Human Health Risk Assessment Applied to Rural Populations Dependent on Unregulated Drinking Water Sources: A Scoping Review

Abstract
1. Introduction
2. Methods
2.1. Research Question
2.2. Data Sources and Search Strategy
2.3. Citation Management
2.4. Eligibility Criteria
2.5. Title and Abstract Relevance Screening
2.6. Data Characterization
2.7. Data Summary and Synthesis
3. Results
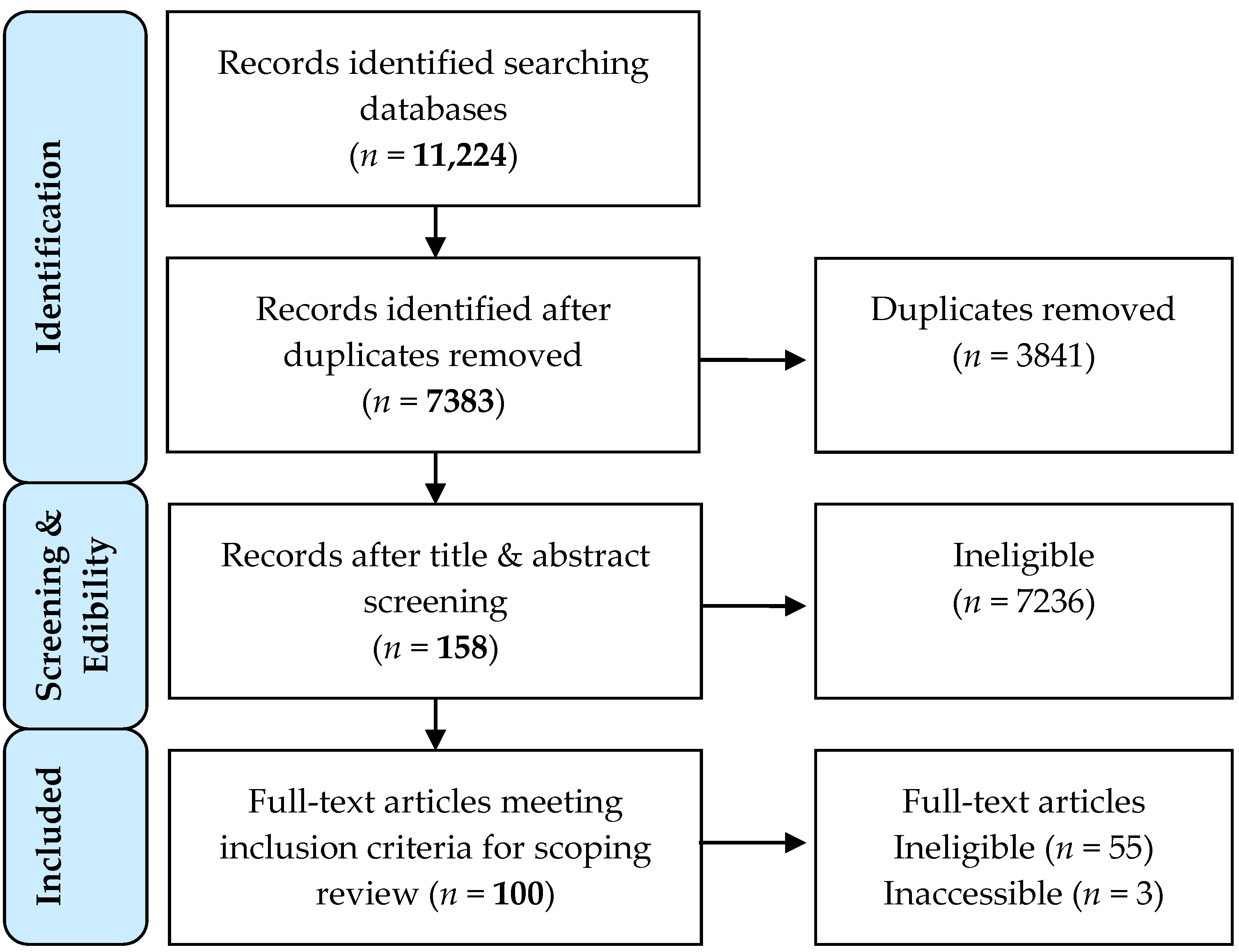
3.1. Search and Selection
3.2. Human Health Risk Assessment Characteristics
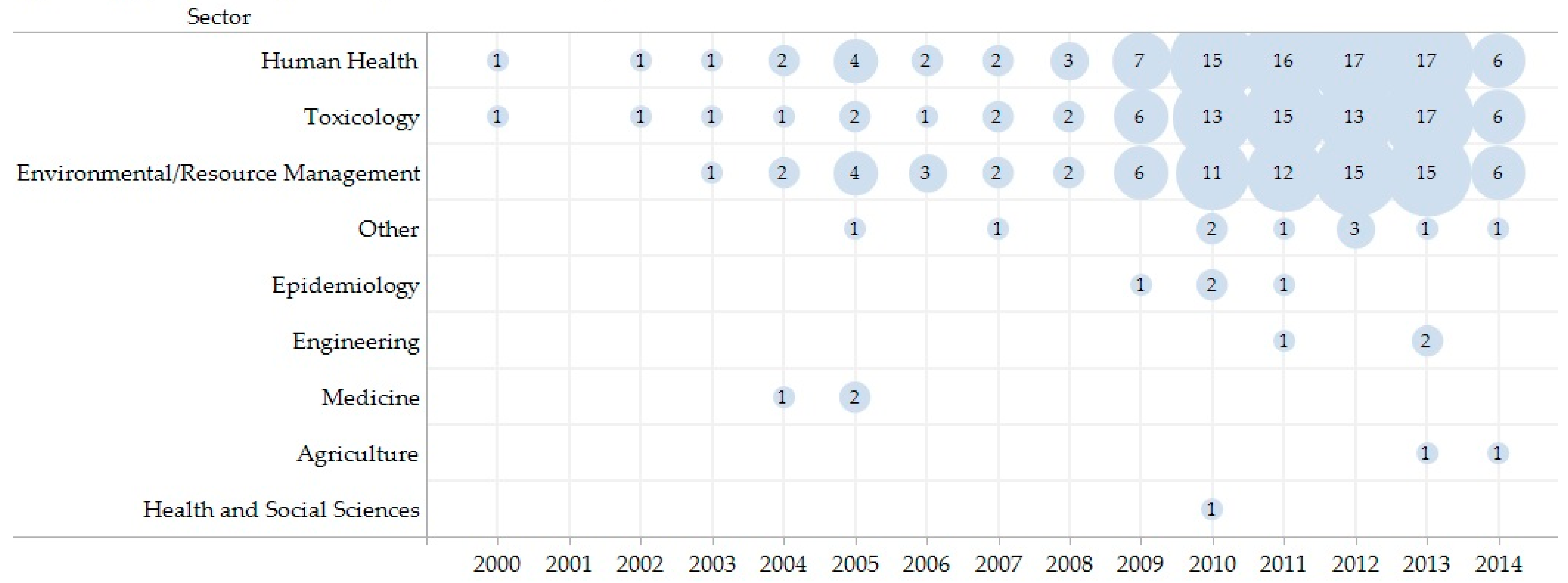
3.3. Literature Characteristics
3.4. Literature Gaps
4. Discussion
5. Strengths and Limitations
6. Conclusions
Recommendations
- Components of the HHRA (e.g., exposure population, source water, hazards, etc.) should be adequately described to improve the detection of potential relevant literature upon title and abstract searches, and the quality of research reporting. Consistent use of terminology and reporting associated with standardized HHRA frameworks is essential. Uncertainty and limitations should be clearly presented to allow for appropriate interpretation of the research.
