A Possible Antioxidant Role for Vitamin D in Soccer Players: A Retrospective Analysis of Psychophysical Stress Markers in a Professional Team

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Cohort
2.2. Samples Collection
2.3. Clinical Data
2.4. Statistical Analysis
3. Results
3.1. Vitamin D
3.2. CK
3.3. Reactive Oxygen Species
3.4. T/C Ratio
3.5. Correlation between Psychophysical Markers
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Eigenschenk, B.; Thomann, A.; McClure, M.; Davies, L.; Gregory, M.; Dettweiler, U.; Inglés, E. Benefits of outdoor sports for society. A systematic literature review and reflections on evidence. Int. J. Environ. Res. Public Health 2019, 16, 937. [Google Scholar]
- Lavie, C.J.; O’Keefe, J.H.; Sallis, R.E. Exercise and the heart-the harm of too little and too much. Curr. Sports Med. Rep. 2015, 14, 104–109. [Google Scholar]
- Meeusen, R.; Duclos, M.; Foster, C.; Fry, A.; Gleeson, M.; Nieman, D.; Raglin, J.; Rietjens, G.; Steinacker, J.; Urhausen, A. Prevention, diagnosis, and treatment of the overtraining syndrome: Joint consensus statement of the european college of sport science and the American College of Sports Medicine. Med. Sci. Sports Exerc. 2013, 45, 186–205. [Google Scholar]
- Halson, S.L.; Jeukendrup, A.E. Does overtraining exist? An analysis of overreaching and overtraining research. Sports Med. 2004, 34, 967–981. [Google Scholar]
- Adlercreutz, H.; Harkonen, M.; Kuoppasalmi, K.; Näveri, H.; Huhtaniemi, I.; Tikkanen, H.; Remes, K.; Dessypris, A.; Karvonen, J. Effect of training on plasma anabolic and catabolic steroid hormones and their response during physical exercise. Int. J. Sports Med. 1986, 7, 27–28. [Google Scholar]
- Newsholme, E.A.; Parry-Billings, M.; McAndrew, N.; Budgett, R. A biochemical mechanism to explain some characteristics of overtraining. In Advances in Nutrition and Top Sport; Karger Publishers: Basel, Switzerland, 2015; pp. 79–93. [Google Scholar]
- Patel, D.R.; Yamasaki, A.; Brown, K. Epidemiology of sports-related musculoskeletal injuries in young athletes in United States. Transl. Pediatr. 2017, 6, 160–166. [Google Scholar]
- Mackay, D.F.; Russell, E.R.; Stewart, K.; MacLean, J.A.; Pell, J.P.; Stewart, W. Neurodegenerative disease mortality among former professional soccer players. N. Engl. J. Med. 2019, 381, 1801–1808. [Google Scholar] [PubMed]
- Pearce, N.; Gallo, V.; McElvenny, D. Head trauma in sport and neurodegenerative disease: An issue whose time has come? Neurobiol. Aging 2015, 36, 1383–1389. [Google Scholar] [PubMed]
- Blecher, R.; Elliott, M.A.; Yilmaz, E.; Dettori, J.R.; Oskouian, R.J.; Patel, A.; Clarke, A.; Hutton, M.; McGuire, R.; Dunn, R.; et al. Contact sports as a risk factor for amyotrophic lateral sclerosis: A systematic review. Glob. Spine J. 2019, 9, 104–118. [Google Scholar]
- Beghi, E.; Logroscino, G.; Chiò, A.; Hardiman, O.; Millul, A.; Mitchell, D.; Swingler, R.; Traynor, B.J. Amyotrophic lateral sclerosis, physical exercise, trauma and sports: Results of a population-based pilot case-control study. Amyotroph. Lateral Scler. 2012, 11, 289–292. [Google Scholar]
- Belli, S.; Vanacore, N. Proportionate mortality of Italian soccer players: Is amyotrophic lateral sclerosis an occupational disease? Eur. J. Epidemiol. 2005, 20, 237–242. [Google Scholar] [PubMed]
- Kuwahara, S.; Sato, Y. Retired American football players have a four times higher chance of getting Alzheimer disease or amyotrophic lateral sclerosis. Brain Nerve 2013, 65, 996–997. [Google Scholar] [PubMed]
- Pansarasa, O.; Bordoni, M.; Diamanti, L.; Sproviero, D.; Gagliardi, S.; Cereda, C. Sod1 in amyotrophic lateral sclerosis: “Ambivalent” behavior connected to the disease. Int. J. Mol. Sci. 2018, 19, 1345. [Google Scholar]
