Effectiveness Studies in Health Promotion: A Review of the Methodological Quality of Studies Reporting Significant Effects on Physical Activity in Working Age Adults

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy and Data Source
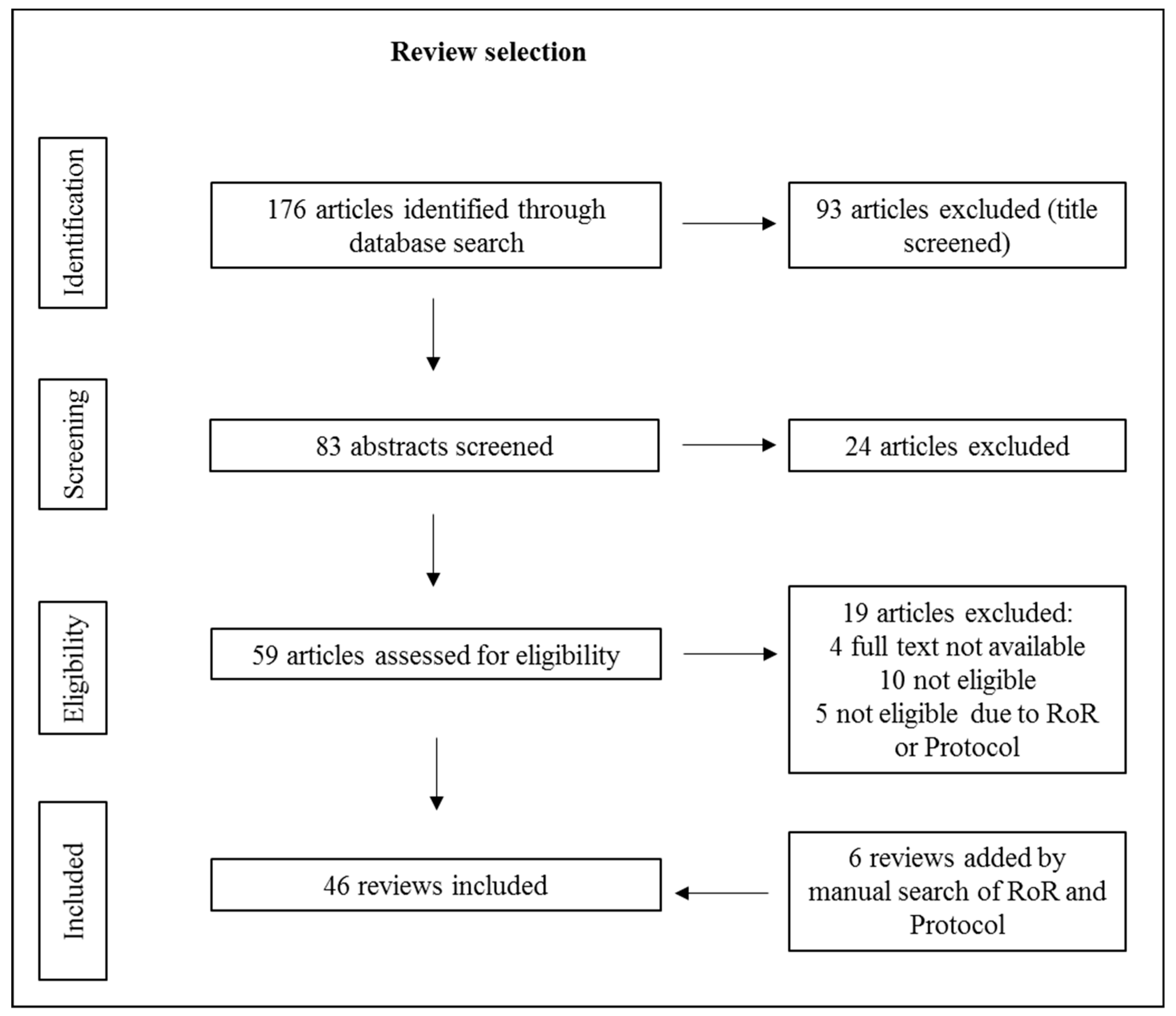
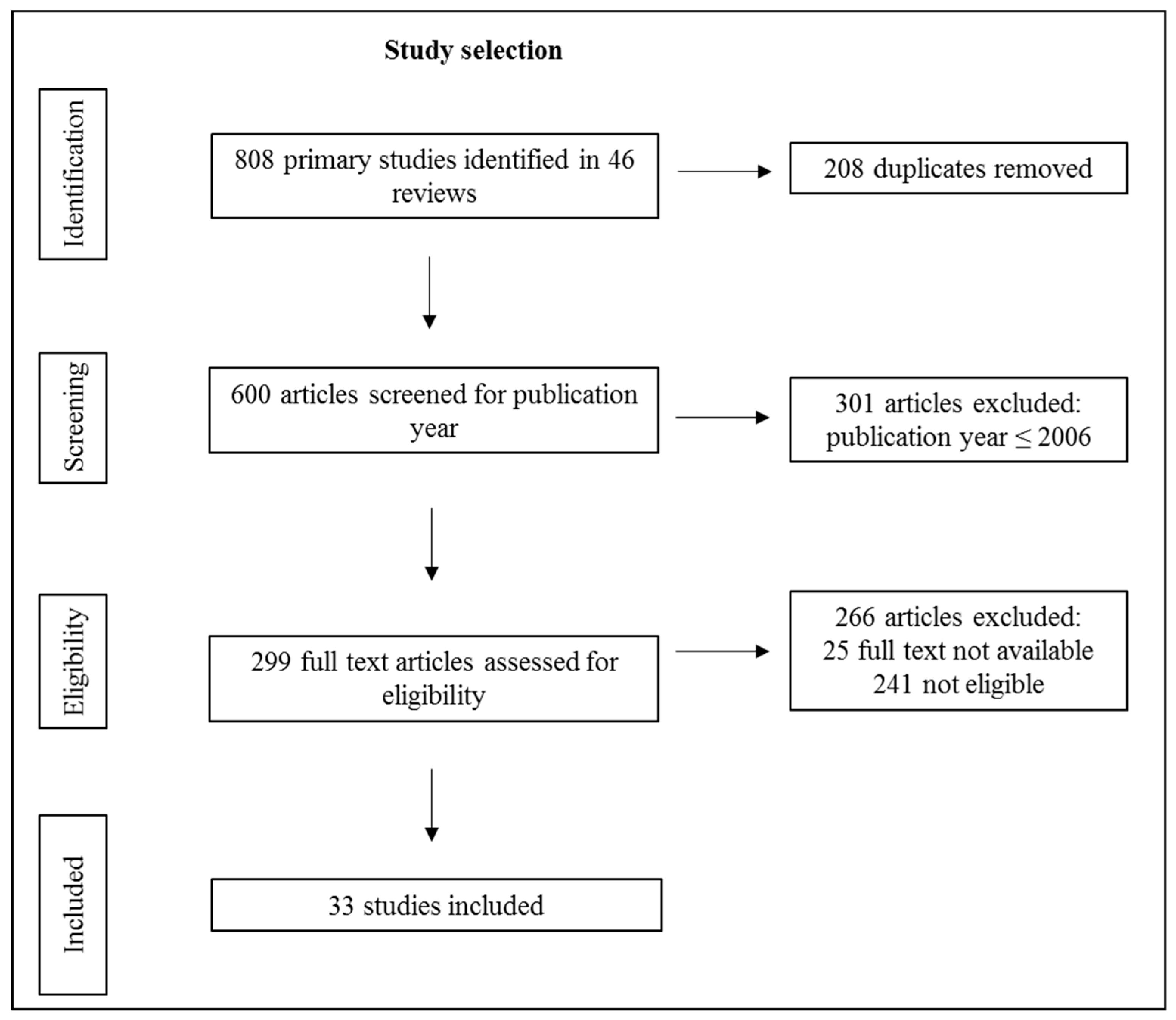
2.2. Study Selection
2.3. Data Collection
- Study design;
- Control group (CG) condition (intervention CG (we define an intervention CG as a group that receives any form of intervention, including usual care and placebos, and is called a CG by the authors of the primary study), non-intervention CG (we define a non-intervention CG as a group which is instructed to continue their lifestyle.) or no CG);
- Sample size (number of participants analyzed in primary outcome results);
- Operationalization of PA (subjective and/or objective measurements, observed time frame);
- Reporting of sample size calculation and achievement of desired number of cases (yes/no);
- Reporting of intention-to-treat (ITT) analyses (we define ITT analyses as analyses of study participants according to the original group allocation, regardless of non-compliance or inconsistency with the study protocol. We did not differentiate between the different methods of handling missing outcome data [22]) (yes/no);
- Checking for baseline group differences (yes/no);
- Reporting of drop-out analyses (yes/no);
- Reporting of standardized effect sizes of the results (e.g., Cohen’s d);
- Follow-up measurements (after the measurement at the end of the intervention).
