Hygiene During Childbirth: An Observational Study to Understand Infection Risk in Healthcare Facilities in Kogi and Ebonyi States, Nigeria

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Setting
2.2. Study Sample
2.3. Data Collection
2.4. Data Analysis
2.5. Ethics
3. Results
3.1. Delivery Unit Conditions
3.2. Labour and Delivery Observations
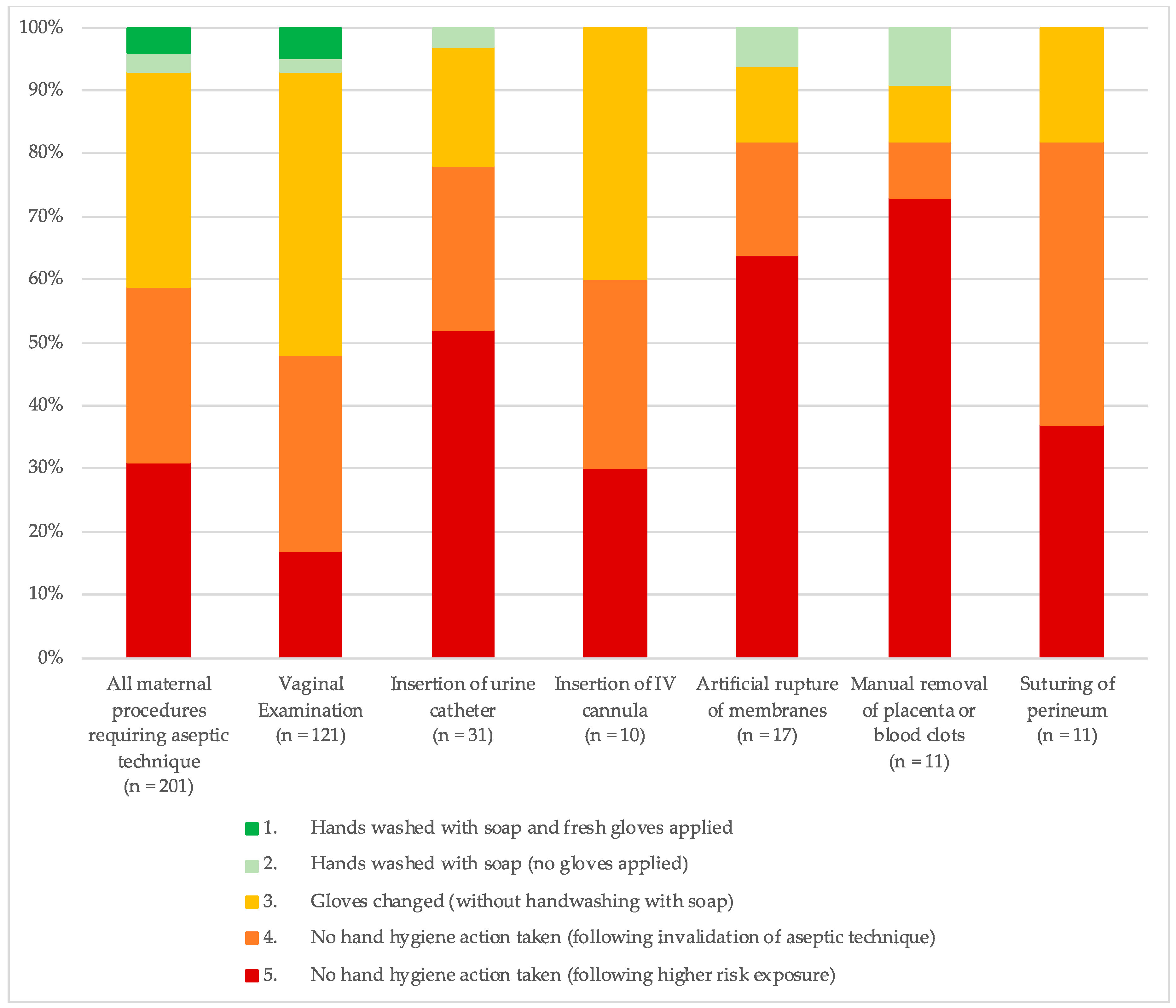
3.2.1. Hygiene Risk during Mother-Specific Procedures
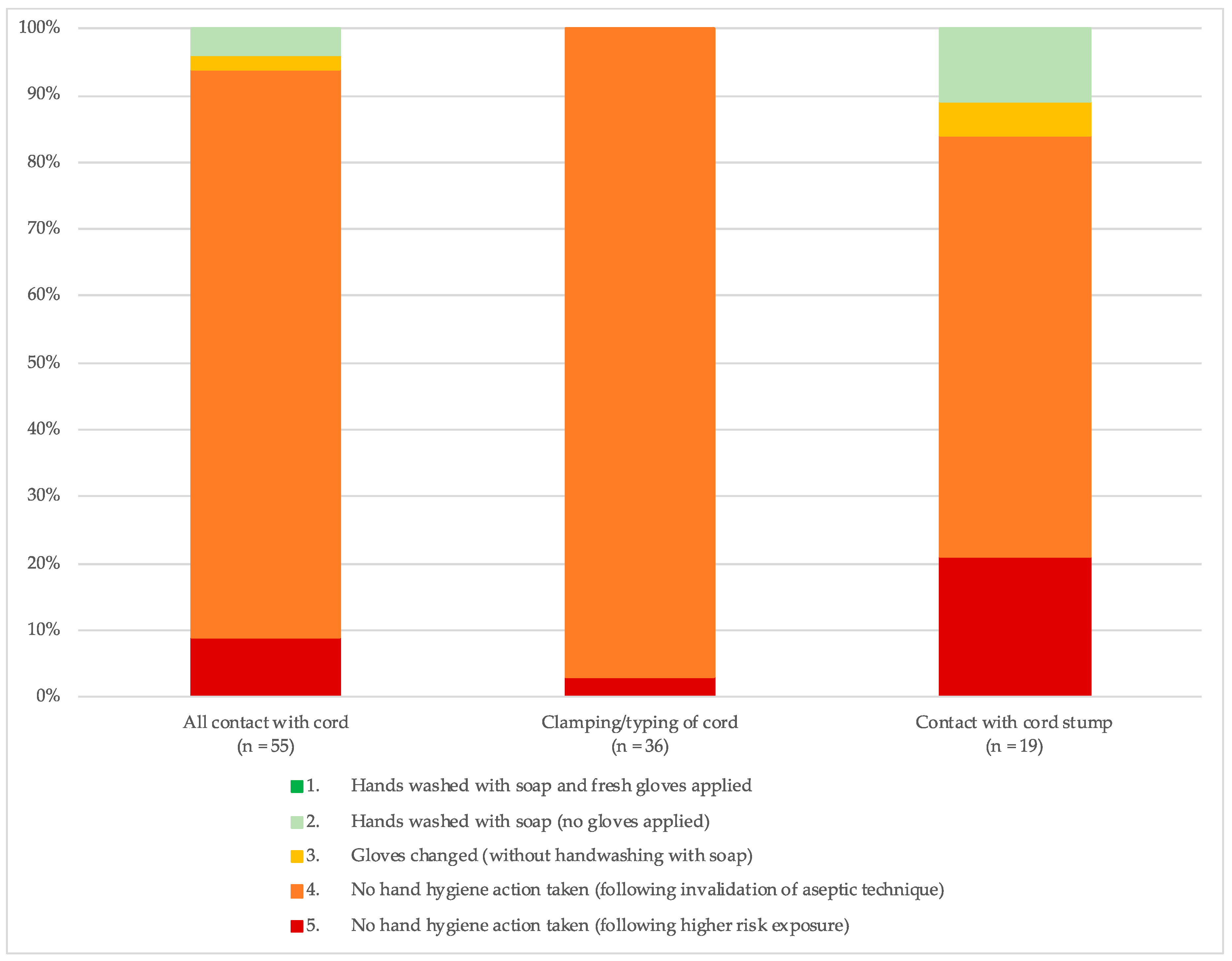
3.2.2. Hygiene Risk during Neonate-Specific Procedures
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- UN Inter-Agency Group for Child Mortality Estimation. Levels and Trend in Child Mortality; UN Inter-agency Group for Child Mortality Estimation: New York, NY, USA, 2017. [Google Scholar]
- Say, L.; Chou, D.; Gemmill, A.; Tunçalp, Ö.; Moller, A.-B.; Daniels, J.; Gülmezoglu, A.M.; Temmerman, M.; Alkema, L. Global causes of maternal death: A WHO systematic analysis. Lancet Glob. Health 2014, 2, e323–e333. [Google Scholar] [CrossRef]
- Bonet, M.; Pileggi, V.N.; Rijken, M.J.; Coomarasamy, A.; Lissauer, D.; Souza, J.P.; Gülmezoglu, A.M. Towards a consensus definition of maternal sepsis: Results of a systematic review and expert consultation. Reprod. Health 2017, 14, 67. [Google Scholar] [CrossRef]
- Simonsen, K.A.; Anderson-Berry, A.L.; Delair, S.F.; Davies, H.D. Early-onset neonatal sepsis. Clin. Microbiol. Rev. 2014, 27, 21–47. [Google Scholar] [CrossRef] [PubMed]
