Socioeconomic Inequalities in the HIV Testing during Antenatal Care in Vietnamese Women

 ,
,  ,
,  , , and
, , and
Abstract
1. Introduction
2. Methods
2.1. Source Data
2.2. Independent and Explanatory Variables
2.2.1. Independent Variable
2.2.2. Selected Explanatory Variables
2.2.3. Ethnic Groups
2.3. Measurement of Socioeconomic Inequality
2.3.1. Concentration Index
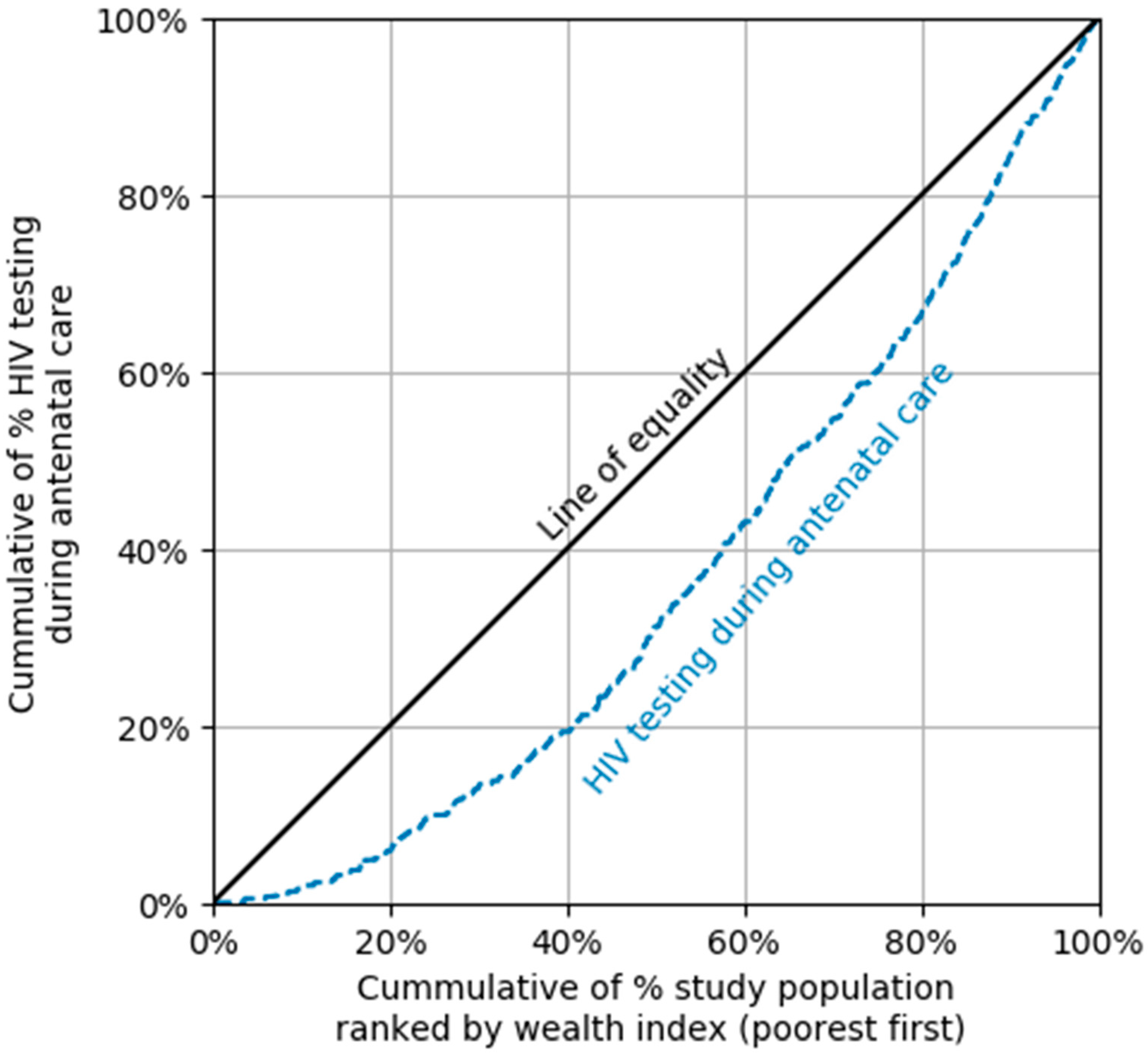
2.3.2. Concentration Curve
2.4. Data Analysis
2.5. Research Ethics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- The Joint United Nations Programme on HIV/AIDS (UNAIDS). UNAIDS DATA 2017, UNAIDS/JC2910E. Geneva, Switzerland, 2017. Available online: https://www.unaids.org/sites/default/files/media_asset/20170720_Data_book_2017_en.pdf (accessed on 4 September 2019).
