Decrease in HDL-C is Associated with Age and Household Income in Adults from the Korean National Health and Nutrition Examination Survey 2017: Correlation Analysis of Low HDL-C and Poverty †



Abstract
1. Introduction
2. Methods
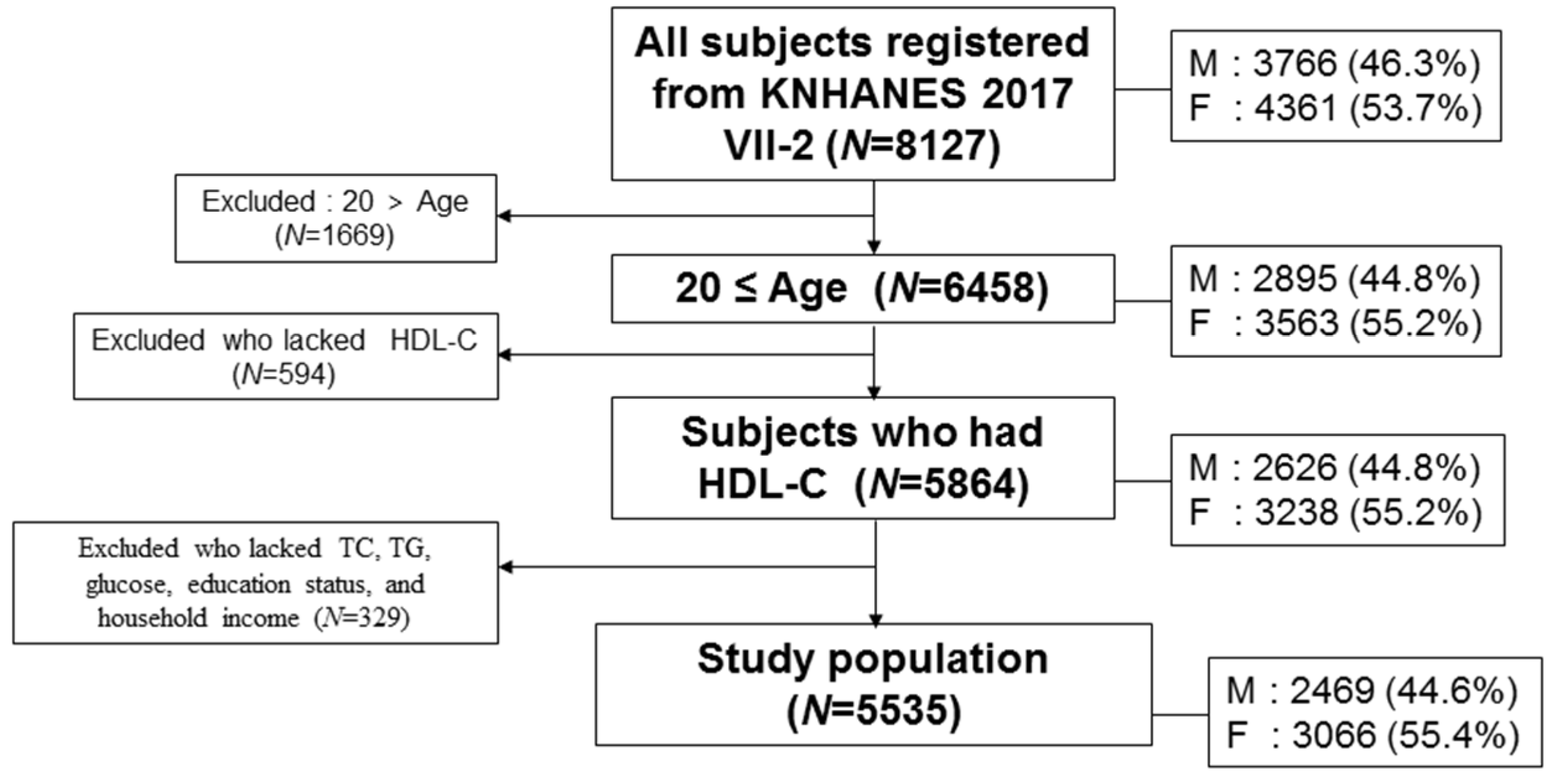
2.1. Study Population
2.2. Statistical Analysis
2.3. Ethics Statement
3. Results
3.1. Baseline Characteristics
3.2. Distribution of Age and Income Grade Depends on HDL-C
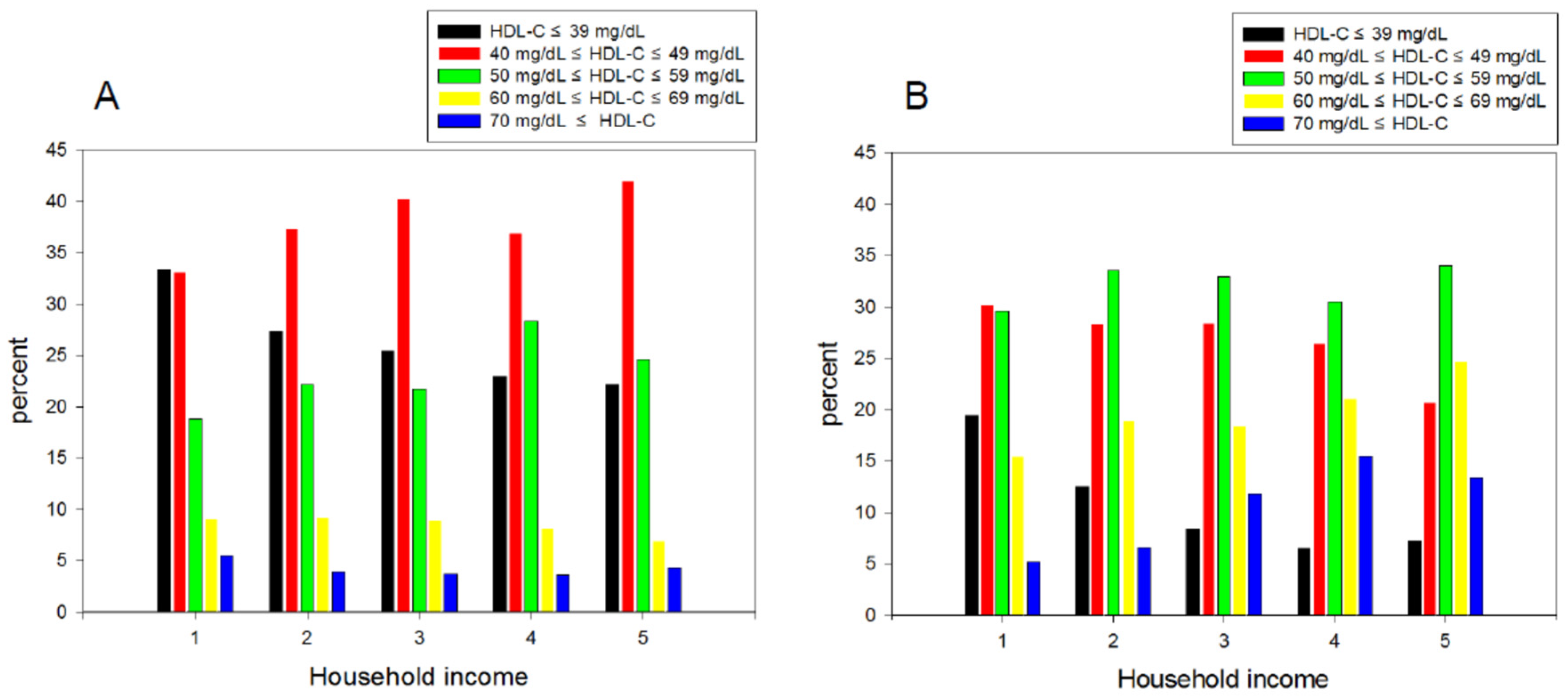
3.3. Percentage Ratio of the HDL-C Level in Each Income Category
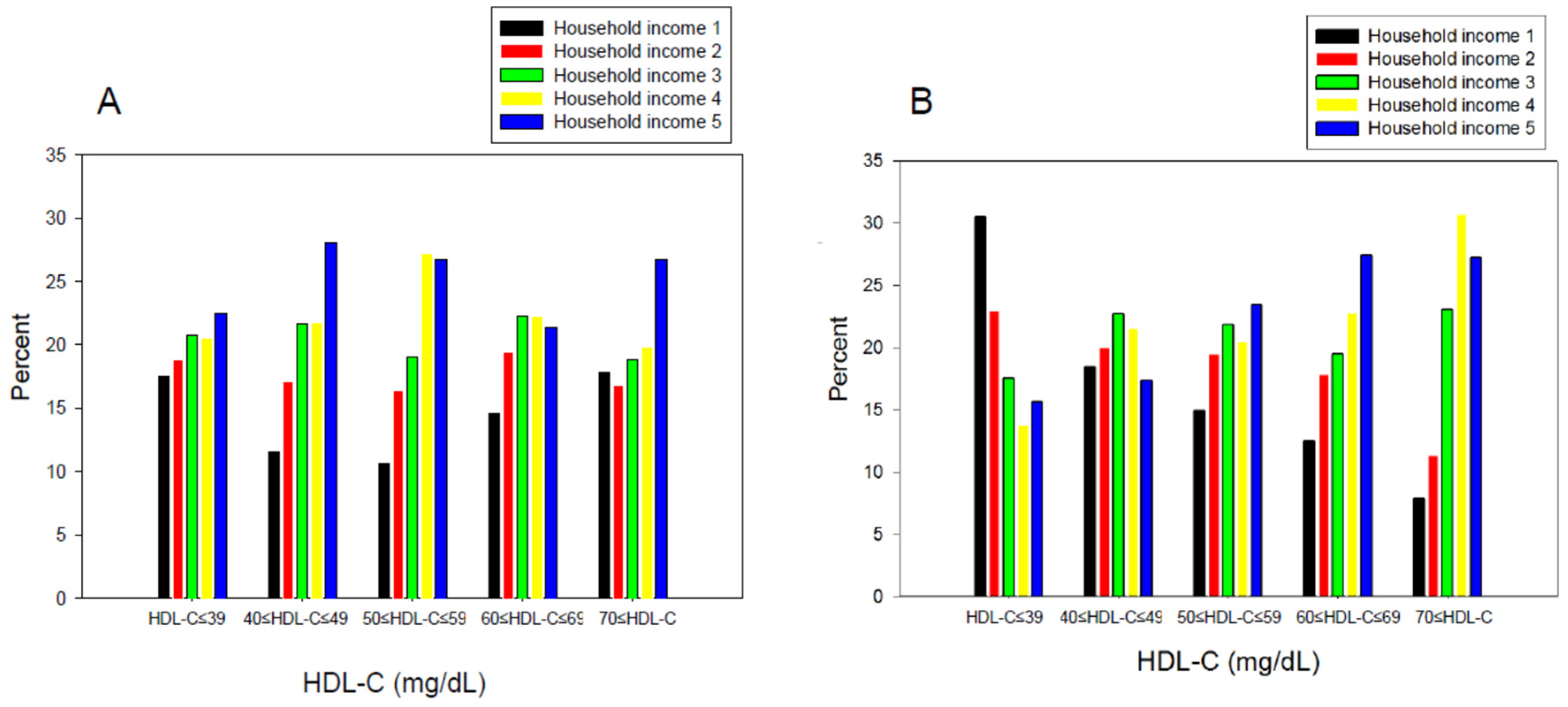
