WHO Environmental Noise Guidelines for the European Region: A Systematic Review on Environmental Noise and Permanent Hearing Loss and Tinnitus

Abstract
:1. Introduction
- the first (lower) action level set at LEX,8h = 80 dBA;
- the second (upper) action level set at LEX,8h = 85 dBA; and,
- the maximum exposure limits set at LEX,8h = 87 dBA.
1.1. Leisure Activities
1.2. Aircraft, Road and Rail Noises
1.3. Impulse Noise
2. Materials and Methods
- High quality—Further research is very unlikely to change our confidence in the estimate of effect;
- Moderate quality—Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate;
- Low quality—Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate; and,
- Very low quality—Any estimate of effect is uncertain.
3. Results
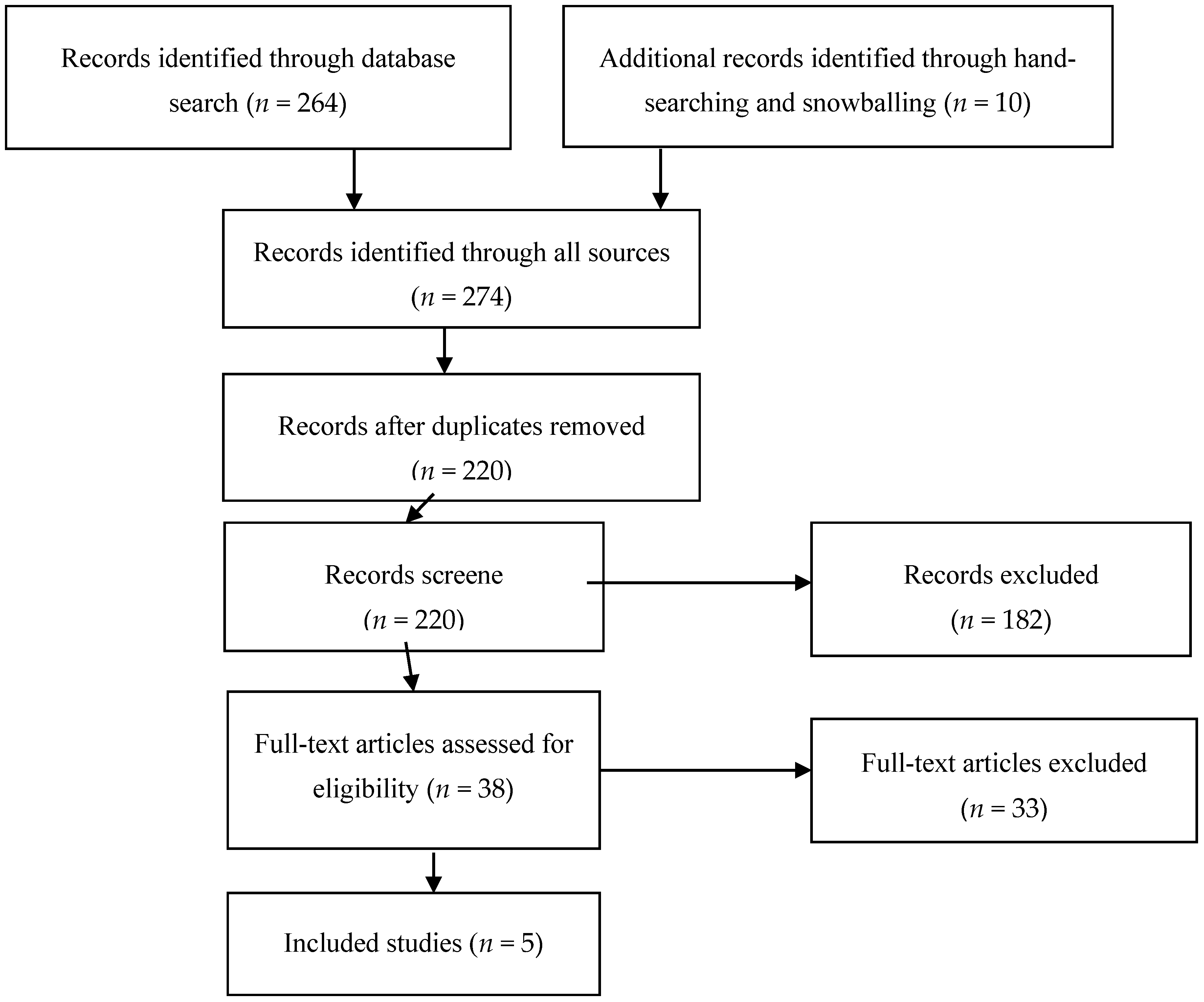
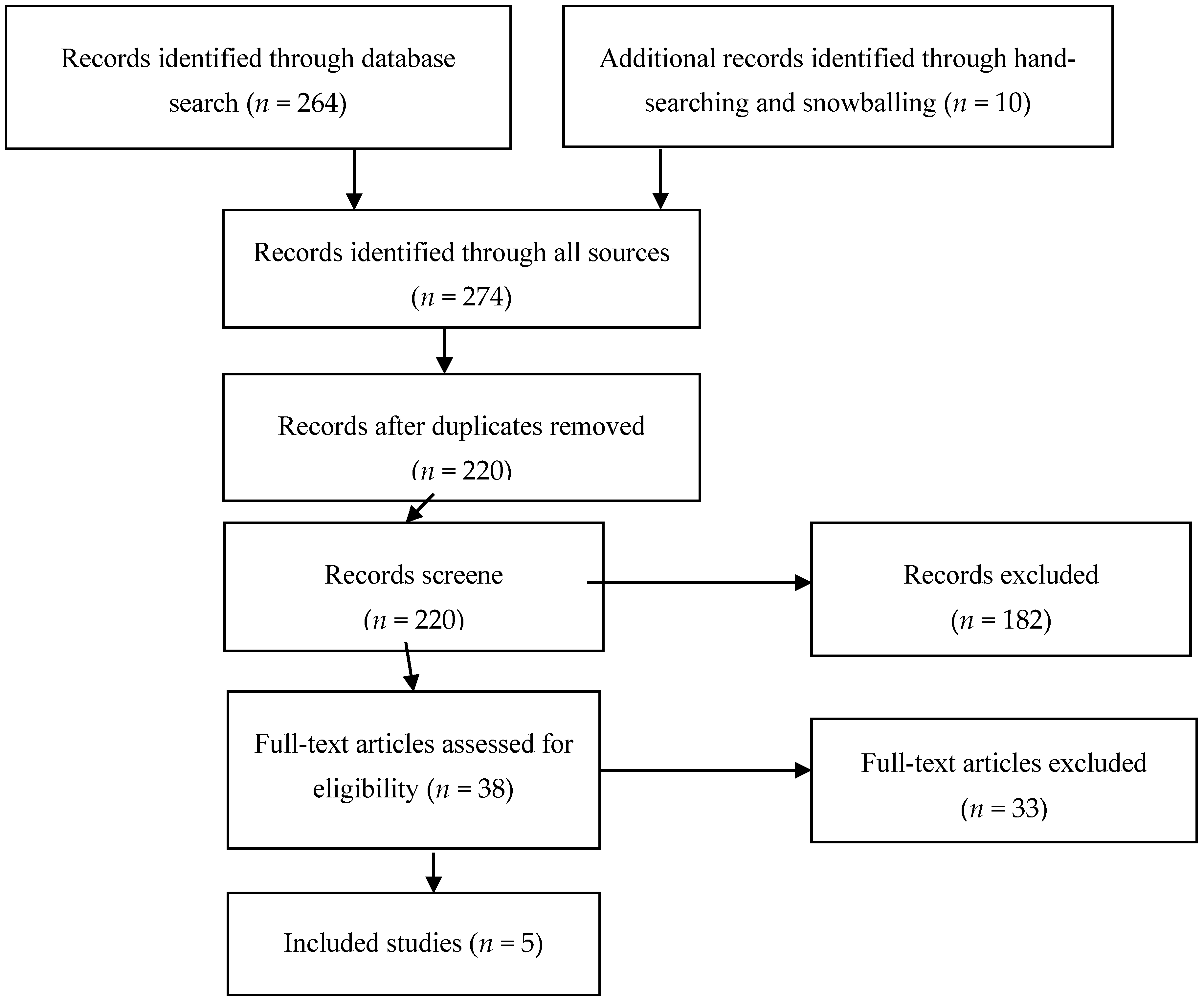
3.1. This Study Selection and Characteristics
3.2. Risk of Bias within Studies
- Feder et al. (2013) [39]—Low participation rate (only 11% of out of 237 invited subjects);
- Sulaiman et al. (2013) [25]—The selection of participants was most likely not random and the response rate was not provided;
- Lévesque et al. (2010) [21]—No inclusion or exclusion criteria were specified. No confounding factors were included. A lack of randomization. The diagnostic criteria of tinnitus were not specified;
- Vogel et al. (2014) [41]—No direct measurement of noise levels; lack of randomization. It is not clear what proportion of subjects with “permanent hearing-related symptoms” experienced permanent tinnitus. No validated method of tinnitus assessment;
- Sulaiman et al. (2014) [40]—No information provided about blinding the health outcome and/or exposure assessment.
