
Who Is Vulnerable to Dengue Fever? A Community Survey of the 2014 Outbreak in Guangzhou, China


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
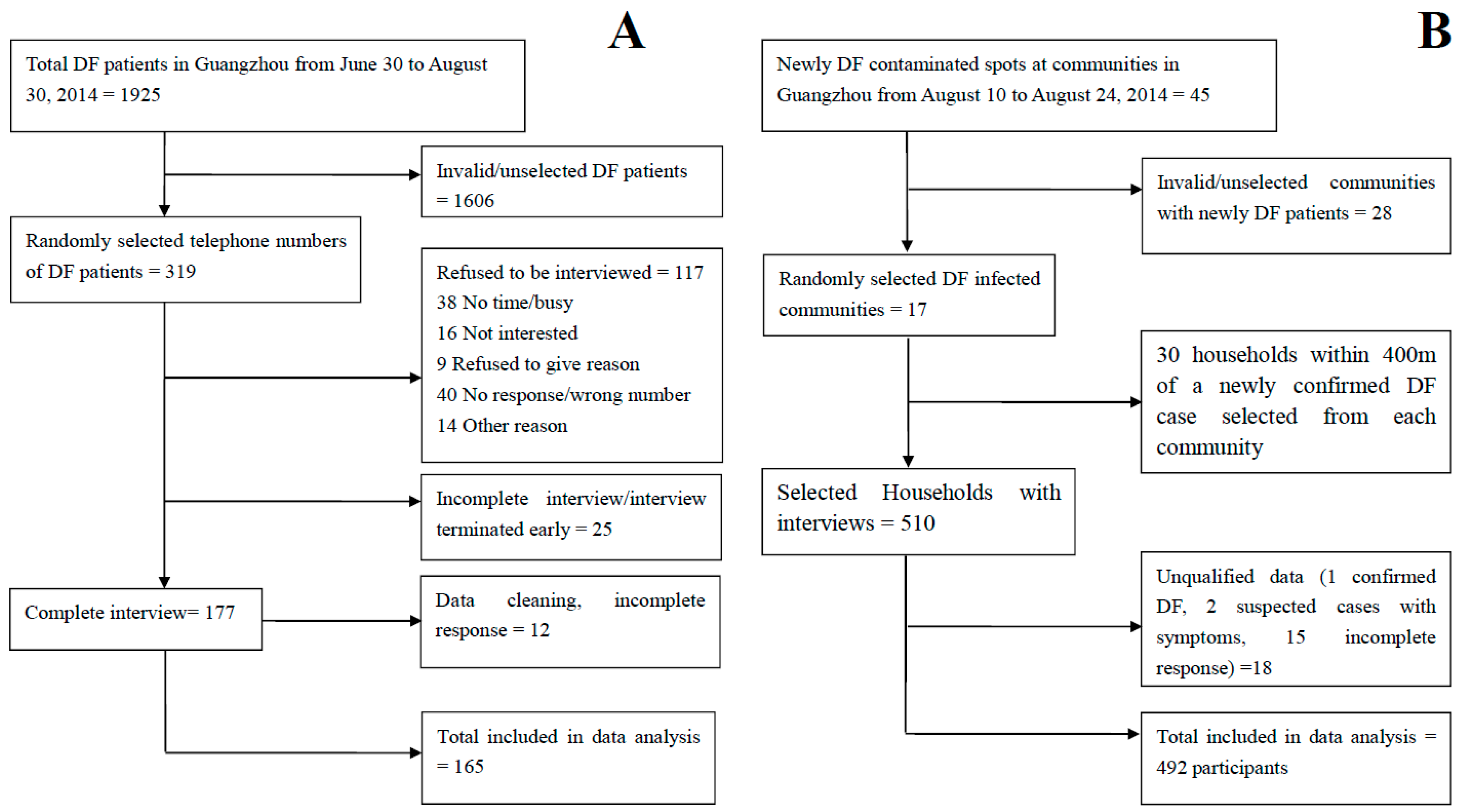
2.2. Cases
2.3. Controls
2.4. Study Sample
2.5. Survey Instruments
2.6. Data Analysis
2.7. Ethical Consideration
3. Results
3.1. Demographic Characteristic
3.2. Univariate Analysis
3.2.1. Exposure Characteristics
3.2.2. Knowledge and Practices
3.3. Multivariate Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Guzman, M.G.; Harris, E. Dengue. Lancet 2015, 385, 453–465. [Google Scholar] [CrossRef]
- Yang, G.J.; Liu, L.; Zhu, H.R.; Griffiths, S.M.; Tanner, M.; Bergquist, R.; Utzinger, J.; Zhou, X.N. China’s sustained drive to eliminate neglected tropical diseases. Lancet Infect. Dis. 2014, 14, 881–892. [Google Scholar] [CrossRef]
- Wu, J.Y.; Lun, Z.R.; James, A.A.; Chen, X.G. Dengue fever in mainland China. Am. J. Trop. Med. Hyg. 2010, 83, 664–671. [Google Scholar] [CrossRef] [PubMed]
- Chen, B.; Liu, Q. Dengue fever in China. Lancet 2015, 385, 1621–1622. [Google Scholar] [CrossRef]
- Ooi, E.E. The re-emergence of dengue in China. BMC Med. Central 2015, 13, 99. [Google Scholar] [CrossRef] [PubMed]
- International Guangzhou. Administrative Regions and Population. Available online: http://english.gz.gov.cn/gzgoven/s3616/201508/849fdfb0543b4fc5bbaadb967aa0fa2f.shtml (accessed on 16 March 2016).
