View of Pakistani Residents toward Coronavirus Disease (COVID-19) during a Rapid Outbreak: A Rapid Online Survey

 ,
,
Abstract
1. Introduction
2. Methods
2.1. Study Design
2.2. Survey Instrument
2.3. Data Collection
2.4. Data Analysis
2.5. Ethical Approval
3. Results
3.1. Demographic Information
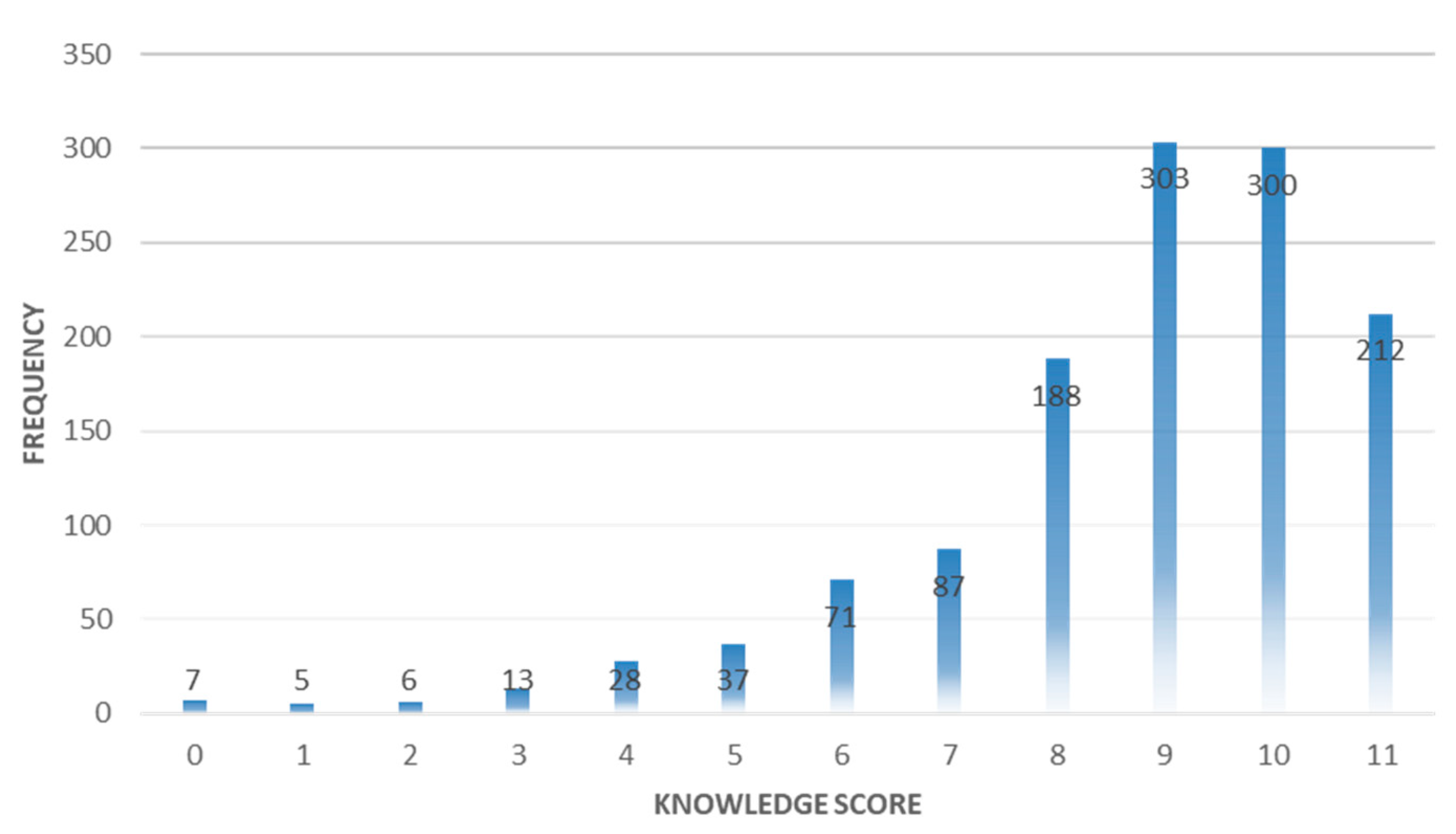
3.2. Knowledge of the Participants
3.3. Attitude of Participants
3.4. Practices of Participants
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- HuiDS, I.A.E.; Madani, T.A.; Ntoumi, F.; Kock, R.; Dar, O.; Ippolito, G.; McHugh, T.D.; Memish, Z.A.; Drosten, C.; Zumla, A.; et al. The continuing 2019-nCoV epidemic threat of novel coronaviruses to global health—The latest 2019 novel coronavirus outbreak in Wuhan, China. Int. J. Infect. Dis. 2020, 91, 264–266. [Google Scholar]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Deng, C.-X. The global battle against SARS-CoV-2 and COVID-19. Int. J. Biol. Sci. 2020, 16, 1676–1677. [Google Scholar] [CrossRef]
- WHO. Coronavirus Disease 2019 (COVID-19) Situation Report–93. 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports (accessed on 22 April 2020).