3.4. Percentage Ratio of Income Grade in Each HDL-C Category
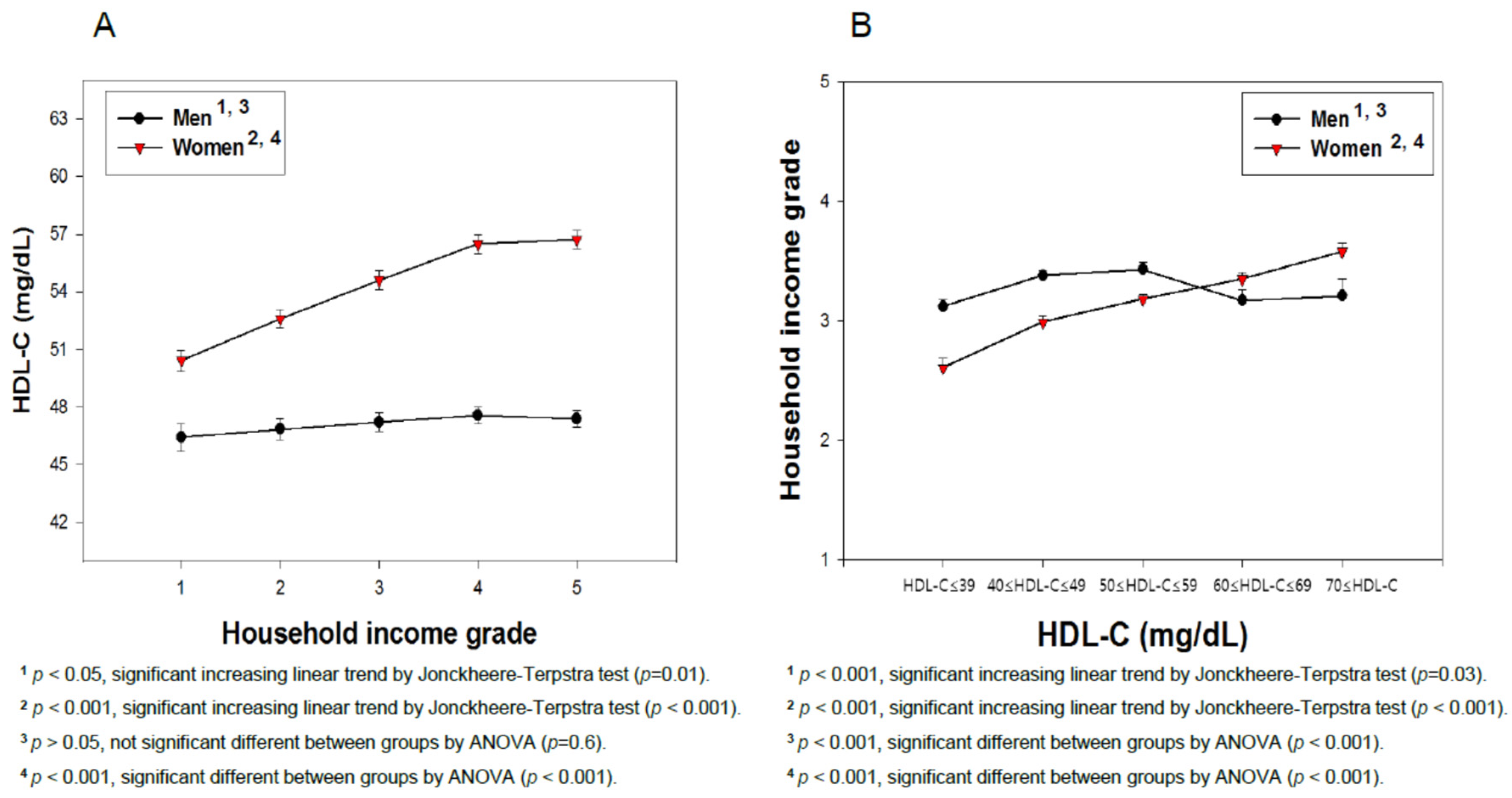
3.5. Average HDL-C Level Depends on the Income Grade
3.6. Average Household Income Grade Depends on the HDL-C Category
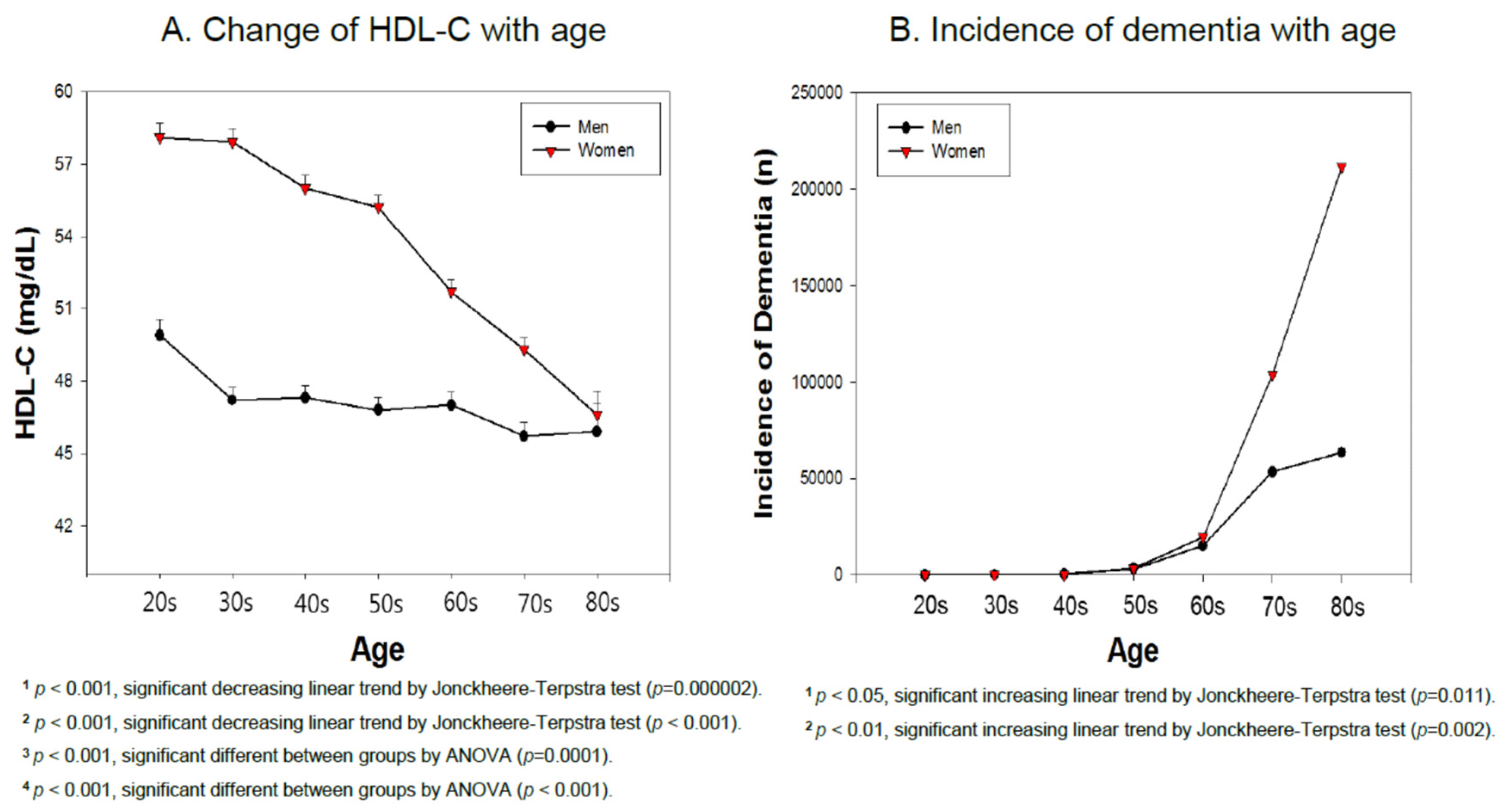
3.7. Incidence of Dementia and HDL-C Based on Age
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- De Melo, L.G.P.; Nunes, S.O.V.; Anderson, G.; Vargas, H.O.; Barbosa, D.S.; Galecki, P.; Carvalho, A.F.; Maes, M. Shared metabolic and immune-inflammatory, oxidative and nitrosative stress pathways