Social Interventions to Prevent Heat-Related Mortality in the Older Adult in Rome, Italy: A Quasi-Experimental Study

 ,
,  , ,
, ,
Abstract
1. Introduction
2. Methods
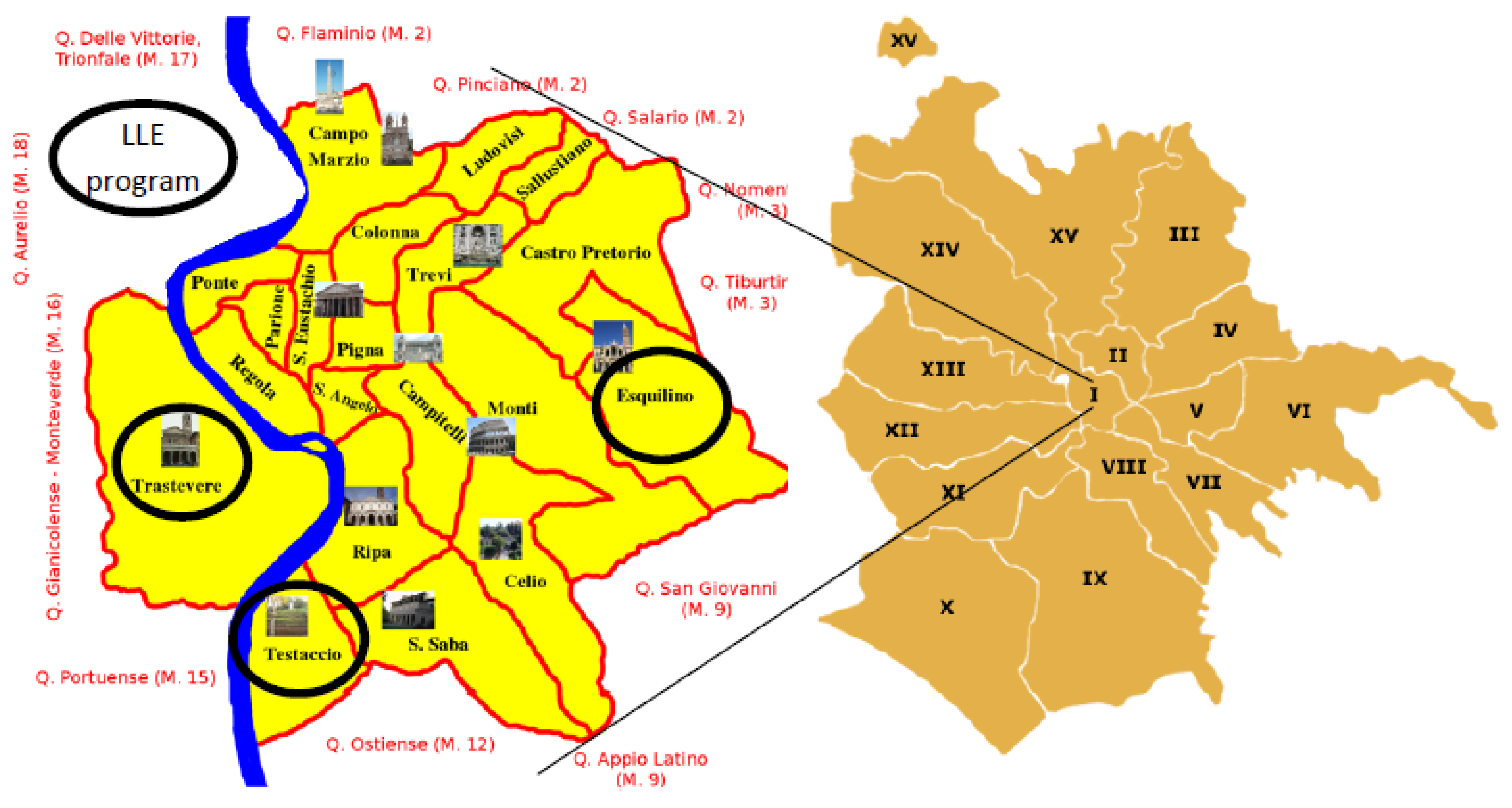
2.1. Population and Settings
2.2. Definition of Heat Waves
2.3. The Intervention
2.4. Data Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Scarcella, P.; Liotta, G.; Marazzi, M.C.; Carbini, R.; Palombi, L. Analysis of survival in a sample of elderly patients from Ragusa, Italy on the basis of a primary care level multidimensional evaluation. Arch. Gerontol. Geriatr. 2005, 40, 147–156. [Google Scholar] [CrossRef] [PubMed]
- Cho, J.; Lee, I.; Park, S.H.; Jin, Y.; Kim, D.; Kong, J.Y.; Kang, H. Socioconomic status, frailty, and all-cause mortality in Korean older adults: A 3-year population-based prospective study. Biomed. Res. Int. 2017. [Google Scholar] [CrossRef] [PubMed]
- Gilardi, F.; Scarcella, P.; Proietti, M.G.; Capobianco, G.; Rocco, G.; Capanna, A.; Mancinelli, S.; Marazzi, M.C.; Palombi, L.; Liotta, G. Identification of the higher rate of death and hospital services use according to frailty: A cluster analysis in a longitudinal cohort study. Eur. J. Public Health 2018. [Google Scholar] [CrossRef] [PubMed]
- Culqui, D.R.; Díaz, J.; Simón, F.; Linares, C. Impact of the effects of heat waves on mortality in the city of Madrid, Spain during the period 1990–2009. Rev. Española Salud Publ. 2013, 87, 277–282. [Google Scholar] [CrossRef] [PubMed]
- Ragettli, M.S.; Vicedo-Cabrera, A.M.; Schindler, C.; Röösli, M. Exploring the association between heat and mortality in Switzerland between 1995 and 2013. Environ. Res. 2017, 158, 703–709. [Google Scholar] [CrossRef] [PubMed]
- Fouillet, A.; Rey, G.; Laurent, F.; Pavillon, G.; Bellec, S.; Guihenneuc-Jouyaux, C.; Clavel, J.; Jougla, E.; Hémon, D. Excess mortality related to the August 2003 heat wave in France. Int. Arch. Occup. Environ. Health 2006, 80, 16. [Google Scholar] [CrossRef] [PubMed]
- García-Herrera, R.; Díaz, J.; Trigo, R.M.; Luterbacher, J.; Fischer, E.M. A review of the European summer heat wave of 2003. J. Crit. Rev. Environ. Sci. Technol. 2010, 40, 167–306. [Google Scholar] [CrossRef]
- Nogueira, P.J.; Falcão, J.M.; Contreiras, M.T.; Paixão, E.; Brandão, J.; Batista, I. Mortality in Portugal associated with the heat wave of August 2003: Early estimation of effect, using a rapid method. Eurosurveillance 2005, 10, 150–153. [Google Scholar] [CrossRef] [PubMed]