- A holistic approach to HHRA should be considered when non-traditional factors are suspected of influencing the human health risk. This can be accomplished with alternative methods of risk assessment (e.g., Bayesian risk assessment) to characterize non-traditional factors and their influence on the human health risks. Gaps in the literature identify the need to consider the effects and uncertainty associated with non-traditional factors with respect to multiple hazards, exposures and pathways.
- Identification of gaps in research, management, community, and risk assessments is a necessary component of HHRA. Recognition of gaps in these areas drives research forward, paving the way for new research to better inform future approaches, frameworks, and decision-making.
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- World Bank. The World Bank: Data. Available online: http://data.worldbank.org/indicator (accessed on 17 July 2016).
- World Health Organization; The United Nations Children’s Fund. 25 Years Progress on Sanitation and Drinking Water: 2015 Update and MDG Assessment; World Health Organization: Geneva, Switzerland, 2015; p. 90. ISBN 978-92-4-150914-5. [Google Scholar]
- World Health Organization. Water Quality and Health Strategy 2013–2020; World Health Organization: New York, NY, USA, 2013; p. 15. [Google Scholar]
- World Health Organization; The United Nations Children’s Fund. Progress on Drinking Water and Sanitation: 2012 Update; World Health Organization: Geneva, Switzerland, 2012; p. 18. ISBN 978-924-1503297. [Google Scholar]
- Shaheed, A.; Orgill, J.; Montgomery, M.A.; Jeuland, M.A.; Brown, J. Why “improved” water sources are not always safe. Bull. World Health Organ. 2014, 92, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Nsiah-Kumi, P.A. Communicating effectively with vulnerable populations during water contamination events. J. Water Health 2008, 6, 63–75. [Google Scholar] [CrossRef] [PubMed]
- Fawell, J.; Nieuwenhuijsen, M. Contaminants in drinking water. Br. Med. Bull. 2003, 68, 199–208. [Google Scholar] [CrossRef] [PubMed]
- Suter, G.; Vermeire, T.; Munns, W.; Sekizawa, J. An integrated framework for health and ecological risk assessment. Toxicol. Appl. Pharmacol. 2005, 207, 611–616. [Google Scholar] [CrossRef] [PubMed]
- Bridges, J. Human health and environmental risk assessment: The need for a more harmonised and integrated approach. Chemosphere 2003, 52, 1347–1351. [Google Scholar] [CrossRef]
- Vermeire, T.; Munns, W.R.; Sekizawa, J.; Suter, G.; Van der Kraak, G. An assessment of integrated risk assessment. Hum. Ecol. Risk Assess. Int. J. 2007, 13, 339–354. [Google Scholar] [CrossRef]
- Munns, W.R.; Kroes, R.; Veith, G.; Suter, G.W., II; Damstra, T.; Waters, M.D. Approaches for integrated risk assessment. Hum. Ecol. Risk Assess. Int. J. 2003, 9, 267–272. [Google Scholar] [CrossRef]
- World Health Organization; Institute of Peace and Conflict Studies. Framework for the Integration of Health and Ecological Risk Assessment; World Health Organization: Geneva, Switzerland, 2001; Volume II, p. 22. [Google Scholar]
- Sexton, K.; Linder, S.H. Integrated assessment of risk and sustainability in the context of regulatory decision making. Environ. Sci. Technol. 2014, 48, 1409–1418. [Google Scholar] [CrossRef] [PubMed]
- Briggs, D.J. A framework for integrated environmental health impact assessment of systemic risks. Environ. Health 2008, 7, 61–77. [Google Scholar] [CrossRef] [PubMed]
- Wilks, M.F.; Roth, N.; Aicher, L.; Faust, M.; Papadaki, P.; Marchis, A.; Calliera, M.; Ginebreda, A.; Andres, S.; Kühne, R.; et al. White paper on the promotion of an integrated risk assessment concept in European regulatory frameworks for chemicals. Sci. Total Environ. 2015, 521–522, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Hart, B.; Pollino, C. Bayesian Modelling for Risk-Based Environmental Water Allocation; Common Wealth of Austrailia: Canberra, Austrailia, 2009; p. 87. ISBN 978-1-921107-74-0.
