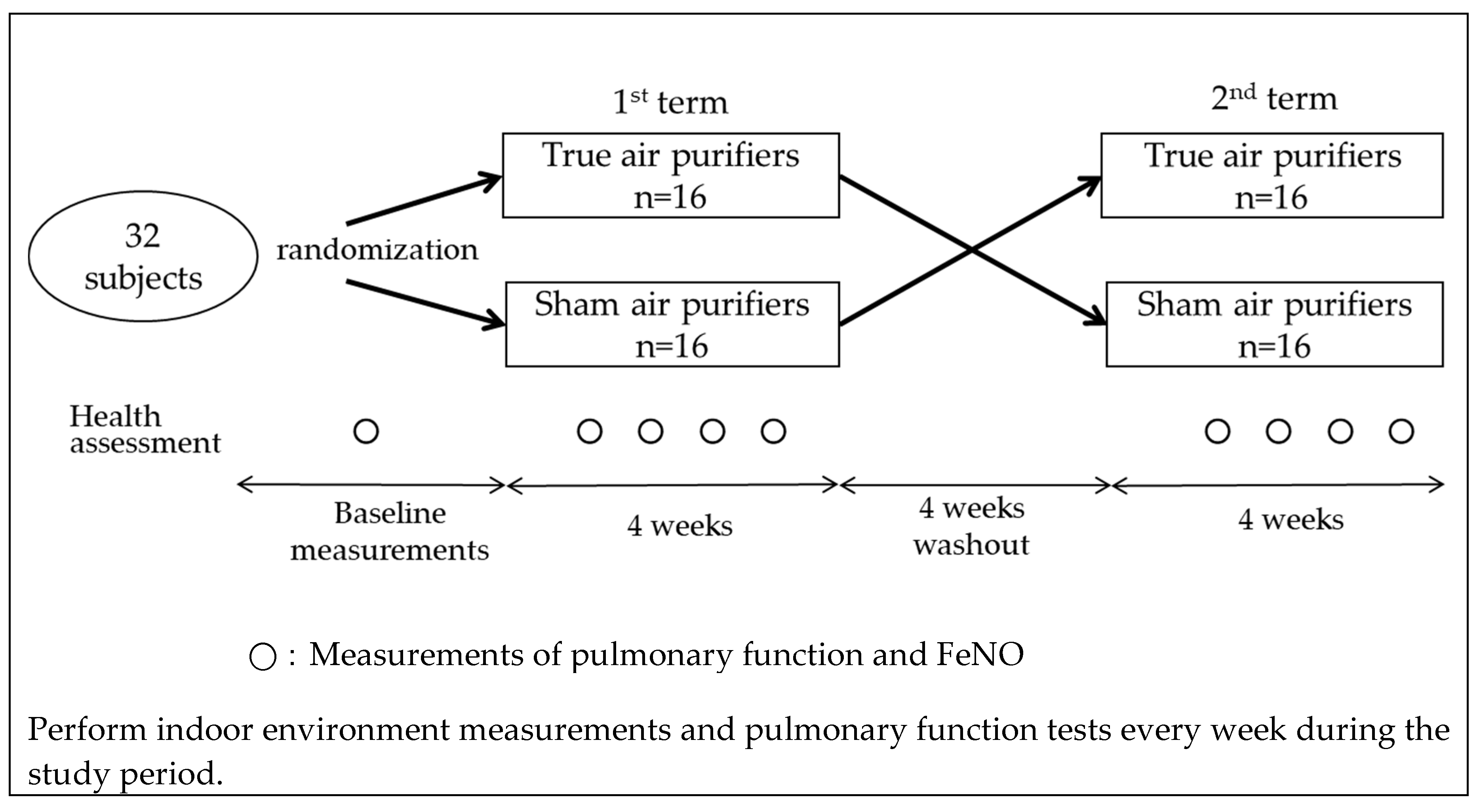
2.1. Study Design
2.2. Sample and Data Collection
2.3. Statistical Analyses
3. Results
3.1. Descriptive Statistics
3.2. Indoor Air Pollutant Levels in Relation to Living Environment Factors
3.3. Associations Air Pollutant Levels and Pulmonary Function
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| PM | particulate matter |
| PM2.5 | fine particulate matter ≤ 2.5 µm in aerodynamic diameter |
| PM10–2.5 | coarse particulate matter between 2.5 and 10 µm in aerodynamic diameter |
| O3 | ozone |
| FEV1.0 | forced expiratory volume in one second |
| FVC | forced vital capacity |
| MMEF | maximal mid-expiratory flow |
| PEF | peak expiratory flow rate |
| 50/25 | The ratio of the maximum expiratory flow rate at 50% of the FVC to the maximum expiratory flow rate at 25% of the FVC |
| FeNO | fractional exhaled nitric oxide |
| I/O ratio | indoor-to-outdoor concentration ratio |
| SD | standard deviation |
| BMI | body mass index |
| CI | confidence interval |
References
- Whitby, K.T. The physical characteristics of sulfur aerosols. Atmos. Environ. 1978, 12, 135–159. [Google Scholar] [CrossRef]
- Wilson, W.E.; Suh, H.H. Fine particles and coarse particles: concentration relationships relevant to epidemiologic studies. J. Air Waste Manag. Assoc. 1997, 47, 1238–1249. [Google Scholar] [CrossRef]
- Kloog, I.; Coull, B.A.; Zanobetti, A.; Koutrakis, P.; Schwartz, J.D. Acute and chronic effects of particles on hospital admissions in New-England. PloS One 2012, 7, e34664. [Google Scholar] [CrossRef]
- Churg, A.; Brauer, M.; del Carmen, A.M.; Fortoul, T.I.; Wright, J.L. Chronic exposure to high levels of particulate air pollution and small airway remodeling. Environ. Health Perspect. 2003, 111, 714–718. [Google Scholar] [CrossRef]
- Barraza-Villarreal, A.; Sunyer, J.; Hernandez-Cadena, L.; Escamilla-Nunez, M.C.; Sienra-Monge, J.J.; Ramirez-Aguilar, M.; Cortez-Lugo, M.; Holguin, F.; Diaz-Sanchez, D.; Olin, A.C.; et al. Air pollution, airway inflammation, and lung function in a cohort study of Mexico City schoolchildren. Environ. Health. Perspect. 2008, 116, 832–838. [Google Scholar] [CrossRef]
