
Patterns of Smoking and Snus Use in Sweden: Implications for Public Health


Abstract
:1. Introduction
- Is primary uptake of snus associated with increased or decreased uptake of smoking as compared to those who have never been regular snus users?
- How does smokers’ uptake of snus use influence continuation or cessation of tobacco use? In particular, is snus use, particularly secondary use (to smoking), associated with increased or reduced success in smoking cessation?
- Have the relationships between the two products changed over time?
- How commonly is snus used as a cessation aid compared to other options, and how does it compare in terms of success rates?
2. Methods
2.1. Data Source
2.2. Sample
2.3. Survey Procedures
2.4. Measures
2.5. Data Processing
2.6. Ethical Considerations
3. Results
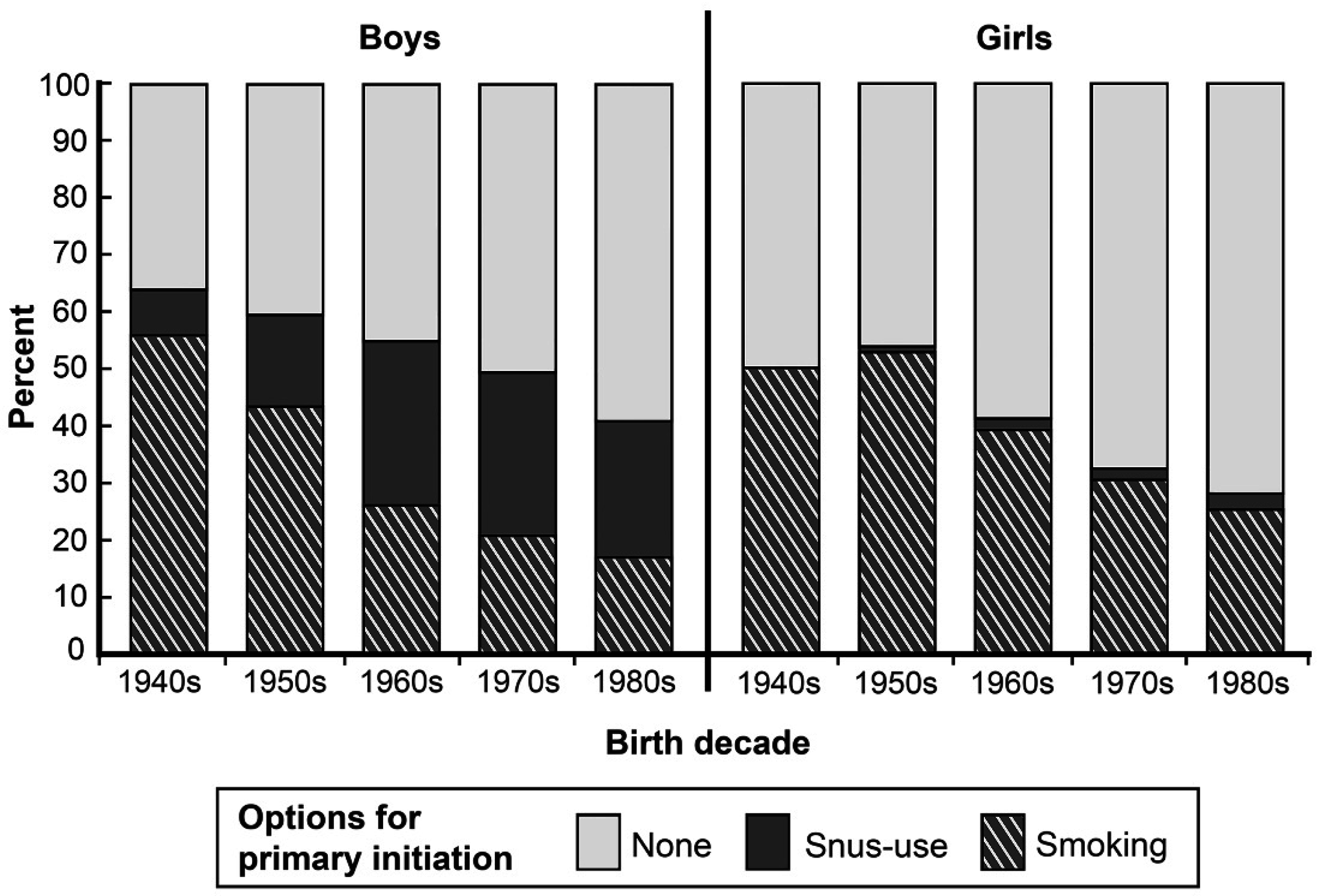
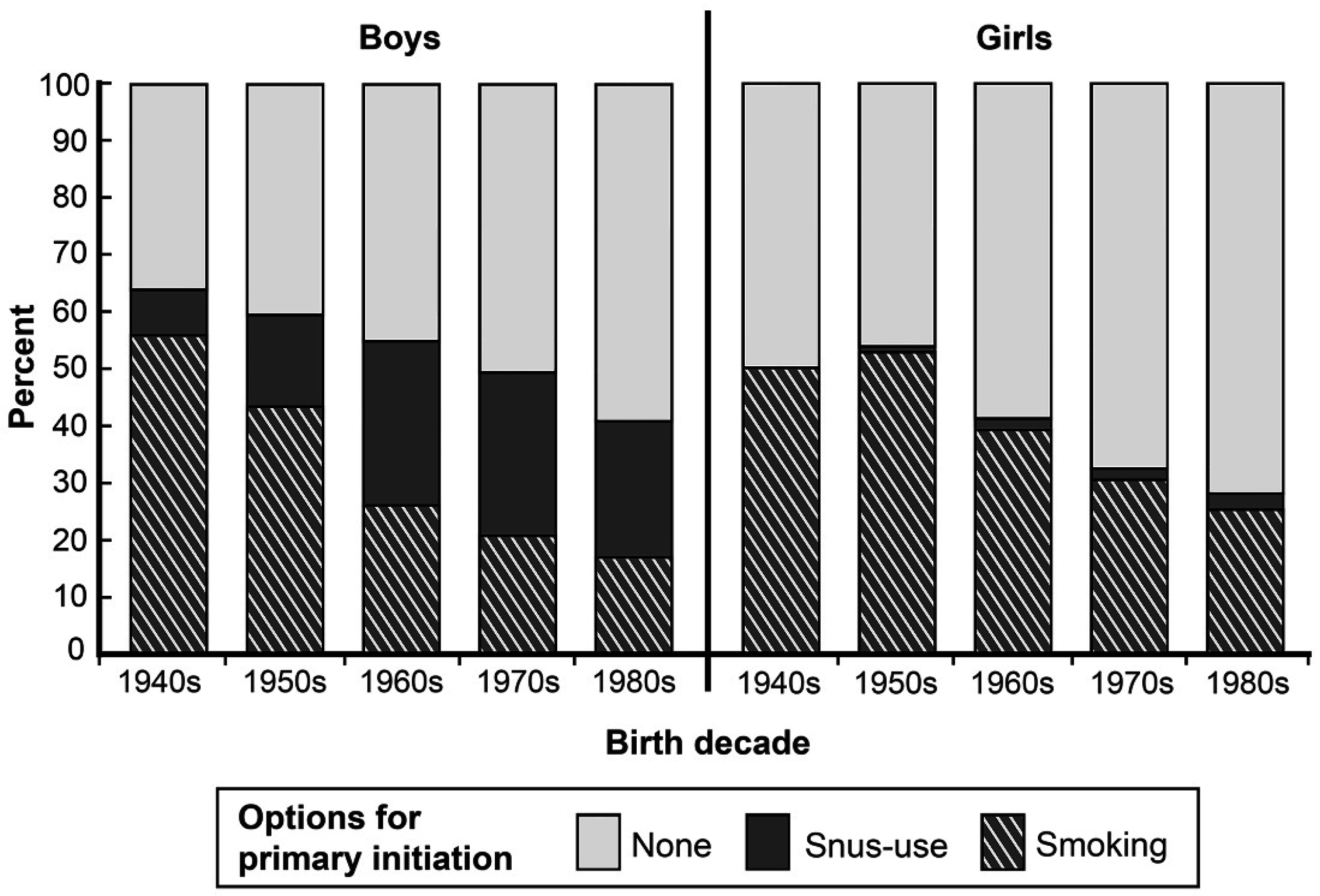
3.1. Primary Initiation of Tobacco Use According to Changes over Time in the Population