3. Results
4. Discussion
Study Limitations and Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Action Plan for the Prevention and Control of Noncommunicable Diseases 2013–2020; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Beighle, A.; Morrow, J.R. Promoting Physical Activity: Addressing Barriers and Moving Forward. J. Phys. Educ. Recreat. Danc. 2014, 85, 23–26. [Google Scholar] [CrossRef]
- Forberger, S.; Bammann, K.; Bauer, J.; Boll, S.; Bolte, G.; Brand, T.; Hein, A.; Koppelin, F.; Lippke, S.; Meyer, J.; et al. How to Tackle Key Challenges in the Promotion of Physical Activity among Older Adults (65+): The AEQUIPA Network Approach. Int. J. Environ. Res. Public Health 2017, 14, 379. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Action Plan on Physical Activity 2018–2030: More Active People for a Healthier World; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Greaves, C.J.; Sheppard, K.E.; Abraham, C.; Hardeman, W.; Roden, M.; Evans, P.H.; Schwarz, P. Systematic review of reviews of intervention components associated with increased effectiveness in dietary and physical activity interventions. BMC Public Health 2011, 11, 119. [Google Scholar] [CrossRef] [PubMed]
- Sanchez, A.; Bully, P.; Martinez, C.; Grandes, G. Effectiveness of physical activity promotion interventions in primary care: A review of reviews. Prev. Med. 2015, 76, S56–S67. [Google Scholar] [CrossRef] [PubMed]
- Heath, G.W.; Parra, D.C.; Sarmiento, O.L.; Andersen, L.B.; Owen, N.; Goenka, S.; Montes, F.; Brownson, R.C. Evidence-based intervention in physical activity: Lessons from around the world. Lancet 2012, 380, 272–281. [Google Scholar] [CrossRef]
- Müller-Riemenschneider, F.; Reinhold, T.; Nocon, M.; Willich, S.N. Long-term effectiveness of interventions promoting physical activity: A systematic review. Prev. Med. 2008, 47, 354–368. [Google Scholar] [CrossRef] [PubMed]
- Malik, S.H.; Blake, H.; Suggs, L.S. A systematic review of workplace health promotion interventions for increasing physical activity. Br. J. Health Psychol. 2014, 19, 149–180. [Google Scholar] [CrossRef] [PubMed]
- Zubala, A.; MacGillivray, S.; Frost, H.; Kroll, T.; Skelton, D.A.; Gavine, A.; Gray, N.M.; Toma, M.; Morris, J. Promotion of physical activity interventions for community dwelling older adults: A systematic review of reviews. PLoS ONE 2017, 12, e0180902. [Google Scholar] [CrossRef] [PubMed]
- Evidence-Based Medicine Working Group. Evidence-based medicine. A new approach to teaching the practice of medicine. JAMA 1992, 268, 2420–2425. [Google Scholar] [CrossRef]
- Sackett, D.L.; Rosenberg, W.M.; Gray, J.A.; Haynes, R.B.; Richardson, W.S. Evidence based medicine: What it is and what it isn’t. BMJ 1996, 312, 71–72. [Google Scholar] [CrossRef]
- Kabisch, M.; Ruckes, C.; Seibert-Grafe, M.; Blettner, M. Randomized controlled trials: Part 17 of a series on evaluation of scientific publications. Dtsch. Arztebl. Int. 2011, 108, 663–668. [Google Scholar] [PubMed]
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. BMJ 2010, 340, c332. [Google Scholar] [CrossRef] [PubMed]
- Manchikanti, L.; Hirsch, J.A.; Smith, H.S. Evidence-based medicine, systematic reviews, and guidelines in interventional pain management: Part 2: Randomized controlled trials. Pain Physician 2008, 11, 717–773. [Google Scholar] [PubMed]
- Rosen, L.; Manor, O.; Engelhard, D.; Zucker, D. In defense of the randomized controlled trial for health promotion research. Am. J. Public Health 2006, 96, 1181–1186. [Google Scholar] [CrossRef] [PubMed]
- Duyx, B.; Urlings, M.J.E.; Swaen, G.M.H.; Bouter, L.M.; Zeegers, M.P. Scientific citations favor positive results: A systematic review and meta-analysis. J. Clin. Epidemiol. 2017, 88, 92–101. [Google Scholar] [CrossRef] [PubMed]
- Jannot, A.-S.; Agoritsas, T.; Gayet-Ageron, A.; Perneger, T.V. Citation bias favoring statistically significant studies was present in medical research. J. Clin. Epidemiol. 2013, 66, 296–301. [Google Scholar] [CrossRef] [PubMed]
- Baxter, S.; Sanderson, K.; Venn, A.J.; Blizzard, C.L.; Palmer, A.J. The relationship between return on investment and quality of study methodology in workplace health promotion programs. Am. J. Health Promot. AJHP 2014, 28, 347–363. [Google Scholar] [CrossRef] [PubMed]
