Race-, Age-, and Anatomic Site-Specific Gender Differences in Cutaneous Melanoma Suggest Differential Mechanisms of Early- and Late-Onset Melanoma

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Population
2.3. Definition of Melanoma
2.4. Variables
2.5. Statistics
3. Results
3.1. Patient Characteristics and Differences in the Mean Age of Diagnosis
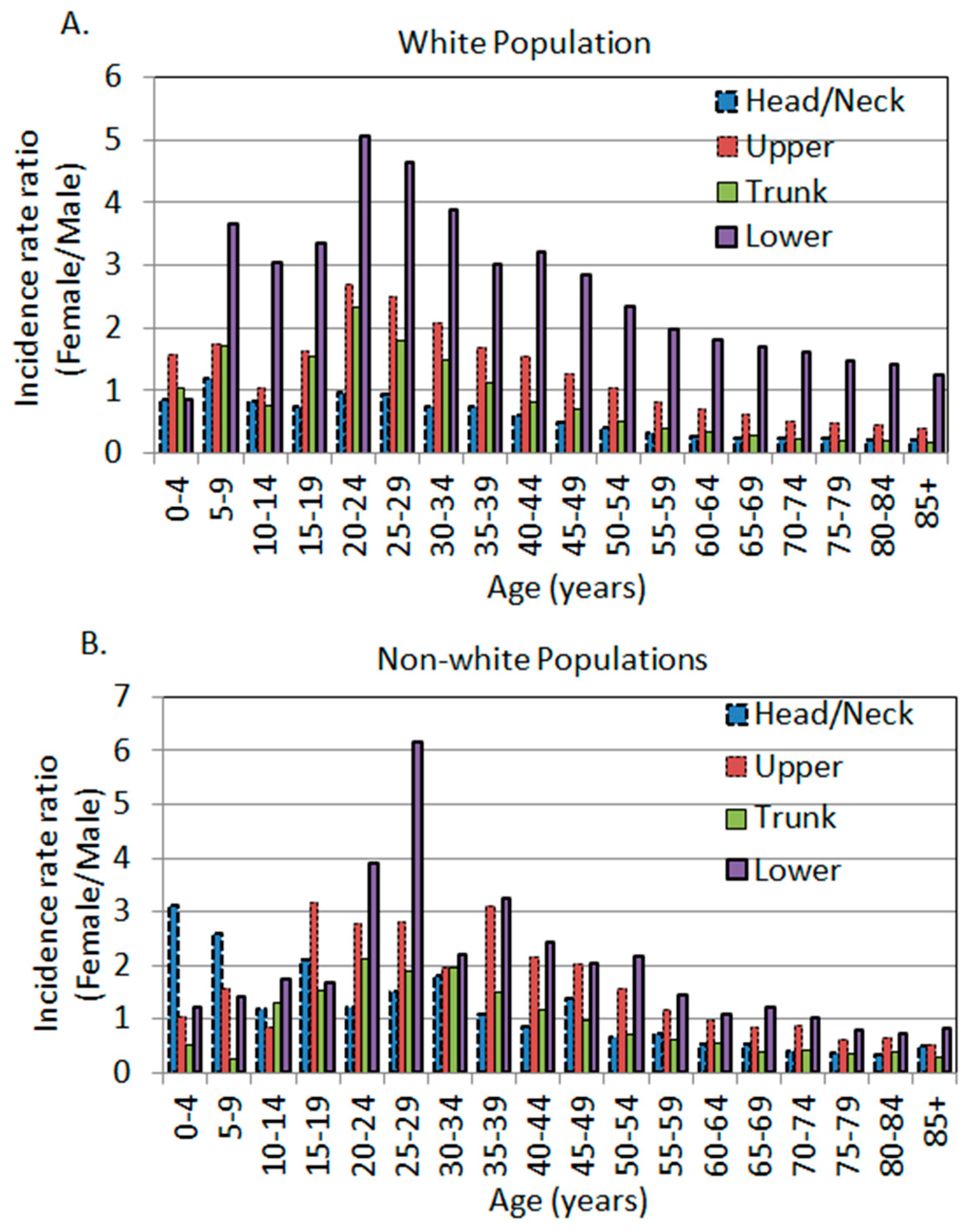
3.2. The Age-Specific Melanoma Incidence Rates in Each Body Site in the White Population
3.3. Sex Differences in Age- and Body Site-Specific Melanoma Incidence Rates in the Non-White Populations
3.4. The Age-Dependent Sex Differences Showed Younger Women and Older Men Were More Susceptible in Comparison to Their Opposite Sex of the Same Age
3.5. The Yearly Trend of Melanoma Incidence Rates in Each Body Site
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- CDC. Melanoma Incidence Rates and Death Rates by Race and Ethnicity: 1999–2012. 2018. Available online: http://www.cdc.gov/cancer/skin/statistics/race.htm (accessed on 2 October 2018).