- Ganatra, H.A.; Stoll, B.J.; Zaidi, A.K. International Perspective on Early-Onset Neonatal Sepsis. Clin. Perinatol. 2010, 37, 501–523. [Google Scholar] [CrossRef] [PubMed]
- Blencowe, H.; Cousens, S.; Mullany, L.C.; Lee, A.C.; Kerber, K.; Wall, S.; Darmstadt, G.L.; Lawn, J.E. Clean birth and postnatal care practices to reduce neonatal deaths from sepsis and tetanus: A systematic review and Delphi estimation of mortality effect. BMC Public Health 2011, 11 (Suppl. 3), S11. [Google Scholar] [CrossRef]
- Delaney, M.M.; Maji, P.; Kalita, T.; Kara, N.; Rana, D.; Kumar, K.; Masoinneuve, J.; Cousens, S.; Gawande, A.A.; Kumar, V.; et al. Improving adherence to essential birth practices using the who safe childbirth checklist with peer coaching: experience from 60 public health facilities in Uttar Pradesh, India. Glob. Health Sci. Pract. 2017, 5, 217–231. [Google Scholar] [CrossRef]
- Kuzu, N.; Ozer, F.; Aydemir, S.; Zencir, M.; Yalçın, A.N. Compliance with hand hygiene and glove use in a university-affiliated hospital. Infect. Control Hosp. Epidemiol. 2005, 26, 312–315. [Google Scholar] [CrossRef] [PubMed]
- Pittet, D. Hand hygiene: Improved standards and practice for hospital care. Curr. Opin. Infect. Dis. 2003, 16, 327–335. [Google Scholar] [PubMed]
- Zingg, W.; Holmes, A.; Dettenkofer, M.; Goetting, T.; Secci, F.; Clack, L.; Allegranzi, B.; Magiorakos, A.-P.; Pittet, D. Hospital organisation, management, and structure for prevention of health-care-associated infection: A systematic review and expert consensus. Lancet Infect. Dis. 2015, 15, 212–224. [Google Scholar] [CrossRef]
