Factors Associated with Suicide Attempts and Suicides in the General Population of Andalusia (Spain)



Abstract
1. Introduction
2. Methods
2.1. Study Variables
2.2. Statistical Analysis
2.3. Ethics
3. Results
3.1. Rates and Ratios of Suicide and Attempted Suicide
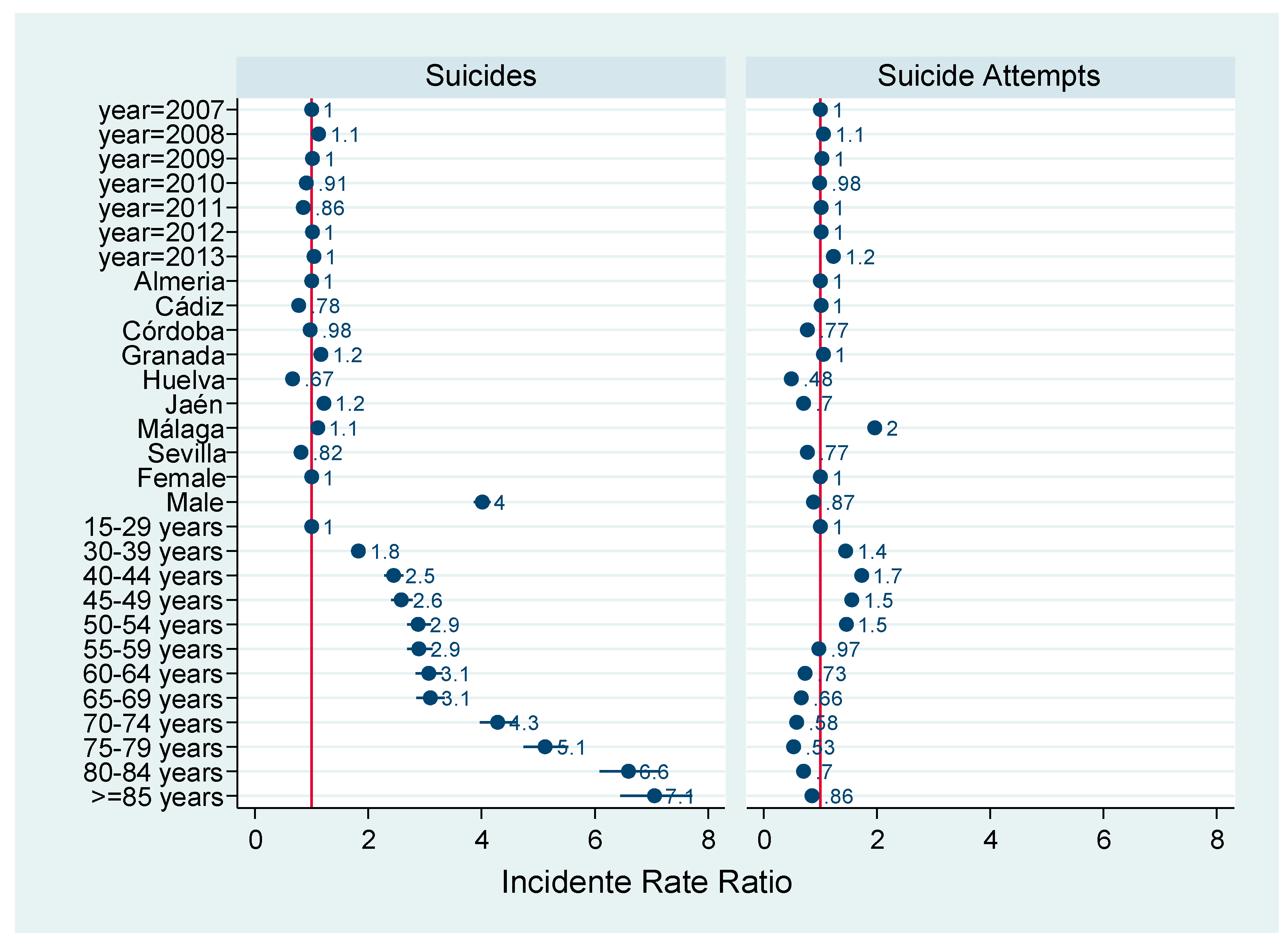
3.2. Association between Suicide and Attempted Suicide by Year, Sex, and Age
3.3. Association between Suicide and Attempted Suicide According to the Method Used
4. Discussion
4.1. Sex Differences between Suicide Attempts and Deaths by Suicide.
4.2. Age and Sex Specific Differences between Attempted Suicides and Suicides
4.3. The Method Used Exerts an Influence on Suicide and Attempted Suicide
4.4. Vulnerability of Elderly Men and Women to Suicidal Behavior
4.5. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Author Statement
References
- World Health Organization. Public Health Action for the Prevention of Suicide: A Framework; World Health Organization: Geneva, Switzerland, 2012; Available online: http://apps.who.int/iris/bitstream/handle/10665/75166/?sequence=1 (accessed on 6 August 2018).