- Jiang, C.; Schieffelin, J.S.; Li, J.; Sun, W. Dengue fever: A new challenge for China? Glob. Health Action 2014, 7, 26421. [Google Scholar] [CrossRef] [PubMed]
- Qin, C.; Shi, P. Dengue in China: Not a passing problem. Sci. China. Life Sci. 2014, 57, 1230–1231. [Google Scholar] [CrossRef] [PubMed]
- Horstick, O.; Runge-Ranzinger, S.; Nathan, M.B.; Kroeger, A. Dengue vector-control services: How do they work? A systematic literature review and country case studies. Trans. R. Soc. Trop. Med. Hyg. 2010, 104, 379–386. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Global Strategic Framework for Integrated Vector Management; World Health Organization: Geneva, Switzerland, 2004; p. 10. [Google Scholar]
- World Health Organization (WHO). Handbook for Integrated Vector Management. Available online: http://whqlibdoc.who.int/publications/2012/9789241502801_eng.pdf (accessed on 16 March 2016).
- Michael, A.T.; Chen, A.A.; Rawlins, S.; Heslop-Thomas, C.; Amarakoon, A.; Bailey, W.; Chadee, D.; Huntley, S.; Rhoden, C.; Stennett, R. Adapting to Dengue Risk—What to Do? AIACC Working Papers: Washington, DC, USA, 2006; Volume 6. [Google Scholar]
- Castro, M.; Sanchez, L.; Perez, D.; Sebrango, C.; Shkedy, Z.; Van der Stuyft, P. The relationship between economic status, knowledge on dengue, risk perceptions and practices. PLoS ONE 2013, 8, e81875. [Google Scholar]
- Isa, A.; Loke, Y.K.; Smith, J.R.; Papageorgiou, A.; Hunter, P.R. Mediational effects of self-efficacy dimensions in the relationship between knowledge of dengue and dengue preventive behaviour with respect to control of dengue outbreaks: A structural equation model of a cross-sectional survey. PLoS Negl. Trop. Dis. 2013, 7, e2401. [Google Scholar] [CrossRef] [PubMed]
- Matthias, J.; Zielinski-Gutierrez, E.C.; Tisch, D.J.; Stanek, D.; Blanton, R.E.; Doyle, M.S.; Eadie, R.B.; Gazdick, E.J.; Leal, A.L.; Pattison, K.J.; et al. Evaluating public housing residents for knowledge, attitudes, and practices following dengue prevention outreach in Key West, Florida. Vector Borne Zoonotic Dis. 2014, 14, 788–793. [Google Scholar] [CrossRef] [PubMed]
- Naeem-Ullah, U.; Akram, W. Dengue knowledge, attitudes and practices in multan, pakistan: An urban area at the verge of dengue infestation. Public Health 2009, 123, 452–453. [Google Scholar] [CrossRef] [PubMed]
- Suwanbamrung, C.; Promsupa, S.; Doungsin, T.; Tongjan, S. Risk factors related to dengue infections in primary school students: Exploring students’ basic knowledge of dengue and examining the larval indices in Southern Thailand. J. Infect. Public Health 2013, 6, 347–357. [Google Scholar] [CrossRef] [PubMed]
- Van Benthem, B.H.; Khantikul, N.; Panart, K.; Kessels, P.J.; Somboon, P.; Oskam, L. Knowledge and use of prevention measures related to dengue in northern Thailand. Trop. Med. Int. Health TM IH 2002, 7, 993–1000. [Google Scholar] [CrossRef] [PubMed]
- Wong, L.P.; AbuBakar, S.; Chinna, K. Community knowledge, health beliefs, practices and experiences related to dengue fever and its association with IgG seropositivity. PLoS Negl. Trop. Dis. 2014, 8, e2789. [Google Scholar] [CrossRef] [PubMed]
- Luo, L.; Liang, H.Y.; Hu, Y.S.; Liu, W.J.; Wang, Y.L.; Jing, Q.L.; Zheng, X.L.; Yang, Z.C. Epidemiological, virological, and entomological characteristics of dengue from 1978 to 2009 in Guangzhou, China. J. Vector Ecol. J. Soc. Vector Ecol. 2012, 37, 230–240. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Wang, Y.; Jin, S.; Wu, Z.; Chin, D.P.; Koplan, J.P.; Wilson, M.E. Emergence and control of infectious diseases in China. Lancet 2008, 372, 1598–1605. [Google Scholar] [CrossRef]
- Diagnostic Criteria for Dengue Fever (ws 216–2008). Available online: http://www.moh.gov.cn/publicfiles/business/htmlfiles/mohzcfgs/pggtg/200804/29860.htm (accessed on 16 March 2016).