- Cosman, B.; Heddle, S.B.; Crikelair, G.F. The increasing incidence of melanoma. Plast. Reconstr. Surg. 1976, 57, 50–56. [Google Scholar] [CrossRef] [PubMed]
- Bulliard, J.L.; Cox, B.; Elwood, J.M. Latitude gradients in melanoma incidence and mortality in the non-Maori population of New Zealand. Cancer Causes Control 1994, 5, 234–240. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; Bessonova, L.; Taylor, T.H.; Ziogas, A.; Meyskens, F.L., Jr.; Anton-Culver, H. A unique gender difference in early onset melanoma implies that in addition to ultraviolet light exposure other causative factors are important. Pigm. Cell Melanoma Res. 2013, 26, 128–135. [Google Scholar] [CrossRef] [PubMed]
- Liu-Smith, F.; Ziogas, A. An age-dependent interaction between sex and geographical UV index in melanoma risk. J. Am. Acad. Derm. 2017. [Google Scholar] [CrossRef]
- Elwood, J.M.; Lee, J.A. Recent data on the epidemiology of malignant melanoma. Semin. Oncol. 1975, 2, 149–154. [Google Scholar]
- Houghton, A.; Flannery, J.; Viola, M.V. Malignant melanoma in Connecticut and Denmark. Int. J. Cancer 1980, 25, 95–104. [Google Scholar] [CrossRef] [PubMed]
- Green, A.; MacLennan, R.; Youl, P.; Martin, N. Site distribution of cutaneous melanoma in Queensland. Int. J. Cancer 1993, 53, 232–236. [Google Scholar] [CrossRef]
- Elwood, J.M.; Gallagher, R.P. Body site distribution of cutaneous malignant melanoma in relationship to patterns of sun exposure. Int. J. Cancer 1998, 78, 276–280. [Google Scholar] [CrossRef]
- Chiarugi, A.; Quaglino, P.; Crocetti, E.; Nardini, P.; De Giorgi, V.; Borgognoni, L.; Brandani, P.; Gerlini, G.; Manganoni, A.M.; Bernengo, M.G.; et al. Melanoma density and relationship with the distribution of melanocytic naevi in an Italian population: A GIPMe study—The Italian multidisciplinary group on melanoma. Melanoma Res. 2015, 25, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Clark, L.N.; Shin, D.B.; Troxel, A.B.; Khan, S.; Sober, A.J.; Ming, M.E. Association between the anatomic distribution of melanoma and sex. J. Am. Acad. Dermatol. 2007, 56, 768–773. [Google Scholar] [CrossRef]
- Hemmings, D.E.; Johnson, S.; Tominaga, G.T.; Wong, J.H. Cutaneous melanoma in a multiethnic population—Is this a different disease? Arch. Surg. 2004, 139, 968–972. [Google Scholar] [CrossRef]
- Alexandrescu, D.T.; Maslin, B.; Kauffman, C.L.; Ichim, T.E.; Dasanu, C.A. Malignant Melanoma in Pigmented Skin: Does the Current Interventional Model Fit a Different Clinical, Histologic, and Molecular Entity? Dermatol. Surg. 2013, 39, 1291–1303. [Google Scholar] [CrossRef]