in the metabolic syndrome and mood disorders. Prog. Neuro Psychopharmacol. Boil. Psychiatry 2017, 78, 34–50. [Google Scholar] [CrossRef] [PubMed]
- Atti, A.R.; Valente, S.; Iodice, A.; Caramella, I.; Ferrari, B.; Albert, U.; Mandelli, L.; De Ronchi, D. Metabolic Syndrome, Mild Cognitive Impairment, and Dementia: A Meta-Analysis of Longitudinal Studies. Am. J. Geriatr. Psychiatry 2019, 27, 625–637. [Google Scholar] [CrossRef] [PubMed]
- Pal, K.; Mukadam, N.; Petersen, I.; Cooper, C. Mild cognitive impairment and progression to dementia in people with diabetes, prediabetes and metabolic syndrome: A systematic review and meta-analysis. Soc. Psychiatry Psychiatr. Epidemiol. 2018, 53, 1149–1160. [Google Scholar] [CrossRef] [PubMed]
- Ronsein, G.E.; Heinecke, J.W. Time to ditch HDL-C as a measure of HDL function? Curr. Opin. Lipidol. 2017, 28, 414–418. [Google Scholar] [CrossRef] [PubMed]
- Zwald, M.L.; Akinbami, L.J.; Fakhouri, T.H.; Fryar, C.D. Prevalence of Low High-density Lipoprotein Cholesterol among Adults, by Physical Activity: United States, 2011–2014; U.S. Department of Health & Human Services: Hyattsville, MD, USA, 2017; pp. 1–8.
