General Practice Care for Patients with Rare Diseases in Belgium. A Cross-Sectional Survey

 , ,
, ,
Abstract
1. Introduction
- Examine care characteristics of rare disease patients; and
- Examine the importance of rare diseases in general practice by its caseload, i.e., the number of cases in the SGP network, its estimated prevalence in the Belgian general practice population and by comparing the GP-encounter frequency among rare disease patients in the SGP and the Belgian general practice population. We also compared patients’ age in the two populations.
2. Materials and Methods
2.1. Settings and Participants
2.2. Data Collection
2.3. Measurements
2.3.1. The Patient Level
2.3.2. The Level of the Sentinel General Practices
2.4. Analysis
3. Results
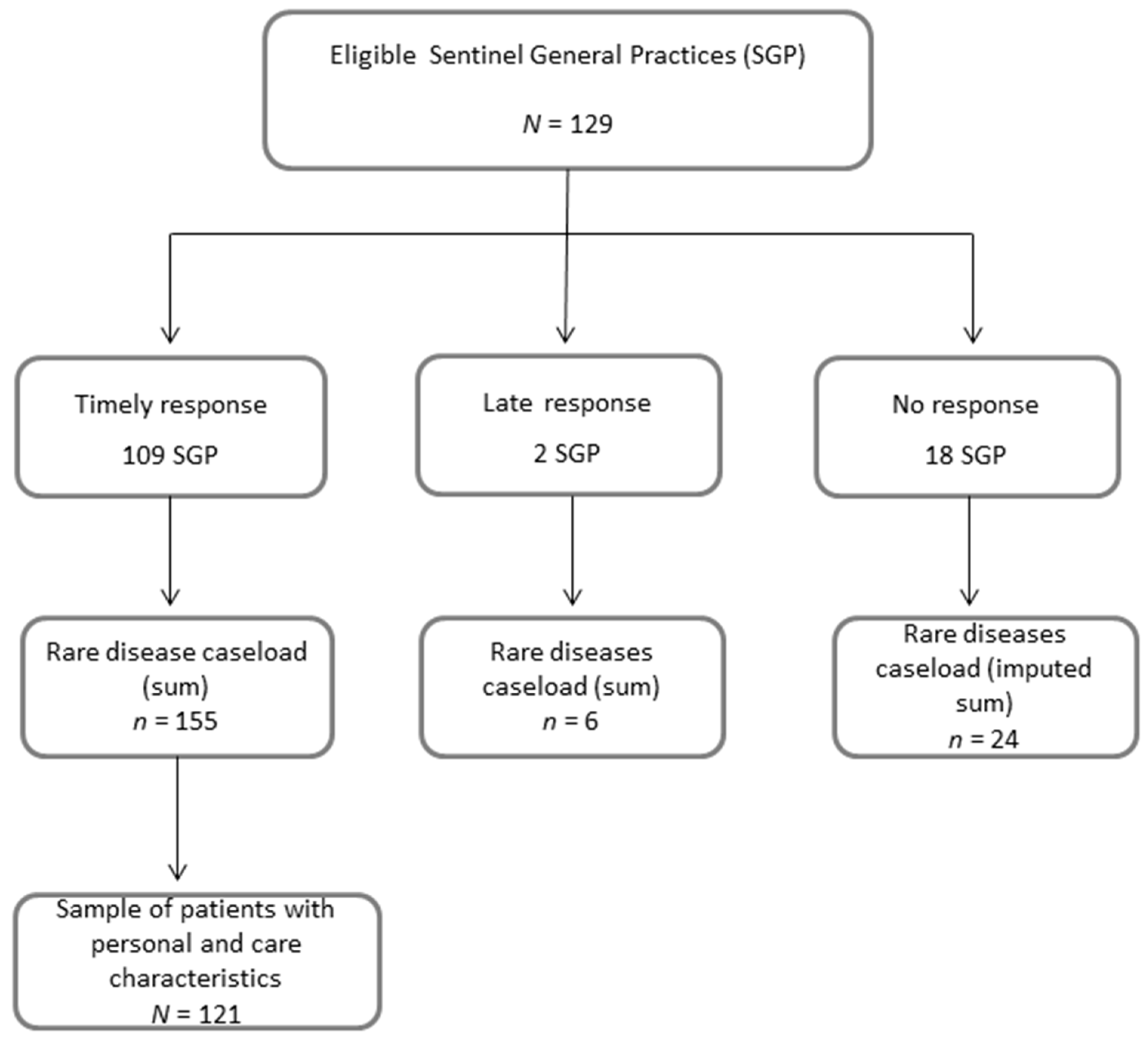
3.1. Study Participation of the Sentinel General Practices
3.2. Personal and Care Characteristics of the Sample of Rare Disease Patients
3.3. Caseload by Sentinel General Practices
3.4. General Practitioner Encounter Frequency by Rare Disease Patients Compared to the Total General Practice Population
3.5. Prevalence of Rare Disease Patients in Belgian General Practice
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kole, A.; Faurisson, F. Rare diseases social epidemiology: Analysis of inequalities. Adv. Exp. Med. Biol. 2010, 686, 223–250. [Google Scholar] [PubMed]
- Knight, A.W.; Senior, T.P. The common problem of rare disease in general practice. Med. J. Aust. 2006, 185, 82–83. [Google Scholar] [PubMed]
- Senior, T.; Knight, A. Rare diseases: A role for primary care. Lancet 2008, 372, 890. [Google Scholar] [CrossRef]
- Brussels, King Baudouin Foundation (www.kbs-frb.be). Fund for Rare Diseases and Orphan Drugs. Primary Care for Rare Disease Patients: The Missing Link? Symposium on 19 November 2015. Available online: https://kce.fgov.be/sites/default/files/atoms/files/d20091027332.pdf (accessed on 23 May 2018).