- Sohrabi, C.; Alsafi, Z.; O’Neill, N.; Khan, M.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, R. World Health Organization declares global emergency: A review of the 2019 novel coronavirus (COVID-19). Int. J. Surg. 2020, 76, 71–76. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Coronavirus Pandemic. 2020. Available online: https://www.worldometers.info/coronavirus/ (accessed on 22 April 2020).
- Lai, C.-C.; Wang, C.-Y.; Wang, Y.-H.; Hsueh, S.-C.; Ko, W.-C.; Hsueh, P.-R. Global epidemiology of coronavirus disease 2019 (COVID-19): Disease incidence, daily cumulative index, mortality, and their association with country healthcare resources and economic status. Int. J. Antimicrob. Agents 2020, 55, 105946. [Google Scholar] [CrossRef] [PubMed]
- Arshad Ali, S.; Baloch, M.; Ahmed, N.; Arshad Ali, A.; Iqbal, A. The outbreak of Coronavirus Disease 2019 (COVID-19)—An emerging global health threat. J. Infect. Public Health 2020, 13, 644–646. [Google Scholar] [CrossRef] [PubMed]
- Administrative Map of Pakistan (Islamic Republic of Pakistan). 2020. Available online: https://www.nationsonline.org/oneworld/map/pakistan-administrative-map.htm (accessed on 17 April 2020).
- Pakistan confirms First Two Cases of Coronavirus. 2020. Available online: https://www.france24.com/en/20200226-pakistan-confirms-first-two-cases-of-coronavirus (accessed on 17 April 2020).
- COVID-19. 2020. Available online: http://covid.gov.pk/ (accessed on 22 April 2020).
- Zarocostas, J. How to fight an infodemic. Lancet 2020, 395, 676. [Google Scholar] [CrossRef]
- Ajilore, K.; Atakiti, I.; Onyenankeya, K. College students’ knowledge, attitudes and adherence to public service announcements on Ebola in Nigeria: Suggestions for improving future Ebola prevention education programmes. Health Educ. J. 2017, 76, 648–660. [Google Scholar] [CrossRef]
- Tachfouti, N.; Slama, K.; Berraho, M.; Nejjari, C. The impact of knowledge and attitudes on adherence to tuberculosis treatment: A case-control study in a Moroccan region. Pan. Afr. Med. J. 2012, 12, 52. [Google Scholar]
- Bell, D.M. Public health interventions and SARS spread, 2003. Emerg Infect. Dis. 2004, 10, 1900. [Google Scholar] [CrossRef]
- Total Number of Active Social Media Users in Pakistan as of 2020. 2020. Available online: Phoneworld.com.pk/active-social-media-users-in-pakistan/ (accessed on 30 April 2020).
