1. Background
Becoming a first-time parent can be an overwhelming experience, providing many unanticipated outcomes. Research has shown that many parents and caregivers (collectively referred to here as “parents”) have questions and self-doubt, particularly when the child is young (e.g., in the infant and toddler stages). Concerns regarding parenting in general and the child’s developmental progress and/or behavior are common among parents of children around 14 months of age [
1]. Indeed, nearly 60% of these parents reported having parental concerns for which they felt they needed assistance or advice from someone outside of the family and approximately 11% of parents report having frequent concerns [
1]. The circumstances in the parents’ lives can cause parenting to become even more challenging and stressful [
2]. Östberg conceptualized parenting stress as the perceived discrepancy between the situation’s requirements and the parents’ personal resources [
3]. Parenting stress can lead to severe parenting practices such as child abuse and neglect [
4], both of which can lead to adverse physical, cognitive, and psychosocial outcomes for the child in both the short and long terms [
5,
6,
7]. Circumstances that can contribute to parenting stress include a lack of social support [
8,
9], being a single parent [
10], being a young parent (<19 years) [
8,
9,
10,
11], ambivalent feelings towards becoming a parent [
9,
12], depressive feelings [
8,
9,
11], spousal violence [
8,
9,
13,
14,
15], alcohol and/or drug abuse [
8,
9,
16], negative experiences during childhood [
8,
9,
11,
12,
13,
17,
18], negative sexual experiences [
11,
12,
18], the tendency to become upset and/or angry [
8], low birth weight of the child [
19], and preterm birth [
19].
In the Netherlands, community-based pediatric care is well organized and focuses on monitoring the child’s growth, health, well-being, behavior, and development by promoting health, and preventing disease; this preventive service is known collectively as Youth Health Care (YHC). Until the age of 19 years, each child in the Netherlands is invited by the YHC to undergo periodic health examinations, which usually take place at a YHC center or at the child’s school; these health examinations are provided free of charge [
20]. Although participation is voluntary, the compliance rate within the first months of childbirth is approximately 95% [
20,
21]. Importantly, the YHC’s goal is to support parents in the development of their parenting skills and to promote the healthy development of all children. Therefore, the YHC contributes to the prevention and to the early detection of parents who experience parenting stress; moreover, the YHC offers suitable interventions to these parents.
One such preventive intervention available to YHC centers is the Supportive Parenting Intervention. This intervention is designed to decrease parenting stress and empower parents with a newborn child who are at risk for developing parenting stress [
22]. The risk assessment tool IPARAN (Instrument for identification of Parents At Risk for child Abuse and Neglect) is used to identify at-risk parents based on the parents’ previous negative experiences (for example, during their own childhood) and current circumstances such as ambivalent feelings regarding becoming a parent and a lack of social support. A trained YHC nurse uses the IPARAN to identify parents who are at risk for developing parenting stress and are therefore eligible to receive the Supportive Parenting Intervention. This intervention consists of six 90-minute home visits by a YHC nurse during the first 18 months of the child’s life. Currently, approximately half of all YHC centers in the Netherlands offer the Supportive Parenting Intervention to parents.
A previous study [
22] assessed the effectiveness of the Supportive Parenting Intervention with respect to the child’s psychosocial development, the parents’ expectations and empathic awareness of their children’s needs, the potential for child abuse, and family support. The authors found significant positive effects in terms of the parents’ expectations, the child’s psychosocial development, and the potential for child abuse [
22].
In this paper we present the results of a more elaborate controlled trial designed to assess effects of the program on the factors targeted by the intervention. Parents who are at risk for developing parenting stress were compared to parents who had the same risk but received care as usual. We evaluated the intervention’s effects on parenting skills, social support (both from family and friends, and from the partner), self-sufficiency, and resilience. In addition, we examined the intervention’s effect on the child’s health, specifically child psychosocial health measured by the Child Behavior Check List (CBCL). We investigated which characteristics of the parents and child affected the Supportive Parenting Intervention’s ability to empower at-risk parents. Finally, we evaluated the experiences of the parents who received the Supportive Parenting Intervention.
2. Methods
2.1. Study Design and Power of the Study
In this study, a non-randomized controlled trial was performed with an intervention group and a control group. The design of this study has been described in detail elsewhere [
23]. The trial was registered with the Netherlands Trial Register retrospectively (
www.trialregister.nl; NTR 5307). This study was approved by the Medical Ethics Committee of Erasmus Medical Center Rotterdam (MEC-2013-568). Because the Supportive Parenting Intervention is currently not available at all YHC centers in the Netherlands, the intervention group was recruited in an area in which the intervention was available. The control group was recruited in an area in which the Supportive Parenting Intervention has not been available since January 2014; the control group received care as usual.
