Canine-Assisted Therapy Improves Well-Being in Nurses

 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Methods
2.1. Participants
2.2. Measures
2.3. General Procedures
2.4. Therapy Dog
2.5. Data Analysis
3. Results
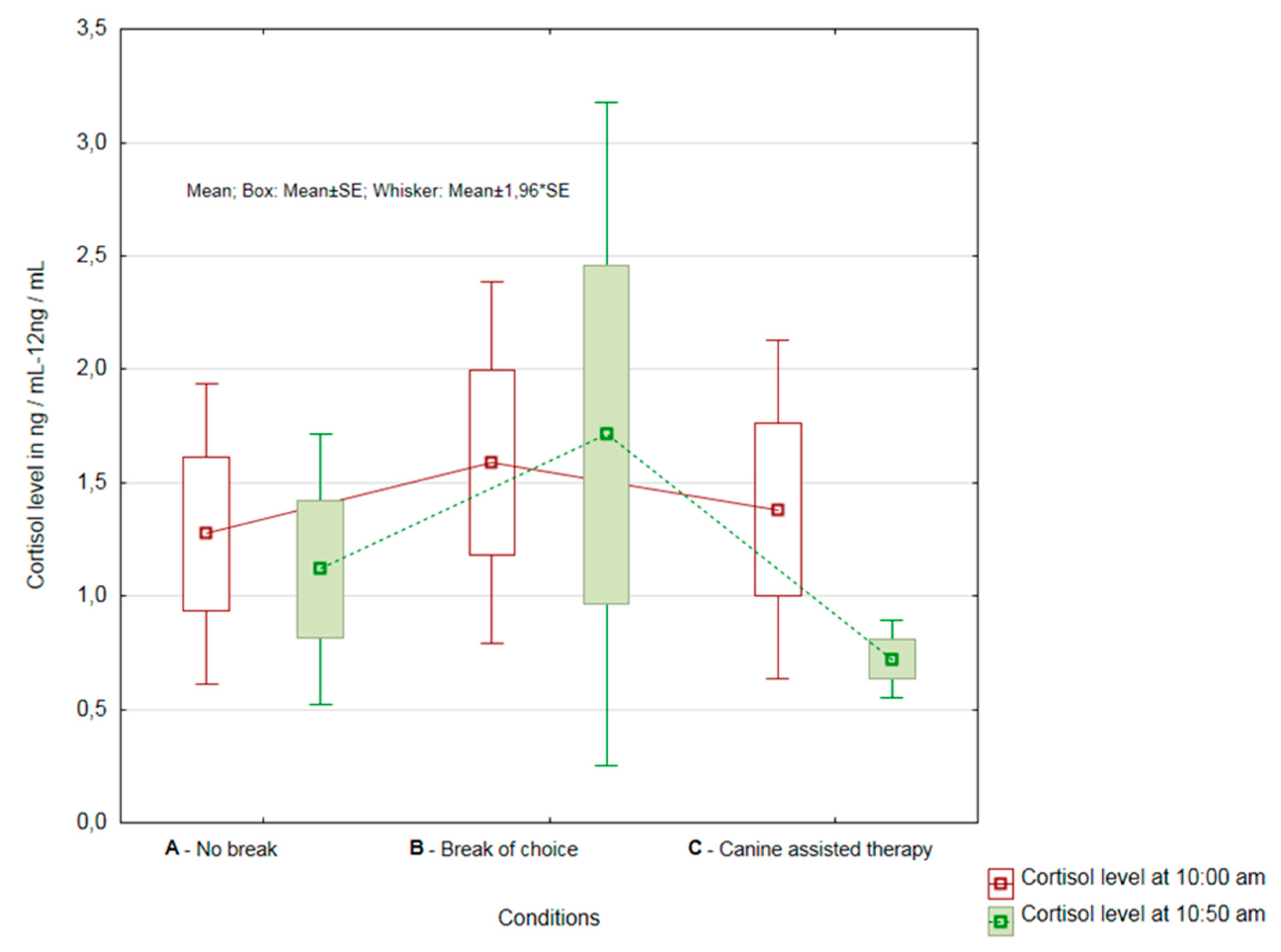
3.1. Overall Results of Cortisol Change Evaluation
3.2. Comparison of Results by the Department of Healthcare Providers
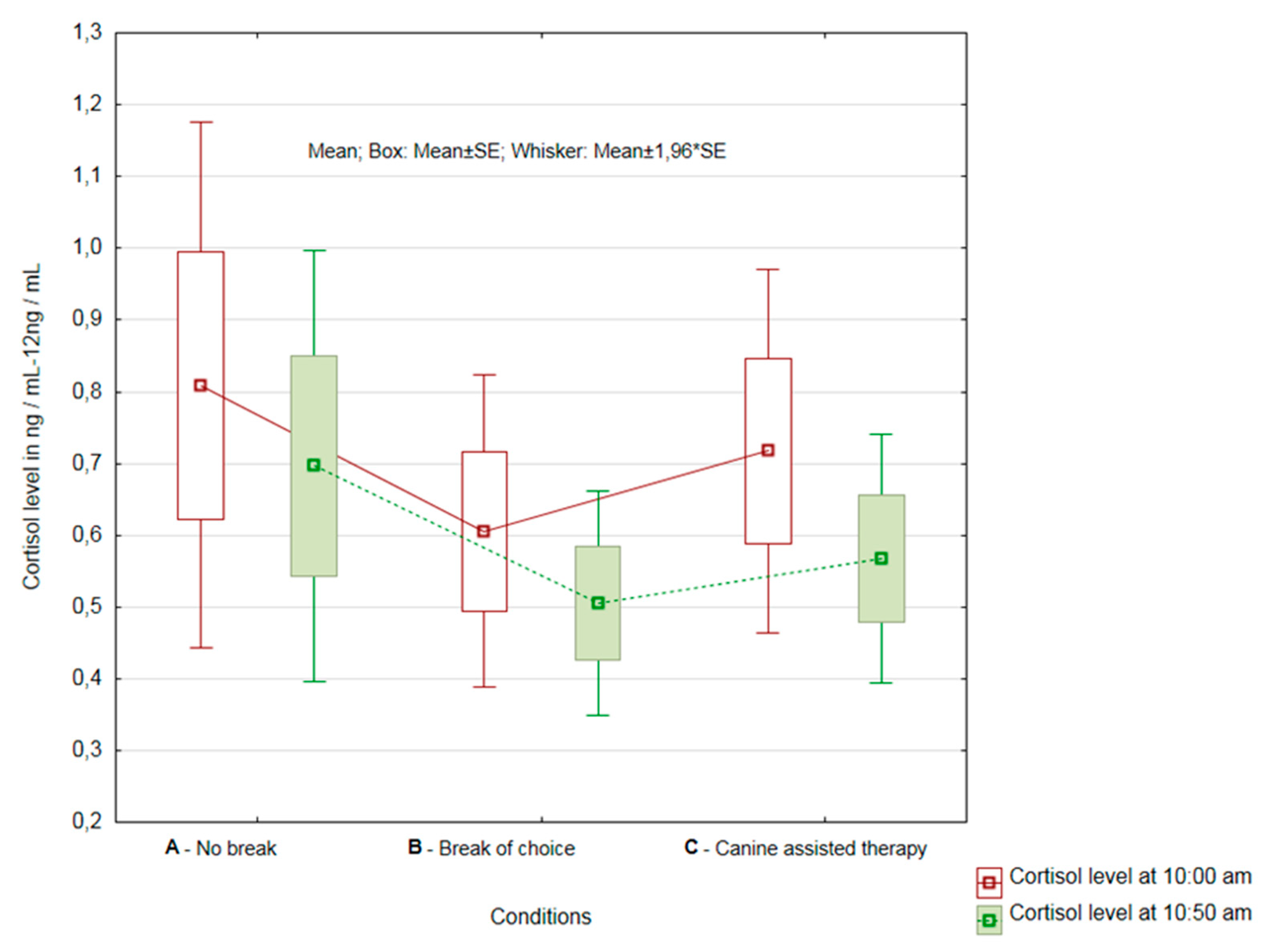
3.2.1. Healthcare Providers from the Department of Rehabilitation
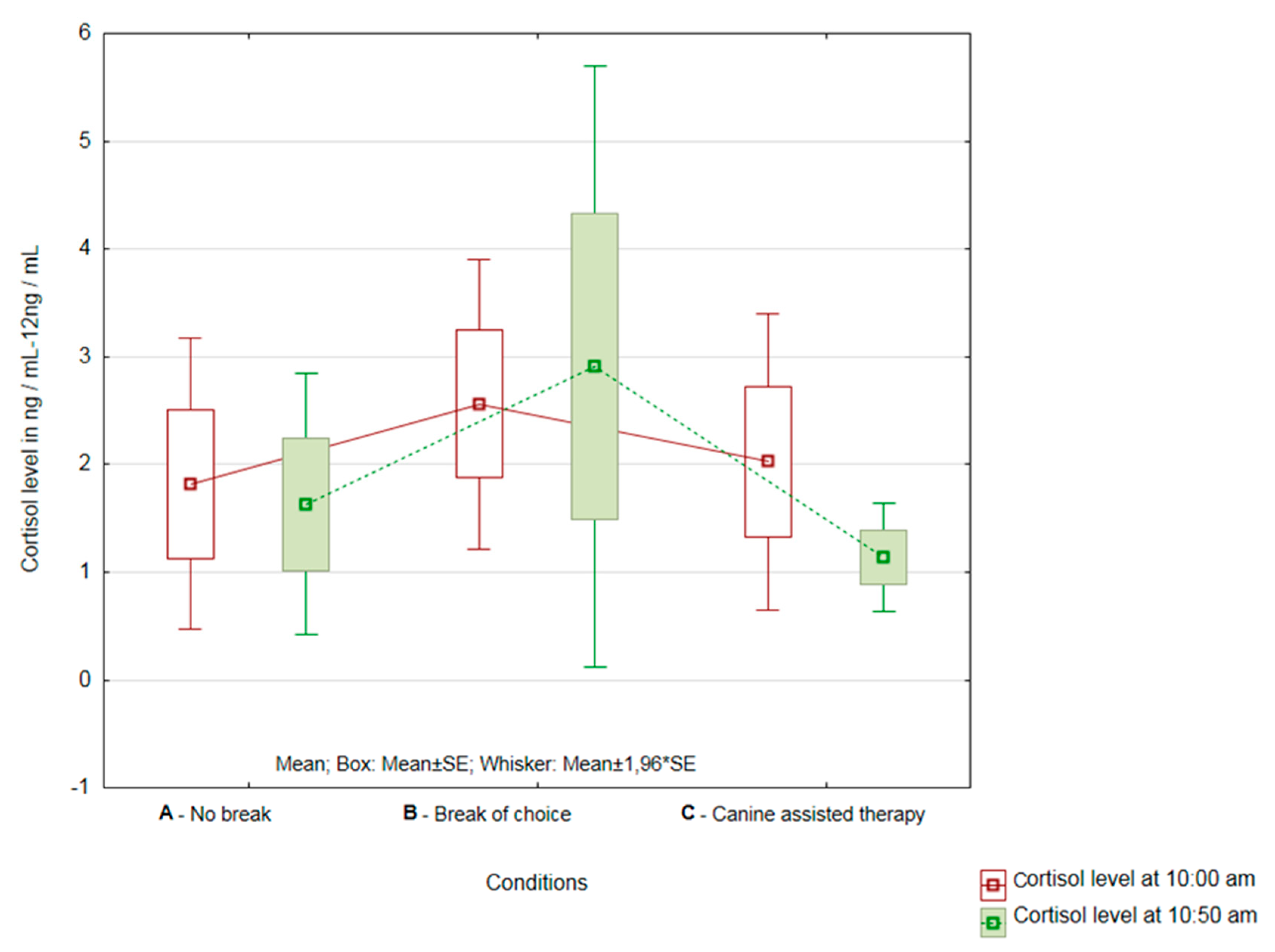
3.2.2. Healthcare Providers from the Department of Internal and Long-Term Care
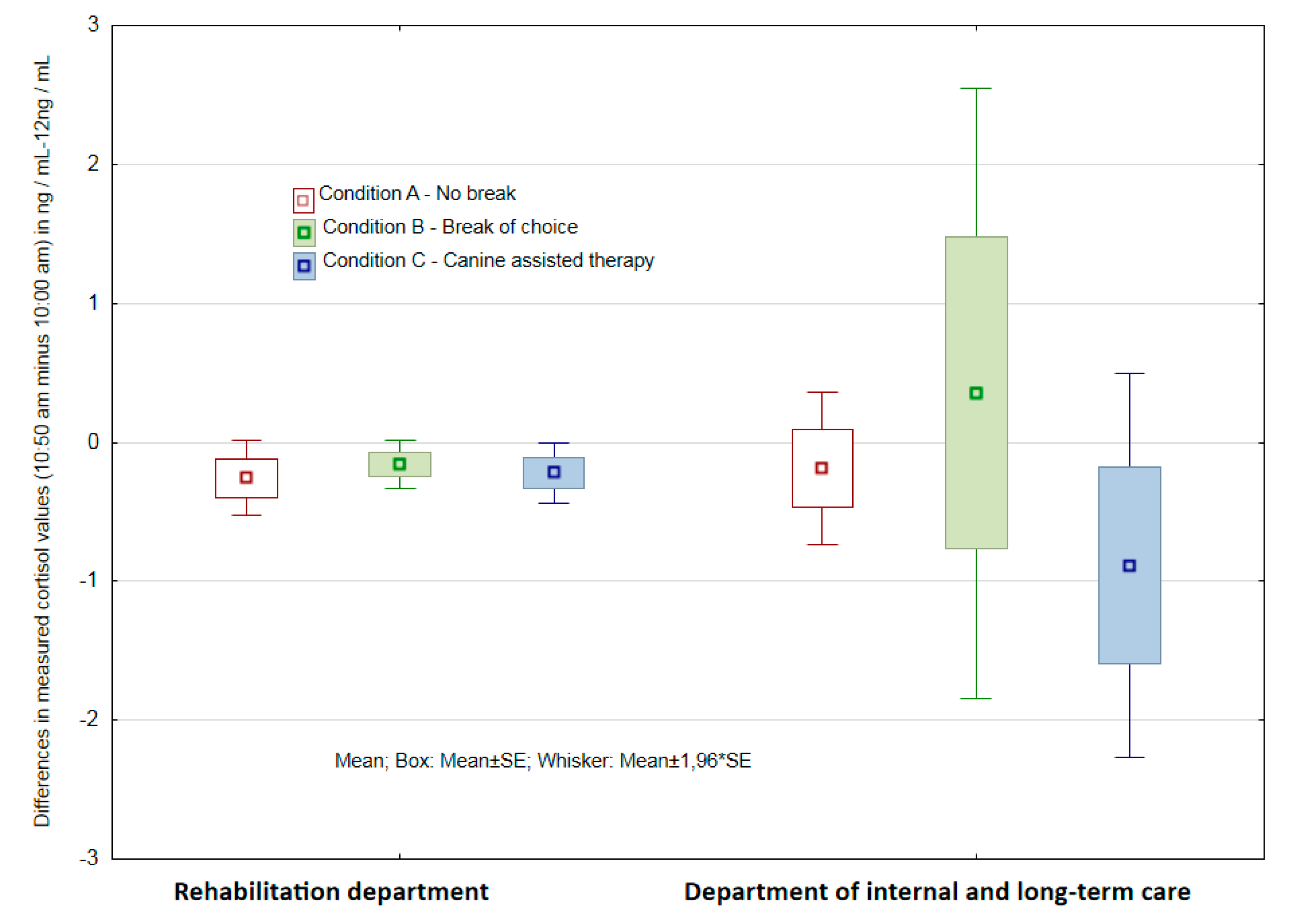
3.2.3. Assessment of the Significance of Differences in Results of both Groups of Respondent-Departments
4. Discussion
5. Limits
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Salak-Johnson, J.L.; McGlone, J.J. Making sense of apparently conflicting data: Stress and immunity in swine and cattle1. J. Anim. Sci. 2007, 85, E81–E88. [Google Scholar] [CrossRef] [PubMed]
- Matheny, J.; Le Fevre, M.; Kolt, G.S. Eustress, distress, and interpretation in occupational stress. J. Manag. Psychol. 2003, 18, 726–744. [Google Scholar]
- Nelson, D.L.; Simmons, B.L. Eustress: An Elusive Construct, an Engaging Pursuit. Emotional and Physiological Processes and Positive Intervention Strategies; Emerald Group Publishing Limited: Bingley, UK, 2003; pp. 265–322. [Google Scholar]
- Kupriyanov, R.; Zhdanov, R. The eustress concept: Problems and outlooks. World J. Med. Sci. 2014, 11, 179–185. [Google Scholar]