- Verweij, L.M.; Coffeng, J.; van Mechelen, W.; Proper, K.I. Meta-analyses of workplace physical activity and dietary behaviour interventions on weight outcomes. Obes. Rev. 2011, 12, 406–429. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Alshurafa, M.; Briel, M.; Akl, E.A.; Haines, T.; Moayyedi, P.; Gentles, S.J.; Rios, L.; Tran, C.; Bhatnagar, N.; Lamontagne, F.; et al. Inconsistent definitions for intention-to-treat in relation to missing outcome data: Systematic review of the methods literature. PLoS ONE 2012, 7, e49163. [Google Scholar] [CrossRef] [PubMed]
- Verhagen, A.P.; de Vet, H.C.W.; de Bie, R.A.; Kessels, A.G.H.; Boers, M.; Bouter, L.M.; Knipschild, P.G. The Delphi List. J. Clin. Epidemiol. 1998, 51, 1235–1241. [Google Scholar] [CrossRef]
- Carter, T.; Morres, I.D.; Meade, O.; Callaghan, P. The Effect of Exercise on Depressive Symptoms in Adolescents: A Systematic Review and Meta-Analysis. J. Am. Acad. Child Adolesc. Psychiatry 2016, 55, 580–590. [Google Scholar] [CrossRef] [PubMed]
- Gerritsen, J.K.W.; Vincent, A.J.P.E. Exercise improves quality of life in patients with cancer: A systematic review and meta-analysis of randomised controlled trials. Br. J. Sports Med. 2016, 50, 796–803. [Google Scholar] [CrossRef] [PubMed]
- Olivo, S.A.; Macedo, L.G.; Gadotti, I.C.; Fuentes, J.; Stanton, T.; Magee, D.J. Scales to assess the quality of randomized controlled trials: A systematic review. Phys. Ther. 2008, 88, 156–175. [Google Scholar] [CrossRef] [PubMed]
- Allen, N.A.; Fain, J.A.; Braun, B.; Chipkin, S.R. Continuous glucose monitoring counseling improves physical activity behaviors of individuals with type 2 diabetes: A randomized clinical trial. Diabetes Res. Clin. Pract. 2008, 80, 371–379. [Google Scholar] [CrossRef] [PubMed]
- Baker, G.; Gray, S.R.; Wright, A.; Fitzsimons, C.; Nimmo, M.; Lowry, R.; Mutrie, N. The effect of a pedometer-based community walking intervention “Walking for Wellbeing in the West” on physical activity levels and health outcomes: A 12-week randomized controlled trial. Int. J. Behav. Nutr. Phys. Act. 2008, 5, 44. [Google Scholar] [CrossRef] [PubMed]
- Carr, L.J.; Bartee, R.T.; Dorozynski, C.; Broomfield, J.F.; Smith, M.L.; Smith, D.T. Internet-delivered behavior change program increases physical activity and improves cardiometabolic disease risk factors in sedentary adults: Results of a randomized controlled trial. Prev. Med. 2008, 46, 431–438. [Google Scholar] [CrossRef] [PubMed]
- Cheung, P.P.Y.; Chow, B.C.; Parfitt, G. Using Environmental Stimuli in Physical Activity Intervention for School Teachers: A Pilot Study. Int. Electron. J. Health Educ. 2008, 11, 47–56. [Google Scholar]
- Conroy, M.B.; Yang, K.; Elci, O.U.; Gabriel, K.P.; Styn, M.A.; Wang, J.; Kriska, A.M.; Sereika, S.M.; Burke, L.E. Physical activity self-monitoring and weight loss: 6-month results of the SMART trial. Med. Sci. Sports Exerc. 2011, 43, 1568–1574. [Google Scholar] [CrossRef] [PubMed]
- Dinger, M.K.; Heesch, K.C.; Cipriani, G.; Qualls, M. Comparison of two email-delivered, pedometer-based interventions to promote walking among insufficiently active women. J. Sci. Med. Sport 2007, 10, 297–302. [Google Scholar] [CrossRef] [PubMed]
- Dirige, O.V.; Carlson, J.A.; Alcaraz, J.; Moy, K.L.; Rock, C.L.; Oades, R.; Sallis, J.F. Siglang Buhay: Nutrition and physical activity promotion in Filipino-Americans through community organizations. J. Public Health Manag. Pract. 2013, 19, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Dunton, G.F.; Robertson, T.P. A tailored Internet-plus-email intervention for increasing physical activity among ethnically-diverse women. Prev. Med. 2008, 47, 605–611. [Google Scholar] [CrossRef] [PubMed]
- Ferney, S.L.; Marshall, A.L.; Eakin, E.G.; Owen, N. Randomized trial of a neighborhood environment-focused physical activity website intervention. Prev. Med. 2009, 48, 144–150. [Google Scholar] [CrossRef] [PubMed]
- Gilson, N.; McKenna, J.; Cooke, C.; Brown, W. Walking towards health in a university community: A feasibility study. Prev. Med. 2007, 44, 167–169. [Google Scholar] [CrossRef] [PubMed]
- Hemmingsson, E.; Hellénius, M.-L.; Ekelund, U.; Bergström, J.; Rössner, S. Impact of social support intensity on walking in the severely obese: A randomized clinical trial. Obesity 2008, 16, 1308–1313. [Google Scholar] [CrossRef] [PubMed]