- Pinedo-Vega, J.L.; Castaneda-Lopez, R.; Davila-Rangel, J.I.; Mireles-Garcia, F.; Rios-Martinez, C.; Lopez-Saucedo, A. Skin cancer incidence in Zacatecas. Rev. Med. Inst. Mex. Seguro Soc. 2014, 52, 282–289. [Google Scholar]
- Pearl, D.K.; Scott, E.L. The anatomical distribution of skin cancers. Int. J. Epidemiol. 1986, 15, 502–506. [Google Scholar] [CrossRef]
- Bulliard, J.L.; De Weck, D.; Fisch, T.; Bordoni, A.; Levi, F. Detailed site distribution of melanoma and sunlight exposure: Aetiological patterns from a Swiss series. Ann. Oncol. 2007, 18, 789–794. [Google Scholar] [CrossRef]
- Lesage, C.; Barbe, C.; Le Clainche, A.; Lesage, F.X.; Bernard, P.; Grange, F. Sex-related location of head and neck melanoma strongly argues for a major role of sun exposure in cars and photoprotection by hair. J. Investig. Derm. 2013, 133, 1205–1211. [Google Scholar] [CrossRef]
- Liu-Smith, F.; Farhat, A.M.; Arce, A.; Ziogas, A.; Taylor, T.; Wang, Z.; Yourk, V.; Liu, J.; Wu, J.; McEligot, A.J.; et al. Sex differences in the association of cutaneous melanoma incidence rates and geographic ultraviolet light exposure. J. Am. Acad. Derm. 2017, 76, 499–505. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2015. CA Cancer J. Clin. 2015, 65, 5–29. [Google Scholar] [CrossRef]
- Coelho, S.G.; Hearing, V.J. UVA tanning is involved in the increased incidence of skin cancers in fair-skinned young women. Pigm. Cell Melanoma Res. 2010, 23, 57–63. [Google Scholar] [CrossRef]
- Franceschi, S.; Levi, F.; Randimbison, L.; LaVecchia, C. Site distribution of different types of skin cancer: New aetiological clues. Int. J. Cancer 1996, 67, 24–28. [Google Scholar] [CrossRef]
- Liu-Smith, F.; Jia, J.; Zheng, Y. UV-Induced Molecular Signaling Differences in Melanoma and Non-melanoma Skin Cancer. Adv. Exp. Med. Biol. 2017, 996, 27–40. [Google Scholar] [PubMed]
- Green, A. A theory of site distribution of melanomas: Queensland, Australia. Cancer Causes Control 1992, 3, 513–516. [Google Scholar] [CrossRef] [PubMed]
- Merrill, S.J.; Ashrafi, S.; Subramanian, M.; Godar, D.E. Exponentially increasing incidences of cutaneous malignant melanoma in Europe correlate with low personal annual UV doses and suggests 2 major risk factors. Dermatoendocrinology 2015, 7, e1004018. [Google Scholar] [CrossRef]
- Planta, M.B. Sunscreen and Melanoma: Is Our Prevention Message Correct? J. Am. Board Fam. Med. 2011, 24, 735–739. [Google Scholar] [CrossRef] [PubMed]
- Yuan, T.A.; Meyskens, F.; Liu-Smith, F. A cancer registry-based analysis on the non-white populations reveals a critical role of the female sex in early-onset melanoma. Cancer Cause Control 2018, 29, 405–415. [Google Scholar] [CrossRef]
