
A Meta-Analysis of Cigarette Smoking Prevalence among Adolescents in China: 1981–2010


Abstract
:1. Introduction
2. Methods
2.1. Literature Search
2.2. Inclusion Criteria
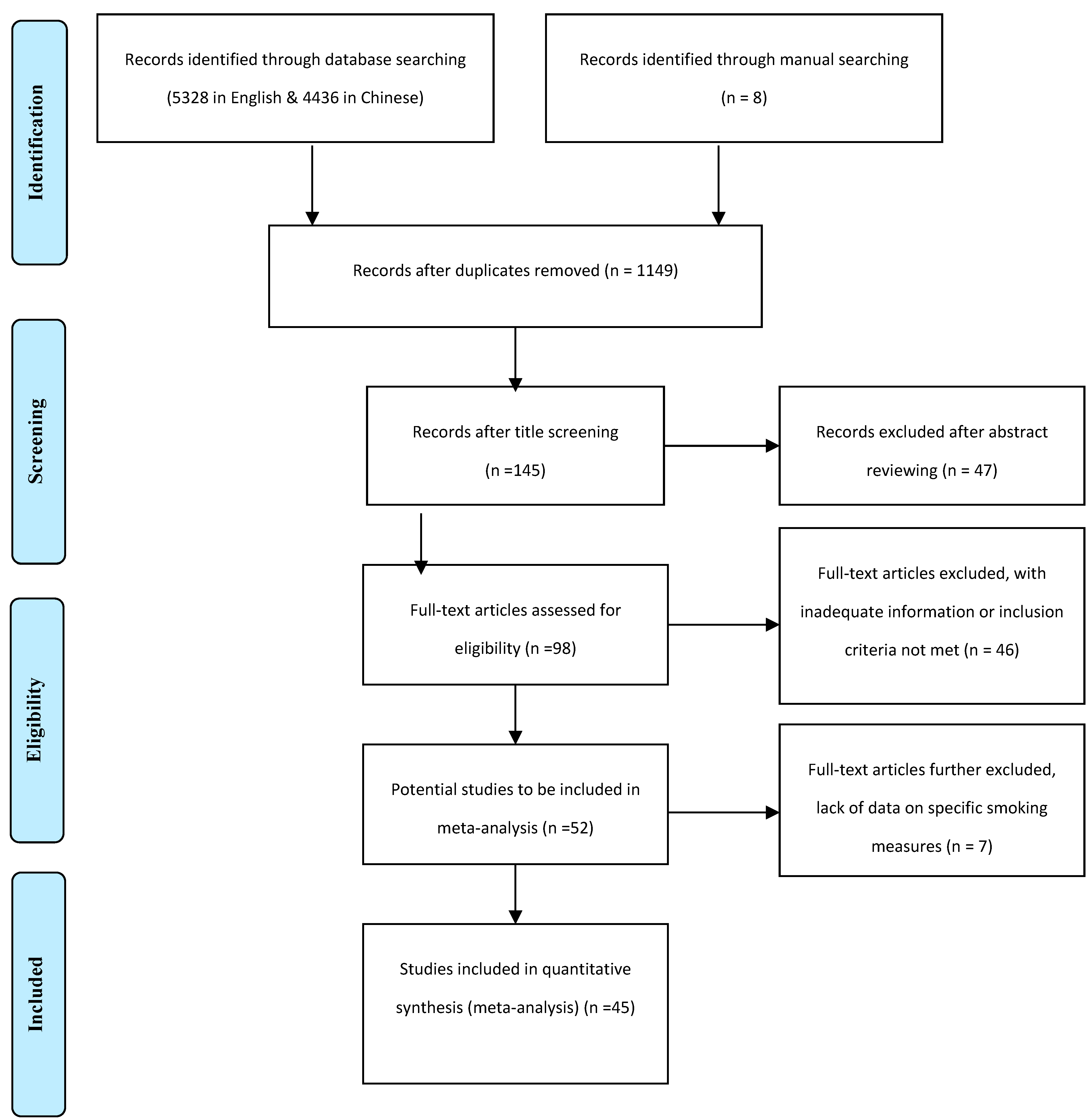
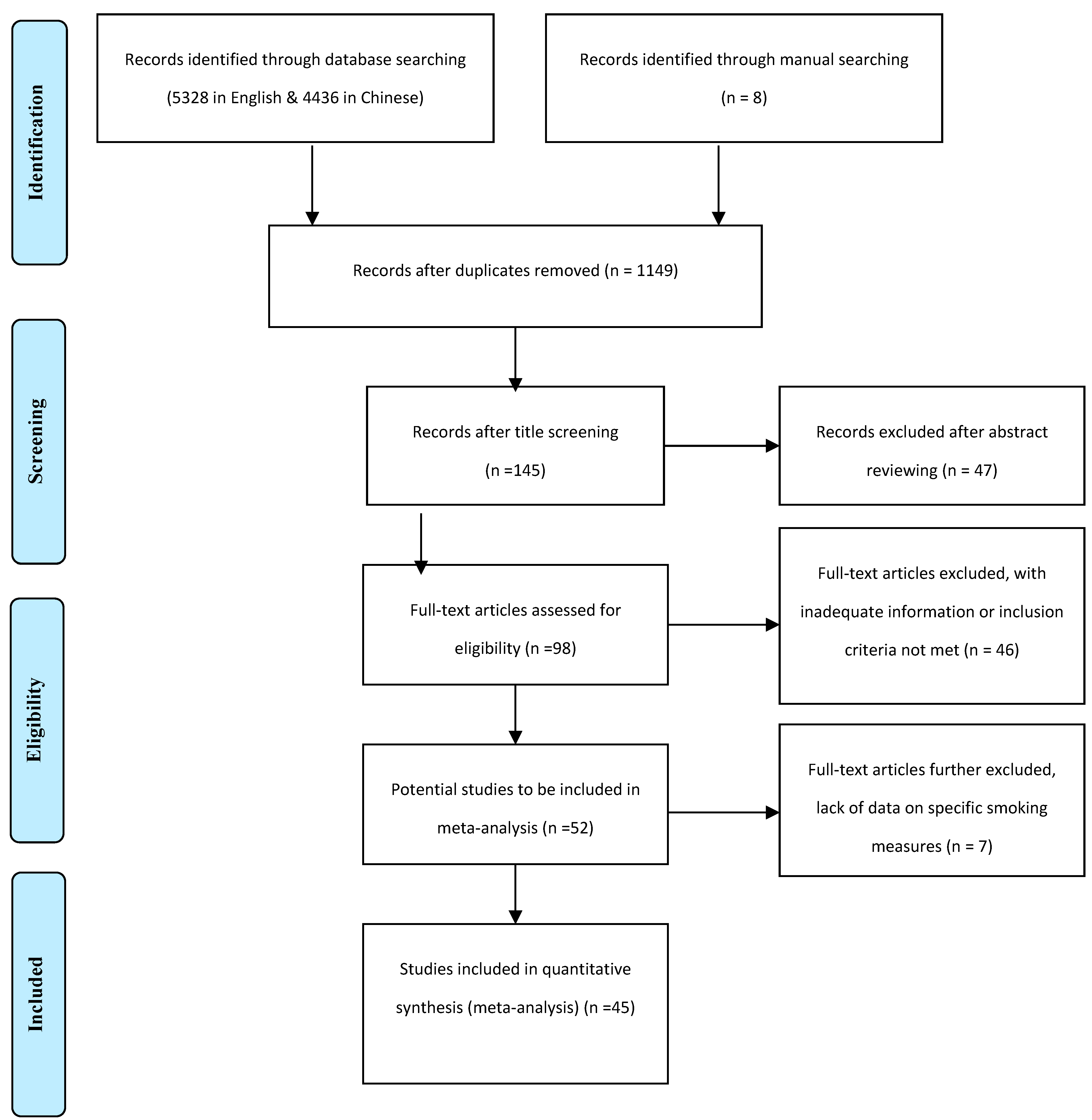
2.3. Paper Selection
2.4. Data Coding and Extracting
2.5. Measurement of Smoking Behavior