- Kolt, G.; Matheny, J.; Le Fevre, M. Eustress, distress and their interpretation in primary and secondary occupational stress management interventions: Which way first? J. Manag. Psychol. 2006, 21, 547–565. [Google Scholar]
- Garkavi, L.K.H.; Kvakina, Y.E.B.; Kuz’menko, T.S. Antistress Reactions and Activation Therapy; Imedis: Мoskva, Russia, 1998. [Google Scholar]
- Gerhart, J.I.; Canetti, D.; Hobfoll, S.E. Traumatic Stress in Overview: Definition, Context, Scope, and Long-Term Outcomes. In Traumatic Stress and Long-Term Recovery; Springer Science and Business Media LLC: Berlin, Germany, 2015; pp. 3–24. [Google Scholar]
- Andrews, J.; Ali, N.; Pruessner, J.C. Reflections on the interaction of psychogenic stress systems in humans: The stress coherence/compensation model. Psychoneuroendocrinology 2013, 38, 947–961. [Google Scholar] [CrossRef] [PubMed]
- Dobnik, M.; Maletič, M.; Skela-Savič, B. Work-Related Stress Factors in Nurses at Slovenian Hospitals—A Cross-sectional Study. Slov. J. Public Health 2018, 57, 192–200. [Google Scholar] [CrossRef]
- Maphangela, T.; Matenge, S. PW 2280 Factors associated with occupational stress among nurses working in government clinics in gaborone, botswana. Injury Prev. 2018, 24 (Suppl. 2), A215. [Google Scholar]
- Kiank, C.; Entleutner, M.; Fürll, B.; Westerholt, A.; Heidecke, C.-D.; Schütt, C. Stress-induced immune conditioning affects the course of experimental peritonitis. Shock 2007, 27, 305–311. [Google Scholar] [CrossRef]
- Glaser, R.; Kiecolt-Glaser, J.K. Stress-induced immune dysfunction: Implications for health. Nat. Rev. Immunol. 2005, 5, 243–251. [Google Scholar] [CrossRef]