- Mehta, R.; Mavalankar, D.V.; Ramani, K.; Sharma, S.; Hussein, J. Infection control in delivery care units, Gujarat state, India: A needs assessment. BMC Pregnancy Childbirth 2011, 11, 37. [Google Scholar] [CrossRef]
- Berhe, M.; Medhaniye, A.A.; Kahsay, G.; Birhane, E.; Abay, M. Essential neonatal care utilization and associated factors among mothers in public health facilities of Aksum Town, North Ethiopia, 2016. PLoS ONE 2017, 12, e0175902. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Guidelines on Hand Hygiene in Health Care; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Semrau, K.E.A.; Hirschhorn, L.R.; Delaney, M.M.; Singh, V.P.; Saurastri, R.; Sharma, N.; Tuller, D.E.; Firestone, R.; Lipsitz, S.; Dhingra-Kumar, N.; et al. Outcomes of a Coaching-Based WHO Safe Childbirth Checklist Program in India. N. Engl. J. Med. 2017, 377, 2313–2324. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization; United Nations Children’s Fund (UNICEF). WASH in Health Care Facilities: Global Baseline Report; UNICEF: Geneva, Switzerland, 2019. [Google Scholar]
- World Health Organization. Trends in Maternal Mortality: 1990 to 2015: Estimates by WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- United Nations. Sustainable Development Knowledge Platform. 2016. Available online: https://sustainabledevelopment.un.org/sdg3 (accessed on 3 September 2018).