- Richter, T.; Nestler-Parr, S.; Babela, R.; Khan, Z.M.; Tesoro, T.; Molsen, E.; Hughes, D.A. Rare Disease Terminology and Definitions-A Systematic Global Review: Report of the ISPOR Rare Disease Special Interest Group. Value Health 2015, 18, 906–914. [Google Scholar] [CrossRef] [PubMed]
- The Council of the European Union. Council recommendation of 8 June 2009 on an action in the field of rare diseases (2009/C 151/02). Off. J. Eur. Union 2009, 52, 7–10. [Google Scholar]
- Avellaneda Fernandez, A.; Izquierdo, M.M.; Luengo, G.S.; Arenas, M.J.; Ramon, J.R. Need for primary care training in rare diseases. Aten Primaria 2006, 38, 345–348. [Google Scholar] [PubMed]
- Avellaneda Fernandez, A.; Perez, M.A.; Pombo, A.G.; Gutierrez, D.E.; Izquierdo, M.M. Perception of rare diseases by the primary care physicians. Semergen 2012, 38, 421–431. [Google Scholar] [PubMed]
- McClain, M.R.; Cooley, W.C.; Keirns, T.; Smith, A. A survey of the preferences of primary care physicians regarding the comanagement with specialists of children with rare or complex conditions. Clin. Pediatr. 2014, 53, 566–570. [Google Scholar] [CrossRef] [PubMed]
- Miteva, T.; Jordanova, R.; Iskrov, G.; Stefanov, R. General knowledge and awareness on rare diseases among general practitioners in Bulgaria. Georgian Med. News 2011, 193, 16–19. [Google Scholar]
- Phillips, W.R. Zebras on the commons: Rare conditions in family practice. J. Am. Board Fam. Pract. 2004, 17, 283–286. [Google Scholar] [CrossRef] [PubMed]
- Van de Laar, F.A.; Bor, H.; van de Lisdonk, E.H. Prevalence of zebras in general practice: Data from the Continuous Morbidity Registration Nijmegen. Eur. J. Gen. Pract. 2008, 14 (Suppl. 1), 44–46. [Google Scholar] [CrossRef] [PubMed]
- Van Nispen, R.; Rijken, M. Ordinary care for the extraordinary patient. Rare diseases in general practice. Huisarts en Wetenschap 2007, 50, 349–354. [Google Scholar]
- Van Casteren, V. Thirty years Registration Network of Sentinel General Practitioners. Arch. Public Health 2009, 67 (Suppl. 2), 3–15. [Google Scholar]
- Boffin, N.; Moreels, S.; Van Casteren, V. The Belgian Network of Sentinel General Practices between 2007 and 2012: A Short Report; Scientific Institute of Public Health: Belgium, Brussels, 2013; Available online: https://www.wiv-isp.be/epidemio/epien/medven/D_2013_2505_40.pdf (accessed on 5 April 2018).
- Ayme, S.; Bellet, B.; Rath, A. Rare diseases in ICD11: Making rare diseases visible in health information systems through appropriate coding. Orphanet J. Rare Dis. 2015, 10, 35. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [PubMed]
- EURORDIS. Survey of the Delay in Diagnosis for 8 Rare Diseases in Europe (‘EURORDISCARE 2’). 2007. Available online: http://www.eurordis.org/sites/default/files/publications/Fact_Sheet_Eurordiscare2.pdf (accessed on 5 April 2018).