- Wu, S.; Ni, Y.; Li, H.; Pan, L.; Yang, D.; Baccarelli, A.A.; Deng, F.; Chen, Y.; Shima, M.; Guo, X. Short-term exposure to high ambient air pollution increases airway inflammation and respiratory symptoms in chronic obstructive pulmonary disease patients in Beijing, China. Environ. Int. 2016, 94, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.H.; Chan, C.C.; Chen, B.Y.; Cheng, T.J.; Guo, Y.L. Effects of particulate air pollution and ozone on lung function in non-asthmatic children. Environ. Res. 2015, 137, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Hwang, B.F.; Chen, Y.H.; Lin, Y.T.; Wu, X.T.; Lee, Y.L. Relationship between exposure to fine particulates and ozone and reduced lung function in children. Environ. Res. 2015, 137, 382–390. [Google Scholar] [CrossRef] [PubMed]
- Yoda, Y.; Takagi, H.; Wakamatsu, J.; Ito, T.; Nakatsubo, R.; Horie, Y.; Hiraki, T.; Shima, M. Acute effects of air pollutants on pulmonary function among students: A panel study in an isolated island. Environ. Health Prev. Med. 2017, 22. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Chen, Q.; Zheng, X.; Li, Y.; Han, M.; Liu, T.; Xiao, J.; Guo, L.; Zeng, W.; Zhang, J.; et al. Effects of ambient ozone concentrations with different averaging times on asthma exacerbations: A meta-analysis. Sci. Total Environ. 2019, 691, 549–561. [Google Scholar] [CrossRef]
- Simoni, M.; Jaakkola, M.S.; Carrozzi, L.; Baldacci, S.; Di Pede, F.; Viegi, G. Indoor air pollution and respiratory health in the elderly. Eur. Respir. J. 2003, 40, 15s–20s. [Google Scholar] [CrossRef] [PubMed]
- Skulberg, K.R.; Skyberg, K.; Kruse, K.; Eduard, W.; Levy, F.; Kongerud, J.; Djupesland, P. The effects of intervention with local electrostatic air cleaners on airborne dust and the health of office employees. Indoor Air 2005, 15, 152–159. [Google Scholar] [CrossRef] [PubMed]
- Hacker, D.W.; Sparrow, E.M. Use of air-cleaning devices to create airborne particle-free spaces intended to alleviate allergic rhinitis and asthma during sleep. Indoor Air 2005, 15, 420–431. [Google Scholar] [CrossRef] [PubMed]
- Batterman, S.; Du, L.; Mentz, G.; Mukherjee, B.; Parker, E.; Godwin, C.; Chin, J.Y.; O’Toole, A.; Robins, T.; Rowe, Z.; et al. Particulate matter concentrations in residences: An intervention study evaluating stand-alone filters and air conditioners. Indoor Air 2012, 22, 235–252. [Google Scholar] [CrossRef]
- Butz, A.M.; Matsui, E.C.; Breysse, P.; Curtin-Brosnan, J.; Eggleston, P.; Diette, G.; Williams, D.; Yuan, J.; Bernert, J.T.; Rand, C. A randomized trial of air cleaners and a health coach to improve indoor air quality for inner-city children with asthma and secondhand smoke exposure. Arch. Pediatr. Adolesc. Med. 2011, 165, 741–748. [Google Scholar] [CrossRef]