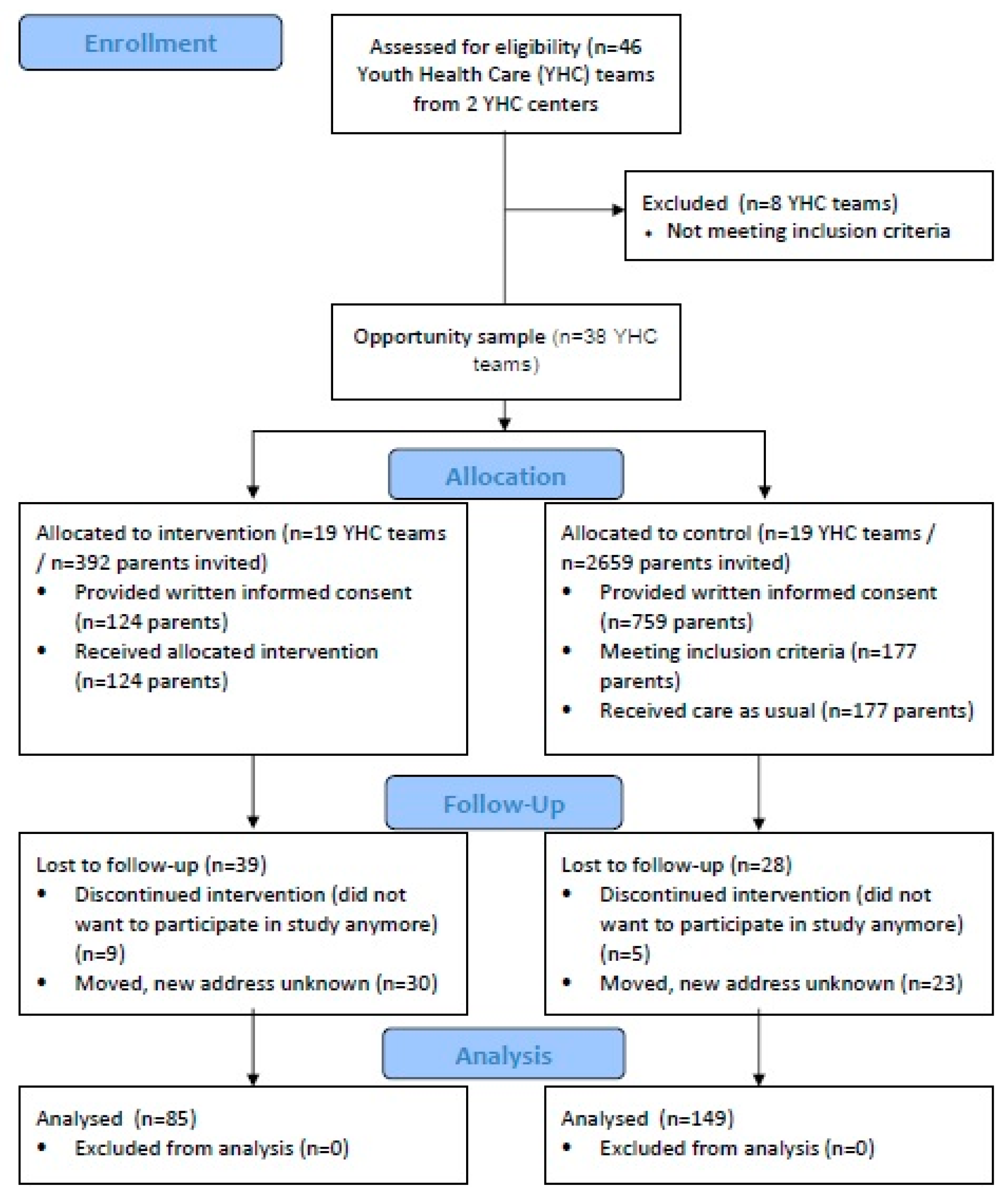
An opportunity sample of two preventive YHC centers (Centre for Youth and Family (CJG) Rijnmond and Rivas Zorggroep) in two regions of the Netherlands participated in this study. All the parents who started the Supportive Parenting Intervention between January 2014 and September 2014 (
n = 392) were invited by CJG Rijnmond to participate in the intervention group. All the parents with a child born between January 2014 and September 2014 who were living in an area in which the Supportive Parenting Intervention was not available (
n = 2659) were invited by Rivas Zorggroep to participate in the control group. Taking into account informed consent by 50% and eligibility of 10% of the parents in the control group, we expected data of 196 parents in the intervention group and 133 parents in the control group, a total of 329 parents. This was slightly more, as described in the design paper [
23].
