Fissure Depth and Caries Incidence in First Permanent Molars: A Five-Year Follow-Up Study in Schoolchildren

 ,
, 


Abstract
1. Introduction
2. Materials and Methods
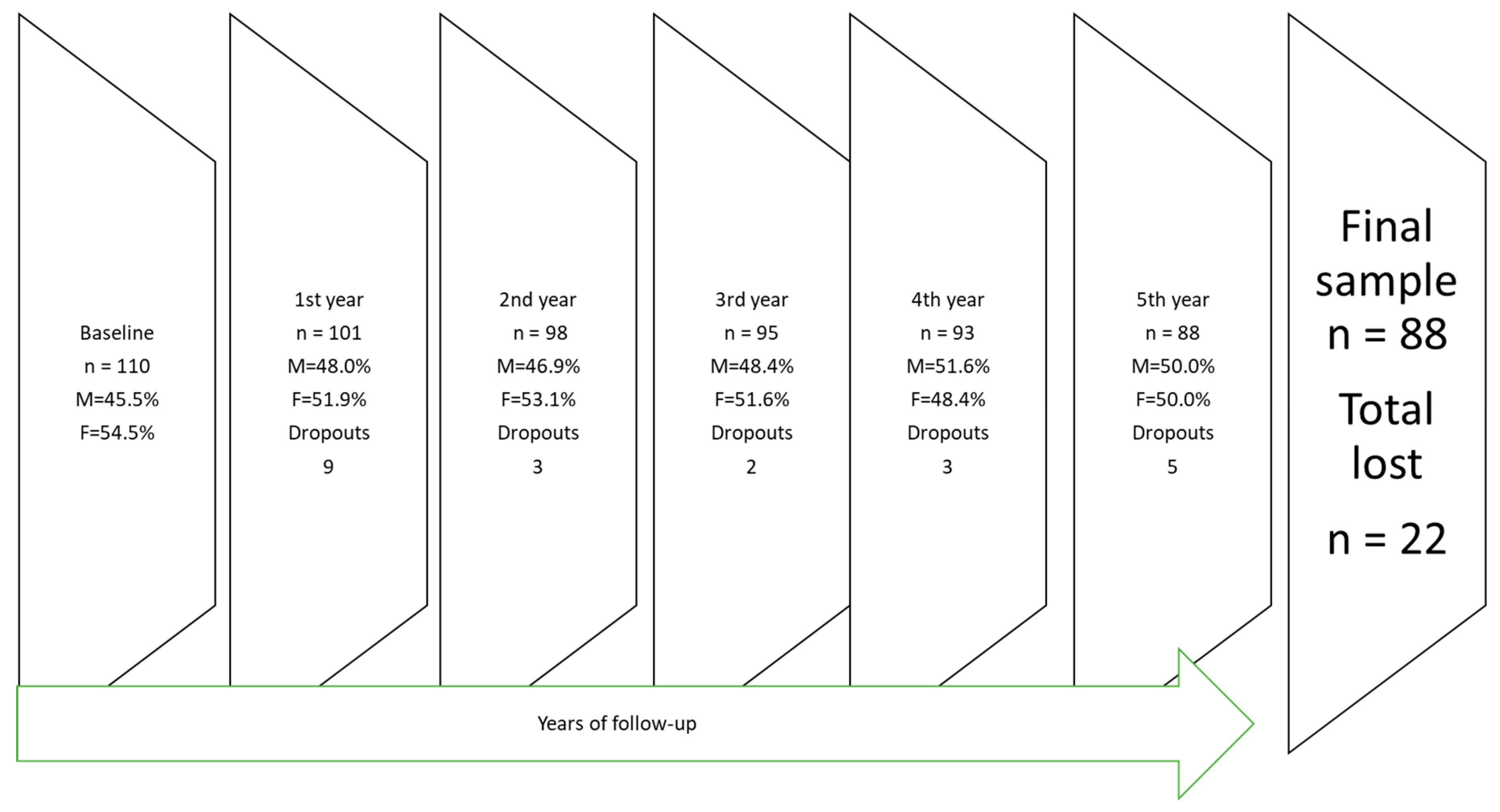
2.1. Participants
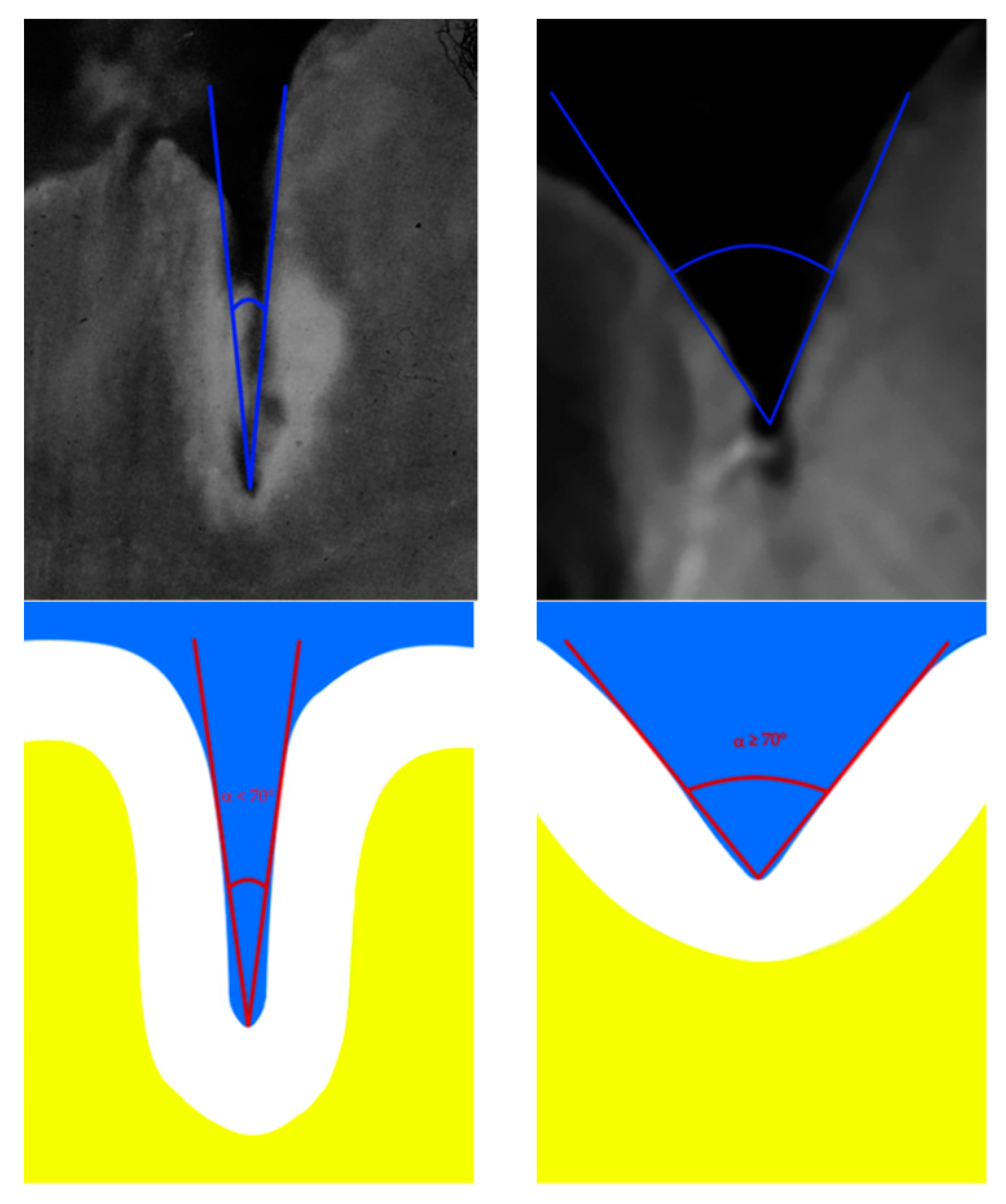
2.2. Fissure Depth
2.3. Calibration
2.4. Caries and Oral Hygiene
2.5. Statistical Analysis
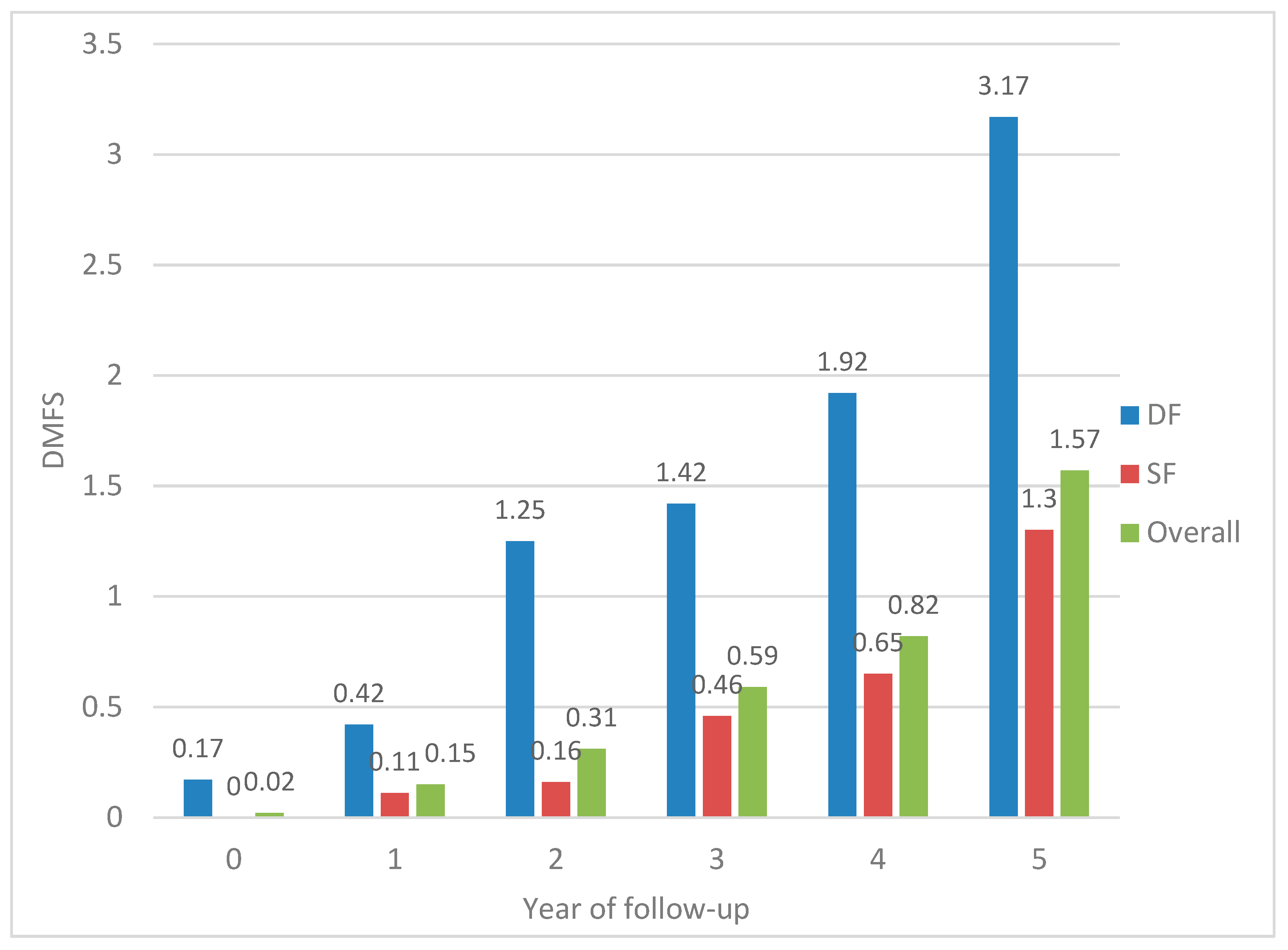
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Fejerskov, O. Changing paradigms in concepts on dental caries: Consequences for oral health care. Caries Res. 2004, 38, 182–191. [Google Scholar] [CrossRef] [PubMed]
- Doméjean, S.; Banerjee, A.; Featherstone, J.D.B. Caries risk/susceptibility assessment: Its value in minimum intervention oral healthcare. Br. Dent. J. 2017, 223, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Zero, D.T.; Fontana, M.; Martínez-Mier, E.A.; Ferreira-Zandoná, A.; Ando, M.; González-Cabezas, C.; Bayne, S. The biology, prevention, diagnosis and treatment of dental caries: Scientific advances in the United States. J. Am. Dent. Assoc. 2009, 140, 25S–34S. [Google Scholar] [CrossRef] [PubMed]
- Harris, R.; Nicoll, A.D.; Adair, P.M.; Pine, C.M. Risk factors for dental caries in young children: A systematic review of the literature. Community Dent. Health 2004, 21, 71–85. [Google Scholar] [PubMed]
- Leroy, R.; Bogaerts, K.; Martens, L.; Declerck, D. Risk factors for caries incidence in a cohort of Flemish preschool children. Clin. Oral Investig. 2012, 16, 805–812. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Bratthall, D.; Hänsel Petersson, G. Cariogram—A multifactorial risk assessment model for a multifactorial disease. Community Dent. Oral Epidemiol. 2005, 33, 256–264. [Google Scholar] [CrossRef] [PubMed]