- Ending, A. Progress toward the 90-90-90 Targets; Joint United Nations Programme on HIV: Geneva, Switzerland, 2017. [Google Scholar]
- The Joint United Nations Programme on HIV/AIDS (UNAIDS). UNAIDS DATA 2018. UNAIDS 2018 estimates. Geneva, Switzerland, 2018. Available online: https://www.unaids.org/sites/default/files/media_asset/unaids-data-2018_en.pdf (accessed on 4 September 2019).
- Morch, E.; Anh, N.; Ha, D.; Hanh, N. Assessment Report; Vietnam Ministry of Health: Hanoi, Vietnam, 2006. [Google Scholar]
- Chen, K.T.; Qian, H.Z. Mother to child transmission of HIV in China. BMJ 2005, 330, 1282–1283. [Google Scholar] [CrossRef] [PubMed]
- Sinha, G.; Dyalchand, A.; Khale, M.; Kulkarni, G.; Vasudevan, S.; Bollinger, R.C. Low utilization of HIV testing during pregnancy: What are the barriers to HIV testing for women in rural India? J. Acquir. Immune Defic. Syndr. 2008, 47, 248–252. [Google Scholar] [PubMed]
- Rakgoasi, S.D. HIV counselling and testing of pregnant women attending antenatal clinics in Botswana, 2001. J. Health Popul. Nutr. 2005, 23, 58–65. [Google Scholar] [PubMed]
- Nuwagaba-Biribonwoha, H.; Mayon-White, R.T.; Okong, P.; Carpenter, L.M. Challenges faced by health workers in implementing the prevention of mother-to-child HIV transmission (PMTCT) programme in Uganda. J. Public Health (Oxf. Engl.) 2007, 29, 269–274. [Google Scholar] [CrossRef] [PubMed]
- Segurado, A.C.; Paiva, V. Rights of HIV positive people to sexual and reproductive health: Parenthood. Reprod. Health Matters 2007, 15, 27–45. [Google Scholar] [CrossRef]
- UNAIDS. HIV in Asia and the Pacific UNAIDS Report 2013; UNAIDS/JC2558; Geneva, Switzerland, 2013; Available online: https://www.unaids.org/sites/default/files/media_asset/2013_HIV-Asia-Pacific_en_0.pdf (accessed on 4 September 2019).
- UNAIDS. Global AIDS Update 2018: Miles to Go—Closing Gaps, Breaking Barriers, Righting Injustices; Joint United Nations Programme on HIV/AIDS (UNAIDS): Geneva, Switzerland, 2018. [Google Scholar]
- HIV/AIDS, UNAIDS. Counselling and voluntary HIV testing for pregnant women in high HIV prevalence countries: Elements and issues. In Counselling and Voluntary HIV Testing for Pregnant Women in High HIV Prevalence Countries: Elements and Issues; UNAIDS: Geneva, Switzerland, 1999. [Google Scholar]
- Ejigu, Y.; Tadesse, B. HIV testing during pregnancy for prevention of mother-to-child transmission of HIV in Ethiopia. PLoS ONE 2018, 13, e0201886. [Google Scholar] [CrossRef] [PubMed]
- Karamagi, C.A.; Tumwine, J.K.; Tylleskar, T.; Heggenhougen, K. Antenatal HIV testing in rural eastern Uganda in 2003: Incomplete rollout of the prevention of mother-to-child transmission of HIV programme? BMC Int. Health Hum. Rights 2006, 6, 6. [Google Scholar] [CrossRef] [PubMed]
- Mahmoud, M.M.; Nasr, A.M.; Gassmelseed, D.E.; Abdalelhafiz, M.A.; Elsheikh, M.A.; Adam, I. Knowledge and attitude toward HIV voluntary counseling and testing services among pregnant women attending an antenatal clinic in Sudan. J. Med. Virol. 2007, 79, 469–473. [Google Scholar] [CrossRef] [PubMed]