3.3. Results of Individual Studies
3.3.1. Permanent Hearing Loss
3.3.2. Permanent Tinnitus
3.4. Synthesis of Results
3.4.1. Permanent Hearing Loss
3.4.2. Permanent Tinnitus
3.4.3. Risk of Bias across Studies
4. Discussion
4.1. Summary of Evidence
4.2. Limitations
5. Conclusions
- While using very strict inclusion criteria, there is low quality GRADE evidence that prolonged listening to loud music through PLDs increases the risk of hearing loss and results in worsening standard frequency audiometric thresholds.
- Specific threshold analyses focused on risk stratification of permanent hearing loss according to clearly defined levels of exposure to music through the PLDs are missing. This is due to many restrictions of conducting such research that are related to the long latency time from exposure to effect, the problems to correctly estimate the exposure, and the lack of sensitive measures to detect early signs of hearing loss.
- Available, yet very limited, data contradict any positive association between prolonged listening to loud music through PLDs and the risk of permanent tinnitus. Future studies are needed to provide actionable guidance for PLDs users.
- No studies fulfilling the inclusion criteria related to other isolated or combined exposures to environmental noise were identified.
- Since measurable audiometric hearing loss requires long exposure periods and individual dosimetry is preferable to overcome the methodological and practical drawbacks in exposure assessment, such cohort studies would be very challenging.
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- World Health Organization (WHO). Global Burden of Hearing Loss in the Year 2000. Available online: www.who.int/healthinfo/statistics/bod_hearingloss.pdf (accessed on 10 October 2016).
- Henderson, D.; Bielehed, E.C.; Harris, K.C.; Hu, B.H. The role of oxidative stress in noise-induced hearing loss. Ear Hear. 2006, 27, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Puel, J.L.; Ruel, J.; Guitton, M.; Pujol, R. The inner hair cell afferent/efferent synapses revisited: A basis for new therapeutic strategies. Adv. Otorhinolaryngol. 2002, 59, 124–130. [Google Scholar] [PubMed]
- Pilati, N.; Ison, M.J.; Barker, M.; Mulheran, M.; Large, C.H.; Forsythe, I.D.; Matthias, J.; Hamann, M. Mechanisms contributing to central excitability changes during hearing loss. Proc. Natl. Acad. Sci. USA 2012, 109, 8292–8297. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.W.; Furman, A.C.; Kujawa, S.G.; Liberman, M.C. Primary neural degeneration in the guinea pig cochlea after reversible noise-induced threshold shift. J. Assoc. Res. Otolaryngol. 2011, 12, 605–616. [Google Scholar] [CrossRef] [PubMed]
- Plack, C.J.; Barker, D.; Prendergast, G. Perceptual consequences of “hidden” hearing loss. Trends Hear. 2014, 18, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Commission. Directive 2003/10/EC of the European Parliament and of the Council of 6 February 2003 on the Minimum Health and Safety Requirements Regarding the Exposure of Workers to the Risks Arising from Physical Agents (Noise); European Commission: Brussels, Belgium, 2013. [Google Scholar]
- International Standard Organization (ISO). ISO 1999:1990: Acoustics—Determination of Occupational Noise Exposure and Estimation of Noise-Induced Hearing Impairment; International Standard Organization: Geneva, Switzerland, 1990. [Google Scholar]
- Beach, E.; Williams, W.; Gilliver, M. Estimating young Australian adults’ risk of hearing damage from selected leisure activities. Ear Hear. 2013, 34, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Johnson, O.; Andrew, B.; Walker, D.; Morgan, S.; Aldren, A. British university students’ attitudes towards noise-induced hearing loss caused by nightclub attendance. J. Laryngol. Otol. 2014, 128, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Lewis, R.C.; Gershon, R.R.; Neitzel, R.L. Estimation of permanent noise-induced hearing loss in an urban setting. Environ. Sci. Technol. 2013, 47, 6393–6399. [Google Scholar] [CrossRef] [PubMed]
- Berg, A.L.; Serpanos, Y.C. High frequency hearing sensitivity in adolescent females of a lower socioeconomic status over a period of 24 years (1985–2008). J. Adolesc. Health 2011, 48, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Cone, B.K.; Wake, M.; Tobin, S.; Poulakis, Z.; Rickards, F.W. Slight-mild sensorineural hearing loss in children: Audiometric, clinical, and risk factor profiles. Ear Hear. 2010, 31, 202–212. [Google Scholar] [CrossRef] [PubMed]
- Vogel, I.; Brug, J.; Van der Ploeg, C.P.; Raat, H. Adolescents risky MP3-player listening and its psychosocial correlates. Health Educ. Res. 2011, 26, 254–264. [Google Scholar] [CrossRef] [PubMed]
- Pellegrino, E.; Lorini, C.; Allodi, G.; Buonamici, C.; Garofalo, G.; Bonaccorsi, G. Music-listening habits with MP3 player in a group of adolescents: A descriptive survey. Ann. Ig. 2013, 25, 367–376. [Google Scholar] [PubMed]
- World Helath Organization (WHO). 2015 Hearing Loss due to Recreational Exposure to Loud Sound. A Review. Available online: http://apps.who.int/iris/bitstream/10665/154589/1/9789241508513_eng.pdf? ua=1 (accessed on 10 October 2016).
