Residential Greenness and Birthweight in the State of Massachusetts, USA

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Data
2.1.1. Study Population
2.1.2. Exposure: Residential Greenness
2.1.3. Outcomes
2.1.4. Covariates
2.2. Analysis
3. Results
3.1. Summary Statistics
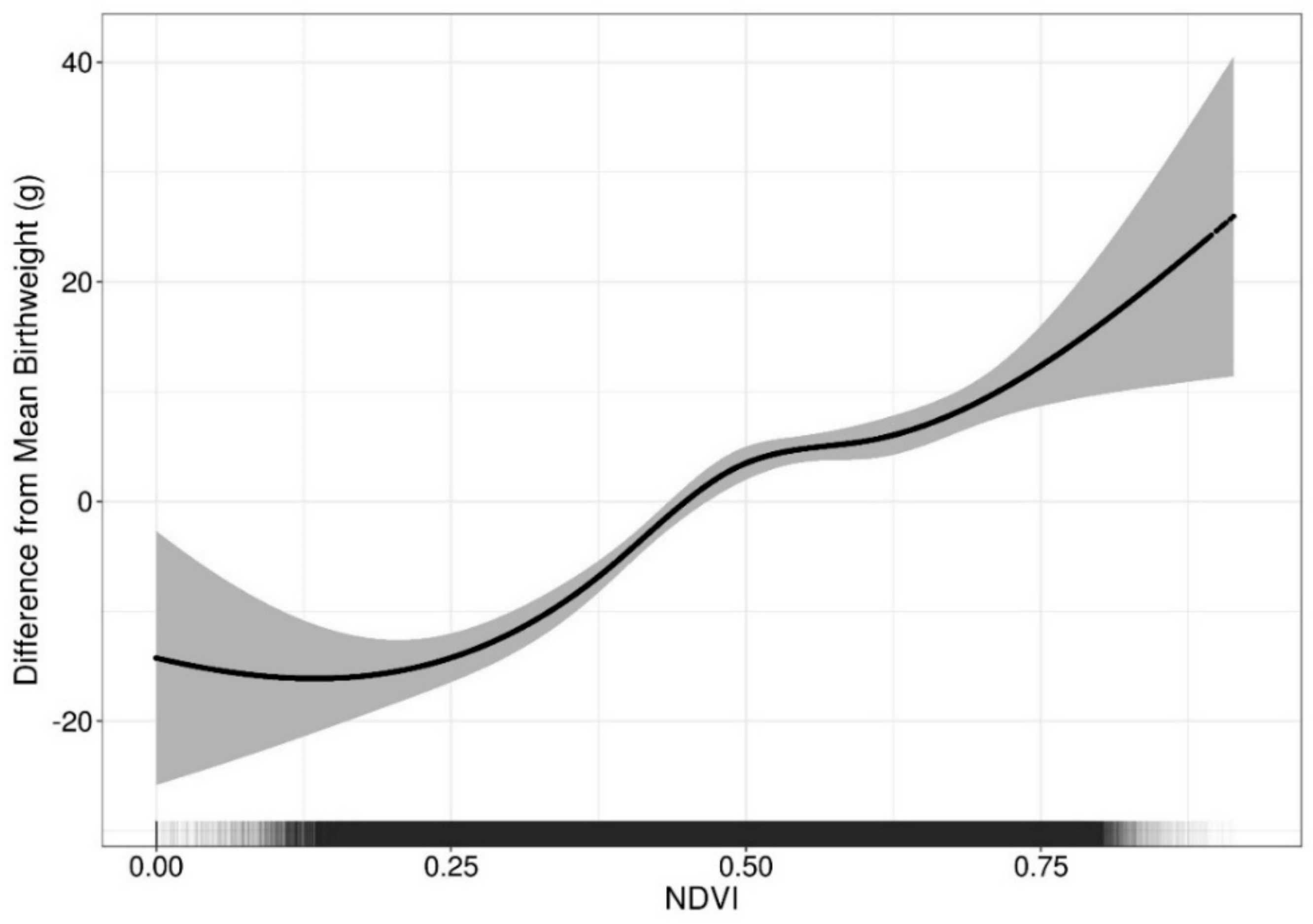
3.2. Continuous Birthweight
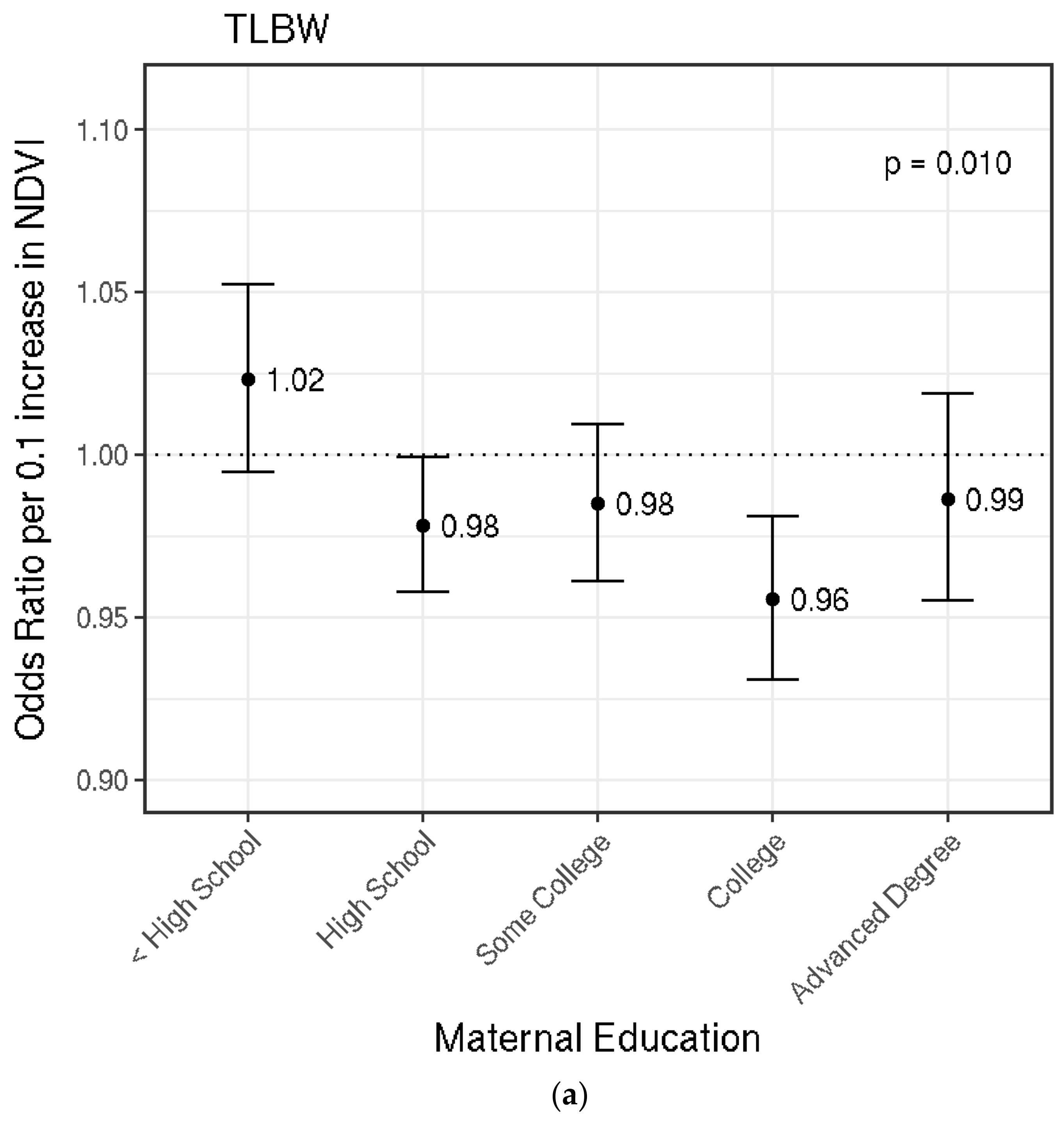
3.3. Term Low Birthweight (TLBW)
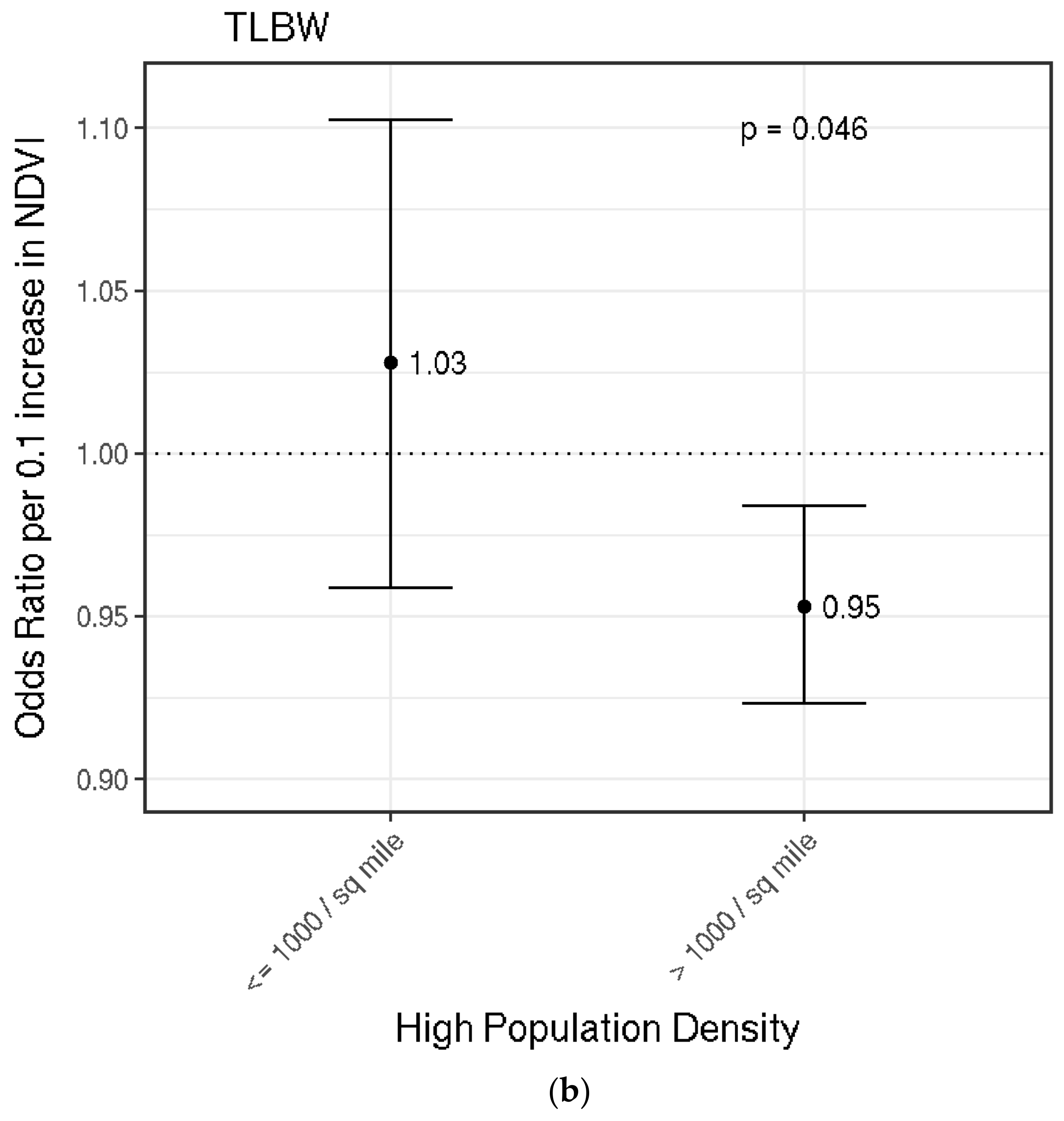
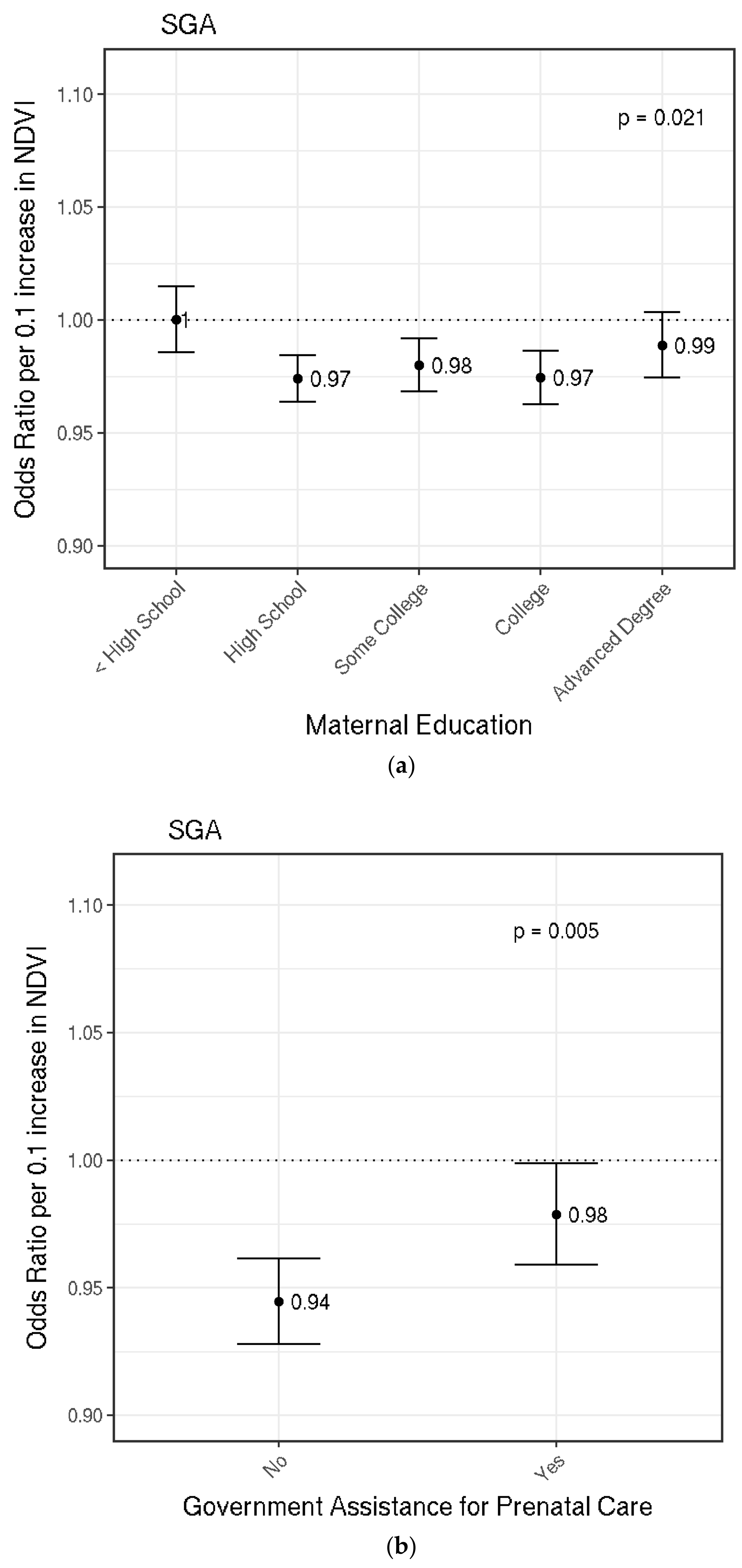
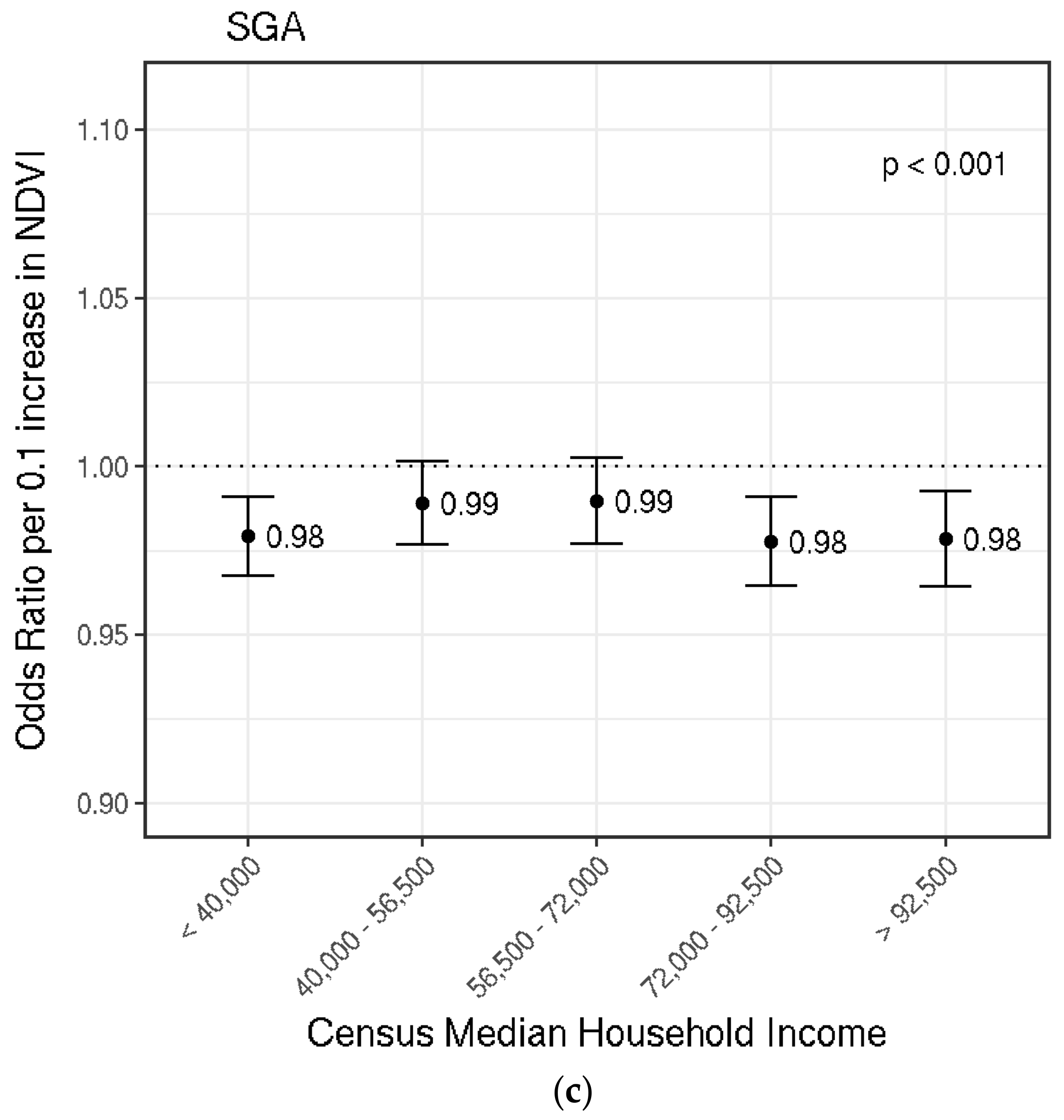
3.4. Small for Gestational Age (SGA)
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Association with 0.1 Increase in NDVI in Model Excluding PM2.5 | |
|---|---|
| Continuous Birthweight | |
| 0.25–0.50 NDVI | 6.92 (95% CI: 5.42, 8.42) |
| 0.50–0.75 NDVI | 2.28 (95% CI: 0.18, 4.38) |
| Term Low Birthweight (TLBW) | 0.98 (95% CI: 0.97, 1.00) |
| Small for Gestational Age (SGA) | 0.98 (95% CI: 0.98, 0.99) |
References
- Belbasis, L.; Savvidou, M.D.; Kanu, C.; Evangelou, E.; Tzoulaki, I. Birth weight in relation to health and disease in later life: An umbrella review of systematic reviews and meta-analyses. BMC Med. 2016, 14, 147. [Google Scholar] [CrossRef] [PubMed]