- Iliyasu, Z.; Kabir, M.; Galadanci, H.S.; Abubakar, I.S.; Aliyu, M.H. Awareness and attitude of antenatal clients towards HIV voluntary counselling and testing in Aminu Kano Teaching Hospital, Kano, Nigeria. Niger. J. Med. J. Natl. Assoc. Resid. Dr. Niger. 2005, 14, 27–32. [Google Scholar] [CrossRef]
- Westheimer, E.F.; Urassa, W.; Msamanga, G.; Baylin, A.; Wei, R.; Aboud, S.; Kaaya, S.; Fawzi, W.W. Acceptance of HIV testing among pregnant women in Dar-es-Salaam, Tanzania. J. Acquir. Immune Defic. Syndr. 2004, 37, 1197–1205. [Google Scholar] [CrossRef]
- Veloso, V.G.; Portela, M.C.; Vasconcellos, M.T.; Matzenbacher, L.A.; Vasconcelos, A.L.; Grinsztejn, B.; Bastos, F.I. HIV testing among pregnant women in Brazil: Rates and predictors. Rev. Saude Publica 2008, 42, 859–867. [Google Scholar] [CrossRef] [PubMed]
- Kominami, M.; Kawata, K.; Ali, M.; Meena, H.; Ushijima, H. Factors determining prenatal HIV testing for prevention of mother to child transmission in Dar Es Salaam, Tanzania. Pediatr. Int. 2007, 49, 286–292. [Google Scholar] [CrossRef] [PubMed]
- Creek, T.; Ntumy, R.; Mazhani, L.; Moore, J.; Smith, M.; Han, G.; Shaffer, N.; Kilmarx, P.H. Factors associated with low early uptake of a national program to prevent mother to child transmission of HIV (PMTCT): Results of a survey of mothers and providers, Botswana, 2003. AIDS Behav. 2009, 13, 356–364. [Google Scholar] [CrossRef] [PubMed]
- Perez, F.; Zvandaziva, C.; Engelsmann, B.; Dabis, F. Acceptability of routine HIV testing (“opt-out”) in antenatal services in two rural districts of Zimbabwe. J. Acquir. Immune Defic. Syndr. 2006, 41, 514–520. [Google Scholar] [CrossRef] [PubMed]
- Dinh, T.H.; Detels, R.; Nguyen, M.A. Factors associated with declining HIV testing and failure to return for results among pregnant women in Vietnam. AIDS 2005, 19, 1234–1236. [Google Scholar] [CrossRef] [PubMed]
- Chu, D.T.; Vo Truong Nhu, N.; Tao, Y.; Le Hoang, S. Achievements and challenges in HIV/AIDS control in Vietnam. HIV Med. 2018, 19, e75–e76. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.A.; Oosterhoff, P.; Hardon, A.; Tran, H.N.; Coutinho, R.A.; Wright, P. A hidden HIV epidemic among women in Vietnam. BMC Public Health 2008, 8, 37. [Google Scholar] [CrossRef]
- UNAIDS HIV Testing Services: New Opportunities and Ongoing Challenges. Available online: http://www.unaids.org/sites/default/files/media_asset/2017_WHO-UNAIDS_statement_HIV-testing-services_en.pdf (accessed on 16 March 2019).
- World Health Organization. Joint Review of the Health Sector Response to HIV in Viet Nam 2014; WHO Regional Office for the Western Pacific: Manila, Philippines, 2016. [Google Scholar]
- General Statistics Office (GSO). Viet Nam Multiple Indicator Cluster Survey (MICS) 2014; Final Report; Ministry of Planning and Investment: Hanoi, Vietnam, 2014.