- Machová, K.; Procházková, R.; Eretová, P.; Svobodová, I.; Kotík, I. Effect of Animal-Assisted Therapy on Patients in the Department of Long-Term Care: A Pilot Study. Int. J. Environ. Res. Public Health 2019, 16, 1362. [Google Scholar] [CrossRef]
- Hoffmann, A.O.; Lee, A.H.; Wertenauer, F.; Ricken, R.; Jansen, J.J.; Gallinat, J.; Lang, U.E. Dog-assisted intervention significantly reduces anxiety in hospitalized patients with major depression. Eur. J. Integr. Med. 2009, 1, 145–148. [Google Scholar] [CrossRef]
- Lass-Hennemann, J.; Schäfer, S.K.; Römer, S.; Holz, E.; Streb, M.; Michael, T. Therapy Dogs as a Crisis Intervention After Traumatic Events?—An Experimental Study. Front. Psychol. 2018, 9, 1627. [Google Scholar] [CrossRef] [PubMed]
- Beetz, A.; Kotrschal, K.; Turner, D.C.; Hediger, K.; Uvnäs-Moberg, K.; Julius, H. The Effect of a Real Dog, Toy Dog and Friendly Person on Insecurely Attached Children During a Stressful Task: An Exploratory Study. Anthrozoös 2011, 24, 349–368. [Google Scholar] [CrossRef]
- Mills, D.; Hall, S. Animal-assisted interventions: Making better use of the human-animal bond. Vet. Rec. 2014, 174, 269–273. [Google Scholar] [CrossRef] [PubMed]
- Giuliani, F.; Jacquemettaz, M. Animal-assisted therapy used for anxiety disorders in patients with learning disabilities: An observational study. Eur. J. Integr. Med. 2017, 14, 13–19. [Google Scholar] [CrossRef]
- Zilcha-Mano, S.; Mikulincer, M.; Shaver, P.R. Pet in the therapy room: An attachment perspective on Animal-Assisted Therapy. Attach. Hum. Dev. 2011, 13, 541–561. [Google Scholar] [CrossRef] [PubMed]