- World Health Organization. Preventing Suicide: A Global Imperative; World Health Organization: Geneva, Switzerland, 2014; Available online: https://www.who.int/mental_health/suicide-prevention/world_report_2014/en/ (accessed on 6 August 2018).
- Nock, M.K.; Borges, G.; Bromet, E.J.; Cha, C.B.; Kessler, R.C.; Lee, S. Suicide and suicidal behavior. Epidemiol. Rev. 2008, 30, 133–154. [Google Scholar] [CrossRef] [PubMed]
- Posner, K.; Oquendo, M.A.; Gould, M.; Stanley, B.; Davies, M. Columbia Classification Algorithm of Suicide Assessment (CCASA): Classification of Suicidal Events in the FDA’s Pediatric Suicidal Risk Analysis of Antidepressants. Am. J. Psychiatry 2007, 164, 1035–1043. [Google Scholar] [CrossRef] [PubMed]
- Silverman, M.M.; Berman, A.L.; Sanddal, M.D.; O’Carroll, P.W.; Joiner, T.E. Rebuilding the tower of Babel: A revised nomenclature for the study of suicide and suicidal behaviors. Part 1: Background, Rationale, and Methodology. Suicide Life Threat. Behav. 2007, 37, 248–263. [Google Scholar] [CrossRef] [PubMed]
- Silverman, M.M.; Berman, A.L.; Sanddal, M.D.; O’Carroll, P.W.; Joiner, T.E. Rebuilding the tower of Babel: A revised nomenclature for the study of suicide and suicidal behaviors. Part 2: Suicide-related ideations, communications, and behaviors. Suicide Life Threat. Behav. 2007, 37, 264–277. [Google Scholar] [CrossRef]
- Turecki, G.; Brent, D.A. Suicide and suicidal behavior. Lancet 2016, 387, 1227–1239. [Google Scholar] [CrossRef]
- Krug, E.G.; Dahlberg, L.L.; Mercy, J.A.; Zwi, A.B.; Lozano, R. World Report on Violence and Health; World Health Organization: Geneva, Switzerland, 2002; Available online: https://apps.who.int/iris/bitstream/handle/10665/42495/9241545615_eng.pdf;jsessionid=84D9C87469A9CE62C2D41A810B5A9152?sequence=1 (accessed on 1 August 2019).
- DeJong, T.M.; Overholser, J.C.; Stockmeier, C.A. Apples to oranges? A direct comparison between suicide attempters and suicide completers. J. Affect. Disord. 2010, 124, 90–97. [Google Scholar] [CrossRef]
- Fushimi, M.; Sugawara, J.; Saito, S. Comparison of completed and attempted suicide in Akita, Japan. Psychiatry Clin. Neurosci. 2006, 60, 289–295. [Google Scholar] [CrossRef]
- Joo, S.H.; Wang, S.M.; Kim, T.W.; Seo, H.J.; Jeong, J.H.; Han, J.H.; Hong, S.C. Factors associated with suicide completion: A comparison between suicide attempters and completers. Asia Pac. Psychiatry 2016, 8, 80–86. [Google Scholar] [CrossRef]
- Stenbacka, M.; Jokinen, J. Violent and non-violent methods of attempted and completed suicide in Swedish young men: The role of early risk factors. BMC Psychiatry 2015, 15, 196. [Google Scholar] [CrossRef]
- Younes, N.; Melchior, M.; Turbelin, C.; Blanchon, T.; Hanslik, T.; Chee, C.C. Attempted and completed suicide in primary care: Not what we expected? J. Affect. Disord. 2015, 170, 150–154. [Google Scholar] [CrossRef]
- Borges, G.; Nock, M.K.; Haro Abad, J.M.; Hwang, I.; Sampson, N.A.; Alonso, J.; Andrade, L.H.; Angermeyer, M.C.; Beautrais, A.; Bromet, E.; et al. Twelve-month prevalence of and risk factors for suicide attempts in the World Health Organization World Mental Health Surveys. J. Clin. Psychiatry 2010, 71, 1617–1628. [Google Scholar] [CrossRef] [PubMed]
- Jordans, M.; Rathod, S.; Fekadu, A.; Medhin, G.; Kigozi, F.; Kohrt, B.; Luitel, N.; Petersen, I.; Shidhaye, R.; Ssebunnya, J.; et al. Suicidal ideation and behaviour among community and health care seeking populations in five low- and middle-income countries: A cross-sectional study. Epidemiol. Psychiatr. Sci. 2018, 27, 393–402. [Google Scholar] [CrossRef] [PubMed]
- Posporelis, S.; Paspali, A.; Takayanagi, Y.; Sawa, A.; Banerjea, P.; Kyriakopoulos, M. Demographic and clinical correlates of suicidality in adolescents attending a specialist community mental health service: A naturalistic study. J. Ment. Health 2015, 24, 225–229. [Google Scholar] [CrossRef] [PubMed]