- Boulet, S.L.; Schieve, L.A.; Boyle, C.A. Birth weight and health and developmental outcomes in US children, 1997–2005. Matern. Child Health J. 2011, 15, 836–844. [Google Scholar] [CrossRef] [PubMed]
- Hack, M.; Klein, N.K.; Taylor, H.G. Long-term developmental outcomes of low birth weight infants. Future Child. Cent. Future Child. David Lucile Packard Found. 1995, 5, 176–196. [Google Scholar] [CrossRef]
- Korten, I.; Ramsey, K.; Latzin, P. Air pollution during pregnancy and lung development in the child. Paediatr. Respir. Rev. 2017, 21, 38–46. [Google Scholar] [CrossRef] [PubMed]
- Reyes, L.; Mañalich, R. Long-term consequences of low birth weight. Kidney Int. Suppl. 2005, 68, S107–S111. [Google Scholar] [CrossRef] [PubMed]
- Abelt, K.; McLafferty, S. Green Streets: Urban Green and Birth Outcomes. Int. J. Environ. Res. Public. Health 2017, 14. [Google Scholar] [CrossRef]
- Casey, J.A.; James, P.; Rudolph, K.E.; Wu, C.-D.; Schwartz, B.S. Greenness and Birth Outcomes in a Range of Pennsylvania Communities. Int. J. Environ. Res. Public. Health 2016, 13. [Google Scholar] [CrossRef] [PubMed]
- Cusack, L.; Larkin, A.; Carozza, S.; Hystad, P. Associations between residential greenness and birth outcomes across Texas. Environ. Res. 2017, 152, 88–95. [Google Scholar] [CrossRef] [PubMed]