- Choi, S.J.; Park, S.H.; Park, H.Y. Increased Prevalence of low High-density Lipoprotein Cholesterol (HDL-C) Levels in Korean Adults: Analysis of the Three Korean National Health and Nutrition Examination Surveys (KNHANES 1998–2005). Public Health Res. Perspect. 2011, 2, 94–103. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Loucks, E.B.; Rehkopf, D.H.; Thurston, R.C.; Kawachi, I. Socioeconomic Disparities in Metabolic Syndrome Differ by Gender: Evidence from NHANES III. Ann. Epidemiol. 2007, 17, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Attems, J.; Jellinger, K.A. The overlap between vascular disease and Alzheimer’s disease—Lessons from pathology. BMC Med. 2014, 12, 206. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Suzuki, H.; Ito, H.; Korenaga, T.; Akatsu, H.; Meno, K.; Uchida, K. Serum levels of proteins involved in amyloid-beta clearance are related to cognitive decline and neuroimaging changes in mild cognitive impairment. Alzheimers Dement (AMST) 2019, 11, 85–97. [Google Scholar]
- Salerno, D.; Grasso, G.; Deriu, M.A.; Danani, A.; Calabresi, L.; Re, F. The Extent of Human Apolipoprotein A-I Lipidation Strongly Affects The beta-Amyloid Efflux Across the Blood-Brain Barrier in vitro. Front Neurosci. 2019, 13, 419. [Google Scholar]
- Zlokovic, B.V.; Yamada, S.; Holtzman, D.; Ghiso, J.; Frangione, B. Clearance of amyloid beta-peptide from brain: Transport or metabolism? Nat. Med. 2000, 6, 718–719. [Google Scholar] [CrossRef]
- Sacks, F.M.; Jensen, M.K. From High-Density Lipoprotein Cholesterol to Measurements of Function: Prospects for the Development of Tests for High-Density Lipoprotein Functionality in Cardiovascular Disease. Arterioscler. Thromb. Vasc. Biol. 2018, 38, 487–499. [Google Scholar] [CrossRef] [PubMed]
- Juren, A.J.; Sarwal, G.; Al-Sarraf, A.; Vrablík, M.; Chan, D.; Humphries, K.H.; Frohlich, J.J. Low prevalence of type 2 diabetes mellitus among patients with high levels of high-density lipoprotein cholesterol. J. Clin. Lipidol. 2013, 7, 194–198. [Google Scholar] [CrossRef] [PubMed]
- Jones, C.A.; Perera, A.; Chow, M.; Ho, I.; Nguyen, J.; Davachi, S. Cardiovascular Disease Risk Among the Poor and Homeless—What We Know So Far. Curr. Cardiol. Rev. 2009, 5, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Loucks, E.B.; Magnússon, K.T.; Cook, S.; Rehkopf, D.H.; Ford, E.S.; Berkman, L.F. Socioeconomic Position and the Metabolic Syndrome in Early, Middle, and Late Life: Evidence from NHANES 1999–2002. Ann. Epidemiol. 2007, 17, 782–790. [Google Scholar] [CrossRef] [PubMed]
- Kannel, W.B.; Hjortland, M.C.; McNamara, P.M.; Gordon, T. Menopause and risk of cardiovascular disease: The Framingham study. Ann. Intern. Med. 1976, 85, 447–452. [Google Scholar] [CrossRef] [PubMed]
- Robison, L.S.; Gannon, O.J.; Salinero, A.E.; Zuloaga, K.L. Contributions of sex to cerebrovascular function and pathology. Brain Res. 2019, 1710, 43–60. [Google Scholar] [CrossRef]
- Ahn, J.; Kim, N.-S.; Lee, B.-K.; Oh, I.; Kim, Y. Changes of Atmospheric and Blood Concentrations of Lead and Cadmium in the General Population of South Korea from 2008 to 2017. Int. J. Environ. Res. Public Heal. 2019, 16, 2096. [Google Scholar] [CrossRef]
- Executive Summary of the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001, 285, 2486–2497. [CrossRef]
- Terpstra, T. The asymptotic normality and consistency of Kendall’s test against trend, when ties are present in one ranking. Indag. Math. (Proc.) 1952, 55, 327–333. [Google Scholar] [CrossRef]