- Beautrais, A.L. Suicides and serious suicide attempts: Two populations or one? Psychol. Med. 2001, 31, 837–845. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.P.; Liu, X.; Jia, C.X. Characteristics of suicide completers and attempters in rural Chinese population. Compr. Psychiatry 2016, 70, 134–140. [Google Scholar] [CrossRef]
- Parra-Uribe, I.; Blasco-Fontecilla, H.; García-Parés, G.; Giró, M.; Llorens, M.; Cebriá, A.; Leon-Martinez, V.; Pérez-Solá, V.; Palao, D.J. Attempted and completed suicide: Not what we expected? J. Affect. Disord. 2013, 150, 840–846. [Google Scholar] [CrossRef]
- Too, L.S.; Pirkis, J.; Milner, A.; Spittal, M.J. Clusters of suicides and suicide attempts: Detection, proximity and correlates. Epidemiol. Psychiatr. Sci. 2017, 26, 491–500. [Google Scholar] [CrossRef]
- Jansen, E.; Buster, M.C.; Zuur, A.L.; Das, C. Fatality of suicide attempts in Amsterdam 1996–2005. Crisis 2009, 30, 180–185. [Google Scholar] [CrossRef]
- Yoshioka, E.; Hanley, S.J.; Kawanishi, Y.; Saijo, Y. Time trends in method-specific suicide rates in Japan, 1990–2011. Epidemiol. Psychiatr. Sci. 2016, 25, 58–68. [Google Scholar] [CrossRef]
- Christiansen, E.; Jensen, B.F. Risk of repetition of suicide attempt, suicide or all deaths after an episode of attempted suicide: A register-based survival analysis. Aust. N. Z. J. Psychiatry 2007, 41, 257–265. [Google Scholar] [CrossRef]
- Hawton, K.; van Heeringen, K. Suicide. Lancet 2009, 373, 1372–1381. [Google Scholar] [CrossRef]
- Ribeiro, J.D.; Joiner, T.E. The interpersonal-psychological theory of suicidal behavior: Current status and future directions. J. Clin. Psychol. 2009, 65, 1291–1299. [Google Scholar] [CrossRef] [PubMed]
- Van Orden, K.A.; Witte, T.K.; Cukrowicz, K.C.; Braithwaite, S.R.; Selby, E.A.; Joiner, T.E. The interpersonal theory of suicide. Psychol. Rev. 2010, 117, 117–575. [Google Scholar] [CrossRef] [PubMed]
- Arias, S.A.; Boudreaux, E.D.; Chen, E.; Miller, I.; Camargo, C.A., Jr.; Jones, R.N.; Uebelacker, L. Which Chart Elements Accurately Identify Emergency Department Visits for Suicidal Ideation or Behavior? Arch. Suicide Res. 2019, 23, 382–390. [Google Scholar] [CrossRef]
- Shahtahmabesi, S. Examining the claim that 80–90% of suicide cases had depression. Front. Public Health 2013, 1, 62. [Google Scholar] [CrossRef]
- Clements, C.; Turnbull, P.; Hawton, K.; Geulayov, G.; Waters, K.; Ness, J.; Townsend, E.; Khundakar, K.; Kapur, N. Rates of self-harm presenting to general hospitals: A comparison of data from the Multicentre Study of Self-Harm in England and Hospital Episode Statistics. BMJ Open 2016, 6, e009749. [Google Scholar] [CrossRef] [PubMed]
- Mejías, Y.; García, M.P.; Schmidt, J.; Quero, A.; Gorlat, B. Estudio preliminar de las características del intento de suicidio en la provincia de Granada. Anales del Sistema Sanitario de Navarra 2011, 34, 431–441. [Google Scholar] [CrossRef]
- Mejías-Martín, Y.; Martí-García, C.; Rodríguez-Mejías, C.; Valencia-Quintero, J.P.; García-Caro, M.P.; Luna, J.D. Suicide attempts in Spain according to prehospital healthcare emergency records. PLoS ONE 2018, 13, e0195370. [Google Scholar] [CrossRef]
- De Leo, D.; Bertolote, J.M.; Lester, D. Self-Directed Violence; Krug, E.G., Dahlberg, L.L., Mercy, J.A., Zwi, A.B., Lozano, R., Eds.; World Report on Violence and Health; World Health Organization: Geneva, Switzerland, 2002; pp. 185–212. [Google Scholar]
- Franklin, J.C.; Ribeiro, J.D.; Fox, K.R.; Bentley, K.H.; Kleiman, E.M.; Huang, X.; Musacchio, K.M.; Jaroszewski, A.C.; Chang, B.P.; Nock, M.K. Risk factors for suicidal thoughts and behaviors: A meta-analysis of 50 years of research. Psychol. Bull. 2017, 143, 187–232. [Google Scholar] [CrossRef]
- Instituto Nacional de Estadística. Defunciones por suicidio. España. Available online: http://www.ine.es (accessed on 12 October 2017).