- Cusack, L.; Larkin, A.; Carozza, S.E.; Hystad, P. Associations between multiple green space measures and birth weight across two US cities. Health Place 2017, 47, 36–43. [Google Scholar] [CrossRef] [PubMed]
- Dadvand, P.; Sunyer, J.; Basagaña, X.; Ballester, F.; Lertxundi, A.; Fernández-Somoano, A.; Estarlich, M.; García-Esteban, R.; Mendez, M.A.; Nieuwenhuijsen, M.J. Surrounding greenness and pregnancy outcomes in four Spanish birth cohorts. Environ. Health Perspect. 2012, 120, 1481–1487. [Google Scholar] [CrossRef] [PubMed]
- Dadvand, P.; Parker, J.; Bell, M.L.; Bonzini, M.; Brauer, M.; Darrow, L.A.; Gehring, U.; Glinianaia, S.V.; Gouveia, N.; Ha, E.; et al. Maternal exposure to particulate air pollution and term birth weight: A multi-country evaluation of effect and heterogeneity. Environ. Health Perspect. 2013, 121, 267–373. [Google Scholar] [CrossRef] [PubMed]
- Ebisu, K.; Holford, T.R.; Bell, M.L. Association between greenness, urbanicity, and birth weight. Sci. Total Environ. 2016, 542, 750–756. [Google Scholar] [CrossRef] [PubMed]
- Hystad, P.; Davies, H.W.; Frank, L.; Van Loon, J.; Gehring, U.; Tamburic, L.; Brauer, M. Residential greenness and birth outcomes: Evaluating the influence of spatially correlated built-environment factors. Environ. Health Perspect. 2014, 122, 1095–1102. [Google Scholar] [CrossRef] [PubMed]