- Zhong, B.-L.; Luo, W.; Li, H.-M.; Zhang, Q.-Q.; Liu, X.-G.; Li, W.-T.; Li, Y. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: A quick online cross-sectional survey. Int. J. Biol. Sci. 2020, 16, 1745. [Google Scholar] [CrossRef] [PubMed]
- Harapan, H.; Itoh, N.; Yufika, A.; Winardi, W.S.; Te, H.; Megawati, D.; Hayati, Z.; Wagner, A.L.; Mudatsir, M. Coronavirus disease 2019 (COVID-19): A literature review. J. Infect. Public Health 2020, 13, 667–673. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Liu, S.-M.; Yu, X.-H.; Tang, S.-L.; Tang, C.-K. Coronavirus disease 2019 (COVID-19): Current status and future perspectives. Int. J. Antimicrob. Agents 2020, 105951. [Google Scholar] [CrossRef] [PubMed]
- Chang, L.; Yan, Y.; Wang, L. Coronavirus Disease 2019: Coronaviruses and Blood Safety. Transfus. Med. Rev. 2020. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, T.; Khan, M.; Haroon; Musa, T.H.; Nasir, S.; Hui, J.; Bonilla-Aldana, D.K.; Rodriguez-Morales, A.J. COVID-19: Zoonotic aspects. Travel. Med. Infect. Dis. 2020, 101607. [Google Scholar] [CrossRef]
- Santos, J.R.A. Cronbach’s alpha: A tool for assessing the reliability of scales. J. Ext. 1999, 37, 1–5. [Google Scholar]
- COVID-19: Pakistan Extends Lockdown until 30 April 2020. Available online: https://www.aa.com.tr/en/asia-pacific/covid-19-pakistan-extends-lockdown-until-april-30/1804544 (accessed on 17 April 2020).
- Pawlowski, B.; Atwal, R.; Dunbar, R. Sex differences in everyday risk-taking behavior in humans. Evol. Psychol. 2008, 6. [Google Scholar] [CrossRef]
- Cobey, K.D.; Laan, F.; Stulp, G.; Buunk, A.P.; Pollet, T.V. Sex differences in risk taking behavior among Dutch cyclists. Evol. Psychol. 2013, 11. [Google Scholar] [CrossRef]
- Coronavirus in Pakistan: Mask-buying Panic Leading to Shortages. 2020. Available online: https://www.aljazeera.com/news/2020/02/coronavirus-pakistan-panic-buying-masks-leading-shortages-200228095738523.html (accessed on 17 April 2020).
- WHO. Coronavirus Disease (COVID-19) Advice for the Public. 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public (accessed on 20 April 2020).
- Carlos, W.G.; Dela Cruz, C.S.; Cao, B.; Pasnick, S.; Jamil, S. Novel wuhan (2019-nCoV) coronavirus. Am. J. Respir. Crit. Care Med. 2020, 201, 7–8. [Google Scholar] [CrossRef]
- Savolainen-Kopra, C.; Korpela, T.; Simonen-Tikka, M.-L.; Amiryousefi, A.; Ziegler, T.; Roivainen, M.; Hovi, T. Single treatment with ethanol hand rub is ineffective against human rhinovirus—Hand washing with soap and water removes the virus efficiently. J. Med. Virol. 2012, 84, 543–547. [Google Scholar] [CrossRef]
- Levy, J.W.; Suntarattiwong, P.; Simmerman, J.M.; Jarman, R.G.; Johnson, K.; Olsen, S.J.; Chotpitayasunondh, T. Increased hand washing reduces influenza virus surface contamination in B angkok households, 2009–2010. Influenza Other Resp. 2014, 8, 13–16. [Google Scholar] [CrossRef] [PubMed]
- Broadband Subscribers Survey. Available online: https://www.pta.gov.pk/media/bb_sub_sur_report_10.pdf (accessed on 29 April 2020).