- Rothman, K.J.; Greenland, S.; Lash, T.L. Modern Epidemiology; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2012. [Google Scholar]
- Kim, H.J.; Fay, M.P.; Feuer, E.J.; Midthune, D.N. Permutation tests for joinpoint regression with applications to cancer rates. Stat. Med. 2000, 19, 335–351. [Google Scholar] [CrossRef]
- Moan, J.; Dahlback, A. The Relationship between Skin Cancers, Solar-Radiation and Ozone Depletion. Br. J. Cancer 1992, 65, 916–921. [Google Scholar] [CrossRef]
- Lucas, R.M.; Norval, M.; Neale, R.E.; Young, A.R.; de Gruijl, F.R.; Takizawa, Y.; Van der Leun, J.C. The consequences for human health of stratospheric ozone depletion in association with other environmental factors. Photochem. Photobiol. Sci. 2015, 14, 53–87. [Google Scholar] [CrossRef] [PubMed]
- Noonan, F.P.; Dudek, J.; Merlino, G.; De Fabo, E.C. Animal models of melanoma: An HGF/SF transgenic mouse model may facilitate experimental access to UV initiating events. Pigm. Cell Res. 2003, 16, 16–25. [Google Scholar] [CrossRef]
- Godar, D.E.; Urbach, F.; Gasparro, F.P.; van der Leun, J.C. UV doses of young adults. Photochem. Photobiol. 2003, 77, 453–457. [Google Scholar] [CrossRef]
- Gloster, H.M.; Neal, K. Skin cancer in skin of color. J. Am. Acad. Derm. 2006, 55, 741–760, quiz 61–64. [Google Scholar] [CrossRef] [PubMed]
- Robles-Espinoza, C.D.; Roberts, N.D.; Chen, S.; Leacy, F.P.; Alexandrov, L.B.; Pornputtapong, N.; Halaban, R.; Krauthammer, M.; Cui, R.; Bishop, D.T.; et al. Germline MC1R status influences somatic mutation burden in melanoma. Nat. Commun. 2016, 7, 12064. [Google Scholar] [CrossRef]
- Nasti, T.H.; Timares, L. MC1R, Eumelanin and Pheomelanin: Their Role in Determining the Susceptibility to Skin Cancer. Photochem. Photobiol. 2015, 91, 188–200. [Google Scholar] [CrossRef] [PubMed]
- Wendt, J.; Mueller, C.; Rauscher, S.; Fae, I.; Fischer, G.; Okamoto, I. Contributions by MC1R Variants to Melanoma Risk in Males and Females. JAMA Derm. 2018, 154, 789–795. [Google Scholar] [CrossRef] [PubMed]
- Dellinger, R.W.; Liu-Smith, F.; Meyskens, F.L. Continuing to illuminate the mechanisms underlying UV-mediated melanomagenesis. J. Photochem. Photobiol. B 2014, 138, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; Fu, Y.; Meyskens, F.L. MiTF Regulates Cellular Response to Reactive Oxygen Species through Transcriptional Regulation of APE-1/Ref-1. J. Investig. Dermatol. 2009, 129, 422–431. [Google Scholar] [CrossRef]