- Markevych, I.; Schoierer, J.; Hartig, T.; Chudnovsky, A.; Hystad, P.; Dzhambov, A.M.; de Vries, S.; Triguero-Mas, M.; Brauer, M.; Nieuwenhuijsen, M.J.; et al. Exploring pathways linking greenspace to health: Theoretical and methodological guidance. Environ. Res. 2017, 158, 301–317. [Google Scholar] [CrossRef] [PubMed]
- Gidlöf-Gunnarsson, A.; Öhrström, E. Noise and well-being in urban residential environments: The potential role of perceived availability to nearby green areas. Landsc. Urban Plan. 2007, 83, 115–126. [Google Scholar] [CrossRef]
- Lafortezza, R.; Carrus, G.; Sanesi, G.; Davies, C. Benefits and well-being perceived by people visiting green spaces in periods of heat stress. Urban For. Urban Green. 2009, 8, 97–108. [Google Scholar] [CrossRef]
- Nowak, D.J.; Crane, D.E.; Stevens, J.C. Air pollution removal by urban trees and shrubs in the United States. Urban For. Urban Green. 2006, 4, 115–123. [Google Scholar] [CrossRef]
- Oliveira, J.C.D; Epiphanio, J.C.N. Noise reduction in MODIS NDVI time series data based on spatial-temporal analysis. In Proceedings of the 2012 IEEE International Geoscience and Remote Sensing Symposium, Munich, Germany, 22–27 July 2012; pp. 2372–2375. [Google Scholar]