- European Commission—Scientific Committee on Emerging and Newly Identified Health Risks. Potential Health Risks of Exposure to Noise from Personal Music Players and Mobile Phones Including a Music Playing Function. 2008. Available online: http://ec.europa.eu/health/ph_risk/committees/04_scenihr/docs/scenihr_o_018.pdf (accessed on 10 October 2016).
- Portnuff, C.D.; Fligor, B.J.; Arehart, K.H. Teenage use of portable listening devices: A hazard to hearing? J. Am. Acad. Audiol. 2011, 22, 663–677. [Google Scholar] [CrossRef] [PubMed]
- Portnuff, C.D.; Fligor, B.J.; Arehart, K.H. Self-report and long-term field measures of MP3 player use: How accurate is self-report? Int. J. Audiol. 2013, 52, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Williams, W. Trends in listening to personal stereos. Int. J. Audiol. 2009, 48, 784–788. [Google Scholar] [CrossRef] [PubMed]
- Lévesque, B.; Fiset, R.; Isabelle, L.; Gauvin, D.; Baril, J.; Larocque, R.; Gingras, S.; Leroux, T.; Picard, M.; Girard, S.A. Exposure of high school students to noise from personal music players in Québec City, Canada. Int. J. Child. Adolesc. Health 2010, 3, 413–420. [Google Scholar]
- Keith, S.E.; Michaud, D.S.; Feder, K.; Haider, I.; Marro, L.; Thompson, E.; Marcoux, A.M. MP3 player listening sound pressure levels among 10 to 17 year old students. J. Acoust. Soc. Am. 2011, 130, 2756–2764. [Google Scholar] [CrossRef] [PubMed]
- Muchnik, C.; Amir, N.; Shabtai, E.; Kaplan-Neeman, R. Preferred listening levels of personal listening devices in young teenagers: Self reports and physical measurements. Int. J. Audiol. 2012, 51, 287–293. [Google Scholar] [CrossRef] [PubMed]
- Breinbauer, H.A.; Anabalón, B.; Gutierrez, D.; Cárcamo, R.; Olivares, C.; Caro, J. Output capabilities of personal music players and assessment of preferred listening levels of test subjects: Outlining recommendations for preventing music-induced hearing loss. Laryngoscope 2012, 122, 2549–2556. [Google Scholar] [CrossRef] [PubMed]
- Sulaiman, A.H.; Seluakumaran, K.; Husain, R. Hearing risk associated with the usage of personal listening devices among urban high school students in Malaysia. Public Health 2013, 127, 710–715. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Occupational Safety and Health (NIOSH). Criteria for Recommended Standard—Occupational Noise Exposure: Revised Criteria; U.S. Department of Health and Human Servives: Cincinnati, OH, USA, 1998.
