
Effect of Personal Exposure to PM2.5 on Respiratory Health in a Mexican Panel of Patients with COPD

Abstract
:1. Introduction
2. Experimental Section
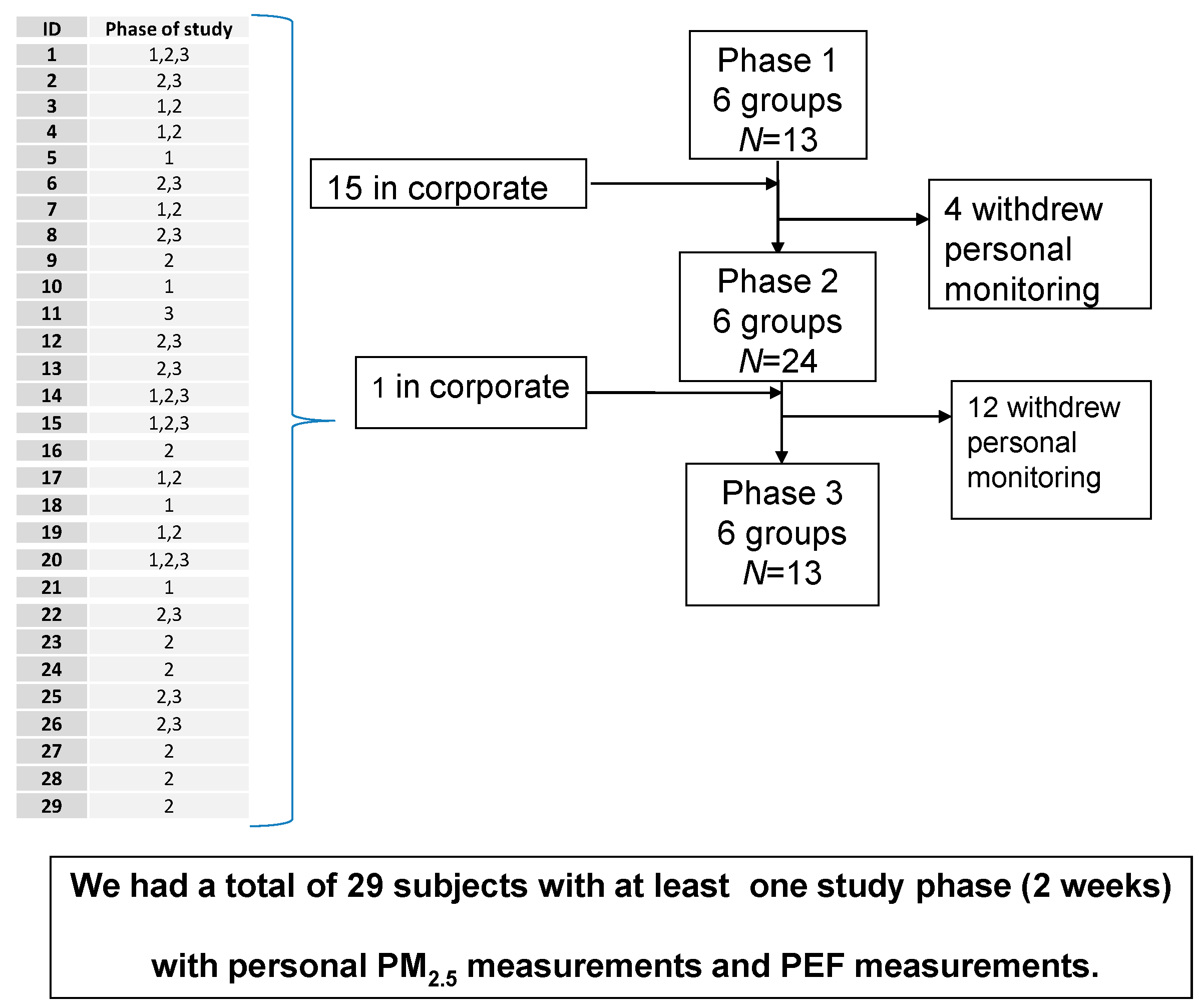
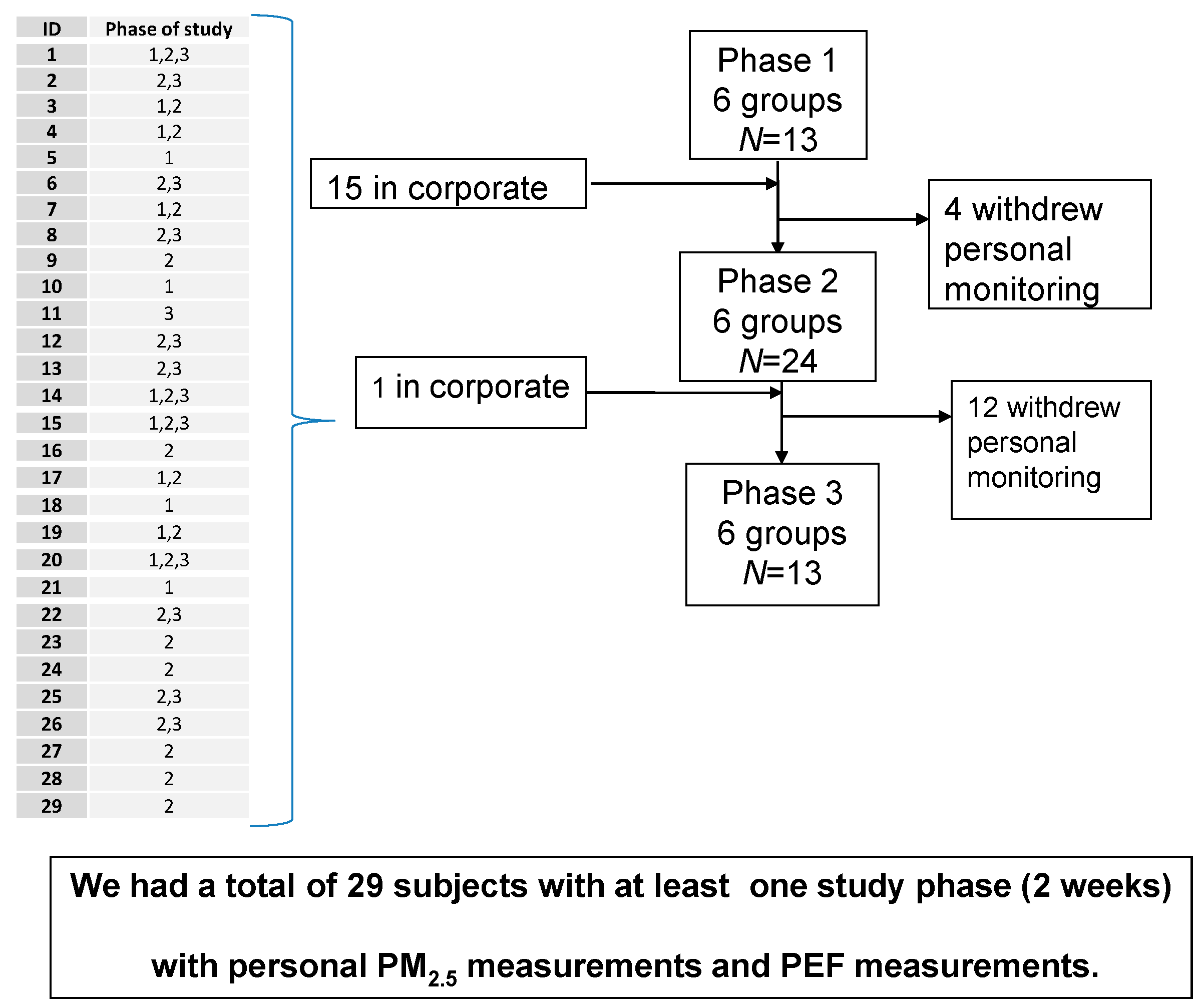
2.1. Participants
2.2. Statistical Analysis

{kind=link}
{kind=link}
{kind=link}
| Variables | Moderate | Severe | Very Severe | Total |
|---|---|---|---|---|
| Subjects, n | 7 | 13 | 9 | 29 |
| Male subjects n (%) | 3 (10) | 9 (31) | 8 (28) | 20 (69) |
| Mean age (years) (range) | 70 (63–76) | 71 (62–80) | 66 (43–72) | 69 (43–80) |
| FEV1 % PREDICTED * | 59 | 35 | 23 | 37 |
| Time indoors % (range) | 87 (57–100) | 90 (54–100) | 93 (38–100) | 90 (38–100) |
| PEF total n | 219 | 447 | 320 | 986 |
| Mean morning PEF (L/min ± SD) | 242. ± 116 | 186 ± 98 | 160 ± 73 | 189 ± 99 |
| Mean night PEF (L/min ± SD) | 267 ± 139 | 183 ± 95 | 153 ± 73 | 192 ± 105 |
| Mean PEF variability (%) | 25.0 | 24.3 | 17.9 | 22.4 |
| Frequency of medication use (%) † | 131 (84) | 340 (96) | 241 (96) | 712 (94) |
| PM2.5 personal total n | 80 | 163 | 122 | 365 |
| Mean and range of n measurements in individuals | 11 (7–16) | 13 (5–22) | 13 (7–20) | 12 (5–22) |
| Mean personal PM2.5 (µg/m3 ± SD) | 44 ± 25.4 | 36 ± 20 | 39 ± 21.9 | 39 ± 22.1 |
3. Results and Discussion
3.1. PEF, Symptoms, and Medication Frequency
| COPD | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Moderate | Severe | Very severe | Total | ||||||||||||
| n = 121 | n = 256 | n = 178 | n = 535 | ||||||||||||
| Symptom | No. | % | X (range) * | No. | % | X (range) * | No. | % | X (range) * | No. | % | X (range) * | |||
| Wheeze | 29 | 24 | 4 (0–9) | 100 | 39 | 8 (0–35) | 74 | 42 | 8 (0–27) | 203 | 37 | 7 (0–35) | |||
| Phlegm | 38 | 31 | 5 (0–21) | 109 | 43 | 8 (0–35) | 29 | 16 | 3 (0–12) | 176 | 32 | 6 (0–35) | |||
| Cough | 36 | 30 | 5 (0–18) | 102 | 40 | 8 (0–35) | 33 | 19 | 4 (0–12) | 171 | 31 | 6 (0–35) | |||
| Cold/influenza | 6 | 5 | 0.9 (0–5) | 9 | 4 | 0.7 (0–3) | 13 | 7 | 1 (0–7) | 28 | 5 | 1 (0–7) | |||
| Fever | 2 | 2 | 0.3 (0–2) | 1 | 0.4 | 0.1 (0–1) | 1 | 0.6 | 0.1 (0–1) | 4 | 0.7 | 0.1 (0–2) | |||
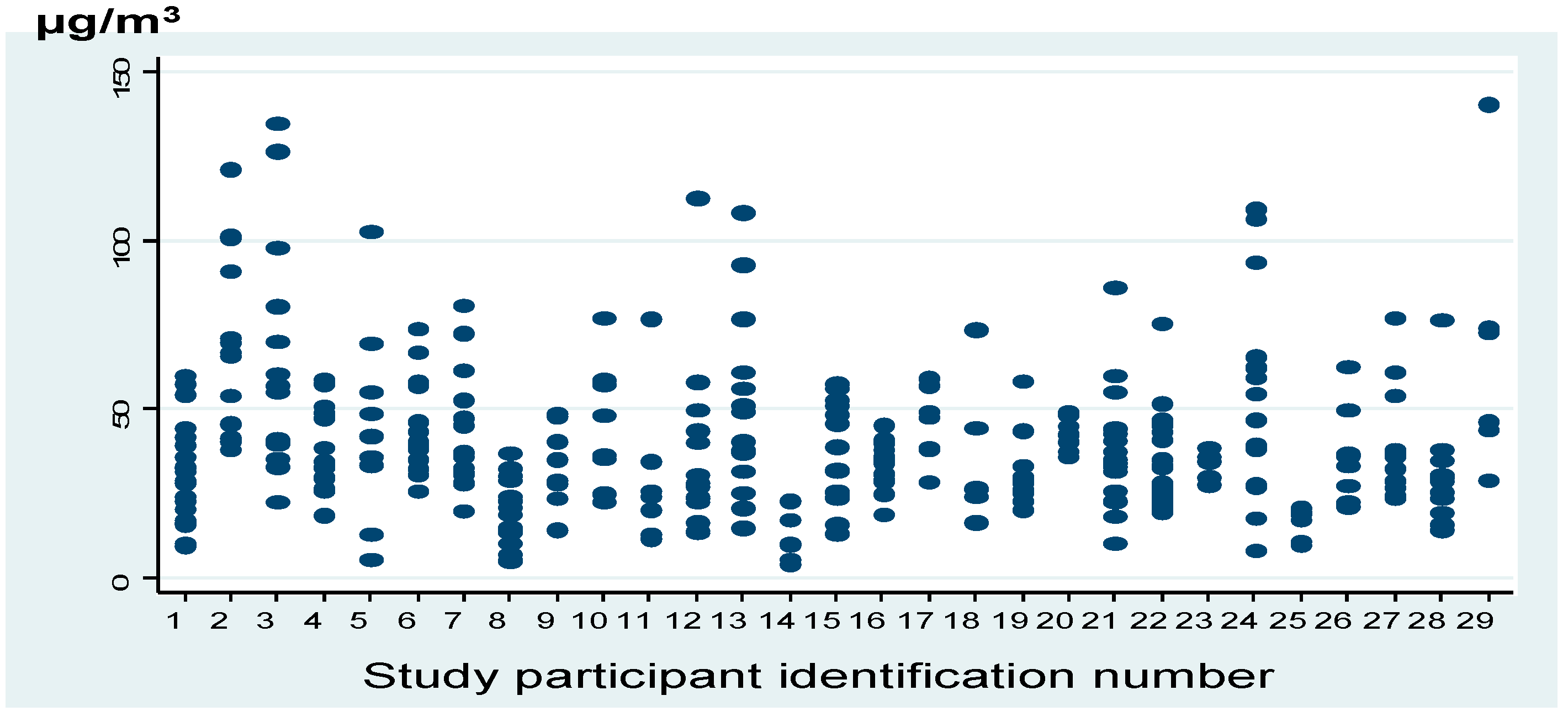