- Frumkin, H.; Bratman, G.N.; Breslow, S.J.; Cochran, B.; Kahn, P.H.; Lawler, J.J.; Levin, P.S.; Tandon, P.S.; Varanasi, U.; Wolf, K.L.; et al. Nature Contact and Human Health: A Research Agenda. Environ. Health Perspect. 2017, 125, 075001. [Google Scholar] [CrossRef] [PubMed]
- Hartig, T.; Mitchell, R.; de Vries, S.; Frumkin, H. Nature and health. Annu. Rev. Public Health 2014, 35, 207–228. [Google Scholar] [CrossRef] [PubMed]
- Bowler, D.E.; Buyung-Ali, L.M.; Knight, T.M.; Pullin, A.S. A systematic review of evidence for the added benefits to health of exposure to natural environments. BMC Public Health 2010, 10, 456. [Google Scholar] [CrossRef] [PubMed]
- McMorris, O.; Villeneuve, P.J.; Su, J.; Jerrett, M. Urban greenness and physical activity in a national survey of Canadians. Environ. Res. 2015, 137, 94–100. [Google Scholar] [CrossRef] [PubMed]
- Richardson, E.A.; Pearce, J.; Mitchell, R.; Kingham, S. Role of physical activity in the relationship between urban green space and health. Public Health 2013, 127, 318–324. [Google Scholar] [CrossRef] [PubMed]