With the use of continuous measures and assuming a standard deviation of 1.00 in both study groups, a power of 0.80 and an alpha of 0.05, and being able to demonstrate a significant difference of 0.35 standard deviation units of continuous outcome measures between the intervention and control group, a total group size of 329 was appropriate to indicate relevant effects [
24,
25].
2.2. Participants and Data Collection
For the intervention group, all the parents of a newborn child received, within 5–14 days of childbirth, the Instrument for identification of Parents At Risk for child Abuse and Neglect (IPARAN) in order to identify risk factors associated with the development of parenting stress (a detailed description of the IPARAN is provided in the
supplementary File 1 and Table S1). Based on their IPARAN score, at-risk parents were offered the Supportive Parenting Intervention. Parents were free to refuse the intervention. In total, 392 parents who started the Supportive Parenting Intervention between January and September 2014 were invited to participate in the study and were given an information leaflet; 124 parents provided written informed consent and completed the baseline questionnaire (a response rate of 31.6%).
For the control group, a total of 2659 parents were invited to participate and were given an information leaflet; 759 parents provided written informed consent and completed the baseline questionnaire (a response rate of 28.5%). Of these 759 parents, 177 (23.3%) were eligible to participate in the control group, based on their IPARAN score.
Data were collected at baseline, when the child was 12 months of age, and at the end of the intervention (when the child was 18 months of age). At baseline, the five primary outcomes of parental empowerment (parenting skills, social support (both from family and friends, and from the partner), self-sufficiency, and resilience) were measured. At the 18-month time point, the five primary outcomes of parental empowerment were measured again, as was the child’s psychosocial health; in addition, the parents in the intervention group were also requested to answer questions regarding whether they appreciated the Supportive Parenting Intervention.
Parents completed the baseline and follow-up questionnaire in their own time, the nurse was not present. At the 18-month time point, the questionnaire was completed by 85/124 (69%) of the parents in the intervention group and by 149/177 (84%) of the parents in the control group. In this study, we evaluated the effect of the Supportive Parenting Intervention on the parental empowerment by comparing data of the baseline with data at 18 months follow-up.
The enrollment, allocation, and participation of parents in the study are summarized in
Figure 1.
2.3. Supportive Parenting Intervention
The Supportive Parenting Intervention is based on the ecological model of Belsky [
26,
27,
28] and Newberger’s concept of parental awareness [
29], which was elaborated upon by Baartman [
30]. More detail on the development of the intervention can be found in the thesis of Bouwmeester-Landweer [
22]. The intervention is designed to decrease stress among parents with a newborn child, specifically among parents who are at risk for developing parenting stress based on their IPARAN scores. Parents are considered to be at risk when they present with one or more of the following risk factors: lack of social support; being a single parent; being a relatively young parent; negative childhood experiences; feelings of depression; alcohol and/or drug abuse; ambivalent feelings towards parenthood; the tendency to become easily upset and/or angry; negative sexual experience; in favor of physical punishment; having a child born pre-term and/or with low birth weight.
The intervention offered to at-risk parents is voluntary and consists of six 90-minute home visits by a YHC nurse during the first 18 months of the child’s life. Although the standard schedule calls for the six home visits to occur at 6 weeks and 3, 6, 9, 12, and 18 months of age, at the parents’ request, more visits can occur during the first several months, with fewer visits toward the end of the intervention. A home visit consists of a fixed part and a flexible part. During the fixed part of the visit, various topics are discussed, including empowering the parents by improving their parenting skills, discussing the parents’ expectations regarding being a parent, and providing advice to the parents regarding how to improve their social network. The flexible part of the visit is client-centered, and the topics discussed are chosen by the parents and can include empowerment issues and troubling experiences regarding parenting. In general, the focus of these home visits is to improve the interaction between the parent and the child, discussing the parents’ expectations regarding parenthood, dealing with the parents’ own childhood experiences, and building social support around the family. The YHC nurses who conduct the home visits have at least three years of experience in the YHC system and have received additional training in order to provide the Supportive Parenting Intervention. Thus, these nurses have the knowledge needed in order to provide parents with information regarding both health- and development-related issues. However, the nurses are not qualified to provide psychotherapy treatment or family therapy; if deemed necessary, the YHC nurse can refer the parents to a specialist for more extensive treatment [
31].