2.6. Prevalence Rate Estimation by Meta-Analysis
2.7. Measures to Deal with Special Issues
3. Results and Discussion
3.1. Summary of the Included Studies
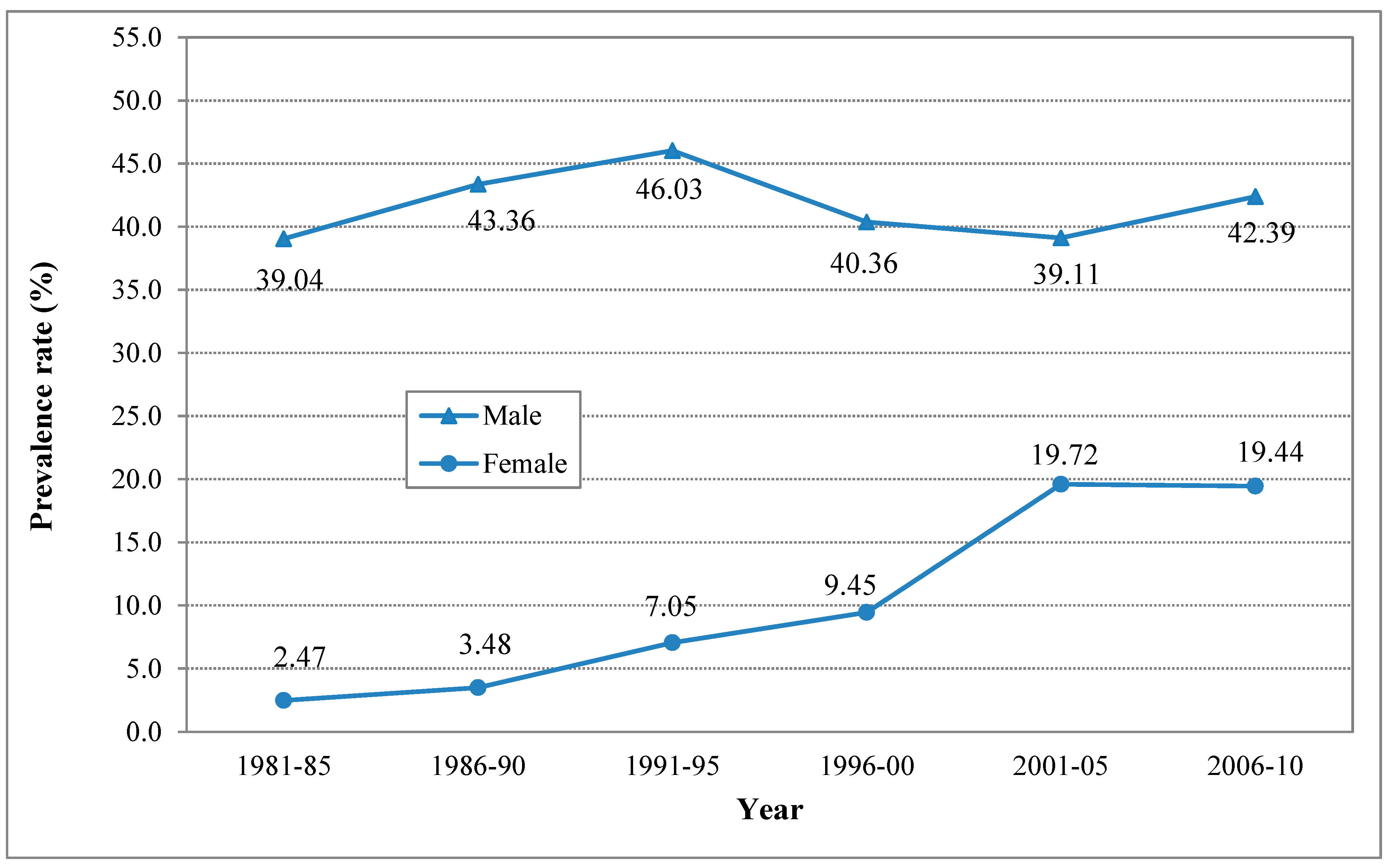