- van Palenstein Helderman, W.H.; Mikx, F.H.; Van’t Hof, M.A.; Truin, G.; Kalsbeek, H. The value of salivary bacterial counts as a supplement to past caries experience as caries predictor in children. Eur. J. Oral Sci. 2001, 109, 312–315. [Google Scholar] [CrossRef] [PubMed]
- Frencken, J.E.; Peters, M.C.; Manton, D.J.; Leal, S.C.; Gordan, V.V.; Eden, E. Minimal intervention dentistry for managing dental caries—A review: Report of a FDI task group. Int. Dent. J. 2012, 62, 223–243. [Google Scholar] [CrossRef] [PubMed]
- Mejàre, I.; Axelsson, S.; Dahlén, G.; Espelid, I.; Norlund, A.; Tranæus, S.; Twetman, S. Caries risk assessment. A systematic review. Acta Odontol. Scand. 2014, 72, 81–91. [Google Scholar] [CrossRef] [PubMed]
- Lussi, A. Validity of diagnostic and treatment decisions of fissure caries. Caries Res. 1991, 25, 296–303. [Google Scholar] [CrossRef] [PubMed]
- Batchelor, P.A.; Sheiham, A. Grouping of tooth surfaces by susceptibility to caries: A study in 5–16 year-old children. BMC Oral Health 2004, 4, 2. [Google Scholar] [CrossRef] [PubMed]
- Fontana, M.; Zero, D.T. Assessing patients’ caries risk. J. Am. Dent. Assoc. 2006, 137, 1231–1239. [Google Scholar] [CrossRef] [PubMed]
- Nagano, T. Relation between the form of pit and fissure and the primary lesion of caries. Dent. Abstr. 1961, 6, 426. [Google Scholar]
- König, K.G. Dental morphology in relation to caries resistance with special reference to fissures as susceptible areas. J. Dent. Res. 1963, 42, 461–476. [Google Scholar] [CrossRef] [PubMed]
- Symons, A.L.; Chu, C.Y.; Meyers, I.A. The effect of fissure morphology and pretreatment of the enamel surface on penetration and adhesion of fissure sealants. J. Oral Rehabil. 1996, 23, 791–798. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Z.; Shaffer, J.R.; Wang, X.; Feingold, E.; Weeks, D.E.; Lee, M.; Cuenco, K.T.; Wendell, S.K.; Weyant, R.J.; Crout, R.; et al. Genome-wide association studies of pit-and-fissure- and smooth-surface caries in permanent dentition. J. Dent. Res. 2013, 92, 432–437. [Google Scholar] [CrossRef] [PubMed]