- Kaminski, M.; Pellino, T.; Wish, J. Play and Pets: The Physical and Emotional Impact of Child-Life and Pet Therapy on Hospitalized Children. Child. Health Care 2002, 31, 321–335. [Google Scholar] [CrossRef]
- Veiga, G.; Rodrigues, A.D.; Lamy, E.; Guiose, M.; Pereira, C.; Marmeleira, J. The effects of a relaxation intervention on nurses’ psychological and physiological stress indicators: A pilot study. Complement. Ther. Clin. Pract. 2019, 35, 265–271. [Google Scholar] [CrossRef] [PubMed]
- Hellhammer, D.H.; Wüst, S.; Kudielka, B.M. Salivary cortisol as a biomarker in stress research. Psychoneuroendocrinology 2009, 34, 163–171. [Google Scholar] [CrossRef]
- Vincent, I.; Michell, A. Comparison of cortisol concentrations in saliva and plasma of dogs. Res. Vet. Sci. 1992, 53, 342–345. [Google Scholar] [CrossRef]
- Inder, W.J.; Dimeski, G.; Russell, A. Measurement of salivary cortisol in 2012—Laboratory techniques and clinical indications. Clin. Endocrinol. 2012, 77, 645–651. [Google Scholar] [CrossRef]
- Owen, L.J.; Haslam, S.; E Adaway, J.; Wood, P.; Glenn, C.; Keevil, B.G. A simplified liquid chromatography tandem mass spectrometry assay, using on-line solid-phase extraction, for the quantitation of cortisol in saliva and comparison with a routine DELFIA method. Ann. Clin. Biochem. Int. J. Lab. Med. 2010, 47, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Hannibal, K.E.; Bishop, M.D. Chronic stress, cortisol dysfunction, and pain: A psychoneuroendocrine rationale for stress management in pain rehabilitation. Phys. Ther. 2014, 94, 1816–1825. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, K.E.; Bryce, C.I.; Granger, D.A.; O’Haire, M.E. The effect of a service dog on salivary cortisol awakening response in a military population with posttraumatic stress disorder (PTSD). Psychoneuroendocrinology 2018, 98, 202–210. [Google Scholar] [CrossRef] [PubMed]
- Eley, D.; Eley, R.; Bertello, M.; Rogers-Clark, C. Why did I become a nurse? Personality traits and reasons for entering nursing. J. Adv. Nurs. 2012, 68, 1546–1555. [Google Scholar] [CrossRef] [PubMed]
- Hart, P.D. The Nurse Shortage: Perspectives from Current Direct Care Nurses and Former Direct Care Nurses; Peter D. Hart Research Associates; The Federation of Nurses and Health Professionals: Washington, DC, USA, 2001; Volume 20. [Google Scholar]
- Pereira, S.M.; Fonseca, A.M.; Carvalho, A.S. Burnout in nurses working in Portuguese palliative care teams: A mixed methods study. Int. J. Palliat. Nurs. 2012, 18, 373–381. [Google Scholar] [CrossRef]
- Diehl, E.; Rieger, S.; Gutendorf, M.; Geißler, B.; Letzel, S.; Pinzon, L.E. Belastungsfaktoren von Pflegekräften in der spezialisierten Palliativversorgung—Ergebnisse einer qualitativen Studie. Z. Palliativmedizin 2018, 19, 306–311. [Google Scholar] [CrossRef]
- Vinothkumar, M.; Arathi, A.; Joseph, M.; Nayana, P.; Jishma, E.J.; Sahana, U. Coping, perceived stress, and job satisfaction among medical interns: The mediating effect of mindfulness. Ind. Psychiatry J. 2016, 25, 195–201. [Google Scholar] [CrossRef]
- Hämmig, O. Explaining burnout and the intention to leave the profession among health professionals—A cross-sectional study in a hospital setting in Switzerland. BMC Health Serv. Res. 2018, 18, 785. [Google Scholar] [CrossRef]