- Hooker, S.P.; Harmon, B.; Burroughs, E.L.; Rheaume, C.E.; Wilcox, S. Exploring the feasibility of a physical activity intervention for midlife African American men. Health Educ. Res. 2011, 26, 732–738. [Google Scholar] [CrossRef] [PubMed]
- Hurling, R.; Catt, M.; Boni, M.D.; Fairley, B.W.; Hurst, T.; Murray, P.; Richardson, A.; Sodhi, J.S. Using internet and mobile phone technology to deliver an automated physical activity program: Randomized controlled trial. J. Med Internet Res. 2007, 9, e7. [Google Scholar] [CrossRef] [PubMed]
- Katz, D.L.; Shuval, K.; Comerford, B.P.; Faridi, Z.; Njike, V.Y. Impact of an educational intervention on internal medicine residents’ physical activity counselling: The Pressure System Model. J. Eval. Clin. Pract. 2008, 14, 294–299. [Google Scholar] [CrossRef] [PubMed]
- Kwak, L.; Kremers, S.P.J.; van Baak, M.A.; Brug, J. A poster-based intervention to promote stair use in blue- and white-collar worksites. Prev. Med. 2007, 45, 177–181. [Google Scholar] [CrossRef] [PubMed]
- Lane, A.; Murphy, N.; Bauman, A.; Chey, T. Randomized controlled trial to increase physical activity among insufficiently active women following their participation in a mass event. Health Educ. J. 2010, 69, 287–296. [Google Scholar] [CrossRef]
- Liebreich, T.; Plotnikoff, R.C.; Courneya, K.S.; Boulé, N. Diabetes NetPLAY: A physical activity website and linked email counselling randomized intervention for individuals with type 2 diabetes. Int. J. Behav. Nutr. Phys. Act. 2009, 6, 18. [Google Scholar] [CrossRef] [PubMed]
- Marcus, B.H.; Napolitano, M.A.; King, A.C.; Lewis, B.A.; Whiteley, J.A.; Albrecht, A.; Parisi, A.; Bock, B.; Pinto, B.; Sciamanna, C.; et al. Telephone versus print delivery of an individualized motivationally tailored physical activity intervention: Project STRIDE. Health Psychol. 2007, 26, 401–409. [Google Scholar] [CrossRef] [PubMed]
- Merom, D.; Rissel, C.; Phongsavan, P.; Smith, B.J.; van Kemenade, C.; Brown, W.J.; Bauman, A.E. Promoting walking with pedometers in the community: The step-by-step trial. Am. J. Prev. Med. 2007, 32, 290–297. [Google Scholar] [CrossRef] [PubMed]
- Migneault, J.P.; Dedier, J.J.; Wright, J.A.; Heeren, T.; Campbell, M.K.; Morisky, D.E.; Rudd, P.; Friedman, R.H. A culturally adapted telecommunication system to improve physical activity, diet quality, and medication adherence among hypertensive African-Americans: A randomized controlled trial. Ann. Behav. Med. A Publ. Soc. Behav. Med. 2012, 43, 62–73. [Google Scholar] [CrossRef] [PubMed]
- Oenema, A.; Brug, J.; Dijkstra, A.; de Weerdt, I.; de Vries, H. Efficacy and use of an internet-delivered computer-tailored lifestyle intervention, targeting saturated fat intake, physical activity and smoking cessation: A randomized controlled trial. Ann. Behav. Med. A Publ. Soc. Behav. Med. 2008, 35, 125–135. [Google Scholar] [CrossRef] [PubMed]
- Opdenacker, J.; Boen, F.; Vanden Auweele, Y.; de Bourdeaudhuij, I. Effectiveness of a lifestyle physical activity intervention in a women’s organization. J. Women’s Health 2008, 17, 413–421. [Google Scholar] [CrossRef] [PubMed]
- Pekmezi, D.W.; Williams, D.M.; Dunsiger, S.; Jennings, E.G.; Lewis, B.A.; Jakicic, J.M.; Marcus, B.H. Feasibility of using computer-tailored and internet-based interventions to promote physical activity in underserved populations. Telemed. J. e-Health 2010, 16, 498–503. [Google Scholar] [CrossRef] [PubMed]
- Prestwich, A.; Perugini, M.; Hurling, R. Can implementation intentions and text messages promote brisk walking? A randomized trial. Health Psychol. 2010, 29, 40–49. [Google Scholar] [CrossRef] [PubMed]
- Prochaska, J.O.; Butterworth, S.; Redding, C.A.; Burden, V.; Perrin, N.; Leo, M.; Flaherty-Robb, M.; Prochaska, J.M. Initial efficacy of MI, TTM tailoring and HRI’s with multiple behaviors for employee health promotion. Prev. Med. 2008, 46, 226–231. [Google Scholar] [CrossRef] [PubMed]
- Sabti, Z.; Handschin, M.; Joss, M.K.; Allenspach, E.C.; Nüscheler, M.; Grize, L.; Braun-Fahrländer, C. Evaluation of a physical activity promotion program in primary care. Fam. Pract. 2010, 27, 279–284. [Google Scholar] [CrossRef] [PubMed]