- Gao, X.L.; Hsu, C.Y.; Xu, Y.; Hwarng, H.B.; Loh, T.; Koh, D. Building caries risk assessment models for children. J. Dent. Res. 2010, 89, 637–643. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Oral Health Surveys-Basic Methods, 4th ed.; World Health Organization: Geneva, Switzerland, 1997. [Google Scholar]
- Greene, J.C.; Vermillion, J.R. The simplified oral hygiene index. J. Am. Dent. Assoc. 1964, 68, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Cui, J. QIC program and model selection in GEE analysis. Stata J. 2007, 7, 209–220. [Google Scholar] [CrossRef]
- Markovic, D.L.; Petrovic, B.B.; Peric, T.O.; Trisic, D.; Kojic, S.; Kuljic, B.L.; Stojanovic, G. Evaluation of sealant penetration in relation to fissure morphology, enamel surface preparation protocol and sealing material. Oral Health Prev. Dent. 2019, 17, 349–355. [Google Scholar]
- Rugarabamu, P.G.N.; Poulsen, S.; Masalu, J.R.P. A longitudinal study of occlusal caries among schoolchildren in Dar es Salaam, Tanzania. Community Dent. Oral Epidemiol. 2002, 30, 47–51. [Google Scholar] [CrossRef]
- Mackenzie, L.; Banerjee, A. The minimally invasive management of early occlusal caries: A practical guide. Prim. Dent. J. 2014, 3, 34–41. [Google Scholar] [CrossRef]
- Quaglio, J.M.; Sousa, M.B.; Ardenghi, T.M.; Mendes, F.M.; Imparato, J.C.; Pinheiro, S.L. Association between clinical parameters and the presence of active caries lesions in first permanent molars. Braz. Oral Res. 2006, 20, 358–363. [Google Scholar] [CrossRef]