- Jonckheere, A.R. A Distribution-Free k-Sample Test against Ordered Alternatives. Biometrika 1954, 41, 133. [Google Scholar] [CrossRef]
- Liu, C.L.; Lin, M.Y.; Hwang, S.J.; Liu, C.K.; Lee, H.L.; Wu, M.T. Factors associated with type 2 diabetes in patients with vascular dementia: A population-based cross-sectional study. BMC Endocr. Disord. 2018, 18, 45. [Google Scholar] [CrossRef]
- Tang, K.L.; Rashid, R.; Godley, J.; Ghali, W.A. Association between subjective social status and cardiovascular disease and cardiovascular risk factors: A systematic review and meta-analysis. BMJ Open 2016, 6, e010137. [Google Scholar] [CrossRef] [PubMed]
- Nakahori, N.; Sekine, M.; Yamada, M.; Tatsuse, T.; Kido, H.; Suzuki, M. A pathway from low socioeconomic status to dementia in Japan: Results from the Toyama dementia survey. BMC Geriatr. 2018, 18, 102. [Google Scholar] [CrossRef] [PubMed]
- Xu, W.; Qiu, C.; Gatz, M.; Pedersen, N.L.; Johansson, B.; Fratiglioni, L. Mid- and late-life diabetes in relation to the risk of dementia: A population-based twin study. Diabetes 2009, 58, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Singh-Manoux, A.; Gimeno, D.; Kivimaki, M.; Brunner, E.; Marmot, M.G. Low HDL cholesterol is a risk factor for deficit and decline in memory in midlife: The Whitehall II study. Arter. Thromb. Vasc. Boil. 2008, 28, 1556–1562. [Google Scholar] [CrossRef] [PubMed]
- Shang, J.; Yamashita, T.; Fukui, Y.; Song, D.; Li, X.; Zhai, Y.; Nakano, Y.; Morihara, R.; Hishikawa, N.; Ohta, Y.; et al. Different Associations of Plasma Biomarkers in Alzheimer’s Disease, Mild Cognitive Impairment, Vascular Dementia, and Ischemic Stroke. J. Clin. Neurol. (Seoul Korea) 2018, 14, 29–34. [Google Scholar] [CrossRef]
- Lemieux, I.; Lamarche, B.; Couillard, C.; Pascot, A.; Cantin, B.; Bergeron, J.; Dagenais, G.R.; Després, J.P. Total cholesterol/HDL cholesterol ratio vs LDL cholesterol/HDL cholesterol ratio as indices of ischemic heart disease risk in men: The Quebec Cardiovascular Study. Arch. Intern. Med. 2001, 161, 2685–2692. [Google Scholar] [CrossRef] [PubMed]
- Knopman, D.S. Bad news and good news in AD, and how to reconcile them. Nat. Rev. Neurol. 2019, 15, 61–62. [Google Scholar] [CrossRef]
- Button, E.B.; Robert, J.; Caffrey, T.M.; Fan, J.; Zhao, W.; Wellington, C.L. HDL from an Alzheimer’s disease perspective. Curr. Opin. Lipidol. 2019, 30, 224–234. [Google Scholar] [CrossRef]
- Svensson, T.; Sawada, N.; Mimura, M.; Nozaki, S.; Shikimoto, R.; Tsugane, S. The association between midlife serum high-density lipoprotein and mild cognitive impairment and dementia after 19 years of follow-up. Transl. Psychiatry 2019, 9, 26. [Google Scholar] [CrossRef]
- Crichton, G.E.; Elias, M.F.; Davey, A.; Sullivan, K.J.; Robbins, M.A. Higher HDL Cholesterol Is Associated with Better Cognitive Function: The Maine-Syracuse Study. J. Int. Neuropsychol. Soc. 2014, 20, 961–970. [Google Scholar] [CrossRef] [PubMed]
- Kalin, M.F.; Zumoff, B. Sex hormones and coronary disease: A review of the clinical studies. Steroids 1990, 55, 330–352. [Google Scholar] [CrossRef]
- De Bruijn, R.F.; Ikram, M.A. Cardiovascular risk factors and future risk of Alzheimer’s disease. BMC Med. 2014, 12, 130. [Google Scholar] [CrossRef] [PubMed]
- Feinkohl, I.; Janke, J.; Hadzidiakos, D.; Slooter, A.; Winterer, G.; Spies, C.; Pischon, T. Associations of the metabolic syndrome and its components with cognitive impairment in older adults. BMC Geriatr. 2019, 19, 77. [Google Scholar] [CrossRef] [PubMed]