- McAlary, L.; Aquilina, J.A.; Yerbury, J.J. Susceptibility of mutant SOD1 to form a destabilized monomer predicts cellular aggregation and toxicity but not in vitro aggregation propensity. Front. Neurosci. 2016, 10, 499. [Google Scholar] [PubMed]
- Silva, J.R.; Rumpf, M.C.; Hertzog, M.; Castagna, C.; Farooq, A.; Girard, O.; Hader, K. Acute and residual soccer match-related fatigue: A systematic review and meta-analysis. Sports Med. 2018, 48, 539–583. [Google Scholar] [PubMed]
- Ascensão, A.; Rebelo, A.; Oliveira, E.; Marques, F.; Pereira, L.; Magalhães, J. Biochemical impact of a soccer match—Analysis of oxidative stress and muscle damage markers throughout recovery. Clin. Biochem. 2008, 41, 841–851. [Google Scholar]
- Fatouros, I.G.; Chatzinikolaou, A.; Douroudos, I.I.; Nikolaidis, M.G.; Kyparos, A.; Margonis, K.; Michailidis, Y.; Vantarakis, A.; Taxildaris, K.; Katrabasas, I.; et al. Time-course of changes in oxidative stress and antioxidant status responses following a soccer game. J. Strength Cond. Res. 2010, 24, 3278–3286. [Google Scholar]
- Romagnoli, M.; Sanchis-Gomar, F.; Alis, R.; Risso-Ballester, J.; Bosio, A.; Graziani, R.L.; Rampinini, E. Changes in muscle damage, inflammation, and fatigue-related parameters in young elite soccer players after a match. J. Sports Med. Phys. Fit. 2016, 56, 1198–1205. [Google Scholar]
- Trecroci, A.; Porcelli, S.; Perri, E.; Pedrali, M.; Rasica, L.; Alberti, G.; Longo, S.; Iaia, F.M. Effects of different training interventions on the recovery of physical and neuromuscular performance after a soccer match. J. Strength Cond. Res. 2019. [Google Scholar] [CrossRef]
- Dupont, G.; Nedelec, M.; McCall, A.; McCormack, D.; Berthoin, S.; Wisløff, U. Effect of 2 soccer matches in a week on physical performance and injury rate. Am. J. Sports Med. 2010, 38, 1752–1758. [Google Scholar]
- Ekstrand, J.; Waldén, M.; Hägglund, M. A congested football calendar and the wellbeing of players: Correlation between match exposure of European footballers before the World Cup 2002 and their injuries and performers during that World Cup. Br. J. Sports Med. 2004, 38, 493–497. [Google Scholar] [PubMed]
- Banfi, G.; Marinelli, M.; Roi, G.S.; Agape, V. Usefulness of free testosterone/cortisol ratio during a season of elite speed skating athletes. Int. J. Sports Med. 1993, 14, 373–379. [Google Scholar]
- Lombardi, G.; Vitale, J.A.; Logoluso, S.; Logoluso, G.; Cocco, N.; Cocco, G.; Cocco, A.; Banfi, G. Circannual rhythm of plasmatic vitamin D levels and the association with markers of psychophysical stress in a cohort of Italian professional soccer players. Chronobiol. Int. 2017, 34, 471–479. [Google Scholar] [PubMed]
- Vitale, J.A.; Lombardi, G.; Cavaleri, L.; Graziani, R.; Schoenhuber, H.; Torre, A.L.; Banfi, G. Rates of insufficiency and deficiency of vitamin D levels in elite professional male and female skiers: A chronobiologic approach. Chronobiol. Int. 2018, 35, 441–449. [Google Scholar] [PubMed]
- Kawamura, T.; Muraoka, I. Exercise-induced oxidative stress and the effects of antioxidant intake from a physiological viewpoint. Antioxidants 2018, 7, 119. [Google Scholar]
- Ferrari, D.; Lombardi, G.; Banfi, G. Concerning the vitamin D reference range: Pre-analytical and analytical variability of vitamin D measurement. Biochem. Med. 2017, 27, 453–466. [Google Scholar]
- Ferrari, D.; Ripa, M.; Premaschi, S.; Banfi, G.; Castagna, A.; Locatelli, M. LC-MS/MS method for simultaneous determination of linezolid, meropenem, piperacillin and teicoplanin in human plasma samples. J. Pharm. Biomed. Anal. 2019, 169, 11–18. [Google Scholar]