- Shaffer, J.R.; Wang, X.; Desensi, R.S.; Wendell, S.; Weyant, R.J.; Cuenco, K.T.; Crout, R.; McNeil, D.W.; Marazita, M.L. Genetic susceptibility to dental caries on pit and fissure and smooth surfaces. Caries Res. 2012, 46, 38–46. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, J.C. Caries process on occlusal surfaces: Evolving evidence and understanding. Caries Res. 2014, 48, 339–346. [Google Scholar] [CrossRef]
- Carvalho, J.C.; Dige, I.; Machiulskiene, V.; Qvist, V.; Bakhshandeh, A.; Fatturi-Parolo, C.; Maltz, M. Occlusal caries: Biological approach for its diagnosis and management. Caries Res. 2016, 50, 527–542. [Google Scholar] [CrossRef]
- Loesche, W.J.; Straffon, L.H. Longitudinal investigation of the role of Streptococcus mutans in human fissure decay. Infect. Immun. 1979, 26, 498–507. [Google Scholar] [PubMed]
- Wang, J.D.; Chen, X.; Frencken, J.; Du, M.Q.; Chen, Z. Dental caries and first permanent molar pit and fissure morphology in 7-to 8-year-old children in Wuhan, China. Int. J. Oral Sci. 2012, 4, 157–160. [Google Scholar] [CrossRef][Green Version]
- Vehkalahti, M.M.; Solavaara, L.; Rytömaa, I. An eight-year follow-up of the occlusal surfaces of first permanent molars. J. Dent. Res. 1991, 70, 1064–1067. [Google Scholar] [CrossRef] [PubMed]
- Ripa, L.W.; Leske, G.S.; Varma, A.O. Longitudinal study of the caries susceptibility of occlusal and proximal surfaces of first permanent molars. J. Public Health Dent. 1988, 48, 8–13. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Year of Study | Present Teeth | Caries Indexes | ||
|---|---|---|---|---|
| Deciduous | Permanent | dmfs | DMFS | |
| Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | |
| Baseline | ||||
| Boys | 16.1 (2.5) | 6.7 (3.4) | 5.4 (8.5) | - |
| Girls | 15.5 (2.4) | 7.4 (2.8) | 5.1 (5.8) | 0.05 (0.2) |
| 1st year | ||||