- Elnour, A.A.; Harrison, J. Lethality of suicide methods. Inj. Prev. 2008, 14, 39–45. [Google Scholar] [CrossRef]
- Instituto de Estadística y Cartografía de Andalucía. Padrón Municipal de Habitantes de. Cifras Oficiales de Población Municipal. Consejería de Economía y Conocimiento. 2016. Available online: http://www.juntadeandalucia.es/institutodeestadisticaycartografia/iea/consultasActividad.jsp?CodOper=6&sub=63567 (accessed on 4 August 2017).
- Santurtún, M.; Santurtún, A.; Agudo, G.; Zarrabeitia, M.T. Método empleado en las muertes por suicidio en España: Envenenamiento y agentes violentos no tóxicos. Cuad. Med. Forense 2016, 22, 73–80. [Google Scholar]
- Värnik, P. Suicide in the world. Int. J. Environ. Res. Public Health 2012, 9, 760–771. [Google Scholar] [CrossRef] [PubMed]
- Mergl, R.; Koburger, N.; Heinrichs, K.; Székely, A.; Tóth, M.D.; Coyne, J.; Quintão, S.; Arensman, E.; Coffey, C.; Maxwell, M.; et al. What Are Reasons for the Large Gender Differences in the Lethality of Suicidal Acts? An Epidemiological Analysis in Four European Countries. PLoS ONE 2015, 10, e0129062. [Google Scholar] [CrossRef] [PubMed]
- Canetto, S.S.; Sakinofsky, I. The Gender Paradox in Suicide. Suicide Life Threat. Behav. 1998, 28, 1–23. [Google Scholar] [CrossRef]
- Schrijvers, D.L.; Bollen, J.; Sabbe, B.G. The gender paradox in suicidal behavior and its impact on the suicidal process. J. Affect. Disord. 2012, 138, 19–26. [Google Scholar] [CrossRef]
- Kumar, C.T.; Mohan, R.; Ranjith, G.; Chandrasekaran, R. Characteristics of high intent suicide attempters admitted to a general hospital. J. Affect. Disord. 2006, 91, 77–81. [Google Scholar] [CrossRef]
- Freeman, A.; Mergl, R.; Kohls, E.; Székel, A.; Gusmao, R.; Arensman, E.; Koburger, N.; Hegerl, U.; Rummel-Kluge, C. A cross-national study on gender differences in suicide intent. BMC Psychiatry 2017, 17, 234. [Google Scholar] [CrossRef]
- The National Institute of Mental Health (NIMH). Health Information. Statistics Suicide. 2017. Available online: https://www.nimh.nih.gov/health/statistics/suicide.shtml (accessed on 18 January 2018).
- McManus, S.; Hassiotis, A.; Jenkins, R.; Dennis, M.; Aznar, C.; Appleby, L. Chapter 12: Suicidal thoughts, suicide attempts, and self-harm. In Mental Health and Wellbeing in England: Adult Psychiatric Morbidity Survey 2014; McManus, S., Bebbington, P., Jenkins, R., Brugha, T., Eds.; NHS Digital: Leicester, UK, 2016; Available online: https://discovery.ucl.ac.uk/id/eprint/1518055/1/APMS%202014-full-rpt.pdf (accessed on 13 November 2019).