2.4. Care as Usual
During the study, the parents in the control group lived in a region in which the Supportive Parenting Intervention was not offered by their YHC center. These parents were therefore offered care as usual, in which the parents were invited to bring their child to the YHC for periodic health examinations. Twelve such examinations are offered within the first 18 months of the child’s life, during which the child’s growth and development are monitored, and the parents receive general advice regarding parenting. If deemed necessary, the parents can be referred to a specialist (e.g., to receive a home visit by a trained YHC nurse, referral to a child psychologist, or invited to attend a course in parenting).
2.5. Ethics Statement
All the questionnaires were completed by the parents on a voluntary basis. Parents received detailed written information regarding the study and were free to decline participation. Parents who chose to participate in the study provided written informed consent. Only anonymous data were used for analysis. The study was approved by the Medical Ethics Committee of Erasmus Medical Center, Rotterdam (MEC-2013-568).
2.6. Measurements
2.6.1. Primary Outcome Measurements
The primary outcomes of this study were five aspects of empowerment (the parents’ parenting skills, social support (both from family and friends, and from the partner), self-sufficiency, and resilience and the child’s psychosocial health at 18 months of age. All the outcomes were collected through questionnaires.
Parenting skills was measured using the subscale “basic parenting skills” of the Family Functioning Questionnaire (FFQ) [
32]. The FFQ assesses the problems that parents encounter within their family and provides an indication of how well the parent believes that his/her family functions, and consists of five subscales in total. The subscale basic parenting skills assesses the extent to which the parent feels capable of managing the household and finances, maintaining contact with the daycare provider (if applicable), and provides for the child’s daily needs. The subscale consists of seven items that are answered using a 4-point response scale ranging from 1 (not true) to 4 (very true). The individual item scores were summed to obtain a total score [
32]. The subscale “basic parenting skills” had a Cronbach’s alpha value of 0.72.
Social support from family and friends was measured using the “social contacts” subscale of the FFQ. Social support from the partner was measured using the “partner relationship” subscale of the FFQ. The “social contacts” subscale assesses the extent to which the parent has contact with his/her neighbors, friends, and family members. The subscale “partner relationship” assesses a person’s perception of his/her relationship with his/her partner and the extent to which he/she feels supported by his/her partner. Each subscale contains five items that are answered using a 4-point response scale ranging from 1 (not true) to 4 (very true). For each subscale, the individual item scores were summed to obtain a total score [
32]. The subscales “social contacts” and “partner relationship” had a Cronbach’s alpha value of 0.74 and 0.89, respectively. The total scores of both subscales were used as outcome measures.
Self-sufficiency was measured using version 2.0 of the Dutch Empowerment Questionnaire for parents [
33]. This questionnaire consists of three subscales: “competence as a person”, “competence as a parent”, and “competence utilization”. The subscale “competence as a parent” (7 items) was used as the primary outcome measure. Each item in the subscale is scored using a 5-point response scale ranging from 1 (strongly disagree) to 5 (strongly agree). Three items in the subscale were not included in the questionnaire, as these items were not yet applicable to parents of a newborn child. The individual item scores were summed and the total score was then converted to a score ranging from 1 to 10. A low score indicates problems [
33]. The subscale “competence as a parent” had a Cronbach’s alpha value of 0.79.
The parents’ resilience was measured using the Dutch version of the Resilience Scale [
34]. This questionnaire consists of a total of 25 items in the subscales “personal competence” (17 items) and “acceptance of self and life” (8 items). The subscale “personal competence” assesses the extent to which a person can rely on himself/herself, is determined to achieve a goal, and is resourceful [
35]. The subscale “acceptance of self and life” assesses a person’s adaptability, flexibility, and balanced perspective on life [
35]. Each item is scored on a 4-point scale ranging from 1 (strongly disagree) to 4 (strongly agree). For each subscale, the individual scores were summed, and a total score was calculated by adding the two summed scores from the two subscales. Thus, the total score ranges from 25 to 100, with a higher score indicating higher resilience [
34]. This questionnaire had a Cronbach’s alpha value of 0.89.