- Crane, P.J.; Ward, S.F. Self-Healing and Self-Care for Nurses. AORN J. 2016, 104, 386–400. [Google Scholar] [CrossRef]
- Walsh, F. Human-Animal Bonds II: The Role of Pets in Family Systems and Family Therapy. Fam. Process. 2009, 48, 481–499. [Google Scholar] [CrossRef] [PubMed]
- Hediger, K.; Hund-Georgiadis, M. Animal-assisted therapy in the view of staff member before and after implementation in a rehabilitation clinic. Hum.-Anim. Interation Bul 2017, 5, 61–73. [Google Scholar]
- Bukhari, G.M.J.; Shaista, H.; Abbasi, M.M.J. Frequency of depression in nurses working in various departments of a federal government hospital of Islamabad. Pak. J. Public Health 2016, 6, 41–44. [Google Scholar]
- Letvak, S.; Ruhm, C.J.; McCoy, T. Depression in Hospital-Employed Nurses. Clin. Nurse Spéc. 2012, 26, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Welsh, D. Predictors of Depressive Symptoms in Female Medical-Surgical Hospital Nurses. Issues Ment. Health Nurs. 2009, 30, 320–326. [Google Scholar] [CrossRef]
- Souter, M.A.; Miller, M.D.; Megan, A. Souter Department of Psychology Northern Arizona University USA, Michelle D. Miller Department of Psychology Northern Arizona University USACorrespondenceMichelle.Millernau.edu Do Animal-Assisted Activities Effectively Treat Depression? A Meta-Analysis. Anthrozoös 2007, 20, 167–180. [Google Scholar] [CrossRef]
- Li, J.; Bidlingmaier, M.; Petru, R.; Gil, F.P.; Loerbroks, A.; Angerer, P. Impact of shift work on the diurnal cortisol rhythm: A one-year longitudinal study in junior physicians. J. Occup. Med. Toxicol. 2018, 13, 23. [Google Scholar] [CrossRef]