3.2. Initiation of Daily Smoking According to Primary Daily Snus Use
3.3. Quitting Smoking According to Uptake of Daily Snus Use
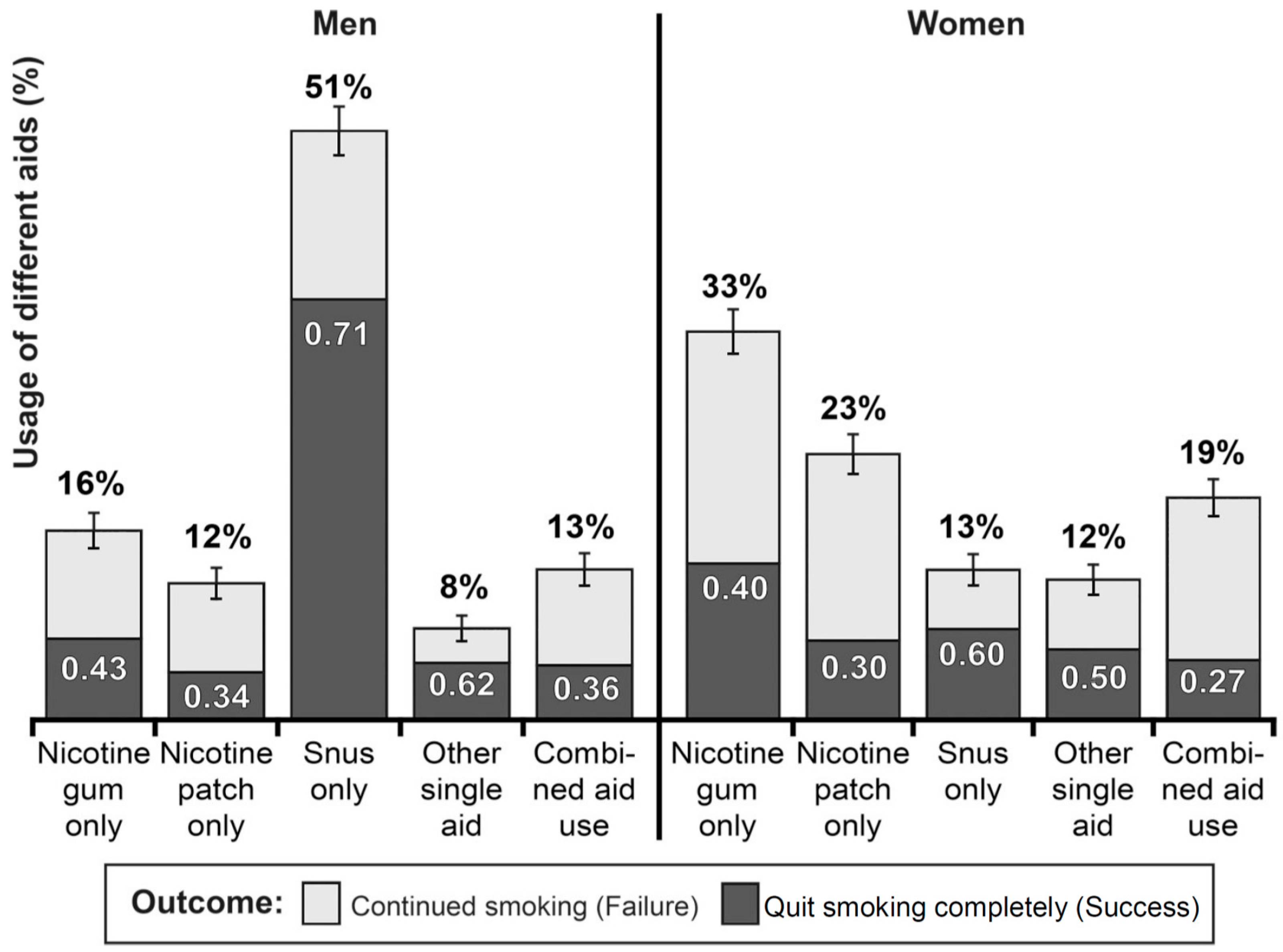
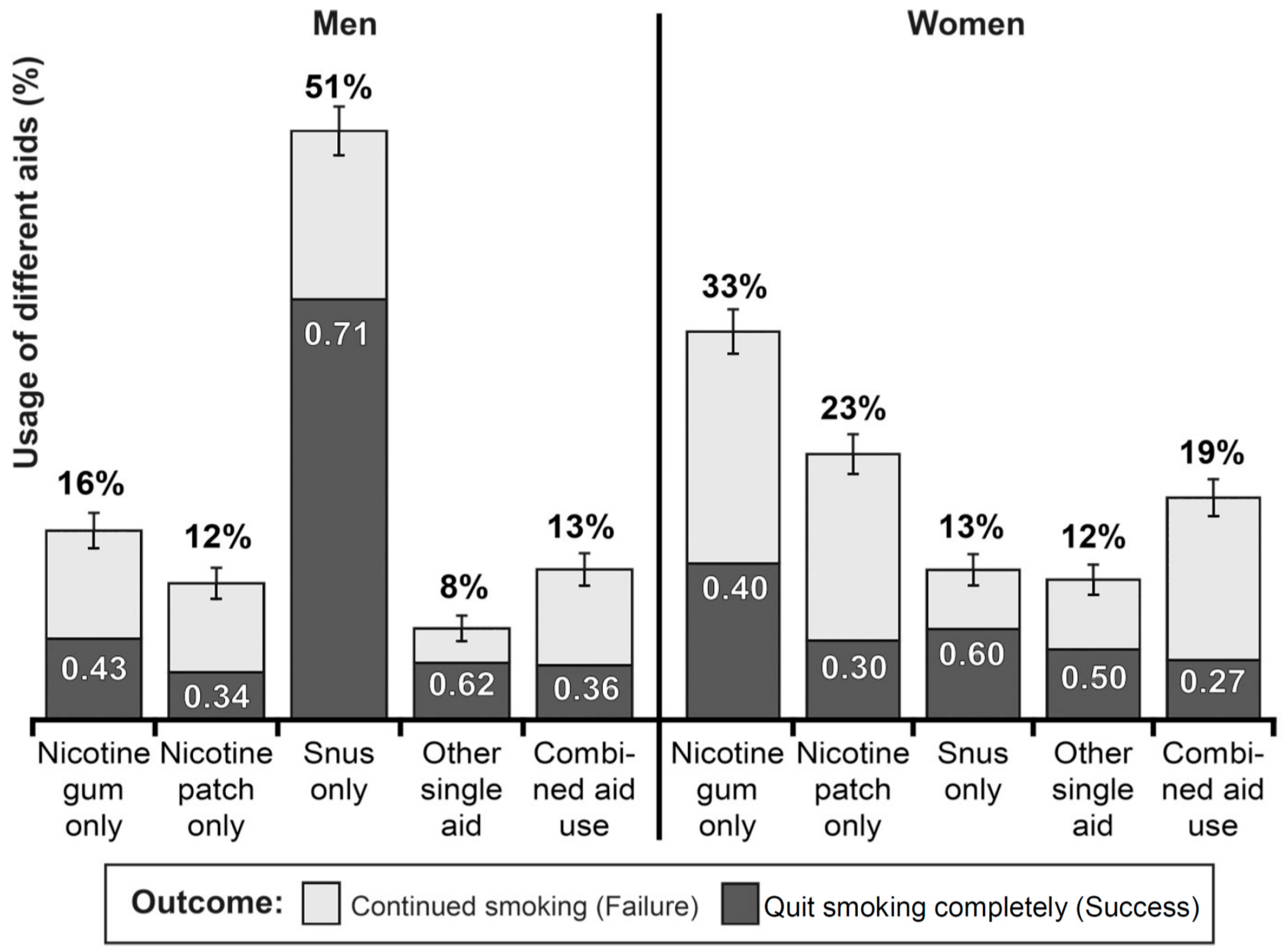
3.4. Self-Treatment Smoking Cessation: Different Cessation Aids and Their Effectiveness
4. Discussion
4.1. Role of Snus in Initiation of Tobacco Use
4.2. Role of Snus Use in Cessation of Smoking
4.3. Implications for Other Harm-Reduced Products
5. Limitations
6. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- The World Bank. Curbing the epidemic: Governments and the economics of tobacco control. Tob. Control 1999, 8, 196–201. [Google Scholar]
- Royal College of Physicians. Harm Reduction in Nicotine Addiction. Helping People Who Can’t Quit; The Tobacco Advisory Group of the Royal College of Physicians: London, UK, 2007; Available online: https://cdn.shopify.com/s/files/1/0924/4392/files/harm-reduction-nicotine-addiction.pdf?15599436013786148553 (accessed on 12 September 2016).
