Decision Tree Approach to the Impact of Parents’ Oral Health on Dental Caries Experience in Children: A Cross-Sectional Study

 ,
, 

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Participants and Study Design
2.2. Clinical Examination
2.3. Microbiological Examination
2.4. Study Analysis
C4.5: A DT-Based Classifier
3. Results
4. Discussion
5. Consent to Publish
6. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix A
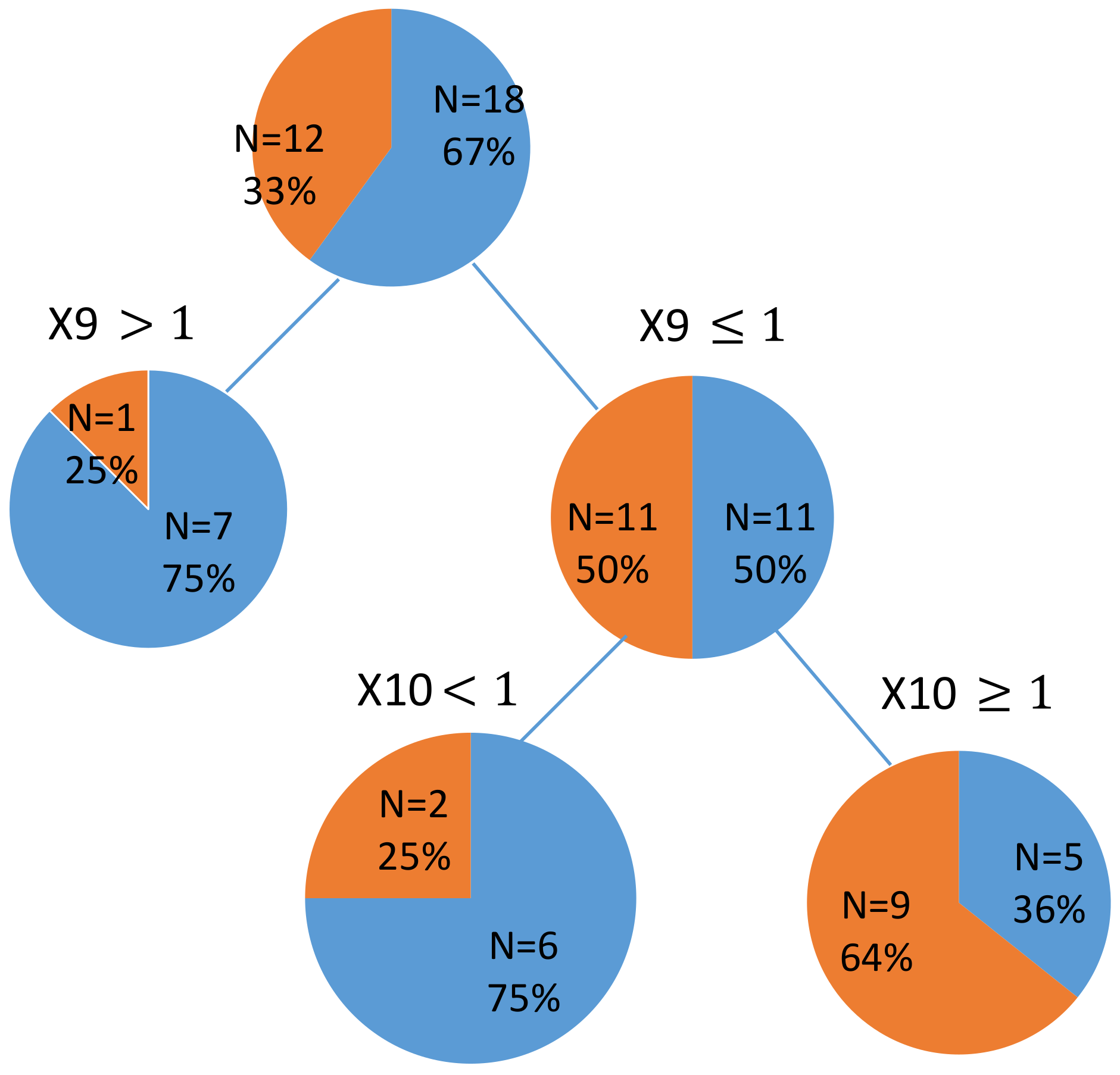
 children with dmft
children with dmft  children with dmft > 10; X9: Perio Check (parent); X10: Perio Check (Children).
children with dmft children with dmft > 10; X9: Perio Check (parent); X10: Perio Check (Children).
children with dmft > 10; X9: Perio Check (parent); X10: Perio Check (Children).
children with dmft children with dmft > 10; X9: Perio Check (parent); X10: Perio Check (Children).