- Conti, S.; Meli, P.; Minelli, G.; Solimini, R.; Toccaceli, V.; Vichi, M.; Beltrano, C.; Perini, L. Epidemiologic study of mortality during the summer 2003 heat wave in Italy. Environ. Res. 2005, 98, 390–399. [Google Scholar] [CrossRef] [PubMed]
- Michelozzi, P.; de’ Donato, F.; Scortichini, M.; De Sario, M.; Asta, F.; Agabiti, N.; Guerra, R.; de Martino, A.; Davoli, M. On the increase in mortality in Italy in 2015: Analysis of seasonal mortality in the 32 municipalities included in the Surveillance system of daily mortality. Epidemiol. Prev. 2016, 40, 22–28. [Google Scholar] [PubMed]
- Urban, A.; Hanzlíková, H.; Kyselý, J.; Plavcová, E. Impacts of the 2015 heat waves on mortality in the Czech Republic—A comparison with previous heat waves. Int. J. Environ. Res. Public Health 2017, 14, 1562. [Google Scholar] [CrossRef] [PubMed]
- Steul, K.; Schade, M.; Heudorf, U. Mortality during heat waves 2003–2015 in Frankfurt am Main—The 2003 heat wave and its implications. Int. J. Hyg. Environ. Health 2018, 221, 81–86. [Google Scholar] [CrossRef] [PubMed]
- Schifano, P.; Leone, M.; De Sario, M.; de’Donato, F.; Bargagli, A.M.; D’Ippoliti, D.; Marino, C.; Michelozzi, P. Changes in the effects of heat on mortality among the elderly from 1998–2010: Results from a multicenter time series study in Italy. Environ. Health 2012, 3, 11–58. [Google Scholar] [CrossRef] [PubMed]
- D’Ippoliti, D.; Michelozzi, P.; Marino, C.; D’Ovidio, M.; Kirchmayer, U.; Menne, B. The role of gender in the impact evaluation of heat waves on mortality in European cities. Epidemiology 2007, 18, S125. [Google Scholar] [CrossRef]
- Perčič, S.; Kukec, A.; Cegnar, T.; Hojs, A. Number of heat wave deaths by diagnosis, sex, age groups, and area, in Slovenia, 2015 vs. 2003. Int. J. Environ. Res. Public Health 2018, 15, 173. [Google Scholar] [CrossRef] [PubMed]
- Pascal, M.; Le Tertre, A.; Saoudi, A. Quantification of the heat wave effect on mortality in nine French cities during summer 2006. Version 2. PLoS Curr. 2012, 4. [Google Scholar] [CrossRef] [PubMed]
- Heudorf, U.; Schade, M. Heat waves and mortality in Frankfurt am Main, Germany, 2003–2013: What effect do heat-health action plans and the heat warning system have? Z. Gerontol. Geriatr. 2014, 47, 475–482. [Google Scholar] [CrossRef] [PubMed]
- Morabito, M.; Crisci, A.; Gioli, B.; Gualtieri, G.; Toscano, P.; Di Stefano, V.; Orlandini, S.; Gensini, G.F. Urban-hazard risk analysis: Mapping of heat-related risks in the elderly in major Italian cities. PLoS ONE 2015, 10, e0127277. [Google Scholar] [CrossRef] [PubMed]