- Liu, F.; Singh, A.; Yang, Z.; Garcia, A.; Kong, Y.; Meyskens, F.L. MiTF links Erk1/2 kinase and p21(CIP1/WAF1) activation after UVC radiation in normal human melanocytes and melanoma cells. Mol. Cancer 2010, 9, 214. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Artomov, M.; Goggins, W.; Daly, M.; Tsao, H. Gender Disparity and Mutation Burden in Metastatic Melanoma. JNCI J. Natl. Cancer Inst. 2015, 107. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Anatomic Site | Head/Neck | Upper | Trunk | Lower | All Sites | ||
|---|---|---|---|---|---|---|---|
| White | Number of cases (N, %) | Male | 42,496 (16.2%) | 36,560 (13.9%) | 59,779 (22.8%) | 13,831 (5.3%) | 152,666 (58.2%) |
| Female | 15,534 (5.9%) | 31,830 (12.1%) | 29,017 (11.1%) | 33,083 (12.6%) | 109,464 (41.8%) | ||
| Total | 58,030 (22.1%) | 68,390 (26.0%) | 88,796 (33.9%) | 46,914 (17.9%) | 262,130 (100%) | ||
| Mean age of diagnosis | Male | 70 | 67 | 65 | 62 | 63 | |
| Female | 66 | 62 | 57 | 59 | 57 | ||
| p-value | 0.03 * | 0.51 | 0.02 | 0.01 | 0.18 | ||
| Non-white | Number of cases (N, %) | Male | 1176 (10.4%) | 955 (8.5%) | 1572 (13.5%) | 1385 (12.3%) | 5088 (45.0%) |
| Female | 946 (8.4%) | 1441 (12.8%) | 1364 (12.1%) | 2456 (21.7%) | 6207 (55.0%) | ||
| Total | 2122 (18.8%) | 2396 (21.2%) | 2936 (26.0%) | 3841 (34.0%) | 11,295 (100%) | ||
| Mean age of diagnosis | Male | 63 | 57 | 59 | 60 | 59 | |
| Female | 57 | 50 | 53 | 55 | 54 | ||
| p-value | 0.34 | 0.24 | 0.33 | 0.08 | 0.69 | ||
| p-value (white vs. non-white, age of diagnosis) | Male | 0.0009 | 0.0002 | 0.0001 | <0.0001 | 0.0002 | |
| Female | 0.0008 | <0.0001 | <0.0001 | <0.0001 | <0.0001 | ||
| Head/Neck | Upper | Trunk | Lower | All Sites | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age | F | M | Ratio (95% CI) | F | M | Ratio (95% CI) | F | M | Ratio (95% CI) | F | M | Ratio (95% CI) | F | M | Ratio (95% CI) |
| 0–4 | 0.04 | 0.05 | 0.86 (0.43, 1.75) | 0.02 | 0.01 | 1.57 (0.44, 5.57) | 0 | 0 | NA | 0.03 | 0.03 | 0.87 (0.38, 2.02) | 0.09 | 0.10 | 0.96 (0.59, 1.55) |
| 5–9 | 0.05 | 0.04 | 1.20 (0.59, 2.46) | 0.06 | 0.03 | 1.75 (0.86, 3.58) | 0.05 | 0.03 | 1.72 (0.81, 3.64) | 0.08 | 0.02 | 3.67 (1.67, 8.06) | 0.25 | 0.13 | 1.91 (1.33, 2.75) |
| 10–14 | 0.11 | 0.13 | 0.83 (0.54, 1.27) | 0.08 | 0.08 | 1.05 (0.63, 1.76) | 0.10 | 0.13 | 0.75 (0.48, 1.18) | 0.14 | 0.05 | 3.03 (1.74, 5.26) | 0.43 | 0.39 | 1.12 (0.89, 1.41) |
| 15–19 | 0.28 | 0.38 | 0.74 (0.57, 0.96) | 0.34 | 0.21 | 1.63 (1.22, 2.17) | 0.84 | 0.55 | 1.53 (1.28, 1.84) | 0.54 | 0.16 | 3.34 (2.49, 4.48) | 2.00 | 1.30 | 1.54 (1.37, 1.74) |
| 20–24 | 0.70 | 0.73 | 0.96 (0.80, 1.14) | 1.29 | 0.48 | 2.69 (2.26, 3.21) ** | 2.71 | 1.16 | 2.33 (2.07, 2.61) | 1.89 | 0.37 | 5.05 (4.20, 6.07) | 6.59 | 2.75 | 2.40 (2.23, 2.58) |