- Vyas, S.; Srivastav, N.; Spears, D. An Experiment with Air Purifiers in Delhi during Winter 2015–2016. PLoS ONE 2016, 11, e0167999. [Google Scholar] [CrossRef]
- Ying, X.; Suresh, R.; Andrea, R.F.; Peter, A.J.; Philip, K.H.; Cheryl, G.; Larry, E.W. Effectiveness of heating, ventilation and air conditioning system with HEPA filter unit on indoor air quality and asthmatic children’s health. Build. Environ. 2010, 45, 330–337. [Google Scholar] [CrossRef]
- Park, H.K.; Cheng, K.C.; Tetteh, A.O.; Hildemann, L.M.; Nadeau, K.C. Effectiveness of air purifier on health outcomes and indoor particles in homes of children with allergic diseases in Fresno, California: A pilot study. J. Asthma 2017, 54, 341–346. [Google Scholar] [CrossRef]
- Martenies, S.E.; Batterman, S.A. Effectiveness of using enhanced filters in schools and homes to reduce indoor exposures to PM2.5 from outdoor sources and subsequent health benefits for children with asthma. Environ. Sci. Technol. 2018, 52, 10767–10776. [Google Scholar] [CrossRef]
- Der Heide, S.V.; Van Aalderen, W.M.; Kauffman, H.F.; Dubois, A.E.; De Monchy, J.G. Clinical effects of air cleaners in homes of asthmatic children sensitized to pet allergens. J. Allergy Clin. Immunol. 1999, 104, 447–451. [Google Scholar] [CrossRef]
- Francis, H.; Fletcher, G.; Anthony, C.; Pickering, C.; Oldham, L.; Hadley, E.; Custovic, A.; Niven, R. Clinical effects of air filters in homes of asthmatic adults sensitized and exposed to pet allergens. Clin. Exp. Allergy 2003, 33, 101–105. [Google Scholar] [CrossRef] [PubMed]
- Karottki, D.G.; Spilak, M.; Frederiksen, M.; Andersen, Z.J.; Madsen, A.M.; Ketzel, M.; Massling, A.; Gunnarsen, L.; Moller, P.; Loft, S. Indoor and outdoor exposure to ultrafine, fine and microbiologically derived particulate matter related to cardiovascular and respiratory effects in a panel of elderly urban citizens. Int. J. Environ. Res. Public Health 2015, 12, 1667–1686. [Google Scholar] [CrossRef] [PubMed]
- Karottki, D.G.; Spilak, M.; Frederiksen, M.; Gunnarsen, L.; Brauner, E.V.; Kolarik, B.; Andersen, Z.J.; Sigsgaard, T.; Barregard, L.; Strandberg, B.; et al. An indoor air filtration study in homes of elderly: Cardiovascular and respiratory effects of exposure to particulate matter. Environ. Health 2013, 12, 116. [Google Scholar] [CrossRef] [PubMed]