- Benmarhnia, T.; Kihal-Talantikite, W.; Ragettli, M.S.; Deguen, S. Small-area spatiotemporal analysis of heatwave impacts on elderly mortality in Paris: A cluster analysis approach. Sci. Total Environ. 2017, 592, 288–294. [Google Scholar] [CrossRef] [PubMed]
- Marazzi, M.C.; Inzerilli, M.C.; Madaro, O.; Palombi, L.; Scarcella, P.; Orlando, S.; Maurici, M.; Liotta, G. Impact of the community-based active monitoring program on the long term care services use and in-patient admissions of the over-74 population. Adv. Aging Res. 2015, 4, 187–194. [Google Scholar] [CrossRef]
- Woolcock, M.; Narayan, D. Social capital: Implications for development theory, research and policy. World Bank Res. Obs. 2000, 15, 225–249. [Google Scholar] [CrossRef]
- Inkpen, A.C.; Tsang, E.W. Social capital, networks, and knowledge transfer. Acad. Manag. Rev. 2005, 30, 146–165. [Google Scholar] [CrossRef]
- Smith, S.G.; Jackson, S.E.; Kobayashi, L.C.; Steptoe, A. Social isolation, health literacy, and mortality risk: Findings from the English Longitudinal Study of Ageing. Health Psychol. 2018, 37, 160–169. [Google Scholar] [CrossRef] [PubMed]
- Holt-Lunstad, J.; Smith, T.B.; Baker, M.; Harris, T.; Stephenson, D. Loneliness and social isolation as risk factors for mortality: A meta-analytic review. Perspect. Psychol. Sci. 2015, 10, 227–237. [Google Scholar] [CrossRef] [PubMed]
- Pantell, M.; Rehkopf, D.; Jutte, D.; Syme, S.L.; Balmes, J.; Adler, N. Social isolation: A predictor of mortality comparable to traditional clinical risk factors. Am. J. Public Health 2013, 103, 2056–2062. [Google Scholar] [CrossRef] [PubMed]
- Semenza, J.C.; Rubin, C.H.; Falter, K.H.; Selanikio, J.D.; Flanders, W.D.; Howe, H.L.; Wilhelm, J.L. Heat-related deaths during the July 1995 heat wave in Chicago. N. Engl. J. Med. 1996, 335, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Klinenberg, E. Heat Wave: A Social Autopsy of Disaster in Chicago; University of Chicago press: Chicago, IL, USA, 2015. [Google Scholar]
- Kaiser, R.; Le Tertre, A.; Schwartz, J.; Gotway, C.A.; Daley, W.R.; Rubin, C.H. The effect of the 1995 heat wave in Chicago on all-cause and cause-specific mortality. Am. J. Public Health Suppl. 1 2007, 97, S158–S162. [Google Scholar] [CrossRef] [PubMed]
- Kalkstein, L.S.; Barthel, C.D.; Green, J.S.; Nichols, M.C. A new spatial synoptic classification: Application to air mass analysis. Int. J. Climatol. 1996, 16, 983–1004. [Google Scholar] [CrossRef]