References
- Powell, L.V. Caries prediction: A review of the literature. Community Dent. Oral Epidemiol. 1998, 26, 361–371. [Google Scholar] [CrossRef] [PubMed]
- Twetman, S.; Fontana, M. Patient caries risk assessment. Monogr. Oral Sci. 2009, 21, 91–101. [Google Scholar] [CrossRef] [PubMed]
- Duijster, D.; de Jong-Lenters, M.; de Ruiter, C.; Thijssen, J.; van Loveren, C.; Verrips, E. Parental and family-related influences on dental caries in children of Dutch, Moroccan and Turkish origin. Community Dent. Oral Epidemiol. 2015, 43, 152–162. [Google Scholar] [CrossRef] [PubMed]
- Hooley, M.; Skouteris, H.; Boganin, C.; Satur, J.; Kilpatrick, N. Parental influence and the development of dental caries in children aged 0–6 years: A systematic review of the literature. J. Dent. 2012, 40, 873–885. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.K.; Lee, W.F.; Wang, M.J.; Chang, Y.H.; Tchaou, W.S.; Chang, W.J.; Lee, S.Y.; Sheu, J.R.; Teng, N.C. Chair-side quantitative oral-microflora screening for assessing familial correlation of periodontal status and caries prevalence. PLoS ONE 2014, 9, e87100. [Google Scholar] [CrossRef] [PubMed]
- Weintraub, J.A.; Prakash, P.; Shain, S.G.; Laccabue, M.; Gansky, S.A. Mothers’ caries increases odds of children's caries. J. Dent. Res. 2010, 89, 954–958. [Google Scholar] [CrossRef] [PubMed]
- Grindefjord, M.; Dahllöf, G.; Modéer, T. Caries Development in Children from 2.5 to 3.5 Years of Age: A Longitudinal Study. Caries Res. 1995, 29, 449–454. [Google Scholar] [CrossRef] [PubMed]
- DeWalt, D.A.; Berkman, N.D.; Sheridan, S.; Lohr, K.N.; Pignone, M.P. Literacy and Health Outcomes. J. Gen. Intern. Med. 2004, 19, 1228–1239. [Google Scholar] [CrossRef] [PubMed]
- Horowitz, A.M.; Kleinman, D.V. Oral health literacy: A pathway to reducing oral health disparities in Maryland. J. Public Health Dent. 2012, 72, S26–S30. [Google Scholar] [CrossRef] [PubMed]
- Selden, C.R.; Zorn, M.; Ratzan, S.C.; Parker, R.M. Health Literacy; National Library of Medicine: Bethesda, MD, USA, 2000. [Google Scholar]
- Association, A.D. American Dental Association Statement on Regular Dental Visits. Availabe online: https://www.ada.org/en/press-room/news-releases/2013-archive/june/american-dental-association-statement-on-regular-dental-visits# (accessed on 10 March 2018).
- Broadbent, J.M.; Zeng, J.; Page, L.A.F.; Baker, S.R.; Ramrakha, S.; Thomson, W.M. Oral Health-related Beliefs, Behaviors, and Outcomes through the Life Course. J. Dent. Res. 2016, 95, 808–813. [Google Scholar] [CrossRef] [PubMed]
- Wilson, A.R.; Brega, A.G.; Campagna, E.J.; Braun, P.A.; Henderson, W.G.; Bryant, L.L.; Batliner, T.S.; Quissell, D.O.; Albino, J. Validation and Impact of Caregivers’ Oral Health Knowledge and Behavior on Children’s Oral Health Status. Pediatr. Dent. 2016, 38, 47–54. [Google Scholar] [PubMed]
- Quinlan, J.R. C4. 5: Programs for Machine Learning; Elsevier: New York, NY, USA, 2014. [Google Scholar]
- Ito, A.; Hayashi, M.; Hamasaki, T.; Ebisu, S. Risk assessment of dental caries by using Classification and Regression Trees. J. Dent. 2011, 39, 457–463. [Google Scholar] [CrossRef] [PubMed]
- Ainamo, J.; Barmes, D.; Beagrie, G.; Cutress, T.; Martin, J.; Sardo-Infirri, J. Development of the World Health Organization (WHO) community periodontal index of treatment needs (CPITN). Int. Dent. J. 1982, 32, 281–291. [Google Scholar] [PubMed]
- Cutress, T.W.; Ainamo, J.; Sardo-Infirri, J. The community periodontal index of treatment needs (CPITN) procedure for population groups and individuals. Int. Dent. J. 1987, 37, 222–233. [Google Scholar] [PubMed]
- O’Leary, T.J.; Drake, R.B.; Naylor, J.E. The plaque control record. J. Periodontol. 1972, 43, 38. [Google Scholar] [CrossRef] [PubMed]
- Dentistry, A.A.O.P. Guideline on Caries-risk Assessment and Management for Infants, Children, and Adolescents. Availabe online: http://www.aapd.org/media/Policies_Guidelines/G_CariesRiskAssessment.pdf (accessed on 10 March 2018).