- Ferrari, D.; Strollo, M.; Vidali, M.; Motta, A.; Pontillo, M.; Locatelli, M. Biochemical, immunochemical and serology analytes validation of the lithium heparin BD Barricor blood collection tube on a highly automated Roche COBAS8000 instrument. Acta Biomed. 2020, 91, 47–55. [Google Scholar]
- Ferrari, D.; Lombardi, G.; Strollo, M.; Pontillo, M.; Motta, A.; Locatelli, M. Association between solar ultraviolet doses and vitamin D clinical routine data in European mid-latitude population between 2006 and 2018. Photochem. Photobiol. Sci. 2019, 18, 2696–2706. [Google Scholar]
- Banfi, G.; Dolci, A. Free testosterone/cortisol ratio in soccer: Usefulness of a categorization of values. J. Sports Med. Phys. Fit. 2006, 46, 611–616. [Google Scholar]
- Urhausen, A.; Gabriel, H.; Kindermann, W. Blood hormones as markers of training stress and overtraining. Sports Med. 1995, 20, 251–276. [Google Scholar] [PubMed]
- Aujla, R.; Patel, R. Creatine Phosphokinase; StatPearls Publishing: Treasure Island, FL, USA, 2019. [Google Scholar]
- Johnsen, S.H.; Lilleng, H.; Wilsgaard, T.; Bekkelund, S.I. Creatine kinase activity and blood pressure in a normal population: The Tromsø study. J. Hypertens. 2011, 29, 36–42. [Google Scholar] [PubMed]
- Brewster, L.M.; Mairuhu, G.; Sturk, A.; van Montfrans, G.A. Distribution of creatine kinase in the general population: Implications for statin therapy. Am. Heart J. 2007, 154, 655–661. [Google Scholar] [PubMed]
- Cooper, C.E.; Vollaard, N.B.; Choueiri, T.; Wilson, M.T. Exercise, free radicals and oxidative stress. Biochem. Soc. Trans. 2002, 30, 280–285. [Google Scholar]
- Venditti, P.; Di Meo, S. The role of reactive oxygen species in the life cycle of the mitochondrion. Int. J. Mol. Sci. 2020, 21, 2173. [Google Scholar]
- Beckhauser, T.F.; Francis-Oliveira, J.; De Pasquale, R. Reactive oxygen species: Physiological and physiopathological effects on synaptic plasticity. J. Exp. Neurosci. 2016, 2016, 23–48. [Google Scholar]
- Song, P.; Zou, M.H. Roles of reactive oxygen species in physiology and pathology. In Atherosclerosis: Risks, Mechanisms, and Therapies; Wiley-Blackwell: Hoboken, NJ, USA, 2015; ISBN 9781118828533. [Google Scholar]
- Ighodaro, O.M.; Akinloye, O.A. First line defence antioxidants-superoxide dismutase (SOD), catalase (CAT) and glutathione peroxidase (GPX): Their fundamental role in the entire antioxidant defence grid. Alex. J. Med. 2018, 54, 287–293. [Google Scholar]
- Rojo, A.I.; Salinas, M.; Martín, D.; Perona, R.; Cuadrado, A. Regulation of Cu/Zn-superoxide dismutase expression via the phosphatidylinositol 3 kinase/Akt pathway and nuclear factor-κB. J. Neurosci. 2004, 24, 7324–7334. [Google Scholar]
- Di Gregorio, S.E.; Duennwald, M.L. Yeast as a model to study protein misfolding in aged cells. FEMS Yeast Res. 2018, 18, foy054. [Google Scholar]
- Abrams, G.D.; Feldman, D.; Safran, M.R. Effects of Vitamin D on skeletal muscle and athletic performance. J. Am. Acad. Orthop. Surg. 2018, 26, 278–285. [Google Scholar]
- Zhang, L.; Quan, M.; Cao, Z.B. Effect of Vitamin D supplementation on upper and lower limb muscle strength and muscle power in athletes: A meta-analysis. PLoS ONE 2019, 14, e0215826. [Google Scholar]
- Seo, M.W.; Song, J.K.; Jung, H.C.; Kim, S.W.; Kim, J.H.; Lee, J.M. The associations of vitamin D status with athletic performance and blood-borne markers in adolescent athletes: A cross-sectional study. Int. J. Environ. Res. Public Health 2019, 16, 3422. [Google Scholar]
- Lanteri, P.; Lombardi, G.; Colombini, A.; Banfi, G. Vitamin D in exercise: Physiologic and analytical concerns. Clin. Chim. Acta 2013, 415, 45–53. [Google Scholar] [PubMed]
- Regione Lombardia Osservatorio Regionale per L’Integrazione e la Multietnicità. Available online: https://www.ismu.org/osservatorio-regionale-orim-pubblicazioni/ (accessed on 10 March 2020).