- Sheridan, S.C. The Re-development of a weather type classification scheme for North America. Int. J. Climatol. 2002, 22, 51–68. [Google Scholar] [CrossRef]
- Michelozzi, P.; de’ Donato, F.K.; Bargagli, A.M.; D’Ippoliti, D.; De Sario, M.; Marino, C.; Schifano, P.; Cappai, G.; Leone, M.; Kirchmayer, U.; et al. Surveillance of Summer Mortality and Preparedness to Reduce the Health Impact of Heat Waves in Italy. Int. J. Environ. Res. Public Health 2010, 7, 2256–2273. [Google Scholar] [CrossRef] [PubMed]
- Ministero Della Salute—Direzione Generale Della Programmazione Sanitaria. Rapporto Annuale sull’attività di Ricovero Ospedaliero, Dati SDO 2015. Roma, Settembre 2016. Pag. 148. Available online: http://www.salute.gov.it/imgs/C_17_pubblicazioni_2548_allegato.pdf (accessed on 5 April 2018).
- Keim, M.E. Building human resilience: The role of public health preparedness and response as an adaptation to climate change. Am. J. Prev. Med. 2008, 35, 508–516. [Google Scholar] [CrossRef] [PubMed]
- Rogers, D.P.; Tsikunov, V. Weather and Climate Resilience: Effective Preparedness through National Meteorological and Hydrological Services; Directions in Development, Environment and Sustainable Development: Washington, DC, USA, 2013. [Google Scholar]
- Jancloes, M.; Anderson, V.; Gosselin, P.; Mee, C.; Chong, N.J. WWOSC 2014: Research Needs for Better Health Resilience to Weather Hazards. Int. J. Environ. Res. Public Health 2015, 12, 2895–2900. [Google Scholar] [CrossRef] [PubMed]
- Yu, W.; Mengersen, K.; Wang, X.; Ye, X.; Guo, Y.; Pan, X.; Tong, S. Daily average temperature and mortality among the elderly: A meta-analysis and systematic review of epidemiological evidence. Int. J. Biometeorol. 2012, 56, 569. [Google Scholar] [CrossRef] [PubMed]
- Ballester, F.; Michelozzi, P.; Inĩguez, C. Weather, climate, and public health. JECH 2018, 57, 759–760. [Google Scholar] [CrossRef]
- Benmarhnia, T.; Deguen, S.; Kaufman, J.S.; Smargiassi, A. Review article: Vulnerability to heat-related mortality: A systematic review, meta-analysis, and meta-regression analysis. Epidemiology 2015, 26, 781–793. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, C.; Bella, A. L’impatto della Stagione Influenzale 2014/2015 in Italia. Available online: http://www.ccm-network.it/imgs/C_27_MAIN_page_1046_listaFile_List11_itemName_3_file.pdf (accessed on 20 December 2016).