- Liu, L.; Oza, S.; Hogan, D.; Chu, Y.; Perin, J.; Zhu, J.; Lawn, J.E.; Cousens, S.; Mathers, C.; Black, R.E. Global, regional, and national causes of under-5 mortality in 2000–2015: An updated systematic analysis with implications for the Sustainable Development Goals. Lancet 2016, 388, 3027–3035. [Google Scholar] [CrossRef]
- National Population Commission (NPC) [Nigeria] and ICF International. Nigeria Demographic and Health Survey 2013; NAI International, Ed.; NPC: Abuja, Nigeria; ICF International: Rockville, MD, USA, 2014. [Google Scholar]
- World Health Organization. Water and Sanitation for Health Facility Improvement Tool (WASH FIT); World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- The Soapbox Collaborative. WASH & CLEAN Toolkit; The Soapbox Collaborative: Aberdeen, Scotland, 2014. [Google Scholar]
- MCHIP. Quality of Antenatal and Delivery Care Services in Six Countries in Sub-Saharan Africa; MCHIP: Washington, DC, USA, 2013. [Google Scholar]
- Alex-Hart, B.A.; Opara, P.I. Handwashing Practices amongst Health Workers in a Teaching Hospital. Am. J. Infect. Dis. 2011, 7, 8–15. [Google Scholar] [CrossRef]
- World Health Organization. WHO Recommendation on Digital Vaginal Examination at Intervals of Four Hours for Routine Assessment of Active First Stage of Labour in Low-Risk Women; TWRH Library, Ed.; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Downe, S.; Gyte, G.M.; Dahlen, H.G.; Singata, M. Routine vaginal examinations for assessing progress of labour to improve outcomes for women and babies at term. Cochrane Database Syst. Rev. 2013, 15, Cd010088. [Google Scholar] [CrossRef]
- Benova, L.; Cumming, O.; Campbell, O.M.R. Systematic review and meta-analysis: Association between water and sanitation environment and maternal mortality. Trop. Med. Int. Health 2014, 19, 368–387. [Google Scholar] [CrossRef]
- Wood, W.; Neal, D.T. A new look at habits and the habit-goal interface. Psychol. Rev. 2007, 114, 843–863. [Google Scholar] [CrossRef] [PubMed]
- Michie, S.; Van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6, 42. [Google Scholar] [CrossRef]
- Curless, M.S.; Ruparelia, C.S.; Thompson, E.; Trexler, P.A. Infection Prevention and Control: Reference Manual for Health Care Facilities with Limited Resources; Jhpiego: Baltimore, MD, USA, 2018. [Google Scholar]
- World Health Organization; United Nations Children’s Fund (UNICEF). Managing Complications in Pregnancy and Childbirth: A Guide for Midwives and Doctors; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Ramasethu, J. Prevention and treatment of neonatal nosocomial infections. Matern. Health Neonatol. Perinatol. 2017, 3, 63. [Google Scholar] [CrossRef]
- Koff, M.D.; Loftus, R.W.; Burchman, C.C.; Schwartzman, J.D.; Read, M.E.; Henry, E.S.; Beach, M.L. Reduction in Intraoperative Bacterial Contamination of Peripheral Intravenous Tubing Through the Use of a Novel Device. J. Am. Soc. Anesthesiol. 2009, 110, 978–985. [Google Scholar] [CrossRef]
- Thomas, B.W.; Berg-Copas, G.M.; Vasquez, D.G.; Jackson, B.L.; Wetta-Hall, R. Conspicuous vs customary location of hand hygiene agent dispensers on alcohol-based hand hygiene product usage in an intensive care unit. J. Am. Osteopath. Assoc. 2009, 109, 263–267. [Google Scholar] [PubMed]
- Kampf, G.; Lemmen, S. Disinfection of gloved hands for multiple activities with indicated glove use on the same patient. J. Hosp. Infect. 2017, 97, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Ng, P.C.; Wong, H.; Lyon, D.; So, K.; Liu, F.; Lam, R.; Wong, E.; Cheng, A.; Fok, T. Combined use of alcohol hand rub and gloves reduces the incidence of late onset infection in very low birthweight infants. Arch. Dis. Child. Fetal Neonatal Ed. 2004, 89, F336–F340. [Google Scholar] [CrossRef] [PubMed]
- Gu, O.; Centre, F.M. Five Moments for Hand Hygiene: A Study of Compliance among Healthcare Workers in a Tertiary Hospital in South East Nigeria. Community Med. Public Health Care 2015, 2, 1–4. [Google Scholar] [CrossRef][Green Version]




{kind=link}
{kind=link}
{kind=link}
| Hygiene Category | Definition |