| Boys | 13.6 (2.5) | 9.1 (3.0) | 5.8 (9.0) | 0.07 (0.3) * |
| Girls | 13.1 (2.5) | 10.1 (2.5) | 5.1 (5.9) | 0.2 (0.4) |
| 2nd year | ||||
| Boys | 12.1 (2.2) | 11.4 (2.5) | 5.4 (7.7) | 0.2 (0.5) |
| Girls | 11.5 (2.8) | 12.2 (2.8) | 4.7 (5.3) | 0.4 (1.3) |
| 3rd year | ||||
| Boys | 9.3 (3.7) | 14.2 (4.1) | 4.6 (7.0) | 0.4 (1.0) |
| Girls | 8.3 (4.4) | 15.6 (4.5) | 3.2 (4.8) | 0.8 (1.9) |
| 4th year | ||||
| Boys | 6.2 (4.0) | 17.7 (4.8) | 2.7 (5.6) | 0.7 (1.3) |
| Girls | 5.5 (4.8) | 18.7 (5.4) | 2.3 (4.1) | 1.0 (2.2) |
| 5th year | ||||
| Boys | 2.3 (3.2) | 23.1 (4.6) | 1.5 (4.1) | 1.5 (2.7) |
| Girls | 2.5 (3.0) | 22.8 (4.4) | 1.3 (3.1) | 1.6 (2.3) |
| 1st Molar (n = 88) | Year of Examination | |||||||
|---|---|---|---|---|---|---|---|---|
| Baseline | 1st | 2nd | 3rd | 4th | 5th | Total | % | |
| Caries Lesions | ||||||||
| Upper right | 0 | 0 | 1 | 3 | 1 | 6 | 11 | 12.5 |
| Upper left | 1 | 0 | 2 | 2 | 2 | 9 | 16 | 18.2 |
| Lower left | 2 | 2 | 4 | 4 | 2 | 8 | 22 | 25.0 |
| Lower right | 0 | 3 | 5 | 6 | 3 | 11 | 28 | 31.8 |
| Total | 3 | 5 | 12 | 15 | 8 | 34 | 77 | 21.9 |
| Fissure Depth | DMFS > 0 | DMFS ≥ 1 | p * | Total | |||
|---|---|---|---|---|---|---|---|
| n | (%) | n | (%) | n | (%) | ||
| Shallow | 46 | (60.5%) | 30 | (39.5%) | 0.023 | 76 | (86.4%) |
| Deep | 3 | (25.0%) | 9 | (75.0%) | 12 | (13.6%) | |
| Characteristic | Crude OR | (95% CI) | p |
| Age | 1.31 | (0.46, 3.72) | 0.648 |
| Sex (female) a | 1.36 | (0.75, 2.46) | 0.310 |
| S-OHI (>1.5) b | 1.83 | (0.92, 3.63) | 0.085 |
| dmfs index | 1.05 | (1.02, 1.07) | 0.001 |
| Fissure depth (deep) c | 2.73 | (1.59, 4.72) | 0.001 |
| Model 1 d | Adjusted OR | (95% CI) | p |
| Age | 1.25 | (0.44, 3.58) | 0.678 |
| Sex (female) a | 1.60 | (0.80, 3.19) | 0.184 |
| S-OHI (>1.5) b | 1.08 | (0.48, 4.41) | 0.851 |
| dmfs index | 1.07 | (1.01, 1.13) | 0.014 |