- Goodfellow, B.; Kõlves, K.; de Leo, D. Contemporary Definitions of Suicidal Behavior: A Systematic Literature Review. Suicide Life Threat. Behav. 2018, 48, 353–366. [Google Scholar] [CrossRef]
- Stewart, J.G.; Esposito, E.C.; Glenn, C.R.; Gilman, S.E.; Pridgen, B.; Gold, J.; Auerbach, R.P. Adolescent self-injurers: Comparing non-ideators, suicide ideators, and suicide attempters. J. Psychiatr. Res. 2017, 84, 105–112. [Google Scholar] [CrossRef]
- Office for National Statistics (ONS). Suicides in the United Kingdom: 2013 Registrations; ONS: London, UK, 2015. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/bulletins/suicidesintheunitedkingdom/2015-02-19 (accessed on 28 August 2018).
- Lipari, R.; Piscopo, K.; Kroutil, L.A.; Miller, G.K. Suicidal Thoughts and Behavior among Adults: Results from the 2014 National Survey on Drug Use and Health. NSDUH Data Review. 2015. Available online: https://www.samhsa.gov/data/sites/default/files/NSDUH-FRR2-2014/NSDUH-FRR2-2014.pdf (accessed on 13 November 2019).
- Bostwick, J.M.; Pabbati, C.; Geske, J.R.; McKean, A.J. Suicide Attempt as a Risk Factor for Completed Suicide: Even More Lethal Than We Knew. Am. J. Psychiatry 2016, 173, 1094–1100. [Google Scholar] [CrossRef] [PubMed]
- Callanan, V.J.; Davis, M.S. Gender differences in suicide methods. Soc. Psychiatry Psychiatr. Epidemiol. 2012, 47, 857–869. [Google Scholar] [CrossRef] [PubMed]
- Cibis, A.; Mergl, R.; Bramesfeld, A.; Althaus, D.; Niklewski, G.; Schmidtke, A.; Hegerl, U. Preference of lethal methods is not the only cause for higher suicide rates in males. J. Affect. Disord. 2012, 136, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Smith, P.N.; Cukrowicz, K.C. Capable of Suicide: A Functional Model of the Acquired Capability Component of the Interpersonal-Psychological Theory of Suicide. Suicide Life Threat. Behav. 2010, 40, 266–275. [Google Scholar] [CrossRef] [PubMed]
- Choi, N.G.; Dinitto, D.M.; Marti, C.N.; Kaplan, M.S. Older Suicide Decedents: Intent Disclosure, Mental and Physical Health, and Suicide Means. Am. J. Prev. Med. 2017, 53, 772–780. [Google Scholar] [CrossRef]
- Hemenway, D. Comparing gun-owning vs non-owning households in terms of firearm and non-firearm suicide and suicide attempts. Prev. Med. 2019, 119, 14–16. [Google Scholar] [CrossRef]
- Cano-Montalbán, I.; Quevedo-Blasco, R. Sociodemographic Variables Most Associated with Suicidal Behaviour and Suicide Methods in Europe and America. A Systematic Review. Eur. J. Psychol. Appl. Leg. Context 2018, 10, 15–25. [Google Scholar] [CrossRef]
- Choi, N.G.; Dinitto, D.M.; Sagna, A.O.; Marti, C.N. Older women who died by suicide: Suicide means, sociodemographic and psychiatric risk factors, and other precipitating circumstances. Int. Psychogeriatr. 2018, 30, 1531–1540. [Google Scholar] [CrossRef]
- Vasiliadis, H.M.; Lamoureux-Lamarche, C.; Guerra, S.G. Gender and age group differences in suicide risk associated with co-morbid physical and psychiatric disorders in older adults. Int. Psychogeriatr. 2017, 29, 249–257. [Google Scholar] [CrossRef]
- Almeida, O.P.; McCaul, K.; Hankey, G.J.; Yeap, B.B.; Golledge, J.; Flicker, L. Suicide in older men: The health in men cohort study (HIMS). Prev. Med. 2016, 20, 33–38. [Google Scholar] [CrossRef]