- Sherman, B.J.; Gilliland, G.; Speckman, J.L.; Freund, K.M. The effect of a primary care exercise intervention for rural women. Prev. Med. 2007, 44, 198–201. [Google Scholar] [CrossRef] [PubMed]
- Spittaels, H.; de Bourdeaudhuij, I.; Brug, J.; Vandelanotte, C. Effectiveness of an online computer-tailored physical activity intervention in a real-life setting. Health Educ. Res. 2007, 22, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Spittaels, H.; de Bourdeaudhuij, I.; Vandelanotte, C. Evaluation of a website-delivered computer-tailored intervention for increasing physical activity in the general population. Prev. Med. 2007, 44, 209–217. [Google Scholar] [CrossRef] [PubMed]
- Steele, R.; Mummery, W.K.; Dwyer, T. Using the Internet to promote physical activity: A randomized trial of intervention delivery modes. J. Phys. Act. Health 2007, 4, 245–260. [Google Scholar] [CrossRef] [PubMed]
- Sternfeld, B.; Block, C.; Quesenberry, C.P.; Block, T.J.; Husson, G.; Norris, J.C.; Nelson, M.; Block, G. Improving diet and physical activity with ALIVE: A worksite randomized trial. Am. J. Prev. Med. 2009, 36, 475–483. [Google Scholar] [CrossRef] [PubMed]
- Yap, T.L.; Davis, L.S.; Gates, D.M.; Hemmings, A.B.; Pan, W. The effect of tailored e-mails in the workplace. Part II. Increasing overall physical activity. Aaohn J. 2009, 57, 313–319. [Google Scholar] [CrossRef]
- Zoellner, J.; Connell, C.; Powers, A.; Avis-Williams, A.; Yadrick, K.; Bogle, M.L. Does a six-month pedometer intervention improve physical activity and health among vulnerable African Americans? A feasibility study. J. Phys. Act. Health 2010, 7, 224–231. [Google Scholar] [CrossRef] [PubMed]
- Shamseer, L.; Hopewell, S.; Altman, D.G.; Moher, D.; Schulz, K.F. Update on the endorsement of CONSORT by high impact factor journals: A survey of journal “Instructions to Authors” in 2014. Trials 2016, 17, 301. [Google Scholar] [CrossRef] [PubMed]
- Button, K.S.; Ioannidis, J.P.A.; Mokrysz, C.; Nosek, B.A.; Flint, J.; Robinson, E.S.J.; Munafò, M.R. Power failure: Why small sample size undermines the reliability of neuroscience. Nat. Rev. Neurosci. 2013, 14, 365–376. [Google Scholar] [CrossRef] [PubMed]
- Faber, J.; Fonseca, L.M. How sample size influences research outcomes. Dent. Press J. Orthod. 2014, 19, 27–29. [Google Scholar] [CrossRef]
- Sullivan, G.M.; Feinn, R. Using Effect Size-or Why the P Value Is Not Enough. J. Grad. Med Educ. 2012, 4, 279–282. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [CrossRef] [PubMed]
- International Union for Health Promotion and Education (IUHPE). The Evidence of Health Promotion Effectiveness. Shaping Public Health in a New Europe, Part Two, 2nd ed.; ECSC-EC-EAEC: Luxembourg, 2000. [Google Scholar]
- Walter, U.; Nöcker, G.; Plaumann, M.; Linden, S.; Pott, E.; Koch, U.; Pawils, S.; Altgeld, T.; Dierks, M.L.; Frahsa, A.; et al. Memorandum zur Präventionsforschung—Themenfelder und Methoden (Langfassung): [Memorandum prevention research - research areas and methods]. Das Gesundh. 2012, 74, e99–e113. [Google Scholar] [CrossRef]
- Karlsson, P.; Bergmark, A. Compared with what? An analysis of control-group types in Cochrane and Campbell reviews of psychosocial treatment efficacy with substance use disorders. Addiction 2015, 110, 420–428. [Google Scholar] [CrossRef] [PubMed]
- Cumming, G.; Fidler, F.; Kalinowski, P.; Lai, J. The statistical recommendations of the American Psychological Association Publication Manual: Effect sizes, confidence intervals, and meta-analysis. Aust. J. Psychol. 2012, 64, 138–146. [Google Scholar] [CrossRef]
- Prince, S.A.; Adamo, K.B.; Hamel, M.E.; Hardt, J.; Connor Gorber, S.; Tremblay, M. A comparison of direct versus self-report measures for assessing physical activity in adults: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2008, 5, 56. [Google Scholar] [CrossRef] [PubMed]
- Rosenbaum, D. Aktuelle Messverfahren zur objektiven Erfassung körperlicher Aktivitäten unter besonderer Berücksichtigung der Schrittzahlmessung. Bundesgesundheitsblatt-Gesundh. Gesundh. 2012, 55, 88–95. [Google Scholar] [CrossRef] [PubMed]
- Ainsworth, B.E.; Caspersen, C.J.; Matthews, C.E.; Mâsse, L.C.; Baranowski, T.; Zhu, W. Recommendations to Improve the Accuracy of Estimates of Physical Activity Derived from Self Report. J. Phys. Act. Health 2012, 9, S76–S84. [Google Scholar] [CrossRef] [PubMed]