- Pateman, K.; Ford, P.; Fizgerald, L.; Mutch, A.; Yuke, K.; Bonevski, B.; Gartner, C. Stuck in the catch 22: Attitudes towards smoking cessation among populations vulnerable to social disadvantage. Addiction 2016, 111, 1048–1056. [Google Scholar] [CrossRef] [PubMed]
- Le Houezec, J.; McNeill, A.; Britton, J. Tobacco, nicotine and harm reduction. Drug Alcohol Rev. 2011, 30, 119–123. [Google Scholar] [CrossRef] [PubMed]
- Levy, D.T.; Mumford, E.A.; Cummings, K.M.; Gilpin, E.A.; Giovino, G.; Hyland, A.; Sweanor, D.; Warner, K.E. The relative risks of a low-nitrosamine smokeless tobacco product compared with smoking cigarettes: Estimates of a panel of experts. Cancer Epidemiol. Biomark. Prev. 2004, 13, 2035–2042. [Google Scholar]
- Lee, P.N. The effect on health of switching from cigarettes to snus—A review. Regul. Toxicol. Pharmacol. 2013, 66, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Hansson, J.; Galanti, M.R.; Hergens, M.P.; Fredlund, P.; Ahlbom, A.; Alfredsson, L.; Bellocco, R.; Eriksson, M.; Hallqvist, J.; Hedblad, B.; et al. Use of snus and acute myocardial infarction: Pooled analysis of eight prospective observational studies. Eur. J. Epidemiol. 2012, 27, 771–779. [Google Scholar] [CrossRef] [PubMed]
- Arefalk, G.; Hambraeus, K.; Lind, L.; Michaëlsson, K.; Lindahl, B.; Sundström, J. Discontinuation of smokeless tobacco and mortality risk after myocardial infarction. Circulation 2014, 130, 325–332. [Google Scholar] [CrossRef] [PubMed]
- Lewin, F.; Norell, S.E.; Johansson, H.; Gustavsson, P.; Wennerberg, J.; Björklund, A.; Rutqvist, L.E. Smoking tobacco, oral snuff, and alcohol in the etiology of squamous cell carcinoma of the head and neck: A population-based case-referent study in Sweden. Cancer 1998, 82, 1367–1375. [Google Scholar] [CrossRef]
- Bertuccio, P.; La Vecchia, C.; Silverman, D.T.; Petersen, G.M.; Bracci, P.M.; Negri, E.; Li, D.; Risch, H.A.; Olson, S.H.; Gallinger, S.; et al. Cigar and pipe smoking, smokeless tobacco use and pancreatic cancer: An analysis from the International Pancreatic Cancer Case-Control Consortium (PanC4). Ann. Oncol. 2011, 22, 1420–1426. [Google Scholar] [CrossRef] [PubMed]
- Khan, Z.; Tönnies, J.; Müller, S. Smokeless tobacco and oral cancer in South Asia: A systematic review with meta-analysis. J. Cancer Epidemiol. 2014, 2014, 394696. [Google Scholar] [CrossRef] [PubMed]
- Royal College of Physicians. Ending Tobacco Smoking in Britain. Radical Strategies for Prevention and Harm Reduction in Nicotine Addiction; The Tobacco Advisory Group of the Royal College of Physicians: London, UK, 2008; ISBN 978-1-86016-345-6. Available online: https://cdn.shopify.com/s/files/1/0924/4392/files/ending-tobacco-smoking.pdf?2801907981964551469 (accessed on 12 September 2016).
- Rhodes, T.; Hedrich, D. (Eds.) Harm reduction: Evidence, Impacts and Challenges. In EMCDDA Scientific Monograph Series No 10; Publications Office of the European Union: Luxembourg, 2010; Available online: http://www.emcdda.europa.eu/attachements.cfm/att_101257_EN_EMCDDAmonograph10-harm%20reduction_final.pdf (accessed on 12 September 2016). [CrossRef]
- Scientific Committee on Emerging and Newly Identified Health Risks. Health Effects of Smokeless Tobacco Products; European Commission: Brussels, Belgium, 2008; Available online: http://ec.europa.eu/health/ph_risk/committees/04_scenihr/docs/scenihr_o_013.pdf (accessed on 12 September 2016).
- Gartner, C.E.; Hall, W.H.; Vos, T.H.; Bertram, M.Y.; Wallace, A.L.; Lim, S.S. Assessment of Swedish snus for tobacco harm reduction: An epidemiological modelling study. Lancet 2007, 369, 2010–2014. [Google Scholar] [CrossRef]
- Mejia, A.B.; Ling, P.M. Tobacco industry consumer research on smokeless tobacco users and product development. Am. J. Public Health 2010, 100, 78–87. [Google Scholar] [CrossRef] [PubMed]
- Wetter, D.W.; McClure, J.B.; de Moor, C.; Cofta-Gunn, L.; Cummings, S.; Cinciripini, P.M.; Gritz, E.R. Concomitant use of cigarettes and smokeless tobacco: Prevalence, correlates, and predictors of tobacco cessation. Prev. Med. 2002, 34, 638–648. [Google Scholar] [CrossRef] [PubMed]
- Tomar, S.L.; Fox, B.J.; Severson, H.H. Is Smokeless Tobacco Use an Appropriate Public Health strategy for reducing societal harm from cigarette smoking? Int. J. Environ. Res. Public Health 2009, 6, 10–24. [Google Scholar] [CrossRef] [PubMed]
- Statistiska Centralbyrån. The Central Bureau of Statistics. Smoking Habits in Sweden. A Mail Survey-Spring 1963; Survey Research Center: Stockholm, Sweden, 1965. [Google Scholar]
- Public Health Agency of Sweden. The National Survey of Public Health: Tobacco. Available online: https://www.folkhalsomyndigheten.se/folkhalsorapportering-statistik/statistikdatabaser-och-visualisering/nationella-folkhalsoenkaten/resultat-a-o/ (accessed on 12 September 2016).