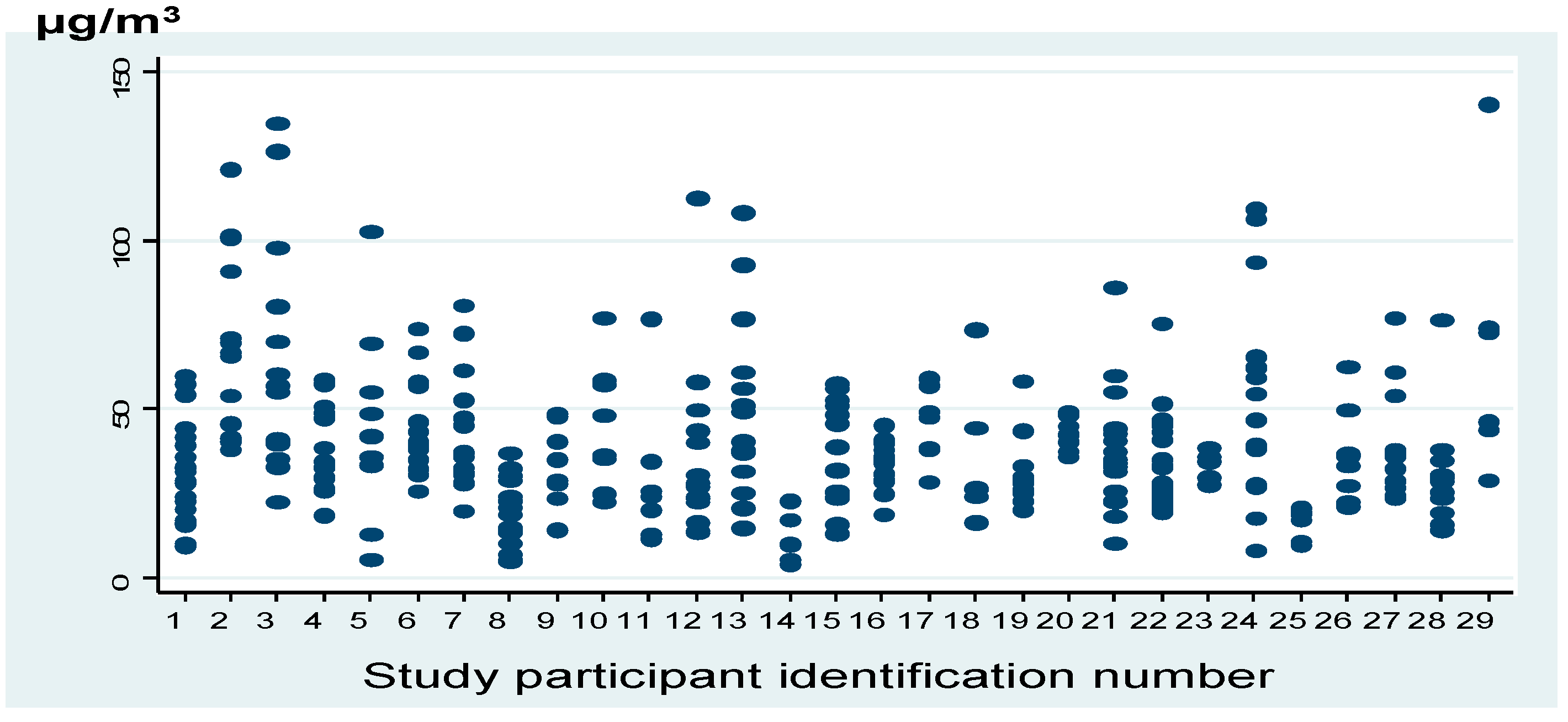
3.2. Personal Exposure to PM2.5
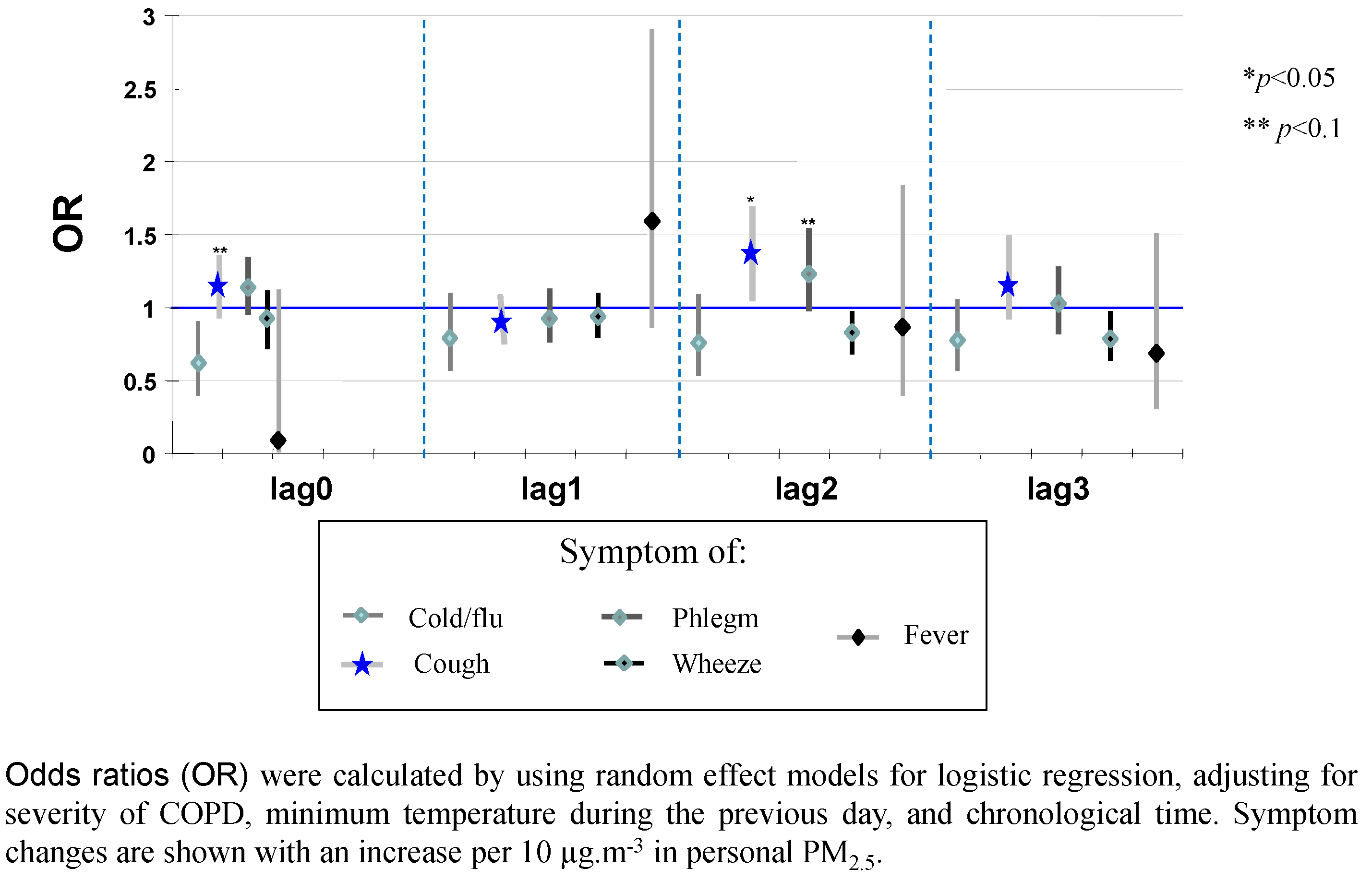
3.3. Personal PM2.5 Effects on Health Outcomes
| Personal PM2.5 | Change a Morning PEF L/min | 95% CI b | Change Night PEF L/min | 95% CI | PEF Varia-Bility (%) | 95% CI |
|---|---|---|---|---|---|---|
| Lag 0 | −0.71 | −2.2–0.77 | 0.008 | −2.1–2.1 | 0.4 | −0.5–1.3 |
| Lag 1 | 0.01 | −1.4–1.4 | 0.16 | −2.3–2.6 | 0.2 | −0.8–1.3 |
| Lag 2 | −1.4 | −2.8–−0.04 * | −3.0 | −5.7 to −0.3 * | 0.7 | −0.5 to 1.9 |
| Lag 3 | −1.2 | −2.9 to 0.43 | −3.6 | −6.5 to −0.7 * | 0.7 | −0.6 to 2.0 |
| Lag 4 | −1.2 | −3.1 to 0.67 | −0.9 | −4.3 to 2.5 | −0.4 | −1.8 to 1.0 |

4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Andersen, Z.J.; Wahlin, P.; Raaschou-Nielsen, O.; Scheike, T.; Loft, S. Ambient particle source apportionment and daily hospital admissions among children and elderly in Copenhagen. J. Expo. Sci. Environ. Epidemiol. 2007, 17, 625–636. [Google Scholar] [CrossRef] [PubMed]
- Bell, M.L.; Ebisu, K.; Leaderer, B.P.; Gent, J.F.; Lee, H.J.; Koutrakis, P.; Wang, Y.; Dominici, F.; Peng, R.D. Associations of PM2.5 constituents and sources with hospital admissions: Analysis of four counties in Connecticut and Massachusetts (USA) for persons ≥65 years of age. Environ. Health Perspect. 2014, 122, 138–144. [Google Scholar] [CrossRef] [PubMed]
- Colucci, M.E.; Veronesi, L.; Roveda, A.M.; Marangio, E.; Sansebastiano, G. Particulate matter (PM10) air pollution, daily mortality, and hospital admissions: Recent findings. Igiene e Sanità Pubblica 2006, 62, 289–304. [Google Scholar] [PubMed]
- Darrow, L.A.; Klein, M.; Flanders, W.D.; Mulholland, J.A.; Tolbert, P.E.; Strickland, M.J. Air pollution and acute respiratory infections among children 0–4 years of age: An 18-year time-series study. Am. J. Epidemiol. 2014, 180, 968–977. [Google Scholar] [CrossRef] [PubMed]
- Gent, J.F.; Koutrakis, P.; Belanger, K.; Triche, E.; Holford, T.R.; Bracken, M.B.; Leaderer, B.P. Symptoms and medication use in children with asthma and traffic-related sources of fine particle pollution. Environ. Health Perspect. 2009, 117, 1168–1174. [Google Scholar] [CrossRef] [PubMed]