- Banay, R.F.; Bezold, C.P.; James, P.; Hart, J.E.; Laden, F. Residential greenness: Current perspectives on its impact on maternal health and pregnancy outcomes. Int. J. Womens Health 2017, 9, 133–144. [Google Scholar] [CrossRef] [PubMed]
- Bezold, C.P.; Banay, R.F.; Coull, B.A.; Hart, J.E.; James, P.; Kubzansky, L.D.; Missmer, S.A.; Laden, F. The relationship between surrounding greenness in childhood and adolescence and depressive symptoms in adolescence and early adulthood. Ann. Epidemiol. 2018, 28, 213–219. [Google Scholar] [CrossRef] [PubMed]
- James, P.; Banay, R.F.; Hart, J.E.; Laden, F. A Review of the Health Benefits of Greenness. Curr. Epidemiol. Rep. 2015, 2, 131–142. [Google Scholar] [CrossRef] [PubMed]
- Weier, J.; Herring, D. Measuring Vegetation (NDVI & EVI). Available online: http://earthobservatory.nasa.gov/Features/MeasuringVegetation/measuring_vegetation_2.php (accessed on 20 May 2016).
- Kessner, D.M.; Singer, J.; Kalk, C.W.; Shlesinger, E.R. Chapter 2. In Infant Death: An Analysis by Maternal Risk and Health Care; Institute of Medicine and National Academy of Sciences: Washington, DC, USA, 1973. [Google Scholar]
- U.S. Census Bureau American Community Survey, 2010 5-Year Estimates. Available online: https://factfinder.census.gov (accessed on 29 November 2017).