- Filmer, D.; Pritchett, L. Estimating wealth effects without expenditure data—Or tears. In Policy Research Working Paper 1980, The World; The World Bank: Washington, DC, USA, 1998. [Google Scholar]
- Kakwani, N.C. Measurement of tax progressivity: An international comparison. Econ. J. 1977, 87, 71–80. [Google Scholar] [CrossRef]
- Wagstaff, A.; Paci, P.; van Doorslaer, E. On the measurement of inequalities in health. Soc. Sci. Med. 1991, 33, 545–557. [Google Scholar] [CrossRef]
- O’Donnell, O.; Van Doorslaer, E.; Wagstaff, A.; Lindelow, M. Analyzing Health Equity Using Household Survey Data: A Guide to Techniques and Their Implementation; The World Bank: Washington, DC, USA, 2007. [Google Scholar]
- O’Donnell, O.; O’Neill, S.; Van Ourti, T.; Walsh, B. Conindex: Estimation of concentration indices. Stata J. 2016, 16, 112–138. [Google Scholar]
- World Health Organization. WHO Consolidated Guidelines on HIV Testing Services; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Car, L.T.; van-Velthoven, M.H.; Brusamento, S.; Elmoniry, H.; Car, J.; Majeed, A.; Atun, R. Integrating prevention of mother-to-child HIV transmission (PMTCT) programmes with other health services for preventing HIV infection and improving HIV outcomes in developing countries. Cochrane Database Syst. Rev. 2011, Cd008741. [Google Scholar] [CrossRef]
- Hanh, N.T.; Gammeltoft, T.M.; Rasch, V. Number and timing of antenatal HIV testing: Evidence from a community-based study in Northern Vietnam. BMC Public Health 2011, 11, 183. [Google Scholar] [CrossRef] [PubMed]
- Gunn, J.K.; Asaolu, I.O.; Center, K.E.; Gibson, S.J.; Wightman, P.; Ezeanolue, E.E.; Ehiri, J.E. Antenatal care and uptake of HIV testing among pregnant women in sub-Saharan Africa: A cross-sectional study. J. Int. AIDS Soc. 2016, 19, 20605. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, L.T.; Christoffersen, S.V.; Rasch, V. Uptake of prenatal HIV testing in Hai Phong Province, Vietnam. Asia-Pac. J. Public Health 2010, 22, 451–459. [Google Scholar] [CrossRef] [PubMed]
- Socialist Republic of Vietnam Government Portal: Ethnic Groups in Vietnam. Available online: http://www.chinhphu.vn/portal/page/portal/English/TheSocialistRepublicOfVietnam/AboutVietnam/AboutVietnamDetail?categoryId=10000103&articleId=10002652 (accessed on 2 January 2019).
- Inter-Parliamentary Union (IPU). Hiv and Aids in Viet Nam—Facing the Challenges; IPU: Geneva, Switzerland, 2015. [Google Scholar]
- Jones, N.; Nguyen, A.; Presler-Marshall, E. Mapping the Reform Process in the Public Delivery of Social Protection Services in Viet Nam; Development and Policies Research Center (DEPOCEN): Hanoi, Vietnam, 2011. [Google Scholar]


{kind=link}
| Characteristics | Individual and Household Characteristics of Women Aged 15–49 | |
|---|---|---|
| n | % | |
| Age group | ||
| 15–19 | 80 | 5.4 |
| 20–34 | 1239 | 83.5 |
| 35–49 | 165 | 11.1 |
| Ethnicity | ||
| Minority | 252 | 17.0 |
| Kinh | 1232 | 83.0 |
| Educational level | ||
| Primary or less | 252 | 17.0 |
| Lower secondary school | 536 | 36.1 |
| Upper secondary school and tertiary | 696 | 46.9 |
| Living area | ||
| Urban | 433 | 29.2 |
| Rural | 1051 | 70.8 |
| Socioeconomic status | ||
| Poorest | 298 | 20.1 |
| Poorer | 292 | 19.7 |
| Middle | 297 | 20.0 |
| Richer | 318 | 21.4 |
| Richest | 279 | 18.8 |
| Characteristics | Women Who Received HIV Testing during ANC | p value | |
|---|---|---|---|
| % | 95%CI | ||