- Shao, D.; Du, Y.; Liu, S.; Brunekreef, B.; Meliefste, K.; Zhao, Q.; Chen, J.; Song, X.; Wang, M.; Wang, J.; et al. Cardiorespiratory responses of air filtration: A randomized crossover intervention trial in seniors living in Beijing: Beijing indoor air purifier study, BIAPSY. Sci. Total Environ. 2017, 603–604, 541–549. [Google Scholar] [CrossRef] [PubMed]
- Weichenthal, S.; Mallach, G.; Kulka, R.; Black, A.; Wheeler, A.; You, H.; St-Jean, M.; Kwiatkowski, R.; Sharp, D. A randomized double-blind crossover study of indoor air filtration and acute changes in cardiorespiratory health in a First Nations community. Indoor Air 2013, 23, 175–184. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.; Zhao, A.; Chen, H.; Zhao, Z.; Cai, J.; Wang, C.; Yang, C.; Li, H.; Xu, X.; Ha, S.; et al. Cardiopulmonary benefits of reducing indoor particles of outdoor origin: A randomized, double-blind crossover trial of air purifiers. J. Am. Coll. Cardiol. 2015, 65, 2279–2287. [Google Scholar] [CrossRef] [PubMed]
- Riley, W.J.; McKone, T.E.; Lai, A.C.; Nazaroff, W.W. Indoor particulate matter of outdoor origin: Importance of size-dependent removal mechanisms. Environ. Sci. Technol. 2002, 36, 200–207. [Google Scholar] [CrossRef]
- Abt, E.; Suh, H.H.; Allen, G.; Koutrakis, P. Characterization of indoor particle sources: A study conducted in the metropolitan Boston area. Environ. Health Perspect. 2000, 108, 35–44. [Google Scholar] [CrossRef]
- Weisel, C.P.; Zhang, J.; Turpin, B.J.; Morandi, M.T.; Colome, S.; Stock, T.H.; Spektor, D.M.; Korn, L.; Winer, A.M.; Kwon, J.; et al. Relationships of indoor, outdoor, and personal air (RIOPA). Part I. Collection methods and descriptive analyses. Res. Rep. Health Eff. Inst. 2005, 130, discussion 109–127. [Google Scholar]
- McCormack, M.C.; Breysse, P.N.; Hansel, N.N.; Matsui, E.C.; Tonorezos, E.S.; Curtin-Brosnan, J.; Williams, D.L.; Buckley, T.J.; Eggleston, P.A.; Diette, G.B. Common household activities are associated with elevated particulate matter concentrations in bedrooms of inner-city Baltimore pre-school children. Environ. Res. 2008, 106, 148–155. [Google Scholar] [CrossRef]
- Cestonaro, L.V.; Marcolan, A.M.; Rossato-Grando, L.G.; Anzolin, A.P.; Goethel, G.; Vilani, A.; Garcia, S.C.; Bertol, C.D. Ozone generated by air purifier in low concentrations: Friend or foe? Environ. Sci. Pollut. Res. Int. 2017, 24, 22673–22678. [Google Scholar] [CrossRef] [PubMed]
- Ogawa & Co., USA, Inc. Protocol for Ozone Measurement Using the Ozone Passive Sampler Badge. Available online: http://ogawausa.com/wp-content/uploads/2014/04/proozone.pdf (accessed on 2 April 2020).