- Haskell, W.L. Physical Activity by Self-Report: A Brief History and Future Issues. J. Phys. Act. Health 2012, 9, S5–S10. [Google Scholar] [CrossRef] [PubMed]
- Godino, J.G.; Watkinson, C.; Corder, K.; Sutton, S.; Griffin, S.J.; van Sluijs, E.M.F. Awareness of physical activity in healthy middle-aged adults: A cross-sectional study of associations with sociodemographic, biological, behavioural, and psychological factors. BMC Public Health 2014, 14, 421. [Google Scholar] [CrossRef] [PubMed]
- Lagersted-Olsen, J.; Korshøj, M.; Skotte, J.; Carneiro, I.G.; Søgaard, K.; Holtermann, A. Comparison of objectively measured and self-reported time spent sitting. Int. J. Sports Med. 2014, 35, 534–540. [Google Scholar] [CrossRef] [PubMed]
- Armijo-Olivo, S.; Stiles, C.R.; Hagen, N.A.; Biondo, P.D.; Cummings, G.G. Assessment of study quality for systematic reviews: A comparison of the Cochrane Collaboration Risk of Bias Tool and the Effective Public Health Practice Project Quality Assessment Tool: Methodological research. J. Eval. Clin. Pract. 2012, 18, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Selection Process | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| First phase (review selection) | Article type: reviews or meta-analyses Focus: effectiveness of PA interventions Participants: working age (16–67 years) | Primary outcome: not PA Focus: only sedentary behavior (e.g., sitting time), fitness (e.g., maximal oxygen consumption), or vital parameters (e.g., blood pressure) |
| Second phase (study selection) | Published: 2007 or later Primary outcome: PA (frequency, duration and/or intensity) Authors reported statistically significant effectiveness of the intervention | Same as the exclusion criteria of the first search |
| Study | Delphi List | Materials and Methods | Results | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Author, Year | Score [0–9] | Study Design | Group Conditions (Sample Size) | Operationalization of PA (Instrument; Time Frame) | Statistics:
| Sample Size Achieved | Effect Size | Follow-Up after end of Intervention (Time; Significant Difference from Baseline) | |
| Subjective | Objective | ||||||||
| Allen et al., 2008 [27] | 5 | RCT | IG (n = 21) ICG (n = 25) | - | ✓ (Accelerometer, 7 days) |
| - | ✓ | - |
| Baker et al., 2008 [28] | 6 | RCT | IG (n = 39) Non-ICG (n = 40) | ✓ (IPAQ, 7 days) | ✓ (Pedometer, 7 days) |
| ✓ | ✓ | - |
| Carr et al., 2008 [29] | 5 | RCT | IG (n = 14) Non-ICG (n = 18) | - | ✓ (Pedometer, 7 daysa) |
| - | ✓ | - |
| Cheung, Chow, & Parfitt, 2008 [30] | 3 | RCT | IG (n = 38) Non-ICG (n = 14) | - | ✓ (Pedometer, 5 daysa) |
| - | - | - |
| Conroy et al., 2011 [31] | 4 | Randomized clinical trial: secondary analysis | IG1 (n = 61) IG2 (n = 64) IG3 (n = 64) No CG | ✓ (Modifiable Activity Questionnaire, 6 months) | - |
| - | - | - |
| Dinger et al., 2007 [32] | 5 | Randomized clinical trial | IG1 (n = 24) IG2 (n = 32) No CG | ✓ (Selection of IPAQ short version items, 7 days) | - |
| - | ✓ | - |
| Dirige et al., 2013 [33] | 4 | RCT | IG (n = 255) ICG (n = 273) | ✓ (Godin Shephard Physical Activity Survey, 7 days) | - |
| - | ✓ | - |
| Dunton & Robertson, 2008 [34] | 6 | RCT | IG (n = 85) Non-ICG (n = 71) | ✓ (Standardized activity inventory format, 2 weeks) | - |
| - | - | - |
| Ferney et al., 2009 [35] | 7 | RCT | IG (n = 52) ICG (n = 54) | ✓ (Active Australian Questionnaire, 7 days; Self-reported neighborhood walking, 7 days) | - |
| - | - | - |
| Gilson, et al., 2007 [36] | 3 | RCT | IG1 (n = 21) IG2 (n = 21) Non-ICG (n = 22) | - | ✓ (Pedometer, 5 days) |
| - | ✓ | - |
| Hemmingsson et al., 2008 [37] | 3 | Randomized clinical trial | IG (n = 22) ICG (n = 20) | - | ✓ (Pedometer, 7 daysa) |
| ✓ | - | - |
| Hooker et al., 2011 [38] | 2 | Quasi experimental pre-post design | IG (n = 25) No CG | ✓ (CHAMPS, 7 days) | - |
| - | - | - |
| Hurling et al., 2007 [39] | 6 | RCT | IG (n = 47) Non-ICG (n = 30) | ✓ (IPAQ, 7 days) | ✓ (Accelerometer, 12 weeks) |
| - | - | - |
| Katz et al., 2008 [40] | 5 | Controlled educational trial | IG (n = 185) ICG (n = 117) | ✓ (Yale Physical Activity Survey, 7 days) | - |
| - | - | ✓ (6 months, significant) |
| Kwak et al., 2007 [41] | 1 | Cohort study | IG (approx. n = 950) No CG | - | ✓ (Count of staircase use, 3 weeks) |