- Sekizawa, J.; Tanabe, S. A comparison between integrated risk assessment and classical health/environmental assessment: Emerging beneficial properties. Toxicol. Appl. Pharmacol. 2005, 207, 617–622. [Google Scholar] [CrossRef] [PubMed]
- Arquette, M.; Cole, M.; Cook, K.; LaFrance, B.; Peters, M.; Ransom, J.; Sargent, E.; Smoke, V.; Stairs, A. Holistic risk-based environmental decision making: A Native perspective. Environ. Health Perspect. 2002, 110, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Serre, M.L.; Kolovos, A.; Christakos, G.; Modis, K. An application of the holistochastic human exposure methodology to naturally occurring arsenic in Bangladesh drinking water. Risk Anal. 2003, 23, 515–528. [Google Scholar] [CrossRef] [PubMed]
- Zargar, A.; Dyck, R.; Islam, M.S.; Mohapatra, A.; Sadiq, R. Data fusion methods for human health risk assessment: Review and application. Hum. Ecol. Risk Assess. Int. J. 2014, 20, 807–838. [Google Scholar] [CrossRef]
- Liu, K.F.-R.; Lu, C.-F.; Chen, C.-W.; Shen, Y.-S. Applying Bayesian belief networks to health risk assessment. Stoch. Environ. Res. Risk Assess. 2012, 26, 451–465. [Google Scholar] [CrossRef]
- Ryan, L. Epidemiologically based environmental risk assessment. Stat. Sci. 2003, 18, 466–480. [Google Scholar] [CrossRef]
- Markon, M.-P.L.; Lemyre, L. Public reactions to risk messages communicating different sources of uncertainty: An experimental test. Hum. Ecol. Risk Assess. Int. J. 2013, 19, 1102–1126. [Google Scholar] [CrossRef]
- Pham, M.; Rajić, A.; Greig, J.; Sargeant, J.; Papadopoulos, A.; McEwen, S. A scoping review of scoping reviews: Advancing the approach and enhancing the consistency. Res. Synth. Methods 2014, 5, 371–385. [Google Scholar] [CrossRef] [PubMed]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Levac, D.; Colquhoun, H.; O’Brien, K. Scoping studies: Advancing the methodology. Implement. Sci. 2010, 5, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Kavcar, P.; Sofuoglu, A.; Sofuoglu, S. A health risk assessment for exposure to trace metals via drinking water ingestion pathway. Int. J. Hyg. Environ. Health 2009, 212, 216–227. [Google Scholar] [CrossRef] [PubMed]
- Titilayo, E.A.; Olufemi, A.G.; Ogbemi, E.T. Chronic exposure to heavy metals in public water supply and human health risk assessment. Terr. Aquat. Environ. Toxicol. 2012, 6, 106–111. [Google Scholar]
- Maqsood, I. Integrated fuzzy-stochastic risk assessment for contaminated groundwater systems. Int. J. Risk Assess. Manag. 2011, 15, 43–65. [Google Scholar] [CrossRef]
- Zhao, J.; Wang, R.; Bian, J.; Zhao, Y. Potential health risk of arsenic in groundwater near Tongyu County, Western of Jilin Province: A case study for health risk assessment based on triangular fuzzy number 26. Adv. Mater. Res. 2012, 982–986. [Google Scholar] [CrossRef]
- Çelebi, A.; Sengörür, B.; Kløve, B. Human health risk assessment of dissolved metals in groundwater and surface waters in the Melen watershed, Turkey. J. Environ. Sci. Health Part A 2014, 49, 153–161. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.; Luo, Y.; Gui, T.; Huang, Y. Concentrations and potential health hazards of organochlorine pesticides in shallow groundwater of Taihu Lake region, China. Sci. Total Environ. 2014, 470–471, 1047–1055. [Google Scholar] [CrossRef] [PubMed]
- Sultana, J.; Farooqi, A.; Ali, U. Arsenic concentration variability, health risk assessment, and source identification using multivariate analysis in selected villages of public water system, Lahore, Pakistan. Environ. Monit. Assess. 2014, 186, 1241–1251. [Google Scholar] [CrossRef] [PubMed]
- Phan, K.; Phan, S.; Huoy, L.; Suy, B.; Wong, M.; Hashim, J.; Mohamed, Y.M.S.; Aljunid, S.; Sthiannopkao, S.; Kim, K. Assessing mixed trace elements in groundwater and their health risk of residents living in the Mekong River basin of Cambodia. Environ. Pollut. 2013, 182, 111–119. [Google Scholar] [CrossRef] [PubMed]
- Su, X.; Wang, H.; Zhang, Y. Health risk assessment of nitrate contamination in groundwater: A case study of an agricultural area in northeast China. Water Resour. Manag. 2013, 27, 3025–3034. [Google Scholar] [CrossRef]
- Papić, P.; Ćuk, M.; Todorović, M.; Stojković, J.; Hajdin, B.; Atanacković, N.; Polomčić, D. Arsenic in tap water of Serbia’s South Pannonian Basin and arsenic risk assessment. Pol. J. Environ. Stud. 2012, 21, 1783–1790. [Google Scholar]
- Peplow, D.; Edmonds, R. Health risks associated with contamination of groundwater by abandoned mines near Twisp in Okanogan County, Washington, USA. Environ. Geochem. Health 2004, 26, 69–79. [Google Scholar] [CrossRef] [PubMed]
- Jamaludin, N.; Sham, S.M.; Ismail, S.N.S. Health risk assessment of nitrate exposure in well water of residents in intensive agriculture area. Am. J. Appl. Sci. 2013, 10, 442–448. [Google Scholar] [CrossRef]
- Kumar, A.; Adak, P.; Gurian, P.; Lockwood, J. Arsenic exposure in US public and domestic drinking water supplies: A comparative risk assessment. J. Expo. Sci. Environ. Epidemiol. 2010, 20, 245–254. [Google Scholar] [CrossRef] [PubMed]
- Nzihou, J.; Bouda, M.; Hamidou, S.; Diarra, J. Arsenic in drinking water toxicological risk assessment in the North Region of Burkina Faso. J. Water Resour. Prot. 2013, 5, 46–52. [Google Scholar] [CrossRef]