- Tang, N.; Yoda, Y.; Otani, N.; Kameda, T.; Toriba, A.; Hayakawa, K.; Shima, M. Personal and atmospheric concentrations of ozone in southeastern Hyogo prefecture, Japan. Chem. Pharm. Bull. (Tokyo). 2012, 60, 962–966. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.R.; Crapo, R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Enright, P.; van der Grinten, C.P.; Gustafsson, P.; et al. General considerations for lung function testing. Eur. Respir. J. 2005, 26, 153–161. [Google Scholar] [CrossRef] [PubMed]
- American Thoracic Society; European Respiratory Society. ATS/ERS recommendations for standardized procedures for the online and offline measurement of exhaled lower respiratory nitric oxide and nasal nitric oxide, 2005. Am. J. Respir. Crit. Care Med. 2005, 171, 912–930. [Google Scholar] [CrossRef]
- Dweik, R.A.; Boggs, P.B.; Erzurum, S.C.; Irvin, C.G.; Leigh, M.W.; Lundberg, J.O.; Olin, A.C.; Plummer, A.L.; Taylor, D.R. An official ATS clinical practice guideline: Interpretation of exhaled nitric oxide levels (FENO) for clinical applications. Am. J. Respir. Crit. Care Med. 2011, 184, 602–615. [Google Scholar] [CrossRef]
- Smith, K.R.; Bruce, N.; Balakrishnan, K.; Adair-Rohani, H.; Balmes, J.; Chafe, Z.; Dherani, M.; Hosgood, H.D.; Mehta, S.; Pope, D.; et al. Millions dead: How do we know and what does it mean? Methods used in the comparative risk assessment of household air pollution. Annu. Rev. Public Health 2014, 35, 185–206. [Google Scholar] [CrossRef]
- Sood, A.; Assad, N.A.; Barnes, P.J.; Churg, A.; Gordon, S.B.; Harrod, K.S.; Irshad, H.; Kurmi, O.P.; Martin, W.J., 2nd; Meek, P.; et al. ERS/ATS workshop report on respiratory health effects of household air pollution. Eur. Respir. J. 2018, 51, 1700698. [Google Scholar] [CrossRef]
- Cui, X.; Li, F.; Xiang, J.; Fang, L.; Chung, M.K.; Day, D.B.; Mo, J.; Weschler, C.J.; Gong, J.; He, L.; et al. Cardiopulmonary effects of overnight indoor air filtration in healthy non-smoking adults: A double-blind randomized crossover study. Environ. Int. 2018, 114, 27–36. [Google Scholar] [CrossRef]
- Pedroletti, C.; Millinger, E.; Dahlen, B.; Soderman, P.; Zetterstrom, O. Clinical effects of purified air administered to the breathing zone in allergic asthma: A double-blind randomized cross-over trial. Respir. Med. 2009, 103, 1313–1319. [Google Scholar] [CrossRef]
- Yoda, Y.; Takagi, H.; Wakamatsu, J.; Ito, T.; Nakatsubo, R.; Horie, Y.; Hiraki, T.; Shima, M. Stronger association between particulate air pollution and pulmonary function among healthy students in fall than in spring. Sci. Total Environ. 2019, 675, 483–489. [Google Scholar] [CrossRef]