- Reiter, P.; Lathrop, S.; Bunning, M.; Biggerstaff, B.; Singer, D.; Tiwari, T.; Baber, L.; Amador, M.; Thirion, J.; Hayes, J.; et al. Texas lifestyle limits transmission of dengue virus. Emerg. Infect. Dis. 2003, 9, 86–89. [Google Scholar] [CrossRef] [PubMed]
- Toan, D.T.; Hoat, L.N.; Hu, W.; Wright, P.; Martens, P. Risk factors associated with an outbreak of dengue fever/dengue haemorrhagic fever in Hanoi, Vietnam. Epidemiol. Infect. 2015, 143, 1594–1598. [Google Scholar] [CrossRef] [PubMed]
- Wong, L.P.; Shakir, S.M.; Atefi, N.; AbuBakar, S. Factors affecting dengue prevention practices: Nationwide survey of the Malaysian public. PLoS ONE 2015, 10, e0122890. [Google Scholar] [CrossRef] [PubMed]
- Fan, J.; Wei, W.; Bai, Z.; Fan, C.; Li, S.; Liu, Q.; Yang, K. A systematic review and meta-analysis of dengue risk with temperature change. Int. J. Environ. Res. Public Health 2014, 12, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Arunachalam, N.; Tana, S.; Espino, F.; Kittayapong, P.; Abeyewickreme, W.; Wai, K.T.; Tyagi, B.K.; Kroeger, A.; Sommerfeld, J.; Petzold, M. Eco-bio-social determinants of dengue vector breeding: A multicountry study in urban and periurban Asia. Bull. World Health Org. 2010, 88, 173–184. [Google Scholar] [CrossRef] [PubMed]
- Wan-Norafikah, O.; Nazni, W.A.; Noramiza, S.; Shafa’ar-Ko’ohar, S.; Azirol-Hisham, A.; Nor-Hafizah, R.; Sumarni, M.G.; Mohd-Hasrul, H.; Sofian-Azirun, M.; Lee, H.L. Vertical dispersal of aedes (stegomyia) spp. in high-rise apartments in Putrajaya, Malaysia. Trop. Biomed. 2010, 27, 662–667. [Google Scholar] [PubMed]
- Dieng, H.; Saifur, R.G.; Hassan, A.A.; Salmah, M.R.; Boots, M.; Satho, T.; Jaal, Z.; AbuBakar, S. Indoor-breeding of Aedes albopictus in northern peninsular Malaysia and its potential epidemiological implications. PLoS ONE 2010, 5, e11790. [Google Scholar] [CrossRef] [PubMed]
- Waldock, J.; Chandra, N.L.; Lelieveld, J.; Proestos, Y.; Michael, E.; Christophides, G.; Parham, P.E. The role of environmental variables on Aedes albopictus biology and chikungunya epidemiology. Pathog. Glob. Health 2013, 107, 224–241. [Google Scholar] [CrossRef] [PubMed]
- Chinnakali, P.; Gurnani, N.; Upadhyay, R.P.; Parmar, K.; Suri, T.M.; Yadav, K. High level of awareness but poor practices regarding dengue fever control: A cross-sectional study from north India. N. Am. J. Med. Sci. 2012, 4, 278–282. [Google Scholar] [CrossRef] [PubMed]
- Lai, S.; Huang, Z.; Zhou, H.; Anders, K.L.; Perkins, T.A.; Yin, W.; Li, Y.; Mu, D.; Chen, Q.; Zhang, Z.; et al. The changing epidemiology of dengue in China, 1990–2014: A descriptive analysis of 25 years of nationwide surveillance data. BMC Med. Central 2015, 13, 100. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Dengue: Guidelines for Diagnosis, Treatment, Prevention, and Control; Special Programme for Research and Training in Tropical Diseases, World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- World Health Organization (WHO). Global Strategy for Dengue Prevention and Control, 2012–2020. Available online: http://apps.who.int/iris/bitstream/10665/75303/1/9789241504034_eng.pdf?ua=1 (accessed on 16 March 2016).