- Lee, G.J.; Lim, M.Y.; Kuan, A.Y.; Teo, J.H.; Tan, H.G.; Low, W.K. The music listening preferences and habits of youths in Singapore and its relation to leisure noise-induced hearing loss. Singap. Med. J. 2014, 55, 72–77. [Google Scholar] [CrossRef]
- Vasconcellos, A.P.; Kyle, M.E.; Gilani, S.; Shin, J.J. Personally modifiable risk factors associated with pediatric hearing loss: A systematic review. Otolaryng. Head Neck 2014, 15, 14–28. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.; Chen, S. Effects of aircraft noise on hearing and auditory pathway function of school-age children. Int. Arch. Occup. Environ. Health 1993, 65, 107–111. [Google Scholar] [CrossRef] [PubMed]
- Green, K.B.; Pasternack, B.S.; Shore, R.E. Effects of aircraft noise on hearing ability of school-age children. Arch. Environ. Health 1982, 37, 284–289. [Google Scholar] [CrossRef] [PubMed]
- Andrus, W.S.; Kerrigan, M.E.; Bird, K.T. Hearing in para-airport children. Aviat. Space Environ. Med. 1975, 46, 740–742. [Google Scholar] [PubMed]
- Fisch, L. Aircraft noise and hearing impairment in children. Br. J. Audiol. 1981, 15, 231–240. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, D. Research on road traffic noise and human health in India: Review of literature from 1991 to current. Noise Health 2012, 14, 113–118. [Google Scholar] [PubMed]
- European Commission, Community Research and Development Information Service. The Policy Interpretation Network on Children’s Health and Environment (PINCHE) Project; Final Report WP1 Exposure Assessment; Public Health Services Gelderland Midden: Arnhem, The Netherlands, 2005. [Google Scholar]
- AS/NZS ISO 8124.1. AS/NZS ISO 8124.1:2010: Safety of Toys, Part 1: Safety Aspects Related to Mechanical and Physical Properties (ISO 8124–1:2009); Standards New Zealand: Wellington, New Zealand, 2010. [Google Scholar]
- AS/NZS ISO 8124.1. AS/NZS ISO 8124.1:2013: Safety of Toys, Part 1: Safety Aspects Related to Mechanical and Physical Properties (ISO 8124–1:2012); Standards New Zealand: Wellington, New Zealand, 2013. [Google Scholar]
- EN 71-1:2011+A2:2013. Safety of Toys—Part 1: Mechanical and Physical Properties; European Committee for Standardization; European Commission: Brussels, Belgium, 2013. [Google Scholar]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE Working Group. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef] [PubMed]
- Feder, K.; Marro, L.; Keith, S.E.; Michaud, D.S. Audiometric thresholds and portable digital audio player user listening habits. Int. J. Audiol. 2013, 52, 606–616. [Google Scholar] [CrossRef] [PubMed]
- Sulaiman, A.H.; Husain, R.; Seluakumaran, K. Evaluation of early hearing damage in personal listening device users using extended high-frequency audiometry and otoacoustic emissions. Eur. Arch. Otorhinolaryngol. 2014, 271, 1463–1470. [Google Scholar] [CrossRef] [PubMed]
- Vogel, I.; van de Looij-Jansen, P.M.; Mieloo, C.L.; Burdorf, A.; de Waart, F. Risky music listening, permanent tinnitus and depression, anxiety, thoughts about suicide and adverse general health. PLoS ONE 2014, 9, e98912. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hodgetts, W.E.; Riecker, J.M.; Szarko, R.A. The effects of listening environment and earphone style on preferred listening levels of normal hearing adults using an MP3 player. Ear Hear. 2007, 28, 290–297. [Google Scholar] [CrossRef] [PubMed]
- Barlow, C. Evidence of noise-induced hearing loss in young people studying popular music. Med. Probl. Perform. Art. 2011, 26, 96–101. [Google Scholar] [PubMed]
- Pawlaczyk-Luszczynska, M.; Dudarewicz, A.; Zaborowski, K.; Zamojska, M.; Sliwinska-Kowalska, M. Noise induced hearing loss: Research in central, eastern and south-eastern Europe and newly independent states. Noise Health 2013, 15, 55–65. [Google Scholar] [CrossRef] [PubMed]
- Meyer-Bisch, C. Epidemiological evaluation of hearing damage related to strongly amplified music (personal cassette players, discotheques, rock concerts) high-definition audiometric survey on 1364 subjects. Audiology 1996, 35, 121–142. [Google Scholar] [CrossRef] [PubMed]
- Marron, K.H.; Sproat, B.; Ross, D.; Wagner, S.; Alessio, H. Music listening behavior, health, hearing and otoacoustic emission levels. Int. J. Environ. Res. Public Health 2014, 11, 7592–7607. [Google Scholar] [CrossRef] [PubMed]