- Walter, M. Interrelationships among HDL Metabolism, Aging, and Atherosclerosis. Arter. Thromb. Vasc. Boil. 2009, 29, 1244–1250. [Google Scholar] [CrossRef] [PubMed]
- Kreisberg, R.A.; Kasim, S. Cholesterol metabolism and aging. Am. J. Med. 1987, 82, 54–60. [Google Scholar] [CrossRef]
- Wilson, P.W.F.; Anderson, K.M.; Harri, T.; Kannel, W.B.; Castelli, W.P. Determinants of Change in Total Cholesterol and HDL-C with Age: The Framingham Study. J. Gerontol. 1994, 49, 252–257. [Google Scholar] [CrossRef] [PubMed]
- Sultan, N.; Nawaz, M.; Sultan, A.; Fayaz, M.; Baseer, A. Effect of menopause on serum HDL-cholesterol level. J. Ayub Med. Coll. Abbottabad 2003, 15, 24–26. [Google Scholar] [PubMed]
- Kilim, S.R.; Chandala, S.R. A Comparative Study of Lipid Profile and Oestradiol in Pre- and Post-Menopausal Women. J. Clin. Diagn. Res. 2013, 7, 1596–1598. [Google Scholar] [CrossRef] [PubMed]
- Ferrara, A.; Barrett-Connor, E.; Shan, J. Total, LDL, and HDL cholesterol decrease with age in older men and women. The Rancho Bernardo Study 1984–1994. Circulation 1997, 96, 37–43. [Google Scholar] [CrossRef]
- Ruiz-Ramie, J.J.; Barber, J.L.; Sarzynski, M.A. Effects of exercise on HDL functionality. Curr. Opin. Lipidol. 2019, 30, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Bahadoran, Z.; Mirmiran, P.; Hosseini-Esfahani, F.; Azizi, F. Fast food consumption and the risk of metabolic syndrome after 3-years of follow-up: Tehran Lipid and Glucose Study. Eur. J. Clin. Nutr. 2013, 67, 1303–1309. [Google Scholar] [CrossRef] [PubMed]
- Shimakawa, T.; Sorlie, P.; Carpenter, M.; Tell, G.; Williams, O.; Dennis, B.; Watson, R. Dietary Intake Patterns and Sociodemographic Factors in the Atherosclerosis Risk in Communities Study. Prev. Med. 1994, 23, 769–780. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.; Thane, C.W.; Bolton-Smith, C.; Jebb, S.A. Consumption of whole-grain foods by British adults: Findings from further analysis of two national dietary surveys. Public Health Nutr. 2003, 6, 479–484. [Google Scholar] [CrossRef] [PubMed][Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Men N = 2469 | Women N = 3066 | * p-Value | Total N = 5535 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | ||||||||
| Age (years) | 51.3 ± 16.4 | 51.9 ± 16.3 | 0.147 | 51.6 ± 16.4 | ||||||
| TC (mg/dL) | 191.3 ± 38.0 | 194.9 ± 38.1 | 0.0004 | 193.3 ± 38.1 | ||||||
| TG (mg/dL) | 158.8 ± 126.1 | 113.4 ± 74.8 | <0.001 | 133.6 ± 103.4 | ||||||
| HDL-C (mg/dL) | 47.2 ± 11.1 | 54.4 ± 12.4 | <0.001 | 51.2 ± 12.4 | ||||||
| HDL-C category | N (%) | Age | N (%) | Age | N (%) | Age | ||||
| <40 | 628 (25.4) | 34.8 ± 3.8 | 54.3 ± 15.8 | 315 (10.3) | 35.3 ± 3.5 | 61.3 ± 14.9 | 0.028 | 943 (17.0) | 35.0 ± 3.7 | 56.6 ± 15.8 |
| 40–49 | 950 (38.5) | 44.5 ± 2.8 | 50.4 ± 16.3 | 814 (26.5) | 45.0 ± 2.8 | 54.5 ± 16.1 | 0.0003 | 1764 (31.9) | 44.7 ± 2.8 | 52.3 ± 16.3 |
| 50–59 | 584 (23.7) | 53.9 ± 2.8 | 50.2 ± 16.6 | 988 (32.3) | 54.4 ± 2.8 | 50.8 ± 16.1 | 0.002 | 1572 (28.4) | 54.2 ± 2.8 | 50.6 ± 16.3 |
| 60–69 | 206 (8.3) | 63.3 ± 2.7 | 49.7 ± 17.1 | 614 (20.0) | 64.0 ± 2.9 | 48.6 ± 16.3 | 0.009 | 820 (14.8) | 63.8 ± 2.9 | 48.9 ± 16.5 |
| >70 | 101 (4.1) | 77.5 ± 7.6 | 49.5 ± 17.6 | 335 (10.9) | 78.1 ± 8.0 | 45.8 ± 14.0 | 0.499 | 436 (7.9) | 77.9 ± 7.9 | 46.7 ± 15.0 |
| Glucose | 104.3 ± 26.6 | 98.8 ± 22.7 | <0.001 | 101.2 ± 24.7 | ||||||