- Fässberg, M.M.; Cheung, G.; Canetto, S.S.; Erlangsen, A.; Lapierre, S.; Lindner, R.; Draper, B.; Gallo, J.J.; Wong, C.; Wu, J.; et al. A systematic review of physical illness, functional disability, and suicidal behaviour among older adults. Aging Ment. Health 2016, 20, 166–194. [Google Scholar] [CrossRef]
- Freeman, D.; Freeman, J. The Stressed Sex: Uncovering the Truth About Men, Women, and Mental Health, 1st ed.; Oxford University Press: Oxford, UK, 2013. [Google Scholar]
- Choi, N.G.; Dinitto, D.M.; Marti, C.N.; Kaplan, M.S.; Conwell, Y. Suicide means among decedents aged 50+ Years, 2005–2014: Trends and associations with sociodemographic and precipitating factors. Am. J. Geriatr. Psychiatry 2017, 25, 1404–1414. [Google Scholar] [CrossRef] [PubMed]
- De Leo, D.; Draper, B.M.; Snowdon, J.; Kõlves, K. Suicides in older adults: A case-control psychological autopsy study in Australia. J. Psychiatr. Res. 2013, 47, 980–988. [Google Scholar] [CrossRef] [PubMed]
- Fässberg, M.M.; van Orden, K.A.; Duberstein, P.; Erlangsen, A.; Lapierre, S.; Bodner, E.; Canetto, S.S.; De Leo, D.; Szanto, K.; Waern, M. A Systematic Review of Social Factors and Suicidal Behavior in Older Adulthood. Int. J. Environ. Res. Public Health 2012, 9, 722–745. [Google Scholar] [CrossRef] [PubMed]
- Canetto, S.S. Suicide: Why Are Older Men So Vulnerable? Men Masc. 2017, 20, 49–70. [Google Scholar] [CrossRef]
- Canetto, S.S.; Cleary, A. Men, masculinities and suicidal behavior. Soc. Sci. Med. 2012, 74, 461–465. [Google Scholar] [CrossRef] [PubMed]
- De Leo, D. Ageism and suicide prevention. Lancet Psychiatry 2018, 5, 192–193. [Google Scholar] [CrossRef]
- Rasmussen, M.L.; Haavind, H.; Dieserud, G. Young Men, Masculinities, and Suicide. Arch. Suicide Res. 2018, 22, 327–343. [Google Scholar] [CrossRef]
- Kimura, A.; Hishimoto, A.; Otsuka, I.; Okazaki, S.; Boku, S.; Horai, T.; Izumi, T.; Takahashi, M.; Ueno, Y.; Shirakawa, O.; et al. Loss of chromosome Y in blood, but not in brain, of suicide completers. PLoS ONE 2018, 13, e0190667. [Google Scholar] [CrossRef]


{kind=link}
| Method | Description | ICD-10 | ICD-9 |
|---|---|---|---|
| Poisoning by drugs | Self-inflicted poisoning with psychotropic drugs, narcotics, or other drugs; or non-dependent substance abuse | X60, X61, X62, X63, X64 | E950, E980, 305 (305.4, 305.8), 969 |
| Poisoning by other means | Intentional self-inflicted poisoning by exposure to alcohol, gases, chemical products, etc. | X65, X66, X67, X68, X69 | E951, E952, E981, E982 |
| Hanging | Intentional self-inflicted harm by hanging, strangulation, suffocation, including cases when its accidental or intentional nature is unknown | X70 | E953, E983 |
| Drowning | Intentional self-inflicted harm by drowning and submersion, including cases when its accidental or intentional nature is unknown | X71 | E954, E984 |
| Firearms | Intentional self-inflicted harm by firearm, including cases when its accidental or intentional nature is unknown | X72, X73, X74, X75 | E955, E985 |
| Sharp objects | Intentional self-inflicted harm by cutting or sharp object, including cases when its accidental or intentional nature is unknown | X78, X79 | E956, E986 |
| Jumping | Intentional self-inflicted harm by jumping from a high place, including cases when its accidental or intentional nature is unknown | X80 | E957, E987 |