- Huynen, M.; Martens, P.; Schram, D.; Weijenberg, M.P.; Kunst, A.E. The impact of heat waves and cold spells on mortality rates in the Dutch population. Environ. Health Perspect. 2001, 109, 463–470. [Google Scholar] [CrossRef] [PubMed]
- Gasparrini, A.; Armstrong, B. The impact of heat waves on mortality. Epidemiology 2011, 22, 68–73. [Google Scholar] [CrossRef] [PubMed]
- Bao, J.; Wang, Z.; Yu, C.; Li, X. The influence of temperature on mortality and its lag effect: A study in four Chinese cities with different latitudes. BMC Public Health 2016, 16, 375. [Google Scholar] [CrossRef] [PubMed]
- Folbert, E.C.; Hegeman, J.H.; Gierveld, R.; Van Netten, J.J.; Van Der Velde, D.; Ten Duis, H.J.; Slaets, J.P. Complications during hospitalization and risk factors in elderly patients with hip fracture following integrated orthogeriatric treatment. Arch. Orthop. Trauma Surg. 2017, 137, 507–515. [Google Scholar] [CrossRef] [PubMed]
- DEP—Regione Lazio. Risultati dei Sistemi di Allarme (HHWWS) e del Sistema di Sorveglianza della Mortalità Giornaliera (SiSMG) e Degli Accessi in Pronto Soccorso—Estate 2017. Available online: http://www.salute.gov.it/imgs/C_17_pubblicazioni_2654_allegato.pdf (accessed on 20 December 2017).




{kind=link}
{kind=link}
{kind=link}