- Halonen, J.I.; Lanki, T.; Yli-Tuomi, T.; Kulmala, M.; Tiittanen, P.; Pekkanen, J. Urban air pollution, and asthma and COPD hospital emergency room visits. Thorax 2008, 63, 635–641. [Google Scholar] [CrossRef] [PubMed]
- Lall, R.; Ito, K.; Thurston, G.D. Distributed lag analyses of daily hospital admissions and source-apportioned fine particle air pollution. Environ. Health Perspect. 2011, 119, 455–460. [Google Scholar] [CrossRef] [PubMed]
- Ostro, B.; Roth, L.; Malig, B.; Marty, M. The effects of fine particle components on respiratory hospital admissions in children. Environ. Health Perspect. 2009, 117, 475–480. [Google Scholar] [CrossRef] [PubMed]
- Peel, J.L.; Tolbert, P.E.; Klein, M.; Metzger, K.B.; Flanders, W.D.; Todd, K.; Mulholland, J.A.; Ryan, P.B.; Frumkin, H. Ambient air pollution and respiratory emergency department visits. Epidemiology 2005, 16, 164–174. [Google Scholar] [CrossRef] [PubMed]
- Rodopoulou, S.; Chalbot, M.C.; Samoli, E.; Dubois, D.W.; San Filippo, B.D.; Kavouras, I.G. Air pollution and hospital emergency room and admissions for cardiovascular and respiratory diseases in Doña Ana County, New Mexico. Environ. Res. 2014, 129, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Tramuto, F.; Cusimano, R.; Cerame, G.; Vultaggio, M.; Calamusa, G.; Maida, C.M.; Vitale, F. Urban air pollution and emergency room admissions for respiratory symptoms: A case-crossover study in Palermo, Italy. Environ. Health 2011, 10. [Google Scholar] [CrossRef] [PubMed]
- Winquist, A.; Klein, M.; Tolbert, P.; Flanders, W.D.; Hess, J.; Sarnat, S.E. Comparison of emergency department and hospital admissions data for air pollution time-series studies. Environ. Health 2012, 11. [Google Scholar] [CrossRef] [PubMed]
- Correia-Deur, J.E.; Claudio, L.; Imazawa, A.T.; Eluf-Neto, J. Variations in peak expiratory flow measurements associated to air pollution and allergic sensitization in children in Sao Paulo, Brazil. Am. J. Ind. Med. 2012, 55, 1087–1098. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, L.; Hacon, S.D.S.; Castro, H.A.; Ignotti, E.; Artaxo, P.; Ponce de León, A.C. Association between fine particulate matter and the peak expiratory flow of schoolchildren in the Brazilian subequatorial Amazon: A panel study. Environ. Res. 2012, 117, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.; MacNeill, M.; Grgicak-Mannion, A.; Nethery, E.; Xu, X.; Dales, R.; Rasmussen, P.; Wheeler, A. Development of temporally refined land-use regression models predicting daily household-level air pollution in a panel study of lung function among asthmatic children. J. Expo. Sci. Environ. Epidemiol. 2013, 23, 259–267. [Google Scholar] [CrossRef] [PubMed]
- Li, J.Y.; Ma, L.; Liu, L.Z.; Zhou, J.; He, M.Q.; Shima, M.; Tamura, K. The short-term effects of particulate matter on lung function of college students in autumn and winter in Wuhan. Zhonghua Yu Fang Yi Xue Za Zhi 2013, 47, 155–159. [Google Scholar] [PubMed]
- Odajima, H.; Yamazaki, S.; Nitta, H. Decline in peak expiratory flow according to hourly short-term concentration of particulate matter in asthmatic children. Inhal. Toxicol. 2008, 20, 1263–1272. [Google Scholar] [CrossRef] [PubMed]
- Tang, C.S.; Chang, L.T.; Lee, H.C.; Chan, C.C. Effects of personal particulate matter on peak expiratory flow rate of asthmatic children. Sci. Total Environ. 2007, 382, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Yamazaki, S.; Shima, M.; Ando, M.; Nitta, H.; Watanabe, H.; Nishimuta, T. Effect of hourly concentration of particulate matter on peak expiratory flow in hospitalized children: A panel study. Environ. Health 2011, 10. [Google Scholar] [CrossRef] [PubMed]
- Jie, Y.; Houjin, H.; Xun, M.; Kebin, L.; Xuesong, Y.; Jie, X. Relationship between pulmonary function and indoor air pollution from coal combustion among adult residents in an inner-city area of southwest China. Braz. J. Med. Biol. Res. 2014, 47, 982–989. [Google Scholar] [CrossRef] [PubMed]
- Mu, L.; Deng, F.; Tian, L.; Li, Y.; Swanson, M.; Ying, J.; Browne, R.W.; Rittenhouse-Olson, K.; Zhang, J.J.; Zhang, Z.F.; Bonner, M.R. Peak expiratory flow, breath rate and blood pressure in adults with changes in particulate matter air pollution during the Beijing Olympics: A panel study. Environ. Res. 2014, 133, 4–11. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Deng, F.; Hao, Y.; Wang, X.; Zheng, C.; Lv, H.; Lu, X.; Wei, H.; Huang, J.; Qin, Y.; Shima, M.; Guo, X. Fine particulate matter, temperature, and lung function in healthy adults: Findings from the HVNR study. Chemosphere 2014, 108, 68–74. [Google Scholar] [CrossRef] [PubMed]