| 25–29 | 1.14 | 1.22 | 0.93 (0.81, 1.07) | 2.31 | 0.92 | 2.50 (2.20, 2.85) | 4.44 | 2.46 | 1.81 (1.66, 1.96) | 3.45 | 0.75 | 4.63 (2.06, 5.29) | 11.33 | 5.35 | 2.12 (2.01, 2.24) |
| 30–34 | 1.26 | 1.67 | 0.75 (0.67, 0.85) | 3.40 | 1.65 | 2.07 (1.87, 2.28) | 5.57 | 3.78 | 1.48 (1.38, 1.58) | 4.98 | 1.28 | 3.87 (3.49, 4.29) | 15.20 | 8.37 | 1.82 (1.74, 1.90) |
| 35–39 | 1.54 | 2.09 | 0.74 (0.66, 0.83) | 4.27 | 2.53 | 1.69 (1.55, 1.83) | 6.48 | 5.77 | 1.12 (1.06, 1.19) | 6.30 | 2.08 | 3.02 (2.78, 3.28) | 18.60 | 12.48 | 1.49 (1.43, 1.55) |
| 40–44 | 1.81 | 3.01 | 0.60 (0.55, 0.66) | 5.86 | 3.81 | 1.54 (1.44, 1.64) | 7.13 | 8.72 | 0.82 (0.78, 0.86) | 8.10 | 2.52 | 3.21 (2.99, 3.46) | 22.90 | 18.06 | 1.27 (1.23, 1.31) |
| 45–49 | 2.23 | 4.51 | 0.49 (0.45, 0.54) | 7.54 | 6.02 | 1.25 (1.18, 1.32) | 8.52 | 12.41 | 0.69 (0.66, 0.72) | 9.50 | 3.34 | 2.84 (2.67, 3.03) | 27.78 | 26.29 | 1.06 (1.03, 1.09) |
| 50–54 | 2.83 | 6.94 | 0.41 (0.38, 0.44) | 9.17 | 8.85 | 1.04 (0.99, 1.09) | 9.06 | 17.61 | 0.51 (0.49, 0.54) | 10.25 | 4.36 | 2.35 (2.22, 2.50) | 31.32 | 37.76 | 0.83 (0.81, 0.85) |
| 55–59 | 3.54 | 11.13 | 0.32 (0.30, 0.34) | 10.72 | 13.03 | 0.82 (0.79, 0.86) | 9.39 | 24.11 | 0.39 (0.37, 0.41) | 10.65 | 5.34 | 1.99 (1.88, 2.12) | 34.29 | 53.62 | 0.64 (0.62, 0.66) |
| 60–65 | 4.72 | 17.85 | 0.26 (0.25, 0.28) | 12.94 | 18.50 | 0.70 (0.67, 0.73) | 10.06 | 30.79 | 0.33 (0.31, 0.34) | 11.62 | 6.40 | 1.81 (1.71, 1.93) | 39.34 | 73.54 | 0.53 (0.52, 0.55) |
| 65–69 | 7.03 | 27.78 | 0.25 (0.24, 0.27) | 15.29 | 24.72 | 0.62 (0.59, 0.65) | 10.69 | 39.82 | 0.27 (0.26, 0.28) | 13.11 | 7.70 | 1.70 (1.60, 1.81) | 46.12 | 100.02 | 0.46 (0.45, 0.47) |
| 70-74 | 9.56 | 39.87 | 0.24 (0.23, 0.25) | 16.17 | 32.14 | 0.50 (0.48, 0.53) | 10.40 | 44.49 | 0.23 (0.22, 0.25) | 13.69 | 8.47 | 1.62 (1.51, 1.73) | 49.82 | 124.99 | 0.40 (0.39, 0.41) |
| 75–79 | 12.08 | 52.09 | 0.23 (0.22, 0.24) | 18.13 | 37.71 | 0.48 (0.46, 0.51) | 10.23 | 49.77 | 0.21 (0.19, 0.22) | 14.55 | 9.95 | 1.46 (1.36, 1.57) | 54.98 | 149.52 | 0.37 (0.36, 0.38) |
| 80–84 | 15.11 | 69.56 | 0.22 (0.21, 0.23) | 18.62 | 42.05 | 0.44 (0.42, 0.47) | 9.43 | 50.44 | 0.19 (0.17, 0.20) | 14.64 | 10.38 | 1.41 (1.30, 1.53) | 57.80 | 172.44 | 0.34 (0.33, 0.35) |
| 85+ | 19.03 | 89.10 | 0.21 (0.20, 0.22) | 17.01 | 43.47 | 0.39 (0.37, 0.41) | 7.46 | 45.08 | 0.17 (0.15, 0.18) | 13.72 | 11.01 | 1.25 (1.14, 1.36) | 57.22 | 188.65 | 0.30 (0.29, 0.31) |
| All age * | 2.64 | 8.94 | 0.30 (0.27, 0.32) | 5.60 | 7.40 | 0.76 (0.71, 0.80) | 5.33 | 11.82 | 0.45 (0.43, 0.48) | 5.98 | 2.74 | 2.18 (2.02, 2.36) | 19.55 | 30.90 | 0.63 (0.61, 0.65) |