- Weichbold, V.; Holzer, A.; Newesely, G.; Stephan, K. Results from high-frequency hearing screening in 14- to 15-year old adolescents and their relation to self-reported exposure to loud music. Int. J. Audiol. 2012, 51, 650–654. [Google Scholar] [CrossRef] [PubMed]
- Peng, J.H.; Tao, Z.Z.; Huang, Z.W. Risk of Damage to Hearing from Personal Listening Devices in Young Adults. J. Otolaryngol. 2007, 36, 181–185. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.G.; Hong, S.M.; Shim, H.J.; Kim, Y.D.; Cha, C.I.; Yeo, S.G. Hearing threshold of Korean adolescents associated with the use of personal music players. Yonsei Med. J. 2009, 50, 771–776. [Google Scholar] [CrossRef] [PubMed]
- Moshammer, H.; Kundi, M.; Wallner, P.; Herbst, A.; Feuerstein, A.; Hutter, H.P. Early prognosis of noise-induced hearing loss. Occup. Environ. Med. 2015, 72, 85–89. [Google Scholar] [CrossRef] [PubMed]
- Vogel, I.; Verschuure, H.; van der Ploeg, C.P.; Brug, J.; Raat, H. Estimating adolescent risk for hearing loss based on data from a large school-based survey. Am. J. Public Health 2010, 100, 1095–1100. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Action Level | LEX,8h | Equivalent Levels for Time Indicated (Trade-Off 3 dB) |
|---|---|---|
| First Action level (minimum) provide protection | 80 dB(A) | 83 dBA-4 h *; 86 dBA-2 h; 89 dBA-1 h; |
| 92 dBA-30 min **; 95 dBA-15 min; 98 dBA-8 min; | ||
| 101 dBA-4 min; 104 dBA-2 min; 107 dBA-1 min | ||
| Second Action level mandatory protection | 85 dB(A) | 88 dBA-4 h; 91 dBA-2 h; 94 dBA-1 h; |
| 97 dBA-30 min; 100 dBA-15 min; 105 dBA-5 min; | ||
| 111 dBA-1 min | ||
| Maximum Exposure limit value | 87 dB(A) | 90 dBA-4 h; 93 dBA-2 h; 96 dBA-1 h; |
| 99 dBA-30 min; 102 dBA-15 min; 107 dBA-5 min; | ||
| 113 dBA-1 min |
| No | Author, Year | Population | Exposure | References Group | Confounding | Outcome |
|---|---|---|---|---|---|---|
| 1. | Keith et al. (2011) [22] | 248 Canadian individuals aged 10–18, 110 males and 138 females, 29 subjects excluded, random school and student selection. | Individual LEX was calculated according to ISO 1999, open-ended question about the hours per week listening to music, weekly allowable listening duration time was divided by seven to derive an estimate of average daily listening duration, measurement made in classrooms, for 32 s listening of music at the typical and “worst-case” volume levels, background noise between 40 and 52 dBA. | ISO 1990 | All uncertainty estimates were based on the ISO/IEC guide (ISO/IEC, 1995). Low participation rate of 11%. | 3.2% of subjects were estimated to exceed the level limit of 85 dBA LEX of the typical volume settings. 77.5% of listeners were exposed to the level for which there is no known risk of permanent noise induced hearing loss, i.e., ≤75 dBA LEX. |
| 2. | Portnuff et al. (2013) [19] | 52 US individuals, aged 18–29, hearing threshold no worse than 20 dB HL, at least 10 h use of PLD a week, 24 from this group were chosen at random for dosimetry. | An earphone data logging system connected with the dosimeter was developed in order to record the real-world use of PLD, dose calculation: self-reported chosen listening level (CLL) (Dose usual), the CLL by volume control increments (Dose vol) and the measured dose from the logg in system (Dose measured). | NIOSH, OSHA | Bias due to participants selection (listening for at least 10 h a week). | Weekly damage risk criteria were exceeded in 16.7% subjects and 8.3% of subjects according to NIOSH and OSHA standards, respectively. |
| 3. | Portnuff et al. (2011) [18] | 29 US individuals (12 males and 17 females), aged 13–17, using MP3 players at least two hours per week, normal hearing thresholds (no worse than 15 dB HL). | Individual noise doses calculated based on self-reported listening time and self-reported volume control setting (based on translation of volume control settings to diffuse-field equivalent output levels). | EPCEU, NIOSH and OSHA criteria | No direct SPL measurement. | Doses of noise higher than damage risk criteria in 0%—OSHA, in 6.9%—NIOSH, 13.8%—EPCEU of subjects. |
| 4. | Lee et al. (2014) [27] | 1928 Singapore university freshman, aged 16–21 years, different races, 129 students excluded, 95.8% regular PLD users. | Based on volume setting and questionnaire. Pre-calibrated MP3 players, so the equivalent A-weighted SPL of the different volume settings was known | TWA 8 h > 85 dBA | No direct SPL measurement | 16.4% students were exposed at TWA 8 h > 85 dBA. Differences between races—Chinese less exposed. |