- European Commission. Attitudes of Europeans towards Tobacco and Electronic Cigarettes; European Commission: Brussels, Belgium, 2015; Special Eurobarometer 429. [Google Scholar]
- Lund, I.; Lund, K.E. How has the availability of snus influenced cigarette smoking in Norway? Int. J. Environ. Res. Public Health 2014, 11, 11705–11717. [Google Scholar] [CrossRef] [PubMed]
- Larsen, E.; Rise, J.; Lund, K.E. The relationship between snus use and smoking cognitions. Addict. Res. Theory 2012, 20, 447–455. [Google Scholar] [CrossRef] [PubMed]
- Borland, R.; Gartner, C. Rethinking therapeutic and recreational nicotine products: A commentary on Hatsukami et al. Tob. Control 2016, 25, 245. [Google Scholar] [CrossRef] [PubMed]
- Svensk författningssamling. Lag (2003:460) om Etikprövning av Forskning som Avser Människor. [Swedish Statute Book. The Act (2003:460) Regarding Ethical Review of Research Involving Humans]. Utbildningsdepartementet. Stockholm. Sweden. 2003. Available online: https://www.riksdagen.se/sv/Dokument-Lagar/Lagar/Svenskforfattningssamling/Lag-2003460-om-etikprovning_sfs-2003-460/ (accessed on 12 September 2016).
- Furberg, H.; Bulik, C.M.; Lerman, C.; Lichtenstein, P.; Pedersen, N.L.; Sullivan, P.F. Is Swedish snus associated with smoking initiation or smoking cessation? Tob. Control 2005, 14, 422–424. [Google Scholar] [CrossRef] [PubMed]
- Galanti, M.R.; Rosendahl, I.; Wickholm, S. The development of tobacco use in adolescence among “snus starters” and “cigarette starters”. An analysis of the Swedish “BROMS” cohort. Nicotine Tob. Res. 2008, 10, 315–323. [Google Scholar] [CrossRef] [PubMed]
- Gilljam, H.; Galanti, M.R. Role of snus (oral moist snuff) in smoking cessation and smoking reduction in Sweden. Addiction 2003, 98, 1183–1189. [Google Scholar] [CrossRef] [PubMed]
- Kozlowski, L.T.; O’Connor, R.J.; Edwards, B.Q.; Flaherty, B.P. Most smokeless tobacco use is not a causal gateway to cigarettes: Using order of product use to evaluate causation in a national US sample. Addiction 2003, 98, 1077–1085. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, R.J.; Kozlowski, L.T.; Flaherty, B.P.; Quinio, B.; Edwards, B.Q. Most smokeless tobacco use does not cause cigarette smoking: Results from the 2000 National Household Survey on Drug Abuse. Addict. Behav. 2005, 30, 325–336. [Google Scholar] [CrossRef] [PubMed]
- Ramström, L.M.; Foulds, J. Role of snus in initiation and cessation of tobacco smoking in Sweden. Tob. Control 2006, 15, 210–214. [Google Scholar] [CrossRef] [PubMed]
- Rodu, B.; Stegmayr, B.; Nasic, S.; Cole, P.; Asplund, K. Evolving patterns of tobacco use in northern Sweden. J. Intern. Med. 2003, 253, 660–665. [Google Scholar] [CrossRef] [PubMed]
- Fagerström, K.; Eissenberg, T. Dependence on Tobacco and Nicotine Products: A Case for Product-Speciefic Assessment. Nicotine Tob. Res. 2012, 14, 1382–1390. [Google Scholar] [CrossRef] [PubMed]
- Lund, E.K.; Scheffels, J.; McNeill, A. The association between use of snus and quit rates for smoking: Results from seven Norwegian cross-sectional studies. Addiction 2011, 106, 162–167. [Google Scholar] [CrossRef] [PubMed]
- Ramström, L.M.; Wikmans, T. Dual Use after Uptake of Snus among Daily Smokers: How Does It Influence the Conditions for Subsequent Cessation of Smoking? Presentation at 13th Annual Meeting of the SRNT Europe. Antalya, Turkey. 2011. Available online: http://www.tobaccofindings.org/wp-content/uploads/2012/03/Ramstrom_Wikmans_Turkiet.pdf (accessed on 12 September 2016).