- Pacitto, A.; Amato, F.; Moreno, T.; Pandolfi, M.; Fonseca, A.; Mazaheri, M.; Stabile, L.; Buonanno, G.; Querol, X. Effect of ventilation strategies and air purifiers on the children’s exposure to airborne particles and gaseous pollutants in school gyms. Sci. Total Environ. 2020, 712, 135673. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Male (n = 10) | Female (n = 22) | Total (n = 32) | |
|---|---|---|---|
| Age (years) | 41.8 ± 8.9 | 40.9 ± 6.9 | 41.2 ± 7.5 |
| Height (cm) | 169.0 ± 6.0 | 158.8 ± 4.3 | 162.0 ± 6.8 |
| Weight (kg) | 66.5 ± 13.3 | 53.3 ± 6.1 | 57.4 ± 10.7 |
| BMI (kg/m2) | 23.2 ± 3.9 | 21.2 ± 2.7 | 21.8 ± 3.2 |
| FVC (L) | 3.87 ± 0.44 | 2.94 ± 0.32 | 3.23 ± 0.56 |
| FEV1.0 (L) | 3.16 ± 0.35 | 2.43 ± 0.26 | 2.66 ± 0.45 |
| FEV1.0/ FVC (%) | 82.1 ± 7.04 | 82.8 ± 6.23 | 82.6 ± 6.39 |
| MMEF (L/s) | 3.31 ± 1.00 | 2.83 ± 0.83 | 2.98 ± 0.90 |
| PEF (L/s) | 8.19 ± 1.83 | 5.29 ± 0.99 | 6.20 ± 1.87 |
| 50/25 | 2.97 ± 0.87 | 3.59 ± 1.24 | 3.40 ± 1.16 |
| FeNO (ppb) * | 23.9 ± 2.1 | 10.8 ± 1.9 | 13.9 ± 2.2 |
| 1st Term | 2nd Term | Total | |||||||
|---|---|---|---|---|---|---|---|---|---|
| True Air Purifiers | Sham Air Purifiers | p Value | True Air Purifiers | Sham Air Purifiers | p Value | True Air Purifiers | Sham Air Purifiers | p Value | |
| Indoor | |||||||||
| PM2.5 (µg/m3) | 8.6 ± 3.8 | 9.7 ± 4.4 | 0.170 | 8.6 ± 5.9 | 9.7 ± 4.3 | 0.270 | 8.6 ± 5.0 | 9.7 ± 4.3 | 0.085 |
| PM10–2.5 (µg/m3) | 3.1 ± 2.1 | 3.4 ± 2.4 | 0.500 | 2.1 ± 1.3 | 2.3 ± 1.9 | 0.531 | 2.6 ± 1.8 | 2.8 ± 2.2 | 0.355 |
| O3 (ppb) | 1.6 ± 1.5 | 2.5 ± 2.0 | 0.002 | 2.8 ± 2.3 | 2.2 ± 1.4 | 0.079 | 2.2 ± 2.0 | 2.4 ± 1.7 | 0.446 |
| Temp (°C) | 18.7 ± 1.7 | 18.7 ± 2.4 | 0.984 | 16.6 ± 2.4 | 17.7 ± 2.3 | 0.020 | 17.7 ± 2.3 | 18.2 ± 2.4 | 0.088 |
| RH (%) | 53.1 ± 7.6 | 50.2 ± 8.4 | 0.048 | 47.0 ± 10.8 | 46.0 ± 9.0 | 0.554 | 50.1 ± 9.7 | 48.2 ± 8.9 | 0.109 |
| Outdoor | |||||||||
| PM2.5 (µg/m3) | 12.8 ± 5.0 | 12.9 ± 5.1 | 0.972 | 12.2 ± 1.8 | 12.1 ± 1.5 | 0.789 | 12.5 ± 3.8 | 12.5 ± 3.8 | 0.973 |
| PM10–2.5 (µg/m3) | 8.9 ± 7.6 | 9.1 ± 7.8 | 0.906 | 6.2 ± 1.8 | 6.1 ± 1.4 | 0.672 | 7.6 ± 5.6 | 7.6 ± 5.9 | 0.938 |
| O3 (ppb) | 20.9 ± 5.6 | 23.1 ± 6.5 | 0.045 | 29.3 ± 5.4 | 27.0 ± 5.7 | 0.025 | 25.1 ± 6.9 | 25.0 ± 6.4 | 0.892 |
| I/Oratio | |||||||||
| PM2.5 | 0.73 ± 0.28 | 0.84 ± 0.69 | 0.123 | 0.71 ± 0.47 | 0.78 ± 0.29 | 0.263 | 0.72 ± 0.38 | 0.81 ± 0.53 | 0.110 |
| PM10–2.5 | 0.51 ± 0.43 | 0.59 ± 1.00 | 0.262 | 0.36 ± 0.27 | 0.38 ± 0.34 | 0.074 | 0.43 ± 0.36 | 0.49 ± 0.76 | 0.182 |
| O3 | 0.08 ± 0.08 | 0.12 ± 0.11 | 0.470 | 0.11 ± 0.10 | 0.08 ± 0.06 | 0.071 | 0.09 ± 0.09 | 0.11 ± 0.09 | 0.052 |