The child’s behavioral and emotional problems were assessed at 18 months of age using the Child Behavior Checklist (CBCL) for ages 1½–5 [
36]. The CBCL consists of 99 items, each of which is scored on a 3-point scale ranging from 1 (not true) to 3 (very true or often true) plus one open-ended item for adding problems that are not mentioned on the form. The CBCL has two domains (Internalizing, and Externalizing) and provides a Total Problem score. A higher score indicates problems [
36]. The two domains Internalizing, and Externalizing, and the Total Problem score had a Cronbach’s alpha value of 0.85, 0.89, and 0.94, respectively.
2.6.2. Parent and Child Characteristics
Data regarding the age, gender, and country of birth of the child and both parents were collected. The education level of both parents, the family structure, and the net monthly family income were also collected, as well as data regarding the gestational age, and the child’s birth weight. The parent’s level of education was classified as low (primary education or lower secondary education), middle (higher secondary education or vocational education), or high (higher vocational education or university). Net family income was classified as low (less than €1800/month) or high (€1800/month or higher). The nationality of the child and both parents was classified as either Dutch or non-Dutch using the definitions established by Statistics Netherlands [
37].
2.6.3. Other Measures
The parents in the intervention group answered questions regarding the number of home visits they received and they were asked six questions regarding what they learned from the Supportive Parenting Intervention. The questionnaire also contained an open question inviting parents to write any comments and/or questions with respect to the study and/or intervention.
2.7. Statistical Analyses
Data were analyzed according to the intention-to-treat principle. Descriptive statistics were used to describe the sample characteristics. The chi-square test and independent Student’s t-test were used to test for differences in the demographic characteristics between the intervention and control groups. In addition, we tested for differences between participants, completing both questionnaires at baseline and follow-up at 18 months, and participants lost-to-follow up (i.e., participants only completing the baseline questionnaire). Descriptive statistics were also used to describe the parents’ evaluation of the Supportive Parenting Intervention.
Complete cases at baseline and follow-up at 18 months were used to evaluate the within-group change between baseline and follow-up with respect to the primary outcomes. A paired Student’s t-test was used. To evaluate differences in primary outcomes between the intervention and control groups, difference scores (i.e., the difference in mean scores between baseline and follow-up) were calculated, and generalized linear models were used, with the study group (i.e., intervention or control group) as the independent variable and the difference scores for the primary outcomes as the dependent variables. Beta values with a 95% confidence interval (95% CI) were calculated, and beta values with a p-value < 0.05 were considered statistically significant.
Potential confounders were added to the model to correct for confounding. Confounders were selected based on a significantly different distribution (categorical variables) or the average (continuous variables) in characteristics between the intervention and control groups (
Table 1), and based on having a significant association with the outcome of interest. The following confounders were included in the models predicting parenting skills, social support (from family and friends, and from the partner), self-sufficiency, and resilience: baseline scores, the age of the child, the nationality of the mother and the mother’s IPARAN score. Models with correction for potential confounders and models without correction for potential confounders are presented. Based on the aforementioned evaluations and a
p-value < 0.05, the child’s age, the mother’s IPARAN score, the family structure, the family’s net monthly income, and the mother’s nationality were included as potential confounders in the models for the child’s psychosocial health.
In addition, the role of socio-demographic characteristics (e.g., family structure, the mother’s IPARAN score, family net monthly income, and the mother’s nationality) on the intervention’s effect was examined by adding an interaction term (e.g., [(study group) x (net monthly income)]) to the model. If the interaction term had a p-value < 0.10, a stratified analysis was performed.
All statistical analyses were conducted using Statistical Package for the Social Sciences (SPSS) version 22 (IBM Corp. Released 2013. IBM SPSS Statistics for Windows, Version 22.0. Armonk, NY: IBM Corp.).
4. Discussion
Here, we evaluated the effect of the Supportive Parenting Intervention with respect to empowering parents who are at risk for developing parenting stress. Specifically, we evaluated parenting skills, social support (both from family and friends, and from the partner), the parents’ self-sufficiency and resilience, and the child’s psychosocial health and behavior. In addition, we evaluated elements of the Supportive Parenting Intervention among parents in the intervention group.
Overall, we found no effect of the intervention on either the parents’ empowerment or the child’s psychosocial health and behavior between baseline and follow-up. Our analysis revealed that neither the intervention group nor the control group improved with respect to any aspect of empowerment between baseline and follow-up. Similar results were obtained when we analyzed only first-time parents (data not shown). With respect to social contacts and partner support, and competence as a parent, the parents’ scores were either unchanged or were worse at follow-up (i.e., when the child was 18 months of age) compared to their baseline scores.