| Urban Area | LLE Program | Population Average by Month during Summer 2015 | Population Weight * | Females (%) | Mean Age (2015) | Share of Population over 90 (%) | Mean Property Tax Valuation (€) (2015) | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Urban Areas | Total | |||||||||
| Centro Storico | No (Controls) | 2837 | 5724 | 162.71 | 55.28 | 81.81 | 8.34 | 10.3 | 1977 | 1767 |
| Aventino | 1136 | 65.16 | 64.24 | 81.83 | 11.11 | 1636 | ||||
| XX Settembre | 1255 | 71.97 | 60.15 | 82.73 | 10.41 | 1787 | ||||
| Celio | 496 | 28.44 | 59.92 | 82.34 | 11.47 | 1669 | ||||
| Trastevere | Yes (Cases) | 1470 | 6483 | 84.27 | 65.35 | 82.41 | 8.58 | 9.0 | 1733 | 1592 |
| Testaccio | 1124 | 64.43 | 62.07 | 82.42 | 8.66 | 1370 | ||||
| Esquilino | 3889 | 223.02 | 59.56 | 82.57 | 9.92 | 1674 | ||||
| Urban Zone | Controls | Cases | Moses’ Rank Test 2 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Centro Storico | Aventino | XX Settembre | Celio | Mean (SD) 1 | Trastevere | Testaccio | Esquilino | Mean (SD) 1 | ||
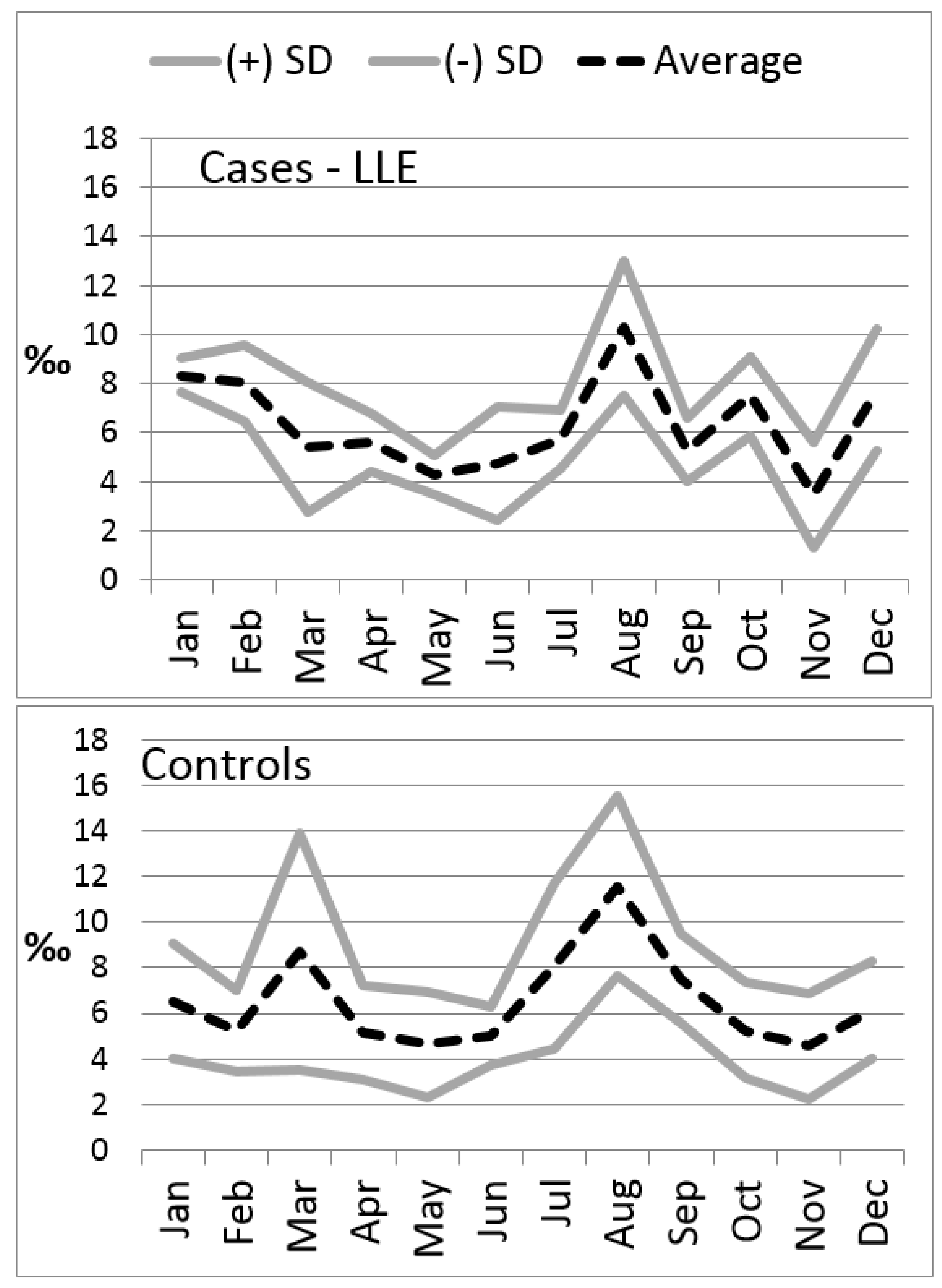
| Monthly average death rate (‰) October 2014–May 2015 | 5.75 | 5.45 | 4.72 | 8.34 | 6.0 (1.5) | 6.17 | 5.86 | 6.67 | 6.2 (0.4) | NS |
| Monthly average death rate (‰) June–September 2014 | 4.17 | 2.82 | 3.65 | 3.50 | 3.7 (0.6) | 3.66 | 4.93 | 4.38 | 4.3 (0.5) | <0.001 |
| Monthly average death rate (‰) June–September 2015 | 5.73 | 8.80 | 9.57 | 8.06 | 7.3 (2.0) | 5.95 | 7.12 | 6.43 | 6.4 (0.4) | <0.001 |