{kind=link}
{kind=link}
| Variable | Controls No. (%) (n = 492) | Cases No. (%) (n = 165) | p-Value | |
|---|---|---|---|---|
| Gender (male) | 222 (45.4) | 73 (44.2) | 0.796 | |
| Age (year) | Mean (SD) | 39.20 (15.01) | 37.87 (14.93) | 0.643 |
| Median (Min.–Max.) | 36 (13–70) | 37 (12–69) | 0.367 | |
| Migrant person | 181 (36.8) | 54 (32.7) | 0.346 | |
| Occupation | <0.001 | |||
| Farmer | 15 (3.2) | 8 (5.5) | ||
| Merchant | 62 (13.2) | 29 (19.9) | ||
| Office worker | 100 (21.4) | 25 (17.1) | ||
| Laborer | 22 (4.7) | 23 (15.8) | ||
| Unemployed | 118 (25.2) | 20 (13.7) | ||
| Retiree | 102 (21.8) | 24 (16.4) | ||
| Pupils/student | 49 (10.5) | 17 (11.6) | ||
| Severe mosquito bites | 157 (38.9) | 83 (51.2) | 0.007 | |
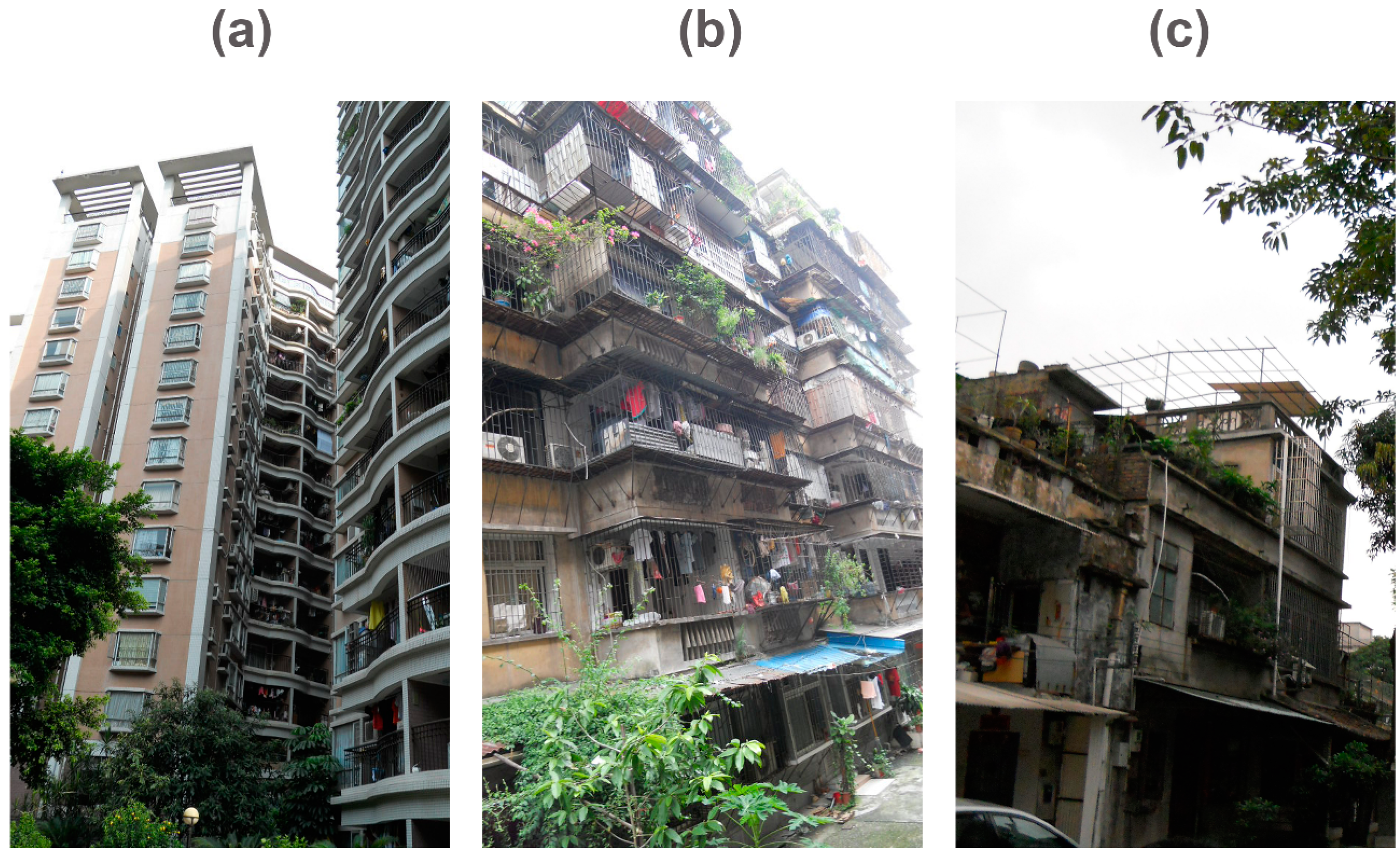
| Living in old flats/sheds | 308 (63.0) | 129 (80.1) | <0.001 | |
| Lacking air conditioner | 187 (38.0) | 47 (56.0) | 0.002 | |
| Plants with water containers | ||||
| Lucky bamboo plant | 163 (40.4) | 30 (18.6) | 0.000 | |
| Frequently change water | 95 (58.3) | 6 (35.3) | 0.069 | |
| Awareness of Dengue | 381 (77.4) | 99 (60.0) | 0.000 | |
| Preventive Measures | ||||
| Repellent | 137 (34.1) | 40 (24.2) | 0.022 | |
| Coil | 140 (34.7) | 101 (61.2) | <0.001 | |
| Net | 126 (31.3) | 88 (53.3) | <0.001 | |
| Screen | 114 (28.3) | 30 (18.2) | 0.012 | |
| Spray | 32 (7.9) | 15 (9.1) | 0.651 | |
| Clothes | 13 (3.2) | 7 (4.2) | 0.554 | |
| Cleaning trash/water | 115 (28.5) | 15 (9.1) | <0.001 | |
| Variables | B | S.E | p Value | Odds Ratio(OR) | 95% CI |
|---|---|---|---|---|---|
| Awareness of Dengue | −2.538 | 0.401 | <0.001 | 0.08 | 0.04–0.17 |