- Podgorelec, V.; Kokol, P.; Stiglic, B.; Rozman, I. Decision trees: An overview and their use in medicine. J. Med. Syst. 2002, 26, 445–463. [Google Scholar] [CrossRef] [PubMed]
- Chapple, I.L.C.; Bouchard, P.; Cagetti, M.G.; Campus, G.; Carra, M.-C.; Cocco, F.; Nibali, L.; Hujoel, P.; Laine, M.L.; Lingström, P.; et al. Interaction of lifestyle, behaviour or systemic diseases with dental caries and periodontal diseases: Consensus report of group 2 of the joint EFP/ORCA workshop on the boundaries between caries and periodontal diseases. J. Clin. Periodontol. 2017, 44, S39–S51. [Google Scholar] [CrossRef] [PubMed]
- Aas, J.A.; Paster, B.J.; Stokes, L.N.; Olsen, I.; Dewhirst, F.E. Defining the normal bacterial flora of the oral cavity. J. Clin. Microbiol. 2005, 43, 5721–5732. [Google Scholar] [CrossRef] [PubMed]
- Liljemark, W.F.; Bloomquist, C. Human oral microbial ecology and dental caries and periodontal diseases. Crit. Rev. Oral Biol. Med. 1996, 7, 180–198. [Google Scholar] [CrossRef] [PubMed]
- Loesche, W. Dental caries and periodontitis: Contrasting two infections that have medical implications. Infect. Dis. Clin. N. Am. 2007, 21, 471–502. [Google Scholar] [CrossRef] [PubMed]
- Harris, R.; Nicoll, A.D.; Adair, P.M.; Pine, C.M. Risk factors for dental caries in young children: A systematic review of the literature. Community Dent. Health 2004, 21, 71–85. [Google Scholar] [PubMed]
- Philip, N.; Suneja, B.; Walsh, L. Beyond Streptococcus mutans: Clinical implications of the evolving dental caries aetiological paradigms and its associated microbiome. Br Dent J. 2018, 224, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Slayton, R.L.; Cooper, M.E.; Marazita, M.L. Tuftelin, mutans streptococci, and dental caries susceptibility. J. Dent. Res. 2005, 84, 711–714. [Google Scholar] [CrossRef] [PubMed]
- Vieira, A.R.; Marazita, M.L.; Goldstein-McHenry, T. Genome-wide scan finds suggestive caries loci. J. Dent. Res. 2008, 87, 435–439. [Google Scholar] [CrossRef] [PubMed]
- Wright, J.T. Defining the contribution of genetics in the etiology of dental caries. J. Dent. Res. 2010, 89, 1173–1174. [Google Scholar] [CrossRef] [PubMed]
- Marshall, R.J. The use of classification and regression trees in clinical epidemiology. J. Clin. Epidemiol. 2001, 54, 603–609. [Google Scholar] [CrossRef]
- Kokol, P.; Zorman, M.; Stiglic, M.M.; Malèiae, I. The limitations of decision trees and automatic learning in real world medical decision making. Stud. Health Technol. Inform. 1998, 52 Pt 1, 529–533. [Google Scholar] [PubMed]
- Zero, D.; Fontana, M.; Lennon, A.M. Clinical applications and outcomes of using indicators of risk in caries management. J. Dent. Educ. 2001, 65, 1126–1132. [Google Scholar] [PubMed]