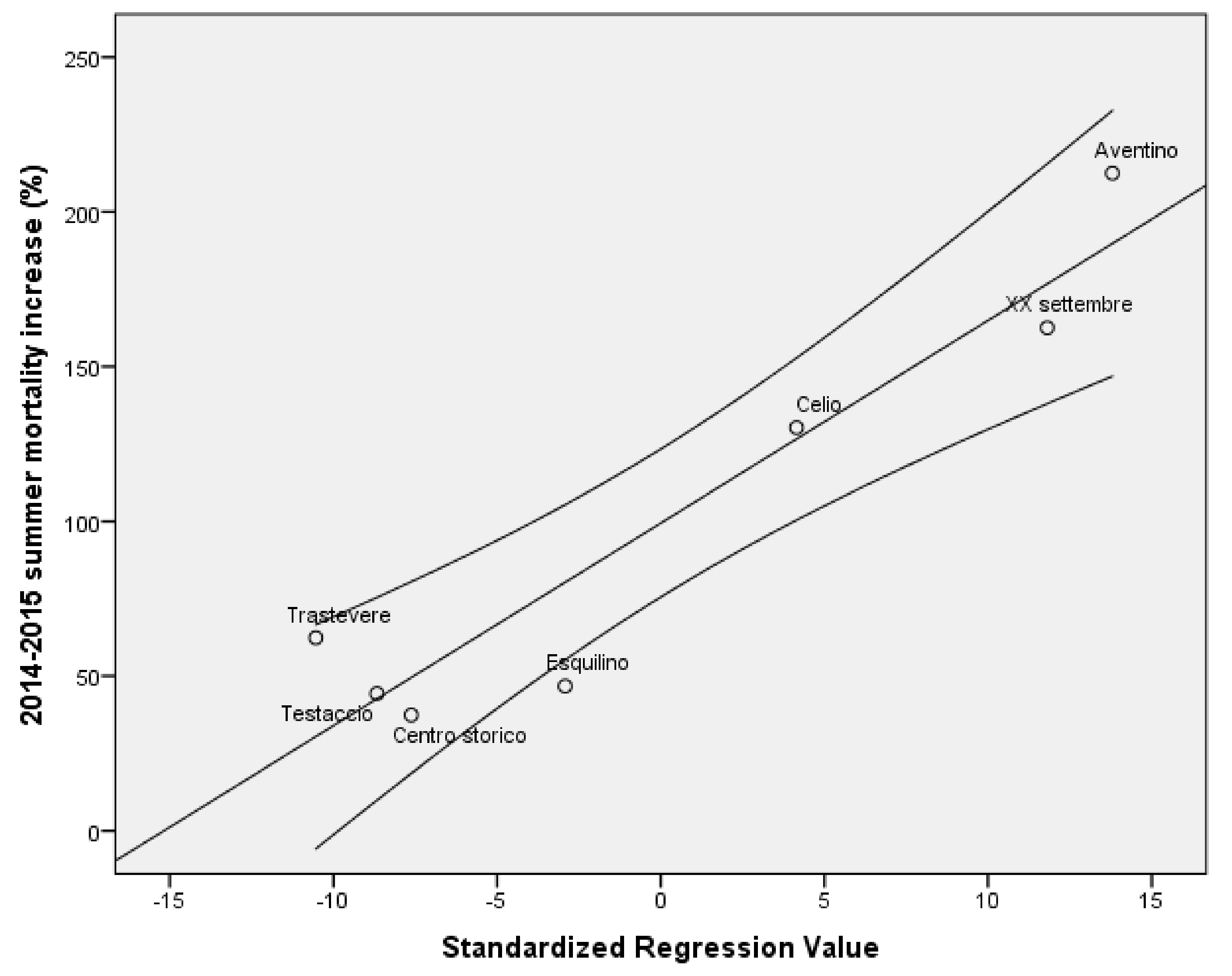
| Δ1: June–September 2015 vs. June–September 2014 (%) | 37.38 | 212.50 | 162.59 | 130.30 | 97.3 (73.1) | 62.37 | 44.32 | 46.71 | 48.8 (6.8) | <0.001 |
| Δ2: June–September 2015 vs. October 2014–May 2015 (%) | −0.41 | 61.62 | 102.96 | −3.34 | 35.4 (43.0) | −3.50 | 21.47 | −3.56 | 6.6 (6.7) | <0.001 |
| Monthly average death rate (‰) October–November 2015 | 5.09 | 6.15 | 2.37 | 5.96 | 4.7 (1.6) | 5.73 | 4.91 | 5.76 | 5.6 (0.4) | <0.001 |
| Δ3: October–November 2015 vs. June–September 2015 (%) | −11.02 | −30.08 | −75.21 | −26.00 | −35.6 (30.1) | −3.67 | −31.07 | −10.46 | −12.5 (10.5) | <0.001 |
| Δ2−Δ3 | 71.0 (67.3) | 19.1 (15.31) | NS | |||||||
| Non-standardized Coefficient | Standardized Coefficient | p | 95.0% Cl | |||
|---|---|---|---|---|---|---|
| B | Standard Error | Beta | Lower | Upper | ||
| (Constant) | −143.628 | 11.681 | <0.001 | −166.583 | −120.673 | |
| October 2014–May 2015 monthly mortality average | −32.714 | 1.567 | −0.431 | <0.001 | −35.793 | −29.634 |
| Share of the over 90 population | 45.481 | 1.046 | 0.792 | <0.001 | 43.426 | 47.537 |
| LLE program (no vs. yes) | −24.372 | 2.370 | −0.210 | <0.001 | −29.029 | −19.714 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liotta, G.; Inzerilli, M.C.; Palombi, L.; Madaro, O.; Orlando, S.; Scarcella, P.; Betti, D.; Marazzi, M.C. Social