- Busset, G.; Vialle, C.; Sablayrolles, C.; Huau, M.; Jacob, S.; Montrejaud-Vignoles, M. Health risk assessment case study for trace metals in rainwater for domestic uses. Fresenius Environ. Bull. 2010, 20, 2277–2283. [Google Scholar]
- Williams, P.R.; Scott, P.; Sheehan, P.; Paustenbach, D. A probabilistic assessment of household exposures to MTBE from drinking water. Hum. Ecol. Risk Assess. Int. J. 2000, 6, 827–849. [Google Scholar] [CrossRef]
- Li, J.; Huang, G.; Zeng, G.; Maqsood, I.; Huang, Y. An integrated fuzzy-stochastic modeling approach for risk assessment of groundwater contamination. J. Environ. Manag. 2007, 82, 173–188. [Google Scholar] [CrossRef] [PubMed]
- Marara, T.; Palamuleni, L.; Ebenso, E. Chemical and radiological risks of drinking water from communities in Wonderfonteinspruit catchment, South Africa. Asian J. Chem. 2013, 25, 9302–9308. [Google Scholar] [CrossRef]
- Deng, Y.; Ni, F.; Yao, Z. The Monte Carlo-Based uncertainty health risk assessment associated with rural drinking water quality. J. Water Resour. Prot. 2012, 4, 772–778. [Google Scholar] [CrossRef]
- Donovan, E.; Unice, K.; Roberts, J.; Harris, M.; Finley, B. Risk of gastrointestinal disease associated with exposure to pathogens in the water of the Lower Passaic River. Appl. Environ. Microbiol. 2008, 74, 994–1003. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Yu, G.; Yu, Y.J.; Huang, J.; Hu, H.Y.; Wang, L.S. Health risk assessment of organic pollutants in Jiangsu Reach of the Huaihe River, China. Water Sci. Technol. 2009, 59, 907–916. [Google Scholar] [CrossRef] [PubMed]
- Hunter, P.; de Sylor, M.; Risebro, H.; Nichols, G.; Kay, D.; Hartemann, P. Quantitative microbial risk assessment of cryptosporidiosis and giardiasis from very small private water supplies. Risk Anal. 2011, 31, 228–236. [Google Scholar] [CrossRef] [PubMed]
- Razzolini, M.; Weir, M.; Matte, M.; Matte, G.; Fernandes, L.; Rose, J. Risk of Giardia infection for drinking water and bathing in a peri-urban area in São Paulo, Brazil. Int. J. Environ. Health Res. 2011, 21, 222–234. [Google Scholar] [CrossRef] [PubMed]
- Mondal, D.; Banerjee, M.; Kundu, M.; Banerjee, N.; Bhattacharya, U.; Giri, A.K.; Ganguli, B.; Sen Roy, S.; Polya, D.A. Comparison of drinking water, raw rice and cooking of rice as arsenic exposure routes in three contrasting areas of West Bengal, India. Environ. Geochem. Health 2010, 32, 463–477. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Lin, C.; Jang, C.; Ling, M.; Tsai, J. Assessing nitrate contamination and its potential health risk to Kinmen residents. Environ. Geochem. Health 2011, 33, 503–514. [Google Scholar] [CrossRef] [PubMed]
- Yu, F.C.; Fang, G.H.; Ru, X.W. Eutrophication, health risk assessment and spatial analysis of water quality in Gucheng Lake, China. Environ. Earth Sci. 2010, 59, 1741–1748. [Google Scholar] [CrossRef]
- Genthe, B.; Le Roux, W.; Schachtschneider, K.; Oberholster, P.; Aneck-Hahn, N.; Chamier, J. Health risk implications from simultaneous exposure to multiple environmental contaminants. Ecotoxicol. Environ. Saf. 2013, 93, 171–179. [Google Scholar] [CrossRef] [PubMed]
- Buczyńska, A.; Szadkowska-Stańczyk, I. Identification of health hazards to rural population living near pesticide dump sites in Poland. Int. J. Occup. Med. Environ. Health 2005, 18, 331–339. [Google Scholar] [PubMed]
- Giri, S.; Singh, A.K. Risk assessment, statistical source identification and seasonal fluctuation of dissolved metals in the Subarnarekha River, India. J. Hazard. Mater. 2014, 265, 305–314. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.K.; Ghosh, A.K. Health risk assessment due to groundwater arsenic contamination: Children are at high risk. Hum. Ecol. Risk Assess. Int. J. 2012, 18, 751–766. [Google Scholar] [CrossRef]
- Yacoub, C.; Blazquez, N.; Pérez-Foguet, A.; Miralles, N. Spatial and temporal trace metal distribution of a Peruvian basin: Recognizing trace metal sources and assessing the potential risk. Environ. Monit. Assess. 2013, 185, 7961–7978. [Google Scholar] [CrossRef] [PubMed]
- De Jongh, C.; Kooij, P.; de Voogt, P.; ter Laak, T. Screening and human health risk assessment of pharmaceuticals and their transformation products in Dutch surface waters and drinking water. Sci. Total Environ. 2012, 427–428, 70–77. [Google Scholar] [CrossRef] [PubMed]
- Hynds, P.; Gill, L.; Misstear, B. A quantitative risk assessment of verotoxigenic E. coli (VTEC) in private groundwater sources in the Republic of Ireland. Hum. Ecol. Risk Assess. 2014, 20, 1446–1468. [Google Scholar] [CrossRef]
- Machdar, E.; van der Steen, N.; Raschid-Sally, L.; Lens, P. Application of quantitative microbial risk assessment to analyze the public health risk from poor drinking water quality in a low income area in Accra, Ghana. Sci. Total Environ. 2013, 449, 134–142. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, W.; Vieritz, A.; Goonetilleke, A.; Gardner, T. Health risk from the use of roof-harvested rainwater in Southeast Queensland, Australia, as potable or nonpotable water, determined using quantitative microbial risk assessment. Appl. Environ. Microbiol. 2010, 76, 7382–7391. [Google Scholar] [CrossRef] [PubMed]