- Yoda, Y.; Otani, N.; Sakurai, S.; Shima, M. Acute effects of summer air pollution on pulmonary function and airway inflammation in healthy young women. J. Epidemiol. 2014, 24, 312–320. [Google Scholar] [CrossRef] [PubMed]
- Islam, T.; Gauderman, W.J.; Berhane, K.; McConnell, R.; Avol, E.; Peters, J.M.; Gilliland, F.D. Relationship between air pollution, lung function and asthma in adolescents. Thorax 2007, 62, 957–963. [Google Scholar] [CrossRef] [PubMed]
- Qian, Z.; Lin, H.M.; Chinchilli, V.M.; Lehman, E.B.; Stewart, W.F.; Shah, N.; Duan, Y.; Craig, T.J.; Wilson, W.E.; Liao, D.; Lazarus, S.C.; Bascom, R. Associations between air pollution and peak expiratory flow among patients with persistent asthma. J. Toxicol. Environ. Health A. 2009, 72, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Hulin, M.; Simoni, M.; Viegi, G.; Annesi-Maesano, I. Respiratory health and indoor air pollutants based on quantitative exposure assessments. Eur. Respir. J. 2012, 40, 1033–1045. [Google Scholar] [CrossRef] [PubMed]
- Lagorio, S.; Forastiere, F.; Pistelli, R.; Iavarone, I.; Michelozzi, P.; Fano, V.; Marconi, A.; Ziemacki, G.; Ostro, B.D. Air pollution and lung function among susceptible adult subjects: A panel study. Environ. Health 2006, 5. [Google Scholar] [CrossRef] [PubMed]
- Trenga, C.A.; Sullivan, J.H.; Schildcrout, J.S.; Shepherd, K.P.; Shapiro, G.G.; Liu, L.J.; Kaufman, J.D.; Koenig, J.Q. Effect of particulate air pollution on lung function in adult and pediatric subjects in a Seattle panel study. Chest 2006, 129, 1614–1622. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Lee, K.; Pérez-Padilla, R.; Hudson, N.L.; Mannino, D.M. Outdoor and indoor air pollution and COPD-related diseases in high- and low-income countries. Int. J. Tuberc. Lung. Dis. 2008, 12, 115–127. [Google Scholar] [PubMed]