{kind=link}
| Province | Total Cases | Active Cases | Total Deaths | Total Recoveries |
|---|---|---|---|---|
| Azad Jammu and Kashmir | 51 | 28 | 0 | 23 |
| Balochistan | 495 | 322 | 6 | 167 |
| Gilgit-Baltistan | 290 | 89 | 3 | 198 |
| Islamabad | 194 | 165 | 3 | 26 |
| Khyber Pakhtunkhwa | 1345 | 930 | 80 | 335 |
| Punjab | 4328 | 3535 | 51 | 742 |
| Sindh | 3373 | 2639 | 69 | 665 |
| Total | 10,076 | 7708 | 212 | 2156 |
| Variable | Frequency (n) | Percentage (%) | Median (IQR) | p-Value |
|---|---|---|---|---|
| Gender | ||||
| Male | 557 | 44.3 | 1.0 (0.00) | <0.001 |
| Female | 700 | 55.7 | 1.0 (0.00) | |
| Age (years) | ||||
| 16–29 | 928 | 73.8 | 1.0 (0.00) | <0.001 |
| ≥30 | 329 | 26.2 | 1.0 (0.00) | |
| Marital status | ||||
| Single | 910 | 72.4 | 1.0 (0.00) | <0.001 |
| Married | 300 | 23.9 | 1.0 (0.00) | |
| Others ^ | 47 | 3.7 | 1.0 (1.00) | |
| Education | ||||
| Matriculation or below | 87 | 6.9 | 1.0 (0.00) | |
| Higher secondary school | 154 | 12.3 | 1.0 (0.00) | |
| Bachelor degree | 544 | 43.3 | 1.0 (0.00) | |
| Master degree | 472 | 37.5 | 1.0 (0.00) | <0.001 |
| Occupation | ||||
| Employed | 386 | 30.7 | 1.0 (0.00) | 0.011 |
| Unemployed | 180 | 14.3 | 1.0 (0.00) | |
| Student | 691 | 55.0 | 1.0 (0.00) | |
| Residence | ||||
| Punjab | 771 | 61.3 | 1.0 (0.00) | 0.033 |
| Sindh | 86 | 6.9 | 1.0 (0.00) | |
| KPK | 107 | 8.5 | 1.0 (0.00) | |
| Others ^^ | 293 | 23.3 | 1.0 (0.00) |
| Question | Yes | No | Unclear | Correct Rate |
|---|---|---|---|---|
| The main clinical symptoms of COVID-19 are fever, fatigue, and dry cough. | 1121 (89.2) | 104 (8.3) | 32 (2.5) | 1121 (89.2) |
| Unlike the common cold, stuffy nose, runny nose, and sneezing are less common in persons infected with the COVID-19 virus. | 841 (66.9) | 271 (21.6) | 145 (11.5) | 841 (66.9) |
| There currently is no effective cure for COVID-19, but early symptomatic and supportive treatment can help most patients recover from the infection. | 1126 (89.6) | 74 (5.9) | 57 (4.5) | 1126 (89.6) |
| Not all persons with COVID-19 will develop severe cases. Only those who are elderly, have chronic illnesses, and are obese are more likely to be severe cases. | 998 (79.4) | 166 (13.2) | 93 (7.4) | 998 (79.4) |
| Persons with COVID-19 cannot infect the virus to others when a fever is not present. | 380 (30.2) | 687 (54.7) | 190 (15.1) | 687 (54.7) |
| The COVID-19 virus spreads via respiratory droplets of infected individuals. | 1038 (82.6) | 219 (17.4) | 117 (9.3) | 1038 (82.6) |
| Ordinary residents can wear general medical masks to prevent the infection by the COVID-19 virus. | 1022 (81.3) | 172 (13.7) | 63 (5.0) | 1022 (81.3) |
| It is not necessary for children and young adults to take measures to prevent the infection by the COVID-19 virus. | 427 (34.0) | 749 (59.6) | 81 (6.4) | 749 (59.6) |
| To prevent the infection by COVID-19, individuals should avoid going to crowded places such as train stations and avoid taking public transportations. | 1118 (88.9) | 85 (6.8) | 54 (4.3) | 1118 (88.9) |