- Wikmans, T.; Ramström, L. Harm perception among Swedish daily smokers regarding nicotine, NRT-products and Swedish Snus. Tob. Induc. Dis. 2010, 8, 9. [Google Scholar] [CrossRef] [PubMed]
- Britton, J. Progress with the global tobacco epidemic. Lancet 2015, 385, 924–926. [Google Scholar] [CrossRef]
- Royal College of Physicians. Nicotine without Smoke: Tobacco Harm Reduction; The Tobacco Advisory Group of the Royal College of Physicians: London, UK, 2016; Available online: file:///C:/Users/tobaksstudier/Downloads/Nicotine%20without%20smoke_0.pdf (accessed on 12 September 2016).
- Ramström, L.M.; Wikmans, T. Mortality attributable to tobacco among men in Sweden and other European countries: An analysis of data in a WHO report. Tob. Induc. Dis. 2014, 12, 14. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Global Report: Mortality Attributable to Tobacco; WHO: Geneva, Switzerland, 2012; ISBN 978-92-4156443-4. [Google Scholar]

{kind=link}
{kind=link}
| Profile of Initiation | |||||||
|---|---|---|---|---|---|---|---|
| Tobacco use | Primary daily smoking | Primary daily snus use | No daily | ||||
| at the time of the survey | no daily | secondary | no daily | secondary | tobacco | ||
| snus use | daily snus use | smoking | daily smoking | use | Total | ||
| Men | n = 6943 | n = 3737 | n = 4144 | n = 877 | n = 12,601 | n = 28,302 | |
| Daily smoking (combined with) | |||||||
| daily snus use | (a) | – | 9.0% n = 337 | – | 15.9% n = 139 | – | 1.7% n = 476 |
| occasional snus use | (b) | 3.9% n = 273 | 0.9% n = 33 | – | 2.0% n = 18 | – | 1.1% n = 324 |
| no snus use | (c) | 36.3% n = 2517 | 3.2% n = 120 | – | 6.0% n = 53 | – | 9.5% n = 2690 |
| Occasional smoking (combined with) | |||||||
| daily snus use | (d) | – | 8.4% n = 315 | 10.7% n = 443 | 10.3% n = 90 | – | 3.0% n = 848 |
| occasional snus use | (e) | 0.5% n = 31 | 0.6% n = 22 | 0.7% n = 29 | 0.8% n = 7 | 0.7% n = 83 | 0.6% n = 172 |
| no snus use | (f) | 4.1% n = 283 | 1.6% n = 59 | 2.1% n = 85 | 2.5% n = 22 | 3.7% n = 468 | 3.2% n = 917 |
| Quit daily smoking, now occasional smoking (sum of d +e + f) | 4.6% n = 314 | 10.6% n = 396 | N/A | 13.6% n = 119 | N/A | 2.9% n = 829 | |
| No smoking (combined with) | |||||||
| daily snus use | (g) | – | 43.8% n = 1636 | 58.4% n = 2421 | 37.3% n = 327 | – | 15.5% n = 4384 |
| occasional snus use | (h) | 1.0% n = 71 | 1.0% n = 37 | 3.5% n = 145 | 0.9% n = 8 | 1.7% n = 216 | 1.7% n = 477 |
| no snus use (tobacco free) | (i) | 54.3% n = 3768 | 31.5% n = 1178 | 24.6% n = 1021 | 24.3% n = 213 | 93.9% n = 11,834 | 63.7% n = 18,014 |
| Quit daily smoking, now completely | 55.3% n = 3839 | 76.3% n = 2851 | N/A | 62.5% n = 548 | N/A | 25.6% n = 7238 | |
| smoke free (sum of g + h + i) | |||||||
| Total (a − i) | 100% | 100% | 100% | 100% | 100% | 100% | |
| Women | n = 11,794 | n = 961 | n = 484 | n = 43 | n = 19,091 | n = 32,373 | |
| Daily smoking (combined with) | |||||||
| daily snus use | (j) | – | 7.3% n = 70 | – | 7.0% n = 3 | – | 0.2% n = 73 |
| occasional snus use | (k) | 1.6% n = 183 | 1.8% n = 17 | – | 11.6% n = 5 | – | 0.6% n = 205 |
| no snus use | (l) | 38.2% n = 4511 | 4.4% n = 42 | – | 20.9% n = 9 | – | 14.1% n = 4562 |
| Occasional smoking (combined with) | |||||||
| daily snus use | (m) | – | 11.2% n = 108 | 11.8% n=57 | 11.6% n = 5 | – | 0.5% n = 170 |