| - | - | ✓ (1 week, non-significant) |
| Lane et al., 2010 [42] | 2 | RCT | IG (n = 55) ICG (n = 57) | ✓ (Subjective questions, 7 days) | - |
| - | - | - |
| Liebreich et al., 2009 [43] | 6 | RCT | IG (n = 23) ICG (n = 24) | ✓ (GLTEQ modified, 1 month) | - |
| - | ✓ | - |
| Marcus et al., 2007 [44] | 6 | RCT | IG1 (n = 80) IG2 (n = 81) ICG (n = 78) | ✓ (7-day PAR) | - |
| - | - | - |
| Merom et al., 2007 [45] | 7 | RCT | IG1 (n = 123) IG2 (n = 123) Non-ICG (n = 123) | ✓ (Active Australian Questionnaire, 7 days; College Alumni Questionnaire, 3 months) | - |
| ✓ | - | - |
| Migneault et al., 2012 [46] | 4 | RCT | IG (n = 169) ICG (n = 168) | ✓ (7-day PAR) | - |
| ✓ | - | - |
| Oenema et al., 2008 [47] | 6 | RCT | IG (n = 462) b Non-ICG (n = 504) | ✓ (Short-form IPAQ, 7 days) | - |
| ✓ | - | - |
| Opdenacker et al., 2008 [48] | 5 | RCT | IG (n = 68) Non-ICG (n = 60) | ✓ (IPAQ, 7 days) | ✓ (Accelerometer, 5 days a) |
| - | - | - |
| Pekmezi et al., 2010 [49] | 4 | RCT | IG1 (n = 11) IG2 (n = 15) ICG (n = 12) | ✓ (7-day PAR) | - |
| - | - | - |
| Prestwich, Perugini, & Hurling, 2010 [50] | 7 | RCT | IG1 (n = 40) IG2 (n = 48) ICG (n = 46) | ✓ (Self-report Walking and Exercise Tables, 17 days) | - |
| ✓ | ✓ | - |
| Prochaska et al., 2008 [51] | 4 | RCT | IG1 (n = 433) c IG2 (n = 503) ICG (n = 464) | ✓ (Self-reported level of exercise, 7 days) | - |
| ✓ | - | - |
| Sabti et al., 2010 [52] | 2 | Cohort study | IG (n = 776) Non-ICG (n = 463) | ✓ (Evaluation questions based on HEPA survey, 7 days) | - |
| - | - | - |
| Sherman et al., 2007 [53] | 1 | Cohort study | IG (n = 60) No CG | - | ✓ (Pedometer, 3 daysa) |
| - | - | - |
| Spittaels et al., 2007 [54] | 6 | Randomized clinical trial | IG1 (n = 116) IG2 (n = 122) ICG (n = 141) | ✓ (IAPQ, 7 days) | - |
| - | - | - |
| Spittaels et al., 2007 [55] | 5 | RCT | IG1 (n = 173) IG2 (n = 129) Non-ICG (n = 132) | ✓ (IPAQ, 7 days) | - |
| - | - | - |
| Steele, Mummery, & Dwyer, 2007 [56] | 6 | Randomized trial | IG1 (n = 65) IG2 (n = 65) IG3 (n = 62) No CG | ✓ (Active Australian Questionnaire, 7 days) | - |
| ✓ | ✓ | ✓ (2 and 5 months, significant) |
| Sternfeld et al., 2009 [57] | 6 | RCT | IG (n = 351) Non-ICG (n = 436) | ✓ (PAQ, adapted from Cross-Cultural Activity Patterns Questionnaire, 7 days in last 4 months) | - |
| - | - | ✓ (4 months, significant) |
| Yap et al., 2009 [58] | 0 | Quasi-experimental design | IG (n = 37) Non-ICG (n = 36) | ✓ (Stanford Brief Activity Survey, 2 weeks) | ✓ (Accelerometer, 24 hours) |
| - | - | - |
| Zoellner et al., 2010 [59] | 2 | Feasibility study | IG (n = 56) No CG | - | ✓ (Pedometer, 1 month a) |
| - | - | - |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rudolf, K.; Dejonghe, L.A.L.; Froböse, I.; Lammer, F.; Rückel, L.-M.; Tetz, J.; Schaller, A. Effectiveness Studies in Health Promotion: A Review of the Methodological Quality of Studies Reporting Significant Effects on Physical Activity in Working Age Adults. Int. J. Environ. Res. Public Health 2019, 16, 813. https://doi.org/10.3390/ijerph16050813
Rudolf K, Dejonghe LAL, Froböse I, Lammer F, Rückel L-M, Tetz J, Schaller A. Effectiveness Studies in Health Promotion: A Review of the Methodological Quality of Studies Reporting Significant Effects on Physical Activity in Working Age Adults. International Journal of Environmental Research and Public Health. 2019; 16(5):813. https://doi.org/10.3390/ijerph16050813
Chicago/Turabian StyleRudolf, Kevin, Lea A. L. Dejonghe, Ingo Froböse, Florian Lammer, Lisa-Marie Rückel, Jessica Tetz, and Andrea Schaller. 2019. "Effectiveness Studies in Health Promotion: A Review of the Methodological Quality of Studies Reporting Significant Effects on Physical Activity in Working Age Adults" International Journal of Environmental Research and Public Health 16, no. 5: 813. https://doi.org/10.3390/ijerph16050813
APA StyleRudolf, K., Dejonghe, L. A. L., Froböse, I., Lammer, F., Rückel, L.-M., Tetz, J., & Schaller, A. (2019). Effectiveness Studies in Health Promotion: A Review of the Methodological Quality of Studies Reporting Significant Effects on Physical Activity in Working Age Adults. International Journal of Environmental Research and Public Health, 16(5), 813. https://doi.org/10.3390/ijerph16050813