- Bell, M.L.; Belanger, K.; Ebisu, K.; Gent, J.F.; Lee, H.J.; Koutrakis, P.; Leaderer, B.P. Prenatal Exposure to Fine Particulate Matter and Birth Weight. Epidemiol. Camb. Mass 2010, 21, 884–891. [Google Scholar] [CrossRef] [PubMed]
- Darrow, L.A.; Klein, M.; Strickland, M.J.; Mulholland, J.A.; Tolbert, P.E. Ambient air pollution and birth weight in full-term infants in Atlanta, 1994–2004. Environ. Health Perspect. 2011, 119, 731–737. [Google Scholar] [CrossRef] [PubMed]
- Kloog, I.; Melly, S.J.; Ridgway, W.L.; Coull, B.A.; Schwartz, J. Using new satellite based exposure methods to study the association between pregnancy PM2.5 exposure, premature birth and birth weight in Massachusetts. Environ. Health Glob. Access Sci. Source 2012, 11, 40. [Google Scholar] [CrossRef] [PubMed]
- Stieb, D.M.; Chen, L.; Eshoul, M.; Judek, S. Ambient air pollution, birth weight and preterm birth: A systematic review and meta-analysis. Environ. Res. 2012, 117, 100–111. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; Luo, X.; Zhao, C.; Zhang, B.; Tao, J.; Yang, Z.; Ma, W.; Liu, T. The associations between birth weight and exposure to fine particulate matter (PM2.5) and its chemical constituents during pregnancy: A meta-analysis. Environ. Pollut. Barking Essex 1987 2016, 211, 38–47. [Google Scholar] [CrossRef] [PubMed]
- Kloog, I.; Chudnovsky, A.A.; Just, A.C.; Nordio, F.; Koutrakis, P.; Coull, B.A.; Lyapustin, A.; Wang, Y.; Schwartz, J. A new hybrid spatio-temporal model for estimating daily multi-year PM2.5 concentrations across northeastern USA using high resolution aerosol optical depth data. Atmos. Environ. 2014, 95, 581–590. [Google Scholar] [CrossRef] [PubMed]
- US Department of Commerce Census Bureau Geographic Areas Reference Manual: Chapter 12. Available online: https://www.census.gov/geo/reference/garm.html (accessed on 17 April 2018).
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2017. [Google Scholar]
- Dadvand, P.; Rivas, I.; Basagaña, X.; Alvarez-Pedrerol, M.; Su, J.; De Castro Pascual, M.; Amato, F.; Jerret, M.; Querol, X.; Sunyer, J.; et al. The association between greenness and traffic-related air pollution at schools. Sci. Total Environ. 2015, 523, 59–63. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.-Y.; Park, S.-A.; Jung, S.-J.; Lee, J.-Y.; Son, K.-C.; An, Y.-J.; Lee, S.-W. Physiological and psychological responses of humans to the index of greenness of an interior space. Complement. Ther. Med. 2016, 28, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Wilker, E.H.; Wu, C.-D.; McNeely, E.; Mostofsky, E.; Spengler, J.; Wellenius, G.A.; Mittleman, M.A. Green space and mortality following ischemic stroke. Environ. Res. 2014, 133, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Sharma, D.; Shastri, S.; Sharma, P. Intrauterine Growth Restriction: Antenatal and Postnatal Aspects. Clin. Med. Insights Pediatr. 2016, 10, 67–83. [Google Scholar] [CrossRef] [PubMed]
- Agay-Shay, K.; Peled, A.; Crespo, A.V.; Peretz, C.; Amitai, Y.; Linn, S.; Friger, M.; Nieuwenhuijsen, M.J. Green spaces and adverse pregnancy outcomes. Occup. Environ. Med. 2014, 71, 562–569. [Google Scholar] [CrossRef] [PubMed]
- James, P.; Hart, J.E.; Hipp, J.A.; Mitchell, J.A.; Kerr, J.; Hurvitz, P.M.; Glanz, K.; Laden, F. GPS-Based Exposure to Greenness and Walkability and Accelerometry-Based Physical Activity. Cancer Epidemiol. Biomark. Prev. Publ. Am. Assoc. Cancer Res. Cosponsored Am. Soc. Prev. Oncol. 2017, 26, 525–532. [Google Scholar] [CrossRef] [PubMed]
- Grazuleviciene, R.; Danileviciute, A.; Dedele, A.; Vencloviene, J.; Andrusaityte, S.; Uždanaviciute, I.; Nieuwenhuijsen, M.J. Surrounding greenness, proximity to city parks and pregnancy outcomes in Kaunas cohort study. Int. J. Hyg. Environ. Health 2015, 218, 358–365. [Google Scholar] [CrossRef] [PubMed]