| occasional snus use | (n) | 0.3% n = 38 | 1.4% n =1 4 | 1.4% n=7 | 2.3% n = 1 | 0.3% n = 58 | 0.4% n = 118 |
| no snus use | (o) | 6.3% n = 748 | 2.2% n = 22 | 2.3% n = 11 | 2.3% n = 1 | 4.5% n = 863 | 5.1% n = 1645 |
| Quit daily smoking, now occasional | 6.6% n = 786 | 14.8% n = 144 | N/A | 16.2% n = 7 | N/A | 2.9% n = 937 | |
| smoking (sum of m + n + o) | |||||||
| No smoking (combined with) | |||||||
| daily snus use | (p) | – | 41.3% n = 397 | 55.8% n = 270 | 27.9% n = 12 | – | 2.1% n = 679 |
| occasional snus use | (q) | 0.4% n=44 | 1.7% n = 16 | 4.5% n = 22 | 0.0% n = 0 | 0.6% n = 118 | 0.6% n = 200 |
| no snus use (tobacco free) | (r) | 53.2% n = 6270 | 28.6% n = 275 | 24.2% n = 117 | 16.3% n = 7 | 94.6% n = 18,052 | 76.4% n = 24,721 |
| Quit daily smoking, now completely | 53.6% n = 6314 | 71.6% n = 688 | N/A | 44.2% n = 19 | N/A | 21.7% n = 7021 | |
| smokefree (sum of p + q + r) | |||||||
| Total (j − r) | 100% | 100% | 100% | 100% | 100% | 100% | |
| Born in | Proportion of uptake of daily nicotine use that is primary smoking | Proportion of non-primary snus users becoming smokers | Proportion of primary snus users becoming smokers | Proportion of primary smokers who take up secondary daily snus use | Quit ratios (quitting smoking completely) | |
|---|---|---|---|---|---|---|
| Primary smokers without daily snus use | Primary smokers with daily snus use | |||||
| 1940s | 87.3% | 60.4% | 19.6% | 34% | 0.60 | 0.83 |
| 1950s | 73.4% | 53.8% | 22.8% | 40% | 0.48 | 0.77 |
| 1960s | 46.8% | 36.6% | 18.6% | 41% | 0.40 | 0.72 |
| 1970s | 42.5% | 28.7% | 13.5% | 45% | 0.31 | 0.66 |
| 1980s | 40.1% | 21.8% | 14.3% | 46% | 0.19 | 0.47 |
| Men | Women | |||
|---|---|---|---|---|
| QR | 95% CI | QR | 95% CI | |
| Never daily snus users (Men: n = 6943, Women: n = 11,794) | 0.55 | (0.54–0.56) | 0.54 | (0.53–0.55) |
| Secondary snus users (Men: n = 3737, Women: n = 961) | 0.76 | (0.75–0.77) | 0.72 | (0.69–0.75) |
| Secondary smokers (Men: n = 877, Women: n = 43) | 0.63 | (0.60–0.66) | 0.44 | (0.29–0.59) |
| All of any daily snus users (Men: n = 4614, Women: n = 1004) | 0.74 | (0.73–0.75) | 0.70 | (0.67–0.73) |
| All ever daily smokers (Men: n = 11,557, Women: n = 12,798) | 0.63 | (0.62–0.64) | 0.55 | (0.54–0.56) |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramström, L.; Borland, R.; Wikmans, T. Patterns of Smoking and Snus Use in Sweden: Implications for Public Health. Int. J. Environ. Res. Public Health 2016, 13, 1110. https://doi.org/10.3390/ijerph13111110
Ramström L, Borland R, Wikmans T. Patterns of Smoking and Snus Use in Sweden: Implications for Public Health. International Journal of Environmental Research and Public Health. 2016; 13(11):1110. https://doi.org/10.3390/ijerph13111110
Chicago/Turabian StyleRamström, Lars, Ron Borland, and Tom Wikmans. 2016. "Patterns of Smoking and Snus Use in Sweden: Implications for Public Health" International Journal of Environmental Research and Public Health 13, no. 11: 1110. https://doi.org/10.3390/ijerph13111110
APA StyleRamström, L., Borland, R., & Wikmans, T. (2016). Patterns of Smoking and Snus Use in Sweden: Implications for Public Health. International Journal of Environmental Research and Public Health, 13(11), 1110. https://doi.org/10.3390/ijerph13111110