- Thomas, K.W.; Pellizzari, E.D.; Clayton, C.A.; Whitaker, D.A.; Shores, R.C.; Spengler, J.; Ozkaynak, H.; Froehlich, S.E.; Wallace, L.A. Particle Total Exposure Assessment Methodology (PTEAM) 1990 study: method performance and data quality for personal, indoor, and outdoor monitoring. J. Expo. Anal. Environ. Epidemiol. 1993, 3, 203–226. [Google Scholar] [PubMed]
- American Thoracic Society. Standardization of Spirometry, 1994 Update. Am. J. Respir. Crit. Care Med. 1994, 152, 1107–1136. [Google Scholar]
- Cortéz-Lugo, M.; Moreno-Macías, H.; Holguín-Molina, F.; Chow, J.C.; Watson, J.G.; Gutiérrez-Avedoy, V.; Mandujano, F.; Hernández-Ávila, M.; Romieu, I. Relationship between indoor, outdoor, and personal fine particle concentrations for individuals with COPD and predictors of indoor-outdoor ratio in Mexico City. J. Expo. Sci. Environ. Epidemiol. 2008, 18, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Ravani, P.; Barrett, B.J.; Parfrey, P.S. Longitudinal studies 3: Data modeling using standard regression models and extensions. Meth. Mol. Biol. 2015, 128, 93–131. [Google Scholar]
- Global Initiative for Obstructive Lung Disease Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary. Am. J. Respir. Crit. Care Med. 2001, 163, 1256–1276.
- Aivazis, V.; Hatzimichail, A.; Stavridis, J.; Bourli, E.; Konstantinidis, T.H.; Katsougiannopoulos, V. Growth and other factors affecting peak expiratory flow in Greek children. Minerva Pediat. 2005, 57, 83–89. [Google Scholar] [PubMed]
- Just, J.; Segala, C.; Sahraoui, F.; Priol, G.; Grimfeld, A.; Neukirch, F. Short-term health effects of particulate and photochemical air pollution in asthmatic children. Eur. Respir. J. 2002, 20, 899–906. [Google Scholar] [CrossRef] [PubMed]
- Franck, U.; Herbarth, O.; Röder, S.; Schlink, U.; Borte, M.; Díez, U.; Krämer, U.; Lehmann, I. Respiratory effects of indoor particles in young children are size dependent. Sci. Total Environ. 2011, 409, 1621–1631. [Google Scholar] [CrossRef] [PubMed]
- Jansen, K.L.; Larson, T.V.; Koenig, J.Q.; Mar, T.F.; Fields, C.; Stewart, J.; Lippmann, M. Associations between health effects and particulate matter and black carbon in subjects with respiratory disease. Environ. Health Perspect. 2005, 113, 1741–1746. [Google Scholar] [CrossRef] [PubMed]