- Santos, M.D.A.; Tavora, B.E.; Koide, S.; Caldas, E.D. Human risk assessment of benzene after a gasoline station fuel leak. Rev. Saude Publica 2013, 47, 335–344. [Google Scholar] [CrossRef] [PubMed]
- Zheng, J.; Chen, K.; Yan, X.; Chen, S.-J.; Hu, G.-C.; Peng, X.-W.; Yuan, J.; Mai, B.-X.; Yang, Z.-Y. Heavy metals in food, house dust, and water from an e-waste recycling area in South China and the potential risk to human health. Ecotoxicol. Environ. Saf. 2013, 96, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Ramirez-Andreotta, M.D.; Brusseau, M.L.; Beamer, P.; Maier, R.M. Home gardening near a mining site in an arsenic-endemic region of Arizona: Assessing arsenic exposure dose and risk via ingestion of home garden vegetables, soils, and water. Sci. Total Environ. 2013, 454–455, 373–382. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Lee, B.; Kim, J.; Kim, K.; Lee, J. Human risk assessment for heavy metals and As contamination in the abandoned metal mine areas, Korea. Environ. Monit. Assess. 2006, 119, 233–244. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.S.; Chon, H.T.; Kim, K.W. Human risk assessment of As, Cd, Cu and Zn in the abandoned metal mine site. Environ. Geochem. Health 2005, 27, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Armah, F.A.; Kuitunen, M.; Luginaah, I.; Mkandawire, P. Non occupational health risk assessment from exposure to chemical contaminants in the gold mining environment of Tarkwa, Ghana. Trends Appl. Sci. Res. 2012, 7, 181–195. [Google Scholar] [CrossRef]
- Törnqvist, R.; Jarsjö, J.; Karimov, B. Health risks from large-scale water pollution: Trends in central Asia. Environ. Int. 2011, 37, 435–442. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Park, H.; Kim, J.; Park, S.; Cho, B.; Sung, I.; Shin, D. Health risk assessment for uranium in Korean groundwater. J. Environ. Radioact. 2004, 77, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Jang, C.; Wang, S.; Liu, C. Evaluation of potential health risk of arsenic-affected groundwater using indicator kriging and dose response model. Sci. Total Environ. 2007, 384, 151–162. [Google Scholar] [CrossRef] [PubMed]
- Ni, F.; Liu, G.; Ye, J.; Ren, H.; Yang, S. ArcGIS-based rural drinking water quality health risk assessment. J. Water Resour. Prot. 2009, 1, 351–361. [Google Scholar] [CrossRef]
- Steyn, M.; Jagals, P.; Genthe, B. Assessment of microbial infection risks posed by ingestion of water during domestic water use and full-contact recreation in a mid southern African region. Water Sci. Technol. 2004, 50, 301–308. [Google Scholar] [PubMed]
- Kelepertzis, E. Investigating the sources and potential health risks of environmental contaminants in the soils and drinking waters from the rural clusters in Thiva area (Greece). Ecotoxicol. Environ. Saf. 2014, 100, 258–265. [Google Scholar] [CrossRef] [PubMed]
- Rapant, S.; Krcmová, K. Health risk assessment maps for arsenic groundwater content: Application of national geochemical databases. Environ. Geochem. Health 2007, 29, 131–141. [Google Scholar] [CrossRef] [PubMed]
- Lee, L.; Chen, C.; Chang, Y.; Liou, S.; Wang, J. An estimation of the health impact of groundwater pollution caused by dumping of chlorinated solvents. Sci. Total Environ. 2010, 408, 1271–1275. [Google Scholar] [CrossRef] [PubMed]
- Kazama, S.; Aizawa, T.; Watanabe, T.; Ranjan, P.; Gunawardhana, L.; Amano, A. A quantitative risk assessment of waterborne infectious disease in the inundation area of a tropical monsoon region. Sustain. Sci. 2012, 7, 45–54. [Google Scholar] [CrossRef]
- Addo, M.; Darko, E.; Gordon, C.; Nyarko, B. Water quality analysis and human health risk assessment of groundwater from open-wells in the vicinity of a cement factory at Akporkloe, Southeastern Ghana. Electr. J. Sci. Technol. 2013, 4, 16–30. [Google Scholar] [CrossRef]
- Obiri, S.; Dodoo, D.; Armah, F.; Essumang, D.; Cobbina, S. Evaluation of lead and mercury neurotoxic health risk by resident children in the Obuasi municipality, Ghana. Environ. Toxicol. Pharmacol. 2010, 29, 209–212. [Google Scholar] [CrossRef] [PubMed]
- Wu, B.; Zhang, Y.; Zhang, X.; Cheng, S. Health risk from exposure of organic pollutants through drinking water consumption in Nanjing, China. Bull. Environ. Contam. Toxicol. 2010, 84, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Howard, G.; Pedley, S.; Tibatemwa, S. Quantitative microbial risk assessment to estimate health risks attributable to water supply: Can the technique be applied in developing countries with limited data? J. Water Health 2006, 4, 49–65. [Google Scholar] [CrossRef] [PubMed]
- Momot, O.; Synzynys, B. Toxic aluminium and heavy metals in groundwater of Middle Russia: Health risk assessment. Int. J. Environ. Res. Public Health 2005, 2, 214–218. [Google Scholar] [CrossRef] [PubMed]
- Buchhamer, E.; Blanes, P.; Osicka, R.; Giménez, M. Environmental risk assessment of arsenic and fluoride in the Chaco Province, Argentina: Research advances. J. Toxicol. Environ. Health Part A 2012, 75, 1437–1450. [Google Scholar] [CrossRef] [PubMed]
- Qiao, M.; An, T.; Zeng, X.; Zhang, D.; Li, G.; Sheng, G.; Fu, J.; Zhang, G.; Guo, J. Safety assessment of the source water within the Pearl River Delta on the aspect of organochlorine pesticides contamination. J. Environ. Monit. 2010, 12, 1666–1677. [Google Scholar] [CrossRef] [PubMed]