- Stewart, P.W.; Stamm, J.W. Classification tree prediction models for dental caries from clinical, microbiological, and interview data. J. Dent. Res. 1991, 70, 1239–1251. [Google Scholar] [CrossRef] [PubMed]
- Gansky, S.A. Dental data mining: Potential pitfalls and practical issues. Adv. Dent. Res. 2003, 17, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Declerck, D.; Leroy, R.; Martens, L.; Lesaffre, E.; Garcia-Zattera, M.J.; Vanden Broucke, S.; Debyser, M.; Hoppenbrouwers, K. Factors associated with prevalence and severity of caries experience in preschool children. Community Dent. Oral Epidemiol. 2008, 36, 168–178. [Google Scholar] [CrossRef] [PubMed]
- Elfrink, M.E.; Schuller, A.A.; Veerkamp, J.S.; Poorterman, J.H.; Moll, H.A.; ten Cate, B.J. Factors increasing the caries risk of second primary molars in 5-year-old Dutch children. Int. J. Paediatr. Dent. 2010, 20, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Wigen, T.I.; Wang, N.J. Caries and background factors in Norwegian and immigrant 5-year-old children. Community Dent. Oral Epidemiol. 2010, 38, 19–28. [Google Scholar] [CrossRef] [PubMed]
- MacRitchie, H.M.B.; Longbottom, C.; Robertson, M.; Nugent, Z.; Chan, K.; Radford, J.R.; Pitts, N.B. Development of the Dundee Caries Risk Assessment Model (DCRAM)—Risk model development using a novel application of CHAID analysis. Community Dent. Oral Epidemiol. 2012, 40, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Aleksejuniene, J.; Holst, D.; Brukiene, V. Dental caries risk studies revisited: Causal approaches needed for future inquiries. Int. J. Environ. Res. Public Health 2009, 6, 2992–3009. [Google Scholar] [CrossRef] [PubMed]
- Jiang, E.M.; Lo, E.C.M.; Chu, C.H.; Wong, M.C.M. Prevention of early childhood caries (ECC) through parental toothbrushing training and fluoride varnish application: A 24-month randomized controlled trial. J. Dent. 2014, 42, 1543–1550. [Google Scholar] [CrossRef] [PubMed]
 children with dmft
children with dmft  children with dmft > 3; Four nodes of DT were determined according to: N1: parent’s periodontal classification; N2: parent’s DMFT score; N3: parent’s Perio-Check test results; N4: parent’s pocket depth.
children with dmft children with dmft > 3; Four nodes of DT were determined according to: N1: parent’s periodontal classification; N2: parent’s DMFT score; N3: parent’s Perio-Check test results; N4: parent’s pocket depth.
children with dmft > 3; Four nodes of DT were determined according to: N1: parent’s periodontal classification; N2: parent’s DMFT score; N3: parent’s Perio-Check test results; N4: parent’s pocket depth.
children with dmft children with dmft > 3; Four nodes of DT were determined according to: N1: parent’s periodontal classification; N2: parent’s DMFT score; N3: parent’s Perio-Check test results; N4: parent’s pocket depth.