- Osunsanya, T.; Prescott, G.; Seaton, A. Acute respiratory effects of particles: Mass or number? Occup. Environ. Med. 2001, 58, 154–159. [Google Scholar] [CrossRef] [PubMed]
- Delfino, R.J.; Quintana, P.J.; Floro, J.; Gastanaga, V.M.; Samimi, B.S.; Kleinman, M.T.; Liu, L.J.; Bufalino, C.; Wu, C.F.; McLaren, C.E. Association of FEV1 in asthmatic children with personal and microenvironmental exposure to airborne particulate matter. Environ. Health Perspect. 2004, 112, 932–941. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, L.S.; Hacon, S.D.S.; de Castro, H.A.; Ignotti, E.; Artaxo, P.; Saldiva, P.H.; de León, A.C. Acute effects of particulate matter and black carbon from seasonal fires on peak expiratory flow of schoolchildren in the Brazilian Amazon. PLoS ONE 2014, 9. [Google Scholar] [CrossRef]
- Abdel-Salam, M.M. Indoor particulate matter in urban residences of Alexandria, Egypt. J. Air Waste Manag. Assoc. 2013, 63, 956–962. [Google Scholar] [CrossRef] [PubMed]
- Rojas-Bracho, L.; Suh, H.H.; Catalano, P.J.; Koutrakis, P. Personal exposures to particles and their relationships with personal activities for chronic obstructive pulmonary disease patients living in Boston. J. Air Waste Manag. Assoc. 2004, 54, 207–217. [Google Scholar] [CrossRef] [PubMed]
- Tsai, S.S.; Chang, C.C.; Yang, C.Y. Fine particulate air pollution and hospital admissions for chronic obstructive pulmonary disease: A case-crossover study in Taipei. Int. J. Environ. Res. Public Health 2013, 10, 6015–6026. [Google Scholar] [CrossRef] [PubMed]
- Hu, G.; Zhong, N.; Ran, P. Air pollution and COPD in China. J. Thorac. Dis. 2015, 7, 59–66. [Google Scholar] [PubMed]
- Ko, F.W.; Hui, D.S. Outdoor air pollution: impact on chronic obstructive pulmonary disease patients. Curr. Opin. Pulm. Med. 2009, 15, 150–157. [Google Scholar] [CrossRef] [PubMed]
- Kunisaki, K.M.; Rice, K.L.; Janoff, E.N.; Rector, T.S.; Niewoehner, D.E. Exhaled nitric oxide, systemic inflammation, and the spirometric response to inhaled fluticasone propionate in severe chronic obstructive pulmonary disease: A prospective study. Ther. Adv. Respir. Dis. 2008, 2, 55–64. [Google Scholar] [CrossRef] [PubMed]