- Budych, K.; Helms, T.M.; Schultz, C. How do patients with rare diseases experience the medical encounter? Exploring role behavior and its impact on patient-physician interaction. Health Policy 2012, 105, 154–164. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Median (IQR) | n/N (%) |
|---|---|---|
| Patient age (N = 121) | 44 (24–60) | - |
| Number of GP–patient encounters in 2015 (N = 118) | 5 (3–10) | - |
| Number of care contacts (with other health professionals) about patient in 2015 (N = 112) | 2 (1–5) | - |
| Length of patient-GP relation in years (N = 112) | 14 (5–19) | - |
| Duration of disease (symptoms) in years (N = 97) | 8 (3–16) | - |
| Patient gender: female | - | 71/120 (59.2) |
| GP was first caregiver seen for rare disease (symptoms) | - | 41/111 (36.9) |
| Diagnosis was confirmed | - | 116/117 (99.2) |
| Diagnostic delay (≥1 year between first suspicion and confirmation of diagnosis) | - | 23/94 (24.5) |
| GP referred patient to facility where diagnosis was established | - | 43/120 (35.8) |
| Reasons(s) why GP referral was unnecessary/unsuccessful | ||
| Diagnosis was already known | - | 40/77 (52.0) |
| Referral by another caregiver or self-referral | - | 24/77 (31.2) |
| GP had first referred to other care facility | - | 6/77 (7.9) |
| GP’s medical knowledge of disease is (very) good | - | 34/116 (29.3) |
| Usefulness of Orphanet information about the patient’s rare disease is not applicable/no use | - | 103/121 (85.1) |
| Rate Ratio for Number of Cases (95% Confidence Intervals (CI)) | Adjusted Rate Ratio for Number of Cases (95% CI) 2,3 | |
|---|---|---|
| SGP gender composition (N = 110) | ||
| <50% men | No significant model obtained | |
| ≥50% men | ||
| SGP age composition (N = 110) | ||
| <median | No significant model obtained | |
| ≥median | ||
| Region (N = 111) | ||
| Wallonia or Brussels | No significant model obtained | |
| Flanders | ||
| Population density of SGP municipality (N = 111) | ||
| Low or mixed | 1.84 (1.12–3.00) | |
| High | ref | |
| Use of certified electronic health records (EHR (N = 110) | ||
| Yes | 4.05 (1.55–10.60) | 2.85 (1.09–7.45) |
| No | ref | Ref |
| Practice organization (N = 111) | ||
| Group practice | 2.37 (1.50–3.76) | 2.05 (1.29–3.28) |
| Solo practice | ref | ref |
| Number of reporting (trainee) GPs (N = 110) | ||
| >1 | 1.76 (0.97–3.18) | |
| 1 | ref | |
| Number of weekly patient contacts in 2015 (N = 111) | ||
| ≥median | No significant model obtained | |
| <median |
| General Practice Population (BCHI) | SGP Rare Disease Population | ||
|---|---|---|---|
| N = 208,029 | N = 121 1 | ||
| Age groups (4) | Mean number of GP encounters (95% CI) 2 | ||
| ≤24 | 3.3 (3.3–3.4) | 6.0 (2.6–9.4) | |
| 25–44 | 4.1 (4.1–4.2) | 8.4 (6.0–10.8) | |
| 45–64 | 5.3 (5.3–5.3) | 7.3 (5.6–9.0) | |
| ≥65 | 8.9 (8.8–8.9) | 8.2 (5.9–10.5) | |
| Total | 5.4 (5.4–5.4) | 7.3 (6.1–8.5) | |
| Age groups (4) | Age distribution [Column % (95% CI)] 2 | ||
| ≤24 | 23.8 (23.6–24.0) | 28.1 (20.3–37.0) | |
| 25–44 | 24.1 (23.9–24.3) | 23.1 (16.0–31.7) | |
| 45–64 | 28.5 (28.3–28.7) | 35.5 (27.0–44.8) | |
| ≥65 | 23.6 (23.4–23.7) | 13.2 (7.8–20.6) | |
| Total | 100% | 100% | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boffin, N.; Swinnen, E.; Wens, J.; Urbina, M.; Van der Heyden, J.; Van Casteren, V. General Practice Care for Patients with Rare Diseases in Belgium. A Cross-Sectional Survey. Int. J. Environ. Res. Public Health 2018, 15, 1180. https://doi.org/10.3390/ijerph15061180
Boffin N, Swinnen E, Wens J, Urbina M, Van der Heyden J, Van Casteren V. General Practice Care for Patients with Rare Diseases in Belgium. A Cross-Sectional Survey. International Journal of Environmental Research and Public Health. 2018; 15(6):1180. https://doi.org/10.3390/ijerph15061180
Chicago/Turabian StyleBoffin, Nicole, Elfriede Swinnen, Johan Wens, Montse Urbina, Johan Van der Heyden, and Viviane Van Casteren. 2018. "General Practice Care for Patients with Rare Diseases in Belgium. A Cross-Sectional Survey" International Journal of Environmental Research and Public Health 15, no. 6: 1180. https://doi.org/10.3390/ijerph15061180
APA StyleBoffin, N., Swinnen, E., Wens, J., Urbina, M., Van der Heyden, J., & Van Casteren, V. (2018). General Practice Care for Patients with Rare Diseases in Belgium. A Cross-Sectional Survey. International Journal of Environmental Research and Public Health, 15(6), 1180. https://doi.org/10.3390/ijerph15061180