| Living in old apartment | 0.866 | 0.358 | 0.015 | 2.38 | 1.18–4.79 |
| Plants with water containers | −0.853 | 0.363 | 0.019 | 0.43 | 0.21–0.87 |
| Preventive Measures | |||||
| Repellent | −1.033 | 0.418 | 0.013 | 0.36 | 0.16–0.81 |
| Nets | 1.069 | 0.322 | 0.001 | 2.91 | 1.55–5.48 |
| Cleaning trash/water | −3.901 | 1.101 | <0.001 | 0.02 | 0.00–0.17 |
| Coils | 0.978 | 0.318 | 0.002 | 2.66 | 1.43–4.96 |
| Constant intercept | −0.285 | 0.435 | 0.512 | 0.75 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, B.; Yang, J.; Luo, L.; Yang, Z.; Liu, Q. Who Is Vulnerable to Dengue Fever? A Community Survey of the 2014 Outbreak in Guangzhou, China. Int. J. Environ. Res. Public Health 2016, 13, 712. https://doi.org/10.3390/ijerph13070712
Chen B, Yang J, Luo L, Yang Z, Liu Q. Who Is Vulnerable to Dengue Fever? A Community Survey of the 2014 Outbreak in Guangzhou, China. International Journal of Environmental Research and Public Health. 2016; 13(7):712. https://doi.org/10.3390/ijerph13070712
Chicago/Turabian StyleChen, Bin, Jun Yang, Lei Luo, Zhicong Yang, and Qiyong Liu. 2016. "Who Is Vulnerable to Dengue Fever? A Community Survey of the 2014 Outbreak in Guangzhou, China" International Journal of Environmental Research and Public Health 13, no. 7: 712. https://doi.org/10.3390/ijerph13070712
APA StyleChen, B., Yang, J., Luo, L., Yang, Z., & Liu, Q. (2016). Who Is Vulnerable to Dengue Fever? A Community Survey of the 2014 Outbreak in Guangzhou, China. International Journal of Environmental Research and Public Health, 13(7), 712. https://doi.org/10.3390/ijerph13070712