| Head/Neck | Upper | Trunk | Lower | All Sites | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age | F | M | Ratio (95% CI) | F | M | Ratio (95% CI) | F | M | Ratio (95% CI) | F | M | Ratio (95% CI) | F | M | Ratio (95% CI) |
| 0–4 | 0.012 | 0.004 | 3.12 (0.32, 30.0) | 0.012 | 0.011 | 1.04 (0.21, 5.16) | 0.004 | 0.007 | 0.52 (0.05, 5.74) | 0.027 | 0.022 | 1.21 (0.41, 3.61) | 0.054 | 0.045 | 1.21 (0.56, 2.62) |
| 5–9 | 0.020 | 0.008 | 2.60 (0.50, 13.4) | 0.012 | 0.008 | 1.56 (0.26, 9.32) | 0.004 | 0.015 | 0.26 (0.03, 2.32) | 0.044 | 0.030 | 1.43 (0.57, 3.55) | 0.079 | 0.061 | 1.30 (0.67, 2.51) |
| 10–14 | 0.031 | 0.026 | 1.19 (0.43, 3.28) | 0.016 | 0.019 | 0.83 (0.22, 3.10) | 0.02 | 0.015 | 1.30 (0.35, 4.84) | 0.059 | 0.034 | 1.73 (0.76, 3.96) | 0.126 | 0.094 | 1.33 (0.79, 2.25) |
| 15–19 | 0.040 | 0.019 | 2.12 (0.73, 6.21) | 0.036 | 0.011 | 3.18 (0.86, 11.8) | 0.064 | 0.042 | 1.54 (0.72, 3.33) | 0.076 | 0.046 | 1.68 (0.82, 3.46) | 0.217 | 0.118 | 1.85 (1.19, 2.88) |
| 20–24 | 0.073 | 0.060 | 1.22 (0.62, 2.38) | 0.146 | 0.053 | 2.78(1.50, 5.15) | 0.191 | 0.090 | 2.12 (1.29, 3.46) | 0.191 | 0.049 | 3.91 (2.11, 7.22) | 0.602 | 0.252 | 2.39 (1.79, 3.19) |
| 25–29 | 0.172 | 0.114 | 1.50 (0.94, 2.41) | 0.188 | 0.067 | 2.81 (1.61, 4.90) | 0.274 | 0.146 | 1.88 (1.26, 2.81) | 0.388 | 0.063 | 6.17 (3.63, 10.5) | 1.022 | 0.390 | 2.62 (2.08, 3.31) |
| 30–34 | 0.268 | 0.148 | 1.81 (1.21, 2.72) ** | 0.404 | 0.206 | 1.97 (1.40, 2.76) | 0.528 | 0.272 | 1.95 (1.45, 2.62) | 0.536 | 0.243 | 2.21 (1.62, 3.00) | 1.737 | 0.868 | 2.00 (1.70, 2.36) |
| 35–39 | 0.234 | 0.213 | 1.10 (0.75, 1.61) | 0.579 | 0.187 | 3.10 (2.20, 4.36) | 0.63 | 0.417 | 1.51 (1.17, 1.95) | 0.817 | 0.252 | 3.24 (2.42, 4.35) | 2.259 | 1.069 | 2.11 (1.82, 2.46) |
| 40–44 | 0.264 | 0.306 | 0.86 (0.61, 1.23) | 0.716 | 0.334 | 2.14 (1.62, 2.83) | 0.649 | 0.552 | 1.18 (0.92, 1.50) | 0.945 | 0.39 | 2.42 (1.88, 3.12) | 2.575 | 1.583 | 1.63 (1.42, 1.86) |
| 45–49 | 0.400 | 0.287 | 1.39 (0.99, 1.96) | 0.677 | 0.334 | 2.03 (1.51, 2.73) | 0.732 | 0.757 | 0.97 (0.77, 1.22) | 1.098 | 0.538 | 2.04 (1.62, 2.58) | 2.907 | 1.916 | 1.52 (1.33, 1.73) |
| 50–54 | 0.368 | 0.560 | 0.66 (0.48, 0.90) | 0.974 | 0.628 | 1.55 (1.21, 1.98) | 0.832 | 1.181 | 0.70 (0.57, 0.87) | 1.489 | 0.689 | 2.16 (1.73, 2.70) | 3.664 | 3.058 | 1.20 (1.07, 1.35) |
| 55–59 | 0.603 | 0.838 | 0.72 (0.54, 0.96) | 0.841 | 0.728 | 1.16 (0.75, 1.23) | 0.806 | 1.297 | 0.62 (0.49, 0.79) | 1.535 | 1.06 | 1.45 (1.17, 1.80) | 3.785 | 3.923 | 0.96 (0.85, 1.09) |
| 60–65 | 0.579 | 1.048 | 0.55 (0.40, 0.76) | 1.214 | 1.265 | 0.96 (0.75, 1.23) | 1.049 | 1.892 | 0.55 (0.44, 0.70) | 1.959 | 1.816 | 1.08 (0.88, 1.32) | 4.801 | 6.021 | 0.80 (0.71, 0.90) |