| 5. | Muchnik et al. (2012) [23] | 74 Israeli individuals (26 males and 48 females), aged 14–16 year, regular PLDs users, no history of hearing problems and middle ear pathologies. | Preferred listening levels of six types of PLDs. Volume control setting transformed to SPLs which were in turn converted to equivalent diffuse field A-weigthed levels, ambient noise 61–70 dBA. LAeq 85 dBA were calculated. | NIOSH | No direct SPL measurement. Measurement done in the presence of background noise. | Mean preferred listening level 89 (SD—9) dBA. 26% of the participants in the noisy condition were found to be at risk according to occupational damage risk NIOSH criteria (NIOSH 1998). |
| 6. | Vogel et al. (2011) [14] | 1687 Dutch students from 15 Dutch secondary schools invited, response rate 89.9% (1512 subjecrts, 89.9% of tjose PLD users) | Average weekly exposure time to MP3 players was estimated by referring the volume of the device to dB(A) value and multiplying days per week and hours per day to calculate (weekly) Permissible Exposure Limits (PELweek = music level of 89 dBA listen for 56 h a week). | 89 dBA for ≥1 h per day. Reffered to the safe level of 80 dBA (like in SCENIHR report) converted to LEX,w of 56 h. | No direct SPL measurement. | 28.6% of risk 89 dBA ≥ 1 h. |
| Source | Leisure Steady-State Noise/Music | Impulse Noise | Aircraft/Traffic Noise and Other Exposures | Total | ||||
|---|---|---|---|---|---|---|---|---|
| Number of Studies | PLD | Bars | Concerts | Sport Events | Toys, Firearms & Firecrackers | |||
| Included studies | 5 | 0 | 0 | 0 | 0 | 0 | 5 | |
| Excluded studies | 116 | 15 | 68 | 6 | 37 | 12 | 215 * | |
| Total | 121 | 15 | 68 | 6 | 37 | 12 | 220 * | |
| No | Author and Year | Study Design and the Number of Subjects | Age of Subjects (Year) | Exposure Assessment | Health Outcome and the Method of Measurement | The Number (Percent) of Subjects with Hearing Loss/Tinnitus | Data Analysis | Main Results and Conclusions | Risk of Bias |
|---|---|---|---|---|---|---|---|---|---|
| 1. | Feder et al. (2013) [39] | Cross-sectional (n = 237) | 10–17 | Individual Leq(32 s) and LEX,8h estimates | Permanent hearing loss; PTA | Data not reported | Multivariate models for audiometric frequencies (estimate (SE), p-value from t-test based on multivariate model). | Positive correlation between Lex(8 h) and hearing threshold at 4 kHz and LFPTA (low frequency pure-tone average for frequencies 0.5, 1 and 2 kHz) Subjects reporting using their player for >5years and those reporting using their player for 1 to <3 years both had higher HT than those using their player for <1 year | High, due to low subject participation rate (only 11%) and no information provided about blinding the health outcome and/or exposure assessment |
| 2. | Sulaiman et al. (2013) [25] | Cross-sectional (n = 177) | 13–16 | Individual LAeq8h | 1. Permanent hearing loss; standard PTA and extended high frequencies PTA 2. Tinnitus (possibly permanent) | Hearing loss found in 13 (7.3%) of subjects in entire population. Tinnitus reported by 30 (16.9%) subjects exposed to music at LAeq8h ≤ 75 dBA and by 7 (4.0%) of those exposed to music at LAeq8h >75 dBA. | Pearson correlation test, Chi-squared test | No significant association between subjects’ LAeq8h exposure levels and the incidence of hearing loss (defined as HT ≥ 25 dB at one or more standard frequencies), or the occurrence of notched audiograms. Weak significant correlation between individual LAeq8h and HT at 11.2 and 14 kHz. No relationship between individual LAeq8h and tinnitus. | High, the response rate was not provided, neither the information about blinding the health outcome and/or exposure assessment. |
| 3. | Sulaiman et al. (2014) [40] | Cross-sectional (35 exposed subjects and equal number of age and sex matched not exposed subjects) | 18–30 | Individual LAeq8h | Permanent hearing loss; standard PTA and extended high frequencies PTA, otoacoustic emissions | Hearing loss (defined as HT ≥ 25 dB at one or more standard frequencies) in 12 (34.3%) of users and 4 (11.4%) of control subjects. | Descriptive analysis, unpaired Student t test, Pearson correlation test, Fisher’s exact test. | Significant association between the incidence of hearing loss and PLDs usage. Weak but significant correlation between users’ LAeq8h exposure levels and their PTA thresholds pooled from 3, 4 and 6 kHz in the right ear only. Hearing thresholds of PLDs users at extended high frequencies significantly higher than in non-users. Otoacoustic emissions amplitudes in users significantly reduced compared with controls. | High, no information provided about blinding the health outcome and/or exposure assessment. |