- Chai, L.; Wang, Z.; Wang, Y.; Yang, Z.; Wang, H.; Wu, X. Ingestion risks of metals in groundwater based on TIN model and dose-response assessment—A case study in the Xiangjiang watershed, central-south China. Sci. Total Environ. 2010, 408, 3118–3124. [Google Scholar] [CrossRef] [PubMed]
- Ujević Bošnjak, M.; Capak, K.; Jazbec, A.; Casiot, C.; Sipos, L.; Poljak, V.; Dadić, Ž. Hydrochemical characterization of arsenic contaminated alluvial aquifers in Eastern Croatia using multivariate statistical techniques and arsenic risk assessment. Sci. Total Environ. 2012, 420, 100–110. [Google Scholar] [CrossRef] [PubMed]
- Williams, P.; Benton, L.; Warmerdam, J.; Sheehans, P. Comparative risk analysis of six volatile organic compounds in California drinking water. Environ. Sci. Technol. 2002, 36, 4721–4728. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.; Qin, X.; Sun, N.; Yang, G. Human health risk of metals in drinking-water source areas from a forest zone after long-term excessive deforestation. Hum. Ecol. Risk Assess. Int. J. 2014, 20, 1200–1212. [Google Scholar] [CrossRef]
- Caylak, E. Health risk assessment for trace metals, polycyclic aromatic hydrocarbons and trihalomethanes in drinking water of Cankiri, Turkey. J. Chem. 2012, 9, 1976–1991. [Google Scholar] [CrossRef]
- Emmanuel, E.; Pierre, M.; Perrodin, Y. Groundwater contamination by microbiological and chemical substances released from hospital wastewater: Health risk assessment for drinking water consumers. Environ. Int. 2009, 35, 718–726. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Ghosh, A.; Kumar, A.; Kislay, K.; Tiwari, R.; Parwez, R.; Kumar, N.; Imam, M. Groundwater arsenic contamination and associatied health risks in Bihar, India. Int. J. Environ. Res. 2014, 8, 49–60. [Google Scholar]
- Etchie, A.; Etchie, T.; Adewuyi, G. Systemic chronic health risk assessment of residential exposure to Cd2+ and Cr6+ in groundwater. Toxicol. Environ. Chem. 2012, 94, 181–194. [Google Scholar] [CrossRef]
- Leung, H.; Jin, L.; Wei, S.; Tsui, M.; Zhou, B.; Jiao, L.; Cheung, P.; Chun, Y.; Murphy, M.; Lam, P. Pharmaceuticals in tap water: Human health risk assessment and proposed monitoring framework in China. Environ. Health Perspect. 2013, 121, 839–846. [Google Scholar] [CrossRef] [PubMed]
- Caylak, E. Health risk assessment for arsenic in water sources of Cankiri Province of Turkey. CLEAN Soil Air Water 2012, 40, 728–734. [Google Scholar] [CrossRef]
- Wang, Z.; Chai, L.; Wang, Y.; Yang, Z.; Wang, H.; Wu, X. Potential health risk of arsenic and cadmium in groundwater near Xiangjiang River, China: A case study for risk assessment and management of toxic substances. Environ. Monit. Assess. 2011, 175, 167–173. [Google Scholar] [CrossRef] [PubMed]
- Karim, M. Microbial contamination and associated health burden of rainwater harvesting in Bangladesh. Water Sci. Technol. 2010, 61, 2129–2135. [Google Scholar] [CrossRef] [PubMed]
- Pons, W.; Young, I.; Truong, J.; Jones-Bitton, A.; McEwen, S.; Pintar, K.; Papadopoulos, A. A systematic review of waterborne disease outbreaks associated with small non-community drinking water systems in Canada and the United States. PLoS ONE 2015, 10, e0141646. [Google Scholar] [CrossRef] [PubMed]
- Kundzewicz, Z.; Doll, P. Will groundwater ease freshwater stress under climate change? Hydrol. Sci. J. 2009, 54, 665–675. [Google Scholar] [CrossRef]
- Famiglietti, J.S. The global groundwater crisis. Nat. Clim. Chang. 2014, 4, 945–948. [Google Scholar] [CrossRef]
- Burns, C.; Wright, M.; Pierson, J.; Bateson, T.; Burstyn, I.; Goldstein, D.; Klaunig, J.; Luben, T.; Mihlan, G.; Ritter, L.; et al. Evaluating uncertainty to strengthen epidemiologic data for use in human health risk assessments. Environ. Health Perspect. 2014, 122, 1160–1165. [Google Scholar] [CrossRef] [PubMed]
- Chowdhury, S.; Champagne, P.; McLellan, P. Uncertainty characterization approaches for risk assessment of DBPs in drinking water: A review. J. Environ. Manag. 2009, 90, 1680–1691. [Google Scholar] [CrossRef] [PubMed]
- Hertwich, E.; McKone, T.; Pease, W. Parameter uncertainty and variability in evaluative fate and exposure models. Risk Anal. 1999, 19, 1193–1204. [Google Scholar] [CrossRef] [PubMed]
- United States Environmental Protection Agency. Probablistic Risk Assessment White Paper and Supporting Documents. Available online: https://www.epa.gov (accessed on 31 July 2016).
- Hooten, M.; Hobbs, N. A guide to Bayesian model selection for ecologists. Ecol. Monogr. 2015, 85, 3–28. [Google Scholar] [CrossRef]
- Slovic, P. Trust, Emotion, Sex, Politics, and Science: Surveying the risk-assessment battlefield. Risk Anal. 1999, 19, 689–701. [Google Scholar] [CrossRef] [PubMed]
- Boholm, Å. On the organizational practice of expert-based risk management: A case of railway planning. Risk Manag. 2010, 12, 235–255. [Google Scholar] [CrossRef]
- Renn, O. Three decades of risk research: Accomplishments and new challenges. J. Risk Res. 1998, 1, 49–71. [Google Scholar] [CrossRef]
- United States Environmental Protection Agency. Risk Assessment Guidance for Superfund. Volume I Human Health Evaluation Manual (Part A); U.S. Environmental Protection Agency: Washington, DC, USA, 1989; p. 291. EPA/540/1-89/002.