| Isolation and treatment of people who are infected with the COVID-19 virus are effective ways to reduce the spread of the virus. | 1125 (89.5) | 66 (5.3) | 66 (5.3) | 1125 (89.5) |
| People who have contact with someone infected with the COVID-19 virus should be immediately isolated in a proper place. In general, the observation period is 14 days. | 1126 (89.6) | 64 (5.1) | 67 (5.3) | 1126 (89.6) |
| Variables | Attitude Frequency (%) | ||||
|---|---|---|---|---|---|
| Controlling COVID-19 Successfully | Winning Confidence | ||||
| Variables | Agree | Disagree | Do not Know | Yes | No/Maybe |
| Gender | |||||
| Male | 418 (75.0) | 74 (13.3) | 65 (11.7) | 438 (78.6) | 119 (21.4) |
| Female | 512 (73.1) | 122 (17.4) | 66(9.4) | 530 (75.7) | 170 (24.3) |
| Age (years) | |||||
| 16–29 | 685 (73.8) | 142 (15.3) | 101 (10.9) | 727 (78.3) | 201 (21.7) |
| ≥30 | 245 (74.5) | 54 (16.4) | 30 (9.1) | 241 (73.3) | 88 (26.7) |
| Marital status | |||||
| Married | 217 (72.3) | 50 (16.7) | 33 (11.0) | 224 (74.7) | 76 (25.3) |
| Single | 677 (74.4) | 137 (15.1) | 96 (10.5) | 710 (78.0) | 200 (22.0) |
| Others ^ | 36 (76.6) | 9 (19.1) | 2 (4.3) | 34 (72.3) | 13 (27.7) |
| Education | |||||
| Matriculation or below | 66 (75.9) | 15 (17.2) | 6 (6.9) *** | 63 (72.4) | 24 (27.6) ** |
| Higher secondary school | 89 (57.8) | 38 (24.7) | 27 (17.5) | 100 (65.0) | 54 (35.0) |
| Bachelor degree | 397 (73.0) | 85 (15.7) | 62 (11.3) | 425 (78.1) | 119 (21.9) |
| Master degree | 378 (80.1) | 58 (12.3) | 36 (7.6) | 380 (80.5) | 92 (19.5) |
| Occupation | |||||
| Employed | 294 (76.2) | 57 (14.8) | 35 (6.4) | 301 (78.0) | 85 (22.0) |
| Unemployed | 126 (70.0) | 27 (15.0) | 27 (15.0) | 131 (72.8) | 49 (27.2) |
| Student | 510 (73.8) | 112 (16.2) | 69 (10.0) | 536 (77.6) | 155 (22.4) |
| Residence | |||||
| Punjab | 545 (70.8) | 140 (18.1) | 86 (11.1) * | 600 (77.8) | 171 (22.8) |
| Sindh | 65 (76.6) | 11 (12.8) | 10 (11.6) | 65 (75.6) | 21 (24.4) |
| KPK | 87 (81.3) | 11 (10.3) | 9 (8.4) | 86 (80.4) | 21 (19.6) |
| Others ^^ | 233 (79.5) | 34 (11.6) | 26 (8.9) | 217 (76.1) | 76 (25.9) |
| Variables | Practices n (%) | |||||
|---|---|---|---|---|---|---|
| Visit Crowdy Place | Wearing a Mask | Hand Washing | ||||
| Yes | No | Yes | No | Yes | No | |
| Gender | ||||||
| Male | 143 (25.7) | 414 (74.2) *** | 488 (87.6) | 69 (12.4) | 475 (85.3) | 82 (14.7) ** |
| Female | 82 (11.7) | 618 (88.3) | 591 (84.4) | 109 (15.6) | 632 (90.3) | 68 (9.7) |
| Age (years) | ||||||
| 16–29 | 121 (13.0) | 807 (87.0) *** | 800 (86.2) | 128 (13.8) | 816 (87.9) | 112 (12.1) |
| 30–49 | 104 (31.6) | 225 (68.4) | 279 (84.8) | 50 (15.2) | 291 (88.5) | 38 (11.5) |
| Marital status | ||||||
| Married | 61 (20.3) | 239 (79.7) *** | 261 (87.0) | 39 (13.0) | 271 (90.3) | 29 (9.7) |
| Single | 138 (15.2) | 772 (84.8) | 780 (85.7) | 130 (14.3) | 796 (87.5) | 114 (12.5) |
| Others ^ | 26 (55.3) | 21 (44.7) | 38 (80.9) | 9 (19.1) | 40 (85.1) | 7 (14.9) |
| Education | ||||||
| Matriculation or below | 42 (59.8) | 45 (51.7) *** | 75 (86.2) | 12 (13.8) *** | 78 (89.7) | 9 (10.3) *** |