|---|---|
| 1 | Hands washed with soap and new gloves applied, no potential recontamination observed |
| 2 | Hands washed with soap, but no gloves are worn, no potential recontamination observed |
| 3 | Gloves are changed but HWWS is not observed, no potential recontamination observed |
| 4 | No hand hygiene actions taken following observed invalidation of aseptic technique (contact with intact skin of the woman/new born or surroundings) |
| 5 | No hand hygiene actions taken following observed potential recontamination from high risk exposure (contact with another patient, bodily fluids, mucous membranes, non-intact skin, clinical waste or faeces) |
| Hygiene Risk Category | Somers’ D Clustered by Actor; p-Value (Confidence Interval) | ||||
|---|---|---|---|---|---|
| n | Procedures Conducted in Category: Risky | Procedures Conducted in Category: Inadequate | Procedures Conducted in Category: Compliant | ||
| All events | 201 | 120 (60%) | 74 (37%) | 7(3%) | |
| Provider Type | |||||
| Nurse/Midwife | 142 | 84 (60%) | 52 (37%) | 6 (4%) | ref |
| Doctor | 58 | 35 (60%) | 22 (38%) | 1 (2%) | −0.02; p = 0.778 (−0.17 to 0.13) |
| Facility Type | |||||
| Primary | 87 | 53 (61%) | 30 (35%) | 4 (5%) | ref |
| Secondary | 61 | 35 (57%) | 24 (39%) | 2 (3%) | −0.01; p = 0.954 (−0.19 to 0.18) |
| Tertiary | 53 | 32 (60%) | 20 (38%) | 1 (2%) | −0.04; p = 0.752 (−0.25 to 0.18) |
| State | |||||
| Ebonyi | 119 | 73 (61%) | 41 (35%) | 5 (4%) | ref |
| Kogi | 82 | 47 (57%) | 33 (40%) | 2 (3%) | 0.32; p = 0.674 (−0.12 to 0.18) |
| Shift | |||||
| Morning | 79 | 37 (47%) | 38 (48%) | 4 (5%) | ref |
| Afternoon | 47 | 31 (66%) | 15 (32%) | 1 (2%) | 0.19; p = 0.034 (−0.37 to 0.02) |
| Night | 75 | 52 (69%) | 21(28%) | 2 (3%) | −0.23; p = 0.008 (−0.04 to −0.06) |
| Hygiene Risk Category | All Procedures Requiring Aseptic Technique | Mother-Specific Procedures Requiring Aseptic Technique | Neonate-Specific Procedures Requiring Aseptic Technique | |||
|---|---|---|---|---|---|---|
| N | % | N | % | N | % | |
| 1. Hands washed with soap and gloves changed | 7 | 3% | 7 | 4% | 0 | 0% |
| 2. Hands washed with soap (no gloves applied) | 7 | 3% | 5 | 2% | 2 | 1% |
| 3. Gloves changed (no handwashing with soap) | 70 | 27% | 68 | 34% | 2 | 4% |
| 4. No hand hygiene actions taken following observed invalidation of aseptic technique * | 104 | 41% | 57 | 28% | 47 | 85% |
| 5. No hand hygiene actions taken following higher risk exposure ** | 68 | 27% | 63 | 31% | 5 | 9% |
| Total | 256 | 201 | 55 | |||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buxton, H.; Flynn, E.; Oluyinka, O.; Cumming, O.; Esteves Mills, J.; Shiras, T.; Sara, S.; Dreibelbis, R. Hygiene During Childbirth: An Observational Study to Understand Infection Risk in Healthcare Facilities in Kogi and Ebonyi States, Nigeria. Int. J. Environ. Res. Public Health 2019, 16, 1301. https://doi.org/10.3390/ijerph16071301
Buxton H, Flynn E, Oluyinka O, Cumming O, Esteves Mills J, Shiras T, Sara S, Dreibelbis R. Hygiene During Childbirth: An Observational Study to Understand Infection Risk in Healthcare Facilities in Kogi and Ebonyi States, Nigeria. International Journal of Environmental Research and Public Health. 2019; 16(7):1301. https://doi.org/10.3390/ijerph16071301
Chicago/Turabian StyleBuxton, Helen, Erin Flynn, Olutunde Oluyinka, Oliver Cumming, Joanna Esteves Mills, Tess Shiras, Stephen Sara, and Robert Dreibelbis. 2019. "Hygiene During Childbirth: An Observational Study to Understand Infection Risk in Healthcare Facilities in Kogi and Ebonyi States, Nigeria" International Journal of Environmental Research and Public Health 16, no. 7: 1301. https://doi.org/10.3390/ijerph16071301
APA StyleBuxton, H., Flynn, E., Oluyinka, O., Cumming, O., Esteves Mills, J., Shiras, T., Sara, S., & Dreibelbis, R. (2019). Hygiene During Childbirth: An Observational Study to Understand Infection Risk in Healthcare Facilities in Kogi and Ebonyi States, Nigeria. International Journal of Environmental Research and Public Health, 16(7), 1301. https://doi.org/10.3390/ijerph16071301