- International Programme on Chemical Safety. Guidance Document on Evaluating and Expressing Uncertainty in Hazard Characterization; World Health Organization: Geneva, Switzerland, 2014; p. 181. ISBN 978-92-4-150761-5. [Google Scholar]
- Kavlock, R.J.; Daston, G.P.; DeRosa, C.; Fenner-Crisp, P.; Gray, L.E.; Kaattari, S.; Lucier, G.; Luster, M.; Mac, M.J.; Maczka, C.; et al. Research needs for the risk assessment of health and environmental effects of endocrine disruptors: A report of the U.S. EPA-sponsored workshop. Environ. Health Perspect. 1996, 104, 715–740. [Google Scholar] [CrossRef] [PubMed]
- Rajagopal, R.; Talcott, R.L. Patterns in groundwater quality: Selected observations in Iowa. Environ. Manag. 1983, 7, 465–473. [Google Scholar] [CrossRef]
- Ritter, L.; Solomon, K.; Sibley, P.; Hall, K.; Keen, P.; Mattu, G.; Linton, B. Sources, pathways, and relative risks of contaminants in surface water and groundwater: A perspective prepared for the Walkerton inquiry. J. Toxicol. Environ. Health Part A 2002, 65, 1–142. [Google Scholar] [CrossRef] [PubMed]
- Villanueva, C.; Kogevinas, M.; Cordier, S.; Templeton, M.; Vermeulen, R.; Nuckols, J.; Nieuwenhuijsen, M.; Levallois, P. Assessing exposure and health consequences of chemicals in drinking water: Current state of knowledge and research needs. Environ. Health Perspect. 2014, 122, 213–221. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Mauzerall, D.L.; Zhu, T.; Liang, S.; Ezzati, M.; Remais, J.V. Environmental health in China: Progress towards clean air and safe water. Lancet 2010, 375, 1110–1119. [Google Scholar] [CrossRef]
- United States Environmental Protection Agency. Process for Conducting Probabilistic Risk Assessment. In Risk Assessment Guidance for Superfund: Volume 111—Part A; U.S. Environmental Protection Agency: Washington, DC, USA, 2001; pp. 1–34. EPA/540/R/02/002. [Google Scholar]
- Bornmann, L.; Mutz, R. Growth rates of modern science: A bibliometric analysis based on the number of publications and cited references. J. Assoc. Inf. Sci. Technol. 2015, 66, 2215–2222. [Google Scholar] [CrossRef]
- Bartram, J.; Brocklehurst, C.; Fisher, M.; Luyendijk, R.; Hossain, R.; Wardlaw, T.; Gordon, B. Global monitoring of water supply and sanitation: History, methods and future challenges. Int. J. Environ. Res. Public Health 2014, 11, 8137–8165. [Google Scholar] [CrossRef] [PubMed]
- United States Environmental Protection Agency. Human Health Risk Assessment. Available online: https://www.epa.gov/risk/human-health-risk-assessment (accessed on 31 July 2016).
- O’Toole, T.P.; Aaron, K.F.; Chin, M.H.; Horowitz, C.; Tyson, F. Community-based participatory research. J. Gen. Intern. Med. 2003, 18, 592–594. [Google Scholar] [CrossRef] [PubMed]
- Daudt, H.; van Mossel, C.; Scott, S. Enhancing the scoping study methodology: A large, inter-professional team’s experience with Arksey and O’Malley’s framework. BMC Med. Res. Methodol. 2013, 13, 1–9. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria |
|---|
| Peer-reviewed |
| Identified applied HHRA |
| Identified water use for human consumption |
| Identified the water source as unregulated or unspecified a |
| Characteristic | Number (n = 100) | Percentage (%) |
|---|---|---|
| Exposure Population | ||
| Geographic Area of Population | ||
| Rural (rural and unregulated) | 28 (7) | 28 (7) |
| Urban (urban and rural) | 16 (4) | 16 (4) |
| Remote (remote and rural) | 2 (0) | 2 (0) |
| Unspecified | 54 | 54 |
| Community a | ||
| Geography | 86 | 86 |
| Topography | 27 | 27 |
| Cultural/Spiritual | 2 | 2 |
| Unspecified | 20 | 20 |
| Receptors a | ||
| Adults | 66 | 66 |
| Local Residents | 41 | 41 |
| Child | 31 | 31 |
| Toddler | 15 | 15 |
| Teen | 15 | 15 |
| Responsible for source water | 13 | 13 |
| Seniors | 11 | 11 |
| General Public | 10 | 10 |
| Infants | 10 | 10 |
| Local Farmers and Families | 5 | 5 |
| Employees | 2 | 2 |
| First Nation/Indigenous | 0 | 0 |
| Age categories not defined | 39 | 39 |
| Other (e.g., gender, visitors, etc.) | 6 | 6 |
| Unspecified | 8 | 8 |
| Exposure Pathway a | ||
| Oral | 100 | 100 |
| Dermal | 23 | 23 |
| Inhalation | 4 | 4 |
| Hazard Identification | ||
| Status of drinking water | ||
| Unregulated (unregulated and untreated) | 21 (14) | 21 (14) |
| Unspecified (unspecified and untreated) | 79 (51) | 79 (51) |
| Source of drinking water a | ||
| Groundwater (unregulated groundwater) | 67 (14) | 67 (14) |
| Surface water (unregulated surface water) | 39 (7) | 39 (7) |
| Other (e.g., bottled, rain, cistern, etc.) | 21 | 21 |
| Unspecified | 5 | 5 |
| Type of drinking water | ||
| Untreated | 56 | 56 |
| Untreated and Treated | 9 | 9 |
| Unspecified | 35 | 35 |
| Hazard in drinking water | ||
| Anthropogenic chemical | 35 | 35 |
| Natural chemical | 22 | 22 |
| Anthropogenic and natural chemical | 25 | 25 |
| Microbiological/Pathogen (microbiological/pathogen and chemical) | 10 (2) | 10 (2) |
| Radiological (radiological and chemical) | 1 (3) | 1 (3) |
| Unspecified | 7 | 7 |
| At least two hazards identified | 5 | 5 |
| Data source a | ||
| Source water sampled | 96 | 96 |
| Historical data | 13 | 13 |
| Predicted/Extrapolated | 11 | 11 |
| Biomarkers (i.e., hair samples) | 3 | 3 |
| Unspecified | 2 | 2 |