Interventions to Prevent Heat-Related Mortality in the Older Adult in Rome, Italy: A Quasi-Experimental Study. Int. J. Environ. Res. Public Health 2018, 15, 715. https://doi.org/10.3390/ijerph15040715
Liotta G, Inzerilli MC, Palombi L, Madaro O, Orlando S, Scarcella P, Betti D, Marazzi MC. Social Interventions to Prevent Heat-Related Mortality in the Older Adult in Rome, Italy: A Quasi-Experimental Study. International Journal of Environmental Research and Public Health. 2018; 15(4):715. https://doi.org/10.3390/ijerph15040715
Chicago/Turabian StyleLiotta, Giuseppe, Maria Chiara Inzerilli, Leonardo Palombi, Olga Madaro, Stefano Orlando, Paola Scarcella, Daniela Betti, and Maria Cristina Marazzi. 2018. "Social Interventions to Prevent Heat-Related Mortality in the Older Adult in Rome, Italy: A Quasi-Experimental Study" International Journal of Environmental Research and Public Health 15, no. 4: 715. https://doi.org/10.3390/ijerph15040715
APA StyleLiotta, G., Inzerilli, M. C., Palombi, L., Madaro, O., Orlando, S., Scarcella, P., Betti, D., & Marazzi, M. C. (2018). Social Interventions to Prevent Heat-Related Mortality in the Older Adult in Rome, Italy: A Quasi-Experimental Study. International Journal of Environmental Research and Public Health, 15(4), 715. https://doi.org/10.3390/ijerph15040715