| Percent Changes (95% CI) | p Value | |
|---|---|---|
| FVC (L) | 0.001 (−0.062, 0.065) | 0.966 |
| FEV1 (L) | −0.008 (−0.065, 0.050) | 0.797 |
| FEV1.0/ FVC (%) | −0.322 (−1.662, 1.018) | 0.637 |
| MMEF (L/s) | −0.071 (−0.219, 0.078) | 0.352 |
| PEF (L/s) | −0.135 (−0.490, 0.220) | 0.455 |
| 50/25 | 0.239 (−0.278, 0.756) | 0.362 |
| Log_FeNO | −0.001 (−0.097, 0.095) | 0.978 |
| Indoor PM2.5 | Indoor PM10–2.5 | Indoor O3 | ||||
|---|---|---|---|---|---|---|
| Percent Changes (95% CI) | p Value | Percent Changes (95% CI) | p Value | Percent Changes (95% CI) | p Value | |
| FVC (L) | 0.02 (0.00, 0.04) | 0.020 | 0.02 (0.00, 0.05) | 0.035 | −0.02 (−0.09, 0.05) | 0.660 |
| FEV1 (L) | 0.01 (−0.01, 0.03) | 0.315 | 0.01 (−0.01, 0.03) | 0.554 | −0.06 (−0.12, 0.00) | 0.058 |
| FEV1.0/FVC (%) | −0.35 (−0.77, 0.08) | 0.108 | −0.52 (−1.00, −0.05) | 0.030 | −1.41 (−2.88, 0.06) | 0.061 |
| MMEF (L/s) | −0.01 (−0.06, 0.04) | 0.723 | −0.02 (−0.08, 0.03) | 0.406 | −0.23 (−0.40, −0.07) | 0.005 |
| PEF (L/s) | 0.07 (−0.05, 0.19) | 0.228 | 0.10 (−0.03, 0.23) | 0.137 | −0.31 (−0.69, 0.08) | 0.117 |
| 50/25 | 0.13 (−0.10, 0.37) | 0.273 | 0.17 (−0.08, 0.42) | 0.174 | −0.31 (−0.80, 0.19) | 0.225 |
| Log_FeNO | 0.03 (−0.01, 0.06) | 0.123 | −0.01 (−0.04, 0.03) | 0.708 | −0.09 (−0.19, 0.01) | 0.083 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoda, Y.; Tamura, K.; Adachi, S.; Otani, N.; Nakayama, S.F.; Shima, M. Effects of the Use of Air Purifier on Indoor Environment and Respiratory System among Healthy Adults. Int. J. Environ. Res. Public Health 2020, 17, 3687. https://doi.org/10.3390/ijerph17103687
Yoda Y, Tamura K, Adachi S, Otani N, Nakayama SF, Shima M. Effects of the Use of Air Purifier on Indoor Environment and Respiratory System among Healthy Adults. International Journal of Environmental Research and Public Health. 2020; 17(10):3687. https://doi.org/10.3390/ijerph17103687
Chicago/Turabian StyleYoda, Yoshiko, Kenji Tamura, Sho Adachi, Naruhito Otani, Shoji F. Nakayama, and Masayuki Shima. 2020. "Effects of the Use of Air Purifier on Indoor Environment and Respiratory System among Healthy Adults" International Journal of Environmental Research and Public Health 17, no. 10: 3687. https://doi.org/10.3390/ijerph17103687
APA StyleYoda, Y., Tamura, K., Adachi, S., Otani, N., Nakayama, S. F., & Shima, M. (2020). Effects of the Use of Air Purifier on Indoor Environment and Respiratory System among Healthy Adults. International Journal of Environmental Research and Public Health, 17(10), 3687. https://doi.org/10.3390/ijerph17103687