| Fissure depth (deep) c | 3.11 | (1.14, 8.47) | 0.026 |
| Model 2 e | Adjusted OR | (95% CI) | p |
| Age | 1.25 | (0.44, 3.62) | 0.670 |
| Sex (female) a | 1.59 | (0.81, 3.15) | 0.184 |
| dmfs index | 1.07 | (1.02, 1.13) | 0.005 |
| Fissure depth (deep) c | 3.15 | (1.13, 8.78) | 0.028 |
| Model 3 f | Adjusted OR | (95% CI) | p |
| Age | 1.36 | (0.43, 4.30) | 0.598 |
| Sex (female) a | 1.70 | (0.87, 3.35) | 0.123 |
| dmfs index | 1.09 | (1.04, 1.14) | 0.001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez-Pérez, L.; Irigoyen-Camacho, M.E.; Molina-Frechero, N.; Zepeda-Zepeda, M. Fissure Depth and Caries Incidence in First Permanent Molars: A Five-Year Follow-Up Study in Schoolchildren. Int. J. Environ. Res. Public Health 2019, 16, 3550. https://doi.org/10.3390/ijerph16193550
Sánchez-Pérez L, Irigoyen-Camacho ME, Molina-Frechero N, Zepeda-Zepeda M. Fissure Depth and Caries Incidence in First Permanent Molars: A Five-Year Follow-Up Study in Schoolchildren. International Journal of Environmental Research and Public Health. 2019; 16(19):3550. https://doi.org/10.3390/ijerph16193550
Chicago/Turabian StyleSánchez-Pérez, Leonor, María Esther Irigoyen-Camacho, Nelly Molina-Frechero, and Marco Zepeda-Zepeda. 2019. "Fissure Depth and Caries Incidence in First Permanent Molars: A Five-Year Follow-Up Study in Schoolchildren" International Journal of Environmental Research and Public Health 16, no. 19: 3550. https://doi.org/10.3390/ijerph16193550
APA StyleSánchez-Pérez, L., Irigoyen-Camacho, M. E., Molina-Frechero, N., & Zepeda-Zepeda, M. (2019). Fissure Depth and Caries Incidence in First Permanent Molars: A Five-Year Follow-Up Study in Schoolchildren. International Journal of Environmental Research and Public Health, 16(19), 3550. https://doi.org/10.3390/ijerph16193550