| Other methods | Intentional self-inflicted harm by non-specified means, vehicles, fire, or vapors; including cases when its accidental or intentional nature is unknown | X76, X77, X81, X82, X83, X84 | E958, E988 |
| Variable | Suicide N = 5202 (n) | Attempted Suicides N = 20,254 (n) | Suicide Rates Per 100,000 Inhabitants | Attempted Suicide Rates Per 100,000 Inhabitants | Attempted Suicide to Suicide Rate | |
|---|---|---|---|---|---|---|
| Sex | Females | 1130 | 10,821 | 4.6 | 43.6 | 9.58 |
| Males | 4072 | 9433 | 17.0 | 39.3 | 2.32 | |
| Year | 2007 | 708 | 2542 | 10.5 | 37.6 | 3.59 |
| 2008 | 822 | 2939 | 12.0 | 42.7 | 3.58 | |
| 2009 | 749 | 2922 | 10.8 | 42.0 | 3.90 | |
| 2010 | 685 | 2784 | 9.8 | 39.7 | 4.06 | |
| 2011 | 651 | 2861 | 9.2 | 40.6 | 4.39 | |
| 2012 | 781 | 2925 | 11.0 | 41.4 | 3.75 | |
| 2013 | 806 | 3281 | 11.4 | 46.5 | 4.07 | |
| Age | 15–29 | 509 | 4087 | 4.4 | 35.6 | 8.03 |
| 30–39 | 794 | 5112 | 8.1 | 52.1 | 6.44 | |
| 40–44 | 511 | 2890 | 10.8 | 60.8 | 5.66 | |
| 45–49 | 494 | 2396 | 11.3 | 55.0 | 4.85 | |
| 50–54 | 467 | 1893 | 12.6 | 51.0 | 4.05 | |
| 55–59 | 389 | 1089 | 12.6 | 35.2 | 2.80 | |
| 60–64 | 372 | 762 | 13.2 | 27.0 | 2.05 | |
| 65–69 | 317 | 572 | 13.1 | 23.7 | 1.80 | |
| 70–74 | 382 | 444 | 17.9 | 20.8 | 1.16 | |
| 75–79 | 400 | 360 | 20.7 | 18.6 | 0.90 | |
| 80-84 | 332 | 325 | 25.3 | 24.8 | 0.98 | |
| ≥85 | 235 | 324 | 24.5 | 33.8 | 1.38 | |
| Variable | Poisson Adjusted Model | ||
|---|---|---|---|
| Suicide IRR (95% CI) | Attempted Suicide IRR (95% CI) | ||
| Sex | Females | Reference | Reference |
| Males | 4.02 c (3.76;4.29) | 0.88c (0.86;0.91) | |
| Year | 2007 | Reference | Reference |
| 2008 | 1.13 a (1.02;1.25) | 1.13 c (1.07;1.19) | |
| 2009 | 1.02 (0.92;1.12) | 1.11 c (1.05;1.17) | |
| 2010 | 0.91 (0.82;1.02) | 1.05 (0.99;1.1) | |
| 2011 | 0.86 b (0.77;0.95) | 1.07 a (1.01;1.13) | |
| 2012 | 1.01 (0.92;1.12) | 1.09 b (1.03;1.15) | |
| 2013 | 1.04 (0.94;1.15) | 1.22 c (1.16;1.28) | |
| Age | 15–29 | Reference | Reference |
| 30–39 | 1.84 c (1.64;2.05) | 1.45 c (1.39;1.52) | |
| 40–44 | 2.45 c (2.17;2.77) | 1.7 c (1.61;1.78) | |
| 45–49 | 2.59 c (2.29;2.93) | 1.53 c (1.46;1.62) | |
| 50–54 | 2.89 c (2.55;3.28) | 1.43 c (1.35;1.51) | |
| 55–59 | 2.9 c (2.55;3.31) | 0.98 (0.92;1.05) | |
| 60–64 | 3.08 c (2.69;3.52) | 0.74 c (0.68;0.8) | |
| 65–69 | 3.1 c (2.69;3.56) | 0.66 c (0.6;0.72) | |
| 70–74 | 4.29 c (3.76;4.9) | 0.58 c (0.52;0.64) | |
| 75–79 | 5.12 c (4.49;5.84) | 0.52 c (0.47;0.58) | |
| 80–84 | 6.6 c (5.74;7.58) | 0.69 c (0.61;0.78) | |
| ≥85 | 7.06 c (6.04;8.24) | 0.93 (0.82;1.05) | |
| Age (years) | Suicide | Attempted Suicide | ||
|---|---|---|---|---|
| Females | Males | Females | Males | |
| IRR (95% CI) | IRR (95% CI) | |||
| 15–29 | Reference | Reference | Reference | Reference |
| 30–39 | 2.01 c (1.55;2.6) | 1.80 c (1.59;2.04) | 1.38 c (1.3;1.47) | 1.53 c (1.44;1.63) |
| 40–44 | 2.79 c (2.11;3.69) | 2.38 c (2.08;2.73) | 1.64 c (1.53;1.76) | 1.76 c (1.64;1.89) |
| 45–49 | 2.88 c (2.17;3.83) | 2.53 c (2.20;2.90) | 1.64 c (1.52;1.76) | 1.42 c (1.31;1.54) |
| 50–54 | 3.54 c (2.67;4.68) | 2.74 c (2.38;3.16) | 1.58 c (1.46;1.7) | 1.26 c (1.15;1.37) |
| 55–59 | 3.83 c (2.88;5.1) | 2.69 c (2.32;3.12) | 1.01 (0.92;1.11) | 0.95 (0.85;1.05) |
| 60–64 | 4.13 c (3.1;5.49) | 2.83 c (2.43;3.29) | 0.79 c (0.71;0.88) | 0.68 c (0.6;0.77) |