- MacNee, W. Pulmonary and systemic oxidant/antioxidant imbalance in chronic obstructive pulmonary disease. Proc. Am. Thorac. Soc. 2005, 2, 50–60. [Google Scholar] [CrossRef] [PubMed]
- Santos, M.C.; Oliveira, A.L.; Viegas-Crespo, A.M.; Vicente, L.; Barreiros, A.; Monteiro, P.; Pinheiro, T.; Bugalho De Almeida, A. Systemic markers of the redox balance in chronic obstructive pulmonary disease. Biomarkers 2004, 9, 461–469. [Google Scholar] [CrossRef] [PubMed]
- Viegi, G.; Maio, S.; Pistelli, F.; Baldacci, S.; Carrozzi, L. Epidemiology of chronic obstructive pulmonary disease: Health effects of air pollution. Respirology 2006, 11, 523–532. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cortez-Lugo, M.; Ramírez-Aguilar, M.; Pérez-Padilla, R.; Sansores-Martínez, R.; Ramírez-Venegas, A.; Barraza-Villarreal, A. Effect of Personal Exposure to PM2.5 on Respiratory Health in a Mexican Panel of Patients with COPD. Int. J. Environ. Res. Public Health 2015, 12, 10635-10647. https://doi.org/10.3390/ijerph120910635
Cortez-Lugo M, Ramírez-Aguilar M, Pérez-Padilla R, Sansores-Martínez R, Ramírez-Venegas A, Barraza-Villarreal A. Effect of Personal Exposure to PM2.5 on Respiratory Health in a Mexican Panel of Patients with COPD. International Journal of Environmental Research and Public Health. 2015; 12(9):10635-10647. https://doi.org/10.3390/ijerph120910635
Chicago/Turabian StyleCortez-Lugo, Marlene, Matiana Ramírez-Aguilar, Rogelio Pérez-Padilla, Raúl Sansores-Martínez, Alejandra Ramírez-Venegas, and Albino Barraza-Villarreal. 2015. "Effect of Personal Exposure to PM2.5 on Respiratory Health in a Mexican Panel of Patients with COPD" International Journal of Environmental Research and Public Health 12, no. 9: 10635-10647. https://doi.org/10.3390/ijerph120910635
APA StyleCortez-Lugo, M., Ramírez-Aguilar, M., Pérez-Padilla, R., Sansores-Martínez, R., Ramírez-Venegas, A., & Barraza-Villarreal, A. (2015). Effect of Personal Exposure to PM2.5 on Respiratory Health in a Mexican Panel of Patients with COPD. International Journal of Environmental Research and Public Health, 12(9), 10635-10647. https://doi.org/10.3390/ijerph120910635