- Eskici, G. The importance of vitamins for soccer players. Int. J. Vitam. Nutr. Res. 2015, 85, 225–244. [Google Scholar]
- Tylavsky, F.A.; Cheng, S.; Lyytikä, A.; Viljakainen, H.; Lamberg-Allardt, C. Symposium: Optimizing Vitamin D intake for populations with special needs: Barriers to effective food fortification and supplementation. J. Nutr. 2006, 136, 1130–1134. [Google Scholar]
- Serrano, M.A.; Cañada, J.; Moreno, J.C.; Gurrea, G. Solar ultraviolet doses and vitamin D in a northern mid-latitude. Sci. Total Environ. 2017, 574, 744–750. [Google Scholar]
- Mokhtari, Z.; Hekmatdoost, Z.; Nourian, M. Antioxidant efficacy of vitamin D. J. Parathyr. Dis. 2017, 5, 11–16. [Google Scholar]



{kind=link}
{kind=link}
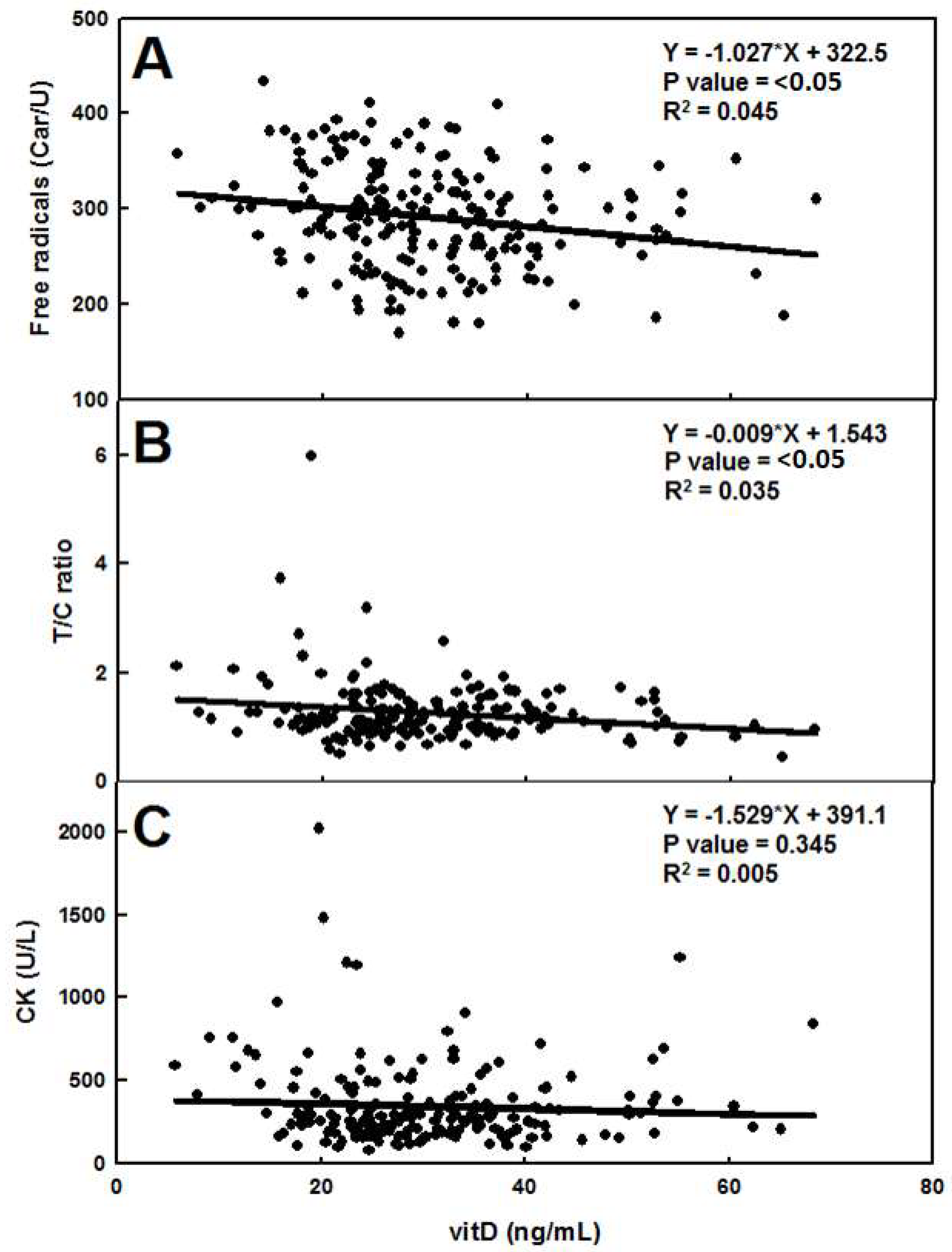
| Equation | R2 | P Value | Deviation from Horizontal | |
|---|---|---|---|---|
| VitD vs. ROS | −1.027*X + 322.5 | 0.045 | <0.05 | SIGNIFICANT |
| VitD vs. CK | −1.529*X + 391.1 | 0.005 | 0.345 | NOT SIGNIFICANT |
| VitD vs. T/C | −0.009*X + 1.543 | 0.035 | <0.05 | SIGNIFICANT |
| CK vs. ROS | 0.537*X + 187.6 | 0.013 | 0.107 | NOT SIGNIFICANT |
| CK vs. T/C | −0.000*X + 1.317 | 0.017 | 0.071 | NOT SIGNIFICANT |