- Copertaro, A.; Bracci, M.; Gesuita, R.; Carle, F.; Amati, M.; Baldassari, M.; Mocchegiani, E.; Santarelli, L. Influence of shift-work on selected immune variables in nurses. Ind. Health 2011, 49, 597–604. [Google Scholar] [CrossRef]
- Liu, W.W.; Pan, F.C.; Wen, P.C.; Chen, S.J.; Lin, S.H. Job Stressors and coping mechanisms among emergency department nurses in the Armed Force hospitals of Taiwan. Int. J. Hum. Soc. Scis 2010, 5, 10. [Google Scholar]





© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Machová, K.; Součková, M.; Procházková, R.; Vaníčková, Z.; Mezian, K. Canine-Assisted Therapy Improves Well-Being in Nurses. Int. J. Environ. Res. Public Health 2019, 16, 3670. https://doi.org/10.3390/ijerph16193670
Machová K, Součková M, Procházková R, Vaníčková Z, Mezian K. Canine-Assisted Therapy Improves Well-Being in Nurses. International Journal of Environmental Research and Public Health. 2019; 16(19):3670. https://doi.org/10.3390/ijerph16193670
Chicago/Turabian StyleMachová, Kristýna, Michaela Součková, Radka Procházková, Zdislava Vaníčková, and Kamal Mezian. 2019. "Canine-Assisted Therapy Improves Well-Being in Nurses" International Journal of Environmental Research and Public Health 16, no. 19: 3670. https://doi.org/10.3390/ijerph16193670
APA StyleMachová, K., Součková, M., Procházková, R., Vaníčková, Z., & Mezian, K. (2019). Canine-Assisted Therapy Improves Well-Being in Nurses. International Journal of Environmental Research and Public Health, 16(19), 3670. https://doi.org/10.3390/ijerph16193670