| 65–69 | 4.48 c (3.35;5.98) | 2.75 c (2.34;3.24) | 0.72 c (0.64;0.81) | 0.58 c (0.5;0.67) |
| 70–74 | 4.75 c (3.55;6.35) | 4.18 c (3.60;4.86) | 0.55 c (0.48;0.63) | 0.61 c (0.53;0.72) |
| 75–79 | 4.22 c (3.11;5.72) | 5.43 c (4.70;6.28) | 0.5 c (0.43;0.59) | 0.55 c (0.46;0.65) |
| 80–84 | 4.58 c (3.3;6.34) | 7.39 c (6.34;8.60) | 0.56 c (0.47;0.65) | 0.93 (0.79;1.11) |
| >=85 | 4.71 c (3.33;6.65) | 8.32 c (7.00;9.90) | 0.81 b (0.69;0.94) | 1.22 (1;1.49) |
| Method | Sex | Suicide N = 5202 | Attempted Suicide N = 6306 | Suicide IRR (95% CI) | Attempted Suicide IRR (95% CI) | ||
|---|---|---|---|---|---|---|---|
| n | % | n | % | ||||
| Poisoning by drugs | Males Females | 205 168 | 55.0 45.0 | 2106 3041 | 40.9 59.1 | Reference 0.84 (0.68, 1.02) | Reference 1.47 (1.40, 1.55) |
| Poisoning by other means | Males Females | 145 85 | 63.0 37.0 | 34 18 | 65.4 34.6 | Reference 0.66 (0.50, 0.87) | Reference 0.57 (0.32, 1.02) |
| Hanging | Males Females | 2616 398 | 86.8 13.2 | 302 115 | 72.4 27.6 | Reference 0.16 (0.14, 0.17) | Reference 0.39 (0.31, 0.48) |
| Drowning | Males Females | 60 40 | 60.0 40.0 | 12 7 | 63.2 36.8 | Reference 0.59 (0.39, 0.90) | Reference 0.51 (0.19, 1.36) |
| Firearms | Males Females | 276 10 | 96.5 3.5 | 45 13 | 77.6 22.4 | Reference 0.04 (0.02, 0.79) | Reference 0.34 (0.18, 0.64) |
| Sharp objects | Males Females | 93 21 | 81.6 18.4 | 144 89 | 61.8 38.2 | Reference 0.23 (0.14, 0.37) | Reference 0.63 (0.48, 0.82) |
| Jumping | Males Females | 588 373 | 61.2 38.8 | 126 68 | 64.9 35.1 | Reference 0.64 (0.57, 0.74) | Reference 0.55 (0.41, 0.74) |
| Other methods | Males Females | 108 40 | 73.0 27.0 | 146 140 | 51.0 49.0 | Reference 0.38 (0.26, 0.54) | Reference 0.98 (0.77, 1.23) |
| Total | Males Females | 4091 1135 | 78.3 21.7 | 2915 3491 | 45.5 54.5 | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mejías-Martín, Y.; Luna del Castillo, J.d.D.; Rodríguez-Mejías, C.; Martí-García, C.; Valencia-Quintero, J.P.; García-Caro, M.P. Factors Associated with Suicide Attempts and Suicides in the General Population of Andalusia (Spain). Int. J. Environ. Res. Public Health 2019, 16, 4496. https://doi.org/10.3390/ijerph16224496
Mejías-Martín Y, Luna del Castillo JdD, Rodríguez-Mejías C, Martí-García C, Valencia-Quintero JP, García-Caro MP. Factors Associated with Suicide Attempts and Suicides in the General Population of Andalusia (Spain). International Journal of Environmental Research and Public Health. 2019; 16(22):4496. https://doi.org/10.3390/ijerph16224496
Chicago/Turabian StyleMejías-Martín, Yolanda, Juan de Dios Luna del Castillo, Candela Rodríguez-Mejías, Celia Martí-García, Juan Pablo Valencia-Quintero, and María Paz García-Caro. 2019. "Factors Associated with Suicide Attempts and Suicides in the General Population of Andalusia (Spain)" International Journal of Environmental Research and Public Health 16, no. 22: 4496. https://doi.org/10.3390/ijerph16224496
APA StyleMejías-Martín, Y., Luna del Castillo, J. d. D., Rodríguez-Mejías, C., Martí-García, C., Valencia-Quintero, J. P., & García-Caro, M. P. (2019). Factors Associated with Suicide Attempts and Suicides in the General Population of Andalusia (Spain). International Journal of Environmental Research and Public Health, 16(22), 4496. https://doi.org/10.3390/ijerph16224496