| T/C vs. ROS | 0.000*X + 1.213 | 0.000 | 0.874 | NOT SIGNIFICANT |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferrari, D.; Lombardi, G.; Strollo, M.; Pontillo, M.; Motta, A.; Locatelli, M. A Possible Antioxidant Role for Vitamin D in Soccer Players: A Retrospective Analysis of Psychophysical Stress Markers in a Professional Team. Int. J. Environ. Res. Public Health 2020, 17, 3484. https://doi.org/10.3390/ijerph17103484
Ferrari D, Lombardi G, Strollo M, Pontillo M, Motta A, Locatelli M. A Possible Antioxidant Role for Vitamin D in Soccer Players: A Retrospective Analysis of Psychophysical Stress Markers in a Professional Team. International Journal of Environmental Research and Public Health. 2020; 17(10):3484. https://doi.org/10.3390/ijerph17103484
Chicago/Turabian StyleFerrari, Davide, Giovanni Lombardi, Marta Strollo, Marina Pontillo, Andrea Motta, and Massimo Locatelli. 2020. "A Possible Antioxidant Role for Vitamin D in Soccer Players: A Retrospective Analysis of Psychophysical Stress Markers in a Professional Team" International Journal of Environmental Research and Public Health 17, no. 10: 3484. https://doi.org/10.3390/ijerph17103484
APA StyleFerrari, D., Lombardi, G., Strollo, M., Pontillo, M., Motta, A., & Locatelli, M. (2020). A Possible Antioxidant Role for Vitamin D in Soccer Players: A Retrospective Analysis of Psychophysical Stress Markers in a Professional Team. International Journal of Environmental Research and Public Health, 17(10), 3484. https://doi.org/10.3390/ijerph17103484