| 65–69 | 0.927 | 1.733 | 0.54 (0.40, 0.72) | 1.171 | 1.401 | 0.84 (0.63, 1.11) | 0.988 | 2.531 | 0.39 (0.30, 0.51) | 2.635 | 2.154 | 1.22 (0.99, 1.51) | 5.722 | 7.819 | 0.73 (0.65, 0.83) |
| 70–74 | 1.199 | 3.085 | 0.39 (0.29, 0.51) | 1.678 | 1.923 | 0.87 (0.66, 1.16) | 1.151 | 2.832 | 0.41 (0.31, 0.54) | 2.861 | 2.789 | 1.03 (0.82, 1.28) | 6.890 | 10.63 | 0.65 (0.57, 0.74) |
| 75–79 | 1.597 | 4.188 | 0.38 (0.29, 0.50) | 1.492 | 2.35 | 0.63 (0.46, 0.88) | 1.156 | 3.103 | 0.37 (0.27, 0.52) | 3.404 | 4.308 | 0.79 (0.63, 0.99) | 7.647 | 13.95 | 0.55 (0.48, 0.63) |
| 80–84 | 1.812 | 5.539 | 0.33 (0.24, 0.45) | 1.873 | 2.842 | 0.66 (0.46, 0.94) | 1.359 | 3.613 | 0.38 (0.26, 0.54) | 3.715 | 5.058 | 0.73 (0.57, 0.95) | 8.760 | 17.05 | 0.51 (0.44, 0.60) |
| 85+ | 3.279 | 6.564 | 0.50 (0.38, 0.66) | 1.689 | 3.25 | 0.52 (0.35, 0.77) | 0.96 | 3.445 | 0.28 (0.18, 0.44) | 4.372 | 5.20 | 0.84 (0.64, 1.11) | 10.30 | 18.46 | 0.56 (0.48, 0.66) |
| All age * | 0.383 | 0.676 | 0.57 (0.39, 0.82) | 0.553 | 0.49 | 1.13 (0.80, 1.58) | 0.504 | 0.763 | 0.66 (0.49, 0.90) | 0.964 | 0.74 | 1.30 (1.00, 1.70) | 2.403 | 2.669 | 0.90 (0.77, 1.05) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yuan, T.-A.; Lu, Y.; Edwards, K.; Jakowatz, J.; Meyskens, F.L.; Liu-Smith, F. Race-, Age-, and Anatomic Site-Specific Gender Differences in Cutaneous Melanoma Suggest Differential Mechanisms of Early- and Late-Onset Melanoma. Int. J. Environ. Res. Public Health 2019, 16, 908. https://doi.org/10.3390/ijerph16060908
Yuan T-A, Lu Y, Edwards K, Jakowatz J, Meyskens FL, Liu-Smith F. Race-, Age-, and Anatomic Site-Specific Gender Differences in Cutaneous Melanoma Suggest Differential Mechanisms of Early- and Late-Onset Melanoma. International Journal of Environmental Research and Public Health. 2019; 16(6):908. https://doi.org/10.3390/ijerph16060908
Chicago/Turabian StyleYuan, Tze-An, Yunxia Lu, Karen Edwards, James Jakowatz, Frank L. Meyskens, and Feng Liu-Smith. 2019. "Race-, Age-, and Anatomic Site-Specific Gender Differences in Cutaneous Melanoma Suggest Differential Mechanisms of Early- and Late-Onset Melanoma" International Journal of Environmental Research and Public Health 16, no. 6: 908. https://doi.org/10.3390/ijerph16060908
APA StyleYuan, T.-A., Lu, Y., Edwards, K., Jakowatz, J., Meyskens, F. L., & Liu-Smith, F. (2019). Race-, Age-, and Anatomic Site-Specific Gender Differences in Cutaneous Melanoma Suggest Differential Mechanisms of Early- and Late-Onset Melanoma. International Journal of Environmental Research and Public Health, 16(6), 908. https://doi.org/10.3390/ijerph16060908