We did observe decreased parental outcomes (i.e., Social Support, Partner Relation, Competence as a Parent) in both study groups between baseline and follow-up. These effects may be explained—at least in part—by the general effect of the child’s developmental phase on the parents’ sense of skills and confidence in terms of raising their child. In general, parenting changes as the child grows, and the toddler months (19–25 months of age) can be a particularly stressful period for parents [
38]. During this period, the child enters a new developmental stage and this is often associated with new challenges for the parents. For example, toddlers often display more challenging behavior as they become better at understanding both their own emotions and the emotions of others. At this age, children learn to communicate their likes and dislikes, and they become capable of asserting their own will [
39]. In their search for autonomy, they often test the limits set by their parents [
38]. In a study by Fraser et al., the effect of a home-visit program to at-risk families shortly after childbirth was evaluated [
40]. Consistently with our results, the authors found a reduction in the parents’ sense of competence 6 weeks after childbirth. However, by 12 months, the competence scores returned to the same values as measured at baseline [
40]. Thus, the effect of the child’s developmental phases—and the corresponding changes in parental skills—warrant further investigation. Although parental confidence may diminish due to changes in the child’s developmental phase and the parental skills required during these phases, our intervention was unable to counteract the changes in parental confidence that occur as the child enters the toddler phase, as we found no differences between the intervention and control groups.
Given the above-mentioned developmental changes that occur at this age, the duration of our study (until the child reached 18 months of age) may have been too short to detect relevant differences. Likewise, the Supportive Parenting Intervention itself can be extended to last beyond 18 months of age, thereby supporting parents beyond the toddler years and improving both their competences as a parent and their use of those competences.
Another potential explanation for not observing an effect of the intervention could be related to other family circumstances. For example, having a limited income. In the current study, half of parents in the intervention group had an income below €1800. For these parents, different types of support might be more appropriate.
It should be noted that the parents in the control group were selected from an area in which the intervention had been performed until the start of this study (January 2014), but was no longer available. It is therefore possible that some of the YHC professionals in this area still used some elements of the intervention during the course of their work, which may have reduced any possible differences between the intervention and control groups. Moreover, the participants in the intervention and control group were not comparable at baseline with regard to social and demographic characteristics. The participants in the intervention group appeared to have a higher level of disadvantage, showing, for example, an average higher IPARAN score. Although we corrected for these differences in the analysis, they may have impacted the potential to observe effects.
Although we found no positive effects of the intervention in terms of empowerment, the parents in the intervention group reported that they were generally satisfied with the intervention. In particular, they felt more confident in their role as a parent and had more self-esteem after the intervention. Moreover, the parents in the intervention group appreciated the personal attention received from the YHC nurse and the fact that the visits occurred in their own home. These results suggest that the Supportive Parenting Intervention likely has clear—albeit less tangible—benefits for the parents.
Methodological Considerations
In addition to the considerations discussed above, this study has methodological limitations that warrant discussion. Due to low response at the start of our study, we extended the inclusion period by 4 months, making the total inclusion period eight months. However, we were not able reach our target number of 196 participants in the intervention group; a total of 124 parents participated in the intervention group. We were able to include more participants in the control group than aimed for: 177 instead of 133. Taking into account lost-to-follow-up, the power of our study slightly decreased. Thereby, the socio-demographic characteristics of the two study groups were not distributed equally; specifically, the intervention group contained larger percentages of parents who were non-Dutch, had a low net monthly income, were single parents, and had higher IPARAN scores. These differences may have arisen due to the methods used to select participating YHC centers, which resulted in the participants in the control group living primarily in a suburban area and the participants in the intervention group living primarily in an urban area. In an attempt to account for this unequal distribution of characteristics, the relevant variables were added to the models as confounders. In addition, in some cases, the parents completed the baseline questionnaire after their first visit by a YHC nurse, which may have influenced their responses. Finally, it is possible that due to differences in practices of the nurses providing the intervention the effect of the intervention may have differed. However, the intervention is provided according to a set structure, which includes nurse training and an intervention manual describing the content of each visit. Therefore, variation in practices between nurses was expected to be low. Nevertheless, we recommend that future studies monitor the nurses’ practices in order to take into account potential variability.
Despite these limitations, a strength of this study lies in the fact that we were able to evaluate this intervention within a group of parents who were at risk for developing parenting stress, using a control group of parents who had the same risk but did not have access to the intervention. Nevertheless, this study should be repeated using a longer follow-up period, including the empowerment of parents as their child passes various developmental stages, thereby increasing the likelihood of detecting inherent changes in empowerment.

 ,
, 

{kind=link}