| Higher secondary school | 42 (27.3) | 112 (72.7) | 112 (72.7) | 42 (27.3) | 114 (74.0) | 40 (26.0) |
| Bachelor degree | 80 (14.7) | 464 (85.3) | 480 (88.2) | 64 (11.8) | 486 (89.3) | 58 (10.7) |
| Master degree | 61 (12.9) | 411 (87.1) | 412 (87.3) | 60 (12.7) | 429 (90.9) | 43 (9.1) |
| Occupation | ||||||
| Employed | 91 (23.6) | 295 (76.4) ** | 331 (85.8) | 55 (14.2) | 345 (89.4) | 41 (10.6) |
| Unemployed | 30 (16.7) | 150 (83.3) | 158 (87.8) | 22 (12.2) | 163 (90.6) | 17 (9.4) |
| Student | 104 (15.1) | 587 (84.9) | 590 (85.4) | 101 (14.6) | 599 (86.7) | 92 (13.3) |
| Residence | ||||||
| Punjab | 63 (8.2) | 708 (91.8) *** | 647 (83.9) | 124 (16.1) * | 668 (86.6) | 103 (13.4) |
| Sindh | 26 (30.2) | 60 (69.8) | 73 (84.9) | 13 (15.1) | 76 (88.4) | 10 (11.6) |
| KPK | 27 (25.2) | 80 (74.8) | 94 (87.9) | 13 (12.1) | 97 (90.7) | 10 (9.3) |
| Others ^^ | 109 (37.2) | 184 (62.8) | 265 (90.4) | 28 (9.6) | 266 (90.8) | 27 (9.2) |
| Variable | OR (95% CI) | p-Value |
|---|---|---|
| Going to a crowded place | ||
| Gender (Male vs. female) | 0.384 (0.285–0.518) | <0.001 |
| Age group (16–29 vs. ≥30 years) | 3.083 (2.282–4.165) | <0.001 |
| Marital status (single vs. others ^) | 0.206 (0.109–0.391) | <0.001 |
| Marital status (married vs. others ^) | 0.144 (0.079–0.264) | <0.001 |
| Education (matriculation or below vs. master degree) | 6.289 (3.817–10.359) | <0.001 |
| Education (higher secondary school vs. master degree) | 2.527 (1.619–3.943) | <0.001 |
| Occupation (employed vs. students) | 1.741 (1.272–2.384) | 0.001 |
| Residence (Punjab vs. others ^) | 0.150 (0.106–0.213) | <0.001 |
| Residence (KPK vs. others ^) | 0.570 (0.347–0.936) | 0.026 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hayat, K.; Rosenthal, M.; Xu, S.; Arshed, M.; Li, P.; Zhai, P.; Desalegn, G.K.; Fang, Y. View of Pakistani Residents toward Coronavirus Disease (COVID-19) during a Rapid Outbreak: A Rapid Online Survey. Int. J. Environ. Res. Public Health 2020, 17, 3347. https://doi.org/10.3390/ijerph17103347
Hayat K, Rosenthal M, Xu S, Arshed M, Li P, Zhai P, Desalegn GK, Fang Y. View of Pakistani Residents toward Coronavirus Disease (COVID-19) during a Rapid Outbreak: A Rapid Online Survey. International Journal of Environmental Research and Public Health. 2020; 17(10):3347. https://doi.org/10.3390/ijerph17103347
Chicago/Turabian StyleHayat, Khezar, Meagen Rosenthal, Sen Xu, Muhammad Arshed, Pengchao Li, Panpan Zhai, Gebrehaweria Kassa Desalegn, and Yu Fang. 2020. "View of Pakistani Residents toward Coronavirus Disease (COVID-19) during a Rapid Outbreak: A Rapid Online Survey" International Journal of Environmental Research and Public Health 17, no. 10: 3347. https://doi.org/10.3390/ijerph17103347
APA StyleHayat, K., Rosenthal, M., Xu, S., Arshed, M., Li, P., Zhai, P., Desalegn, G. K., & Fang, Y. (2020). View of Pakistani Residents toward Coronavirus Disease (COVID-19) during a Rapid Outbreak: A Rapid Online Survey. International Journal of Environmental Research and Public Health, 17(10), 3347. https://doi.org/10.3390/ijerph17103347