{kind=link}
{kind=link}
| X: Variables Included in DT | Item | Description |
|---|---|---|
| X¹ | PCR (parent) | Parent’s PCR score |
| X² | PCR (child) | Child’s PCR score |
| X³ | PD | Parent’s pocket depth (mm) |
| X⁴ | Parent SM (tongue) | Parent’s S. mutans level (tongue) |
| X⁵ | Parent SM (plaque) | Parent’s S. mutans level (plaque) |
| X⁶ | Child SM (tongue) | Child’s S. mutans level (tongue) |
| X⁷ | Child SM (plaque) | Child’s S. mutans level (plaque) |
| X⁸ | CPI Index | Parent’s periodontal classification |
| X⁹ | PerioCheck (parent) | Parent’s PerioCheck results |
| X¹⁰ | PerioCheck (child) | Child’s PerioCheck results |
| X¹¹ | GI | Parent’s gingival index |
| X¹² | DMFT | Decayed, missing, filled (because of caries only) permanent teeth |
| Y: outcome variable | ||
| Y¹ | dmft index | Decayed, missing, filled (because of caries only) primary teeth |
| Parent | Child | |||
|---|---|---|---|---|
| Median | IQR | Median | IQR | |
| DMFT/dmft | 13.00 | 6.00 | 9.00 | 8.00 |
| PCR | 87.45 | 20.25 | 94.55 | 20.00 |
| Pocket depth | 1.87 | 0.62 | - | - |
| Gingival index | 1.37 | 0.59 | - | - |
| N | % | N | % | |
| SM (plaque) | ||||
| 0 | 8 | 26.67 | 9 | 30.00 |
| 1 | 7 | 23.33 | 10 | 33.33 |
| 2 | 5 | 16.67 | 4 | 13.33 |
| 3 | 10 | 33.33 | 7 | 23.33 |
| SM (tongue) | ||||
| 0 | 6 | 20.00 | 13 | 43.33 |
| 1 | 9 | 30.00 | 4 | 13.33 |
| 2 | 8 | 26.67 | 6 | 20.00 |
| 3 | 7 | 23.33 | 7 | 23.33 |
| Periodontal classification | ||||
| 0 | 18 | 60.00 | 30 | 100.00 |
| 1 | 7 | 23.33 | ||
| 2 | 2 | 6.67 | ||
| 3 | 3 | 10.00 | ||
| PerioCheck | ||||
| 0 | 8 | 26.67 | 9 | 30.00 |
| 1 | 14 | 46.67 | 21 | 70.00 |
| 2 | 8 | 26.67 | ||
| a. Parents | |||||||
| PCR | SM (Plaque) | SM (Tongue) | Periodontal Classification | Perio Check | Pocket Depth | Gingival Index | |
| DMFT | 0.06 | 0.17 | 0.27 + | −0.24 | 0.18 | −0.10 | 0.11 |
| PCR | 0.23 | 0.19 | 0.11 | 0.00 | 0.13 | 0.22 + | |
| SM (plaque) | 0.57 *** | 0.05 | 0.20 | 0.12 | 0.34 * | ||
| SM (tongue) | −0.16 | 0.07 | −0.09 | 0.13 | |||
| Periodontal classification | 1.00 | 0.30 + | 0.65 *** | 0.15 | |||
| PerioCheck | 0.33 * | 0.18 | |||||
| Pocket depth | 0.19 | ||||||
| b. Children | |||||||
| PCR | SM (Plaque) | SM (Tongue) | PerioCheck | ||||
| dmft | 0.05 | 0.14 | 0.23 + | 0.16 | |||
| PCR | 0.24 | 0.10 | −0.04 | ||||
| SM (plaque) | 0.68 *** | 0.32 + | |||||
| SM (tongue) | 0.38 * | ||||||
| Sensitivity (%) | Specificity (%) | |
|---|---|---|
| N1 (parent’s periodontal classification) | 100.0 | 66.67 |
| N2 (parent’s DMFT score) | 100.0 | 100.0 |
| N3 (parent’s PerioCheck results) | 100.0 | 100.0 |
| N4 (parent’s periodontal pocket depth) | 100.0 | 100.0 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dima, S.; Wang, K.-J.; Chen, K.-H.; Huang, Y.-K.; Chang, W.-J.; Lee, S.-Y.; Teng, N.-C. Decision Tree Approach to the Impact of Parents’ Oral Health on Dental Caries Experience in Children: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2018, 15, 692. https://doi.org/10.3390/ijerph15040692
Dima S, Wang K-J, Chen K-H, Huang Y-K, Chang W-J, Lee S-Y, Teng N-C. Decision Tree Approach to the Impact of Parents’ Oral Health on Dental Caries Experience in Children: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2018; 15(4):692. https://doi.org/10.3390/ijerph15040692
Chicago/Turabian StyleDima, Shinechimeg, Kung-Jeng Wang, Kun-Huang Chen, Yung-Kai Huang, Wei-Jen Chang, Sheng-Yang Lee, and Nai-Chia Teng. 2018. "Decision Tree Approach to the Impact of Parents’ Oral Health on Dental Caries Experience in Children: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 15, no. 4: 692. https://doi.org/10.3390/ijerph15040692
APA StyleDima, S., Wang, K.-J., Chen, K.-H., Huang, Y.-K., Chang, W.-J., Lee, S.-Y., & Teng, N.-C. (2018). Decision Tree Approach to the Impact of Parents’ Oral Health on Dental Caries Experience in Children: A Cross-Sectional Study. International Journal of Environmental Research and Public Health, 15(4), 692. https://doi.org/10.3390/ijerph15040692