| Income grade | 3.3 ± 1.4 | 3.15 ± 1.4 | 0.00006 | 3.22 ± 1.4 | ||||||
| 1 | 329 (13.4) | 1 | 63.2 ± 17.0 | 496 (16.2) | 1 | 67.9 ± 12.7 | 825 (14.9) | 1 | 66.0 ± 14.7 | |
| 2 | 433 (17.5) | 2 | 56.9 ± 16.7 | 575 (18.8) | 2 | 54.9 ± 16.2 | 1008 (18.2) | 2 | 55.8 ± 16.4 | |
| 3 | 512 (20.7) | 3 | 49.4 ± 15.9 | 652 (21.3) | 3 | 48.9 ± 15.4 | 1164 (21.0) | 3 | 49.1 ± 15.6 | |
| 4 | 561 (22.7) | 4 | 46.9 ± 14.2 | 663 (21.5) | 4 | 46.1 ± 14.1 | 1224 (22.1) | 4 | 46.4 ± 14.1 | |
| 5 | 634 (25.7) | 5 | 46.6 ± 14.0 | 680 (22.2) | 5 | 46.1 ± 13.2 | 1314 (23.8) | 5 | 46.3 ± 13.6 | |
| Characteristics | Men N = 2469 | Women N = 3066 | * p-Value | Total N = 5535 | |||
|---|---|---|---|---|---|---|---|
| N (%) | Mean ± SD | N (%) | Mean ± SD | N (%) | Mean ± SD | ||
| Age | |||||||
| 20–29 | 300 (12.2) | 49.9 ± 11.1 | 327 (10.7) | 58.1 ± 11.3 | <0.001 | 627 (11.3) | 54.2 ± 11.9 |
| 30–39 | 376 (15.2) | 47.2 ±10.2 | 460 (15.0) | 57.9 ± 12.4 | <0.001 | 836 (15.1) | 53.1 ± 12.7 |
| 40–49 | 454 (18.4) | 47.3 ±10.6 | 585 (19.1) | 56.0 ± 12.6 | <0.001 | 1039 (18.8) | 52.2 ± 12.5 |
| 50–59 | 502 (20.3) | 46.8 ±11.2 | 617 (20.1) | 55.2 ± 12.4 | <0.001 | 1119 (20.2) | 51.4 ± 12.6 |
| 60–69 | 435 (17.6) | 47.0 ±11.6 | 564 (18.4) | 51.7 ± 12.0 | <0.001 | 999 (18.0) | 49.6 ± 12.0 |
| 70–79 | 320 (13.0) | 45.7 ±11.7 | 387 (12.6) | 50.2 ± 11.4 | <0.001 | 707 (12.8) | 48.1 ± 11.8 |
| <80 | 82 (3.3) | 45.9 ± 10.9 | 126 (4.1) | 46.6 ± 10.9 | 0.656 | 208 (3.8) | 46.3 ± 10.9 |
| Income grade | |||||||
| 1 | 329 (13.3) | 46.4 ± 12.8 | 496 (16.2) | 50.4 ± 12.0 | 0.000006 | 825 (14.9) | 48.8 ± 12.5 |
| 2 | 433 (17.5) | 46.9 ± 11.7 | 575 (18.8) | 52.6 ± 11.7 | <0.001 | 1008 (18.2) | 50.1 ± 12.0 |
| 3 | 512 (20.7) | 47.2 ± 10.8 | 652 (21.3) | 54.6 ± 12.3 | <0.001 | 1164 (21.0) | 51.4 ± 12.2 |
| 4 | 561 (22.7) | 47.6 ± 10.3 | 663 (21.6) | 56.5 ± 12.8 | <0.001 | 1224 (22.1) | 52.4 ± 12.5 |
| 5 | 634 (25.8) | 47.4 ± 10.7 | 680 (22.1) | 56.7 ± 12.3 | <0.001 | 1314 (23.8) | 52.2 ± 12.4 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cho, K.-H.; Park, H.-J.; Kim, S.-J.; Kim, J.-R. Decrease in HDL-C is Associated with Age and Household Income in Adults from the Korean National Health and Nutrition Examination Survey 2017: Correlation Analysis of Low HDL-C and Poverty. Int. J. Environ. Res. Public Health 2019, 16, 3329. https://doi.org/10.3390/ijerph16183329
Cho K-H, Park H-J, Kim S-J, Kim J-R. Decrease in HDL-C is Associated with Age and Household Income in Adults from the Korean National Health and Nutrition Examination Survey 2017: Correlation Analysis of Low HDL-C and Poverty. International Journal of Environmental Research and Public Health. 2019; 16(18):3329. https://doi.org/10.3390/ijerph16183329
Chicago/Turabian StyleCho, Kyung-Hyun, Hye-Jeong Park, Suk-Jeong Kim, and Jae-Ryong Kim. 2019. "Decrease in HDL-C is Associated with Age and Household Income in Adults from the Korean National Health and Nutrition Examination Survey 2017: Correlation Analysis of Low HDL-C and Poverty" International Journal of Environmental Research and Public Health 16, no. 18: 3329. https://doi.org/10.3390/ijerph16183329
APA StyleCho, K.-H., Park, H.-J., Kim, S.-J., & Kim, J.-R. (2019). Decrease in HDL-C is Associated with Age and Household Income in Adults from the Korean National Health and Nutrition Examination Survey 2017: Correlation Analysis of Low HDL-C and Poverty. International Journal of Environmental Research and Public Health, 16(18), 3329. https://doi.org/10.3390/ijerph16183329