| 4. | Lévesque et al. (2010) [21] | Cross-sectional (n = 124) | 14–17 | Individual LAeq8h | Tinnitus (possibly permanent); questionnaire | Tinnitus reported by 2 (4.1%) of subjects exposed to music at LAeq8h ≤ 80 dBA and by 12 (16.0%) of those exposed to music at LAeq8h > 80 dBA. Tinnitus reported by 5 (6.9%) of subjects exposed to music at LAeq8h ≤ 85 dBA and by 9 (17.3%) of those exposed to music at LAeq8h > 85 dBA. | Binary outcome, chi2 test | Significant difference in prevalence of tinnitus between groups when the LAeq8h reference value set at 80 dBA. No significant difference in prevalence of tinnitus when the LAeq8h reference value set at 85 dBA. | Very high, due to the lack of specification of inclusion/exclusion criteria, participation rate 63.3%, diagnostic criteria of tinnitus not specified, no confounding factors included, no information provided about blinding the health outcome and/or exposure assessment. |
| 5. | Vogel et al. (2014) [41] | Cross-sectional (n = 943) | 16–25 | Individual sound levels in dBA for 56 h per week, estimated based on PLD volume setting (Permissible Exposure Limits (PELweek = music level of 89 dBA listen for 56 h a week) | Permanent hearing-related symptoms; questionnaire (not clear what proportion of subjects with “permanent hearing-related symptoms” experienced permanent tinnitus) | Permanent hearing-related symptoms reported by 101 (10.7%) of subjects not at risk (<80 dBA), 93 (9.9%) of subjects at low risk (80–85 dBA), 97 (10.3%) of subjects at moderate risk (85–90 dBA) and 41 (4.4%) of subjects at high risk (≥90 dBA). | Multiple logistic regression; ORs: 0.86 (0.49–1.46), 0.93 (0.50–1.75) 0.39 (0.18–0.86) for low risk (80–85 dBA), moderate risk (85–90 dBA) and high risk (≥90 dBA) group of listeners. | Students not experiencing permanent hearing-related symptoms listen > 2.5 times more often to high-risk sound levels (equivalent to ≥ 90 dBA for 56 h per week). | High, because of the lack of direct measurement of sound pressure levels, health outcome assessment leading to information bias. |
| No | Author and Year | Health Outcome | Reference Values (LAeq8h) | OR | (95% CI) | Number of Participants | Risk of Bias |
|---|---|---|---|---|---|---|---|
| 1. | Sulaiman et al. (2013) [25] | Tinnitus | ≤75 dBA | 1.00 | 177 | High | |
| >75 dBA | 1.13 1 | (0.44—2.89) 1 | |||||
| 2. | Levesque et al. (2010) [21] | Tinnitus | ≤80 dBA | 1.00 | 124 | Very high | |
| >80 dBA | 4.48 1 | (0.94–21.29) 1 | |||||
| ≤85 dBA | 1.00 | ||||||
| >85 dBA | 2.80 1 | (0.87–9.04) 1 | |||||
| 3. | Vogel et al. (2014) [41] | Permanent hearing related symptoms (tinnitus) | <80 dBA | 1.00 | 943 | High | |
| 80–85 dBA | 0.86 | (0.49–1.49) | |||||
| 85–90 dBA | 0.93 | (0.50–1.75) | |||||
| ≥90 dBA | 0.39 | (0.18–0.86) | |||||
| 4. | Sulaiman et al. (2014) [40] | Permanent hearing loss * | non users | 1.00 | 70 | High | |
| Users ** | 4.04 1 | (1.13–14.49) 1 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Śliwińska-Kowalska, M.; Zaborowski, K. WHO Environmental Noise Guidelines for the European Region: A Systematic Review on Environmental Noise and Permanent Hearing Loss and Tinnitus. Int. J. Environ. Res. Public Health 2017, 14, 1139. https://doi.org/10.3390/ijerph14101139
Śliwińska-Kowalska M, Zaborowski K. WHO Environmental Noise Guidelines for the European Region: A Systematic Review on Environmental Noise and Permanent Hearing Loss and Tinnitus. International Journal of Environmental Research and Public Health. 2017; 14(10):1139. https://doi.org/10.3390/ijerph14101139
Chicago/Turabian StyleŚliwińska-Kowalska, Mariola, and Kamil Zaborowski. 2017. "WHO Environmental Noise Guidelines for the European Region: A Systematic Review on Environmental Noise and Permanent Hearing Loss and Tinnitus" International Journal of Environmental Research and Public Health 14, no. 10: 1139. https://doi.org/10.3390/ijerph14101139
APA StyleŚliwińska-Kowalska, M., & Zaborowski, K. (2017). WHO Environmental Noise Guidelines for the European Region: A Systematic Review on Environmental Noise and Permanent Hearing Loss and Tinnitus. International Journal of Environmental Research and Public Health, 14(10), 1139. https://doi.org/10.3390/ijerph14101139