| Applied Method | ||
| Deterministic | 86 | 86 |
| Probabilistic/Stochastic | 9 | 9 |
| Deterministic and Probabilistic/Stochastic | 5 | 5 |
| Scope a | ||
| Human Health Risk Assessment | 100 | 100 |
| Integrated (human and environmental) | 4 | 4 |
| Holistic (integration of non-traditional data) | 0 | 0 |
| Framework Used a | ||
| US EPA | 75 | 75 |
| World Health Organization | 6 | 6 |
| Other (i.e., studies, government) | 15 | 15 |
| Unspecified | 12 | 12 |
| HHRA Terminology | ||
| Health (risk) Assessment | 47 | 47 |
| Human Health Risk Assessment | 25 | 25 |
| Risk Assessment | 24 | 24 |
| Other (e.g., cancer risk, risk estimate, etc.) | 14 | 14 |
| Factors and Uncertainty | ||
| Non-Traditional Factors acknowledged a | ||
| At least one non-traditional factor | 90 | 90 |
| Geography | 76 | 76 |
| Social | 23 | 23 |
| Economic | 13 | 13 |
| Risk Perception | 3 | 3 |
| Cultural/Spiritual | 2 | 2 |
| Other (e.g., behaviours, additional risks, temporal effects, etc.) | 22 | 22 |
| Non-Traditional Factors applied a | ||
| At least one non-traditional factor | 69 | 69 |
| Geography | 56 | 56 |
| Social | 4 | 4 |
| Economic | 2 | 2 |
| Risk Perception | 1 | 1 |
| Cultural/Spiritual | 1 | 1 |
| Other (e.g., behaviours, additional risks, temporal effects, etc.) | 16 | 16 |
| Uncertainty acknowledged a | ||
| At least one uncertainty acknowledged | 83 | 83 |
| Dedicated section to uncertainty | 20 | 20 |
| Quality Assurance/Quality Control | 47 | 47 |
| Analytical detection limits | 38 | 38 |
| Seasonal/Environment | 38 | 38 |
| Data gaps | 30 | 30 |
| Sufficiency of sampling | 28 | 28 |
| Quality of historical data | 10 | 10 |
| Other (e.g., exposures, toxicological factors, effects of unknown variables, etc.) | 18 | 18 |
| Outcomes | ||
| Result a | ||
| Exposure Assessment | 96 | 96 |
| Hazard Assessment | 95 | 95 |
| Hazard Quotient/Index | 81 | 81 |
| Epidemiological Assessment | 4 | 4 |
| Other (i.e., quantitative microbial risk assessment and cancer risk) | 27 | 27 |
| Conclusion by Authors | ||
| Quantitative | 94 | 94 |
| Quantitative and Qualitative | 4 | 4 |
| Qualitative | 2 | 2 |
| Characteristic | ||
|---|---|---|
| World Region | Number (n = 101 a) | Percentage (%) |
| Asia | 58 | 57.4 |
| West Africa | 9 | 8.9 |
| Europe | 7 | 6.9 |
| European Union | 8 | 7.9 |
| North America | 7 | 6.9 |
| South America | 4 | 4.0 |
| South Africa | 3 | 3.0 |
| Middle East | 2 | 2.0 |
| Caribbean | 1 | 1.0 |
| East Africa | 1 | 1.0 |
| Oceania | 1 | 1.0 |
| Publication Year | Number (n = 100) | Percentage (%) |
| January 2010–May 2014 | 75 | 75 |
| January 2005–December 2009 | 20 | 20 |
| January 2000–December 2004 | 5 | 5 |
| Gap Description | References |
|---|---|
| Research in HHRA | |
| Use of biomonitoring | [78] |
| Improved methods or application | [48,61,72,79,80] |
| Sources of uncertainty | [37,47] |
| Determining temporal exposures | [81] |
| Determining future exposures | [42,74] |
| Considering all pathways of exposure | [41,50,82,83,84,85] |
| Exposure to additional hazard sources | [41,63,73,86] |
| Exposure to mixtures | [34,53,58,83,87] |
| Guides to direct researchers | [88] |
| Gather more epidemiological evidence and toxicological data | [37,44,49,64,65,73,79,89] |
| Risk Management | |
| Collect data to inform management | [49,60,64,71] |
| Knowledge of geochemistry and aquifers | [89,90] |
| Monitoring | [58,79] |
| Evaluation of exposures | [54,59,86] |
| Establish national/regional HHRAs | [39,61,77,91] |
| Standardize methods for mixtures | [47] |
| Standardize regulations | [57,92] |
| Improved communication, response and determination of risk | [53,62,64,72] |
| Community Exposure | |
| Inclusion of specific community (i.e., sensitive community members) | [42] |
| Isolate risks specific to communities | [48,55,93] |
| Consider quality of life, socioeconomic, and political factors | [75,90,94] |
| Improve community involvement, engagement, education, and risk management | [49,53,95] |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ford, L.; Bharadwaj, L.; McLeod, L.; Waldner, C. Human Health Risk Assessment Applied to Rural Populations Dependent on Unregulated Drinking Water Sources: A Scoping Review. Int. J. Environ. Res. Public Health 2017, 14, 846. https://doi.org/10.3390/ijerph14080846
Ford L, Bharadwaj L, McLeod L, Waldner C. Human Health Risk Assessment Applied to Rural Populations Dependent on Unregulated Drinking Water Sources: A Scoping Review. International Journal of Environmental Research and Public Health. 2017; 14(8):846. https://doi.org/10.3390/ijerph14080846
Chicago/Turabian StyleFord, Lorelei, Lalita Bharadwaj, Lianne McLeod, and Cheryl Waldner. 2017. "Human Health Risk Assessment Applied to Rural Populations Dependent on Unregulated Drinking Water Sources: A Scoping Review" International Journal of Environmental Research and Public Health 14, no. 8: 846. https://doi.org/10.3390/ijerph14080846
APA StyleFord, L., Bharadwaj, L., McLeod, L., & Waldner, C. (2017). Human Health Risk Assessment Applied to Rural Populations Dependent on Unregulated Drinking Water Sources: A Scoping Review. International Journal of Environmental Research and Public Health, 14(8), 846. https://doi.org/10.3390/ijerph14080846