| Age group | 0.1664 | ||
| 15–19 | 21.8 | 12.6–35.0 | |
| 20–34 | 29.8 | 26.3–33.6 | |
| 35–49 | 35.6 | 27.4–44.6 | |
| Ethnicity | 0.0000 *** | ||
| Minority | 8.5 | 5.1–13.6 | |
| Kinh | 34.4 | 30.6–38.6 | |
| Educational level | 0.0000 *** | ||
| Primary or less | 17.0 | 12.1–23.5 | |
| Lower secondary school | 25.3 | 20.9–30.3 | |
| Upper secondary school and tertiary | 38.4 | 33.6–43.4 | |
| Living area | 0.0000 *** | ||
| Urban | 42.2 | 6.79–8.75 | |
| Rural | 25.0 | 20.8–29.7 | |
| Socioeconomic status | 0.0000 *** | ||
| Poorest | 8.7 | 5.7–13.2 | |
| Poorer | 20.5 | 15.5–26.7 | |
| Middle | 34.9 | 28.0–42.6 | |
| Richer | 36.5 | 30.0–43.6 | |
| Richest | 50.1 | 42.4–57.8 | |
| Characteristics | Women Who Received HIV Testing during ANC | |
|---|---|---|
| CCI | SE | |
| Age group | ||
| 15–19 | 0.4 ** | 0.13 |
| 20–34 | 0.3 *** | 0.03 |
| 35–49 | 0.3 *** | 0.06 |
| Ethnicity | ||
| Minority | 0.5 *** | 0.11 |
| Kinh | 0.2 *** | 0.03 |
| Educational level | ||
| Primary or less | 0.4 *** | 0.08 |
| Lower secondary school | 0.2 *** | 0.05 |
| Upper secondary school and tertiary | 0.2 *** | 0.03 |
| Living area | ||
| Urban | 0.1 *** | 0.04 |
| Rural | 0.3 *** | 0.04 |
| Characteristics | Women Who Received HIV Testing during ANC | |
|---|---|---|
| OR | 95%CI | |
| Age group | ||
| 15–19 | 1 | - |
| 20–34 | 0.77 | 0.4–1.6 |
| 35–49 | 1.01 | 0.5–2.2 |
| Ethnicity | ||
| Minority | 1 | - |
| Kinh | 2.52 ** | 1.4–4.7 |
| Educational level | ||
| Primary or less | 1 | - |
| Lower secondary school | 1.09 | 0.7–1.7 |
| Upper secondary school and tertiary | 1.37 | 0.9–2.2 |
| Living area | ||
| Urban | 1 | - |
| Rural | 0.82 | 0.5–1.3 |
| Socioeconomic status | ||
| Poorest | 1 | - |
| Poorer | 1.81 | 0.9–3.3 |
| Middle | 3.38 *** | 1.9–6.2 |
| Richer | 3.30 *** | 1.7–6.3 |
| Richest | 4.99 *** | 2.4–10.3 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chu, D.-T.; Vo, H.-L.; Tran, D.-K.; Nguyen Si Anh, H.; Bao Hoang, L.; Tran Nhu, P.; Nguyen Ngoc, K.; Thu Nguyen, T.; Pham Van, Q.; Tien, N.L.B.; et al. Socioeconomic Inequalities in the HIV Testing during Antenatal Care in Vietnamese Women. Int. J. Environ. Res. Public Health 2019, 16, 3240. https://doi.org/10.3390/ijerph16183240
Chu D-T, Vo H-L, Tran D-K, Nguyen Si Anh H, Bao Hoang L, Tran Nhu P, Nguyen Ngoc K, Thu Nguyen T, Pham Van Q, Tien NLB, et al. Socioeconomic Inequalities in the HIV Testing during Antenatal Care in Vietnamese Women. International Journal of Environmental Research and Public Health. 2019; 16(18):3240. https://doi.org/10.3390/ijerph16183240
Chicago/Turabian StyleChu, Dinh-Toi, Hoang-Long Vo, Dang-Khoa Tran, Hao Nguyen Si Anh, Long Bao Hoang, Phong Tran Nhu, Khanh Nguyen Ngoc, Trang Thu Nguyen, Quyet Pham Van, Nguyen Le Bao Tien, and et al. 2019. "Socioeconomic Inequalities in the HIV Testing during Antenatal Care in Vietnamese Women" International Journal of Environmental Research and Public Health 16, no. 18: 3240. https://doi.org/10.3390/ijerph16183240
APA StyleChu, D.-T., Vo, H.-L., Tran, D.-K., Nguyen Si Anh, H., Bao Hoang, L., Tran Nhu, P., Nguyen Ngoc, K., Thu Nguyen, T., Pham Van, Q., Tien, N. L. B., Thanh, V. V., Nga, V. T., Luu Quang, T., Minh, L. B., & Pham, V. H. (2019). Socioeconomic Inequalities in the HIV Testing during Antenatal Care in Vietnamese Women. International Journal of Environmental Research and Public Health, 16(18), 3240. https://doi.org/10.3390/ijerph16183240