- Duncan, G.J.; Daly, M.C.; McDonough, P.; Williams, D.R. Optimal Indicators of Socioeconomic Status for Health Research. Am. J. Public Health 2002, 92, 1151–1157. [Google Scholar] [CrossRef]
- Winkleby, M.A.; Jatulis, D.E.; Frank, E.; Fortmann, S.P. Socioeconomic status and health: How education, income, and occupation contribute to risk factors for cardiovascular disease. Am. J. Public Health 1992, 82, 816–820. [Google Scholar] [CrossRef] [PubMed]





| Variable | Overall | NDVI Q1 (Mean < 0.38) | NDVI Q4 (Mean > 0.60) |
|---|---|---|---|
| Continuous Variables (mean ± s.d.) | |||
| Residential Greenness (NDVI) | 0.49 ± 0.15 | 0.29 ± 0.07 | 0.67 ± 0.05 |
| Birthweight (g) | 3441 ± 472 | 3400 ± 472 | 3477 ± 468 |
| PM2.5 (µg/m3) | 10.1 ± 1.4 | 10.5 ± 1.4 | 9.8 ± 1.3 |
| Clinical Gestational Age (weeks) | 39.3 ± 1.2 | 39.4 ± 1.2 | 39.3 ± 1.1 |
| Mother’s Age (years) | 30.1 ± 6.0 | 28.8 ± 6.2 | 31.3 ± 5.7 |
| Census Black Population Proportion | 0.08 ± 0.15 | 0.11 ± 0.17 | 0.04 ± 0.10 |
| Census Median Household Income ($10,000s) | 6.8 ± 3.3 | 5.2 ± 2.7 | 8.2 ± 3.3 |
| Binary and Categorical Variables (%) | |||
| Newborn Female Sex | 49.0 | 49.0 | 49.1 |
| Term Low Birthweight | 2.1 | 2.1 | 1.8 |
| Small for Gestational Age | 9.1 | 9.1 | 8.3 |
| Parity: First-born | 54.7 | 54.7 | 57.8 |
| Mother Married | 68.9 | 68.9 | 78.7 |
| Government Support for Prenatal Care | 33.0 | 33.0 | 21.5 |
| Maternal Smoking | 13.7 | 13.7 | 13.2 |
| Gestational Diabetes | 4.0 | 4.0 | 3.8 |
| Other Diabetes | 0.9 | 0.9 | 0.8 |
| High Blood Pressure during Pregnancy | 3.3 | 3.3 | 3.3 |
| Chronic High Blood Pressure | 1.2 | 1.2 | 1.1 |
| Census Tract Population Density > 1000 people/sq. mile | 76.8 | 94.9 | 53.0 |
| Season of Birth | |||
| Winter | 24.4 | 24.4 | 28.2 |
| Spring | 25.1 | 25.1 | 14.1 |
| Summer | 26.0 | 26.0 | 16.1 |
| Fall | 24.5 | 24.5 | 41.7 |
| Mode of Delivery | |||
| Vaginal | 65.5 | 65.5 | 64.4 |
| Forceps | 0.6 | 0.6 | 0.6 |
| Vacuum | 3.6 | 3.6 | 3.5 |
| First Caesarian Birth | 16.7 | 16.7 | 16.4 |
| Repeat Caesarian | 12.1 | 12.1 | 13.5 |
| Vaginal Birth after previous Caesarean Birth | 1.6 | 1.6 | 1.7 |
| Maternal Race | |||
| White | 71.9 | 71.9 | 85.4 |
| Black | 8.4 | 8.4 | 4.5 |
| Asian | 7.6 | 7.6 | 5.8 |
| American Indian | 0.2 | 0.2 | 0.3 |
| Other | 11.9 | 11.9 | 4.0 |
| Kessner Index for Prenatal Care | |||
| Adequate | 78.6 | 78.6 | 81.9 |
| Intermediate | 17.0 | 17.0 | 14.6 |
| Inadequate | 3.3 | 3.3 | 2.5 |
| No Prenatal Care | 1.2 | 1.2 | 1.0 |
| Maternal Education | |||
| Less than High School | 10.7 | 10.7 | 5.4 |
| High School | 24.0 | 24.0 | 19.0 |
| Some College | 22.3 | 22.3 | 23.1 |
| College | 26.3 | 26.3 | 32.6 |
| Advanced Degree | 16.7 | 16.7 | 20.0 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fong, K.C.; Kloog, I.; Coull, B.A.; Koutrakis, P.; Laden, F.; Schwartz, J.D.; James, P. Residential Greenness and Birthweight in the State of Massachusetts, USA. Int. J. Environ. Res. Public Health 2018, 15, 1248. https://doi.org/10.3390/ijerph15061248
Fong KC, Kloog I, Coull BA, Koutrakis P, Laden F, Schwartz JD, James P. Residential Greenness and Birthweight in the State of Massachusetts, USA. International Journal of Environmental Research and Public Health. 2018; 15(6):1248. https://doi.org/10.3390/ijerph15061248
Chicago/Turabian StyleFong, Kelvin C., Itai Kloog, Brent A. Coull, Petros Koutrakis, Francine Laden, Joel D. Schwartz, and Peter James. 2018. "Residential Greenness and Birthweight in the State of Massachusetts, USA" International Journal of Environmental Research and Public Health 15, no. 6: 1248. https://doi.org/10.3390/ijerph15061248
APA StyleFong, K. C., Kloog, I., Coull, B. A., Koutrakis, P., Laden, F., Schwartz, J. D., & James, P. (2018). Residential Greenness and Birthweight in the State of Massachusetts, USA. International Journal of Environmental Research and Public Health, 15(6), 1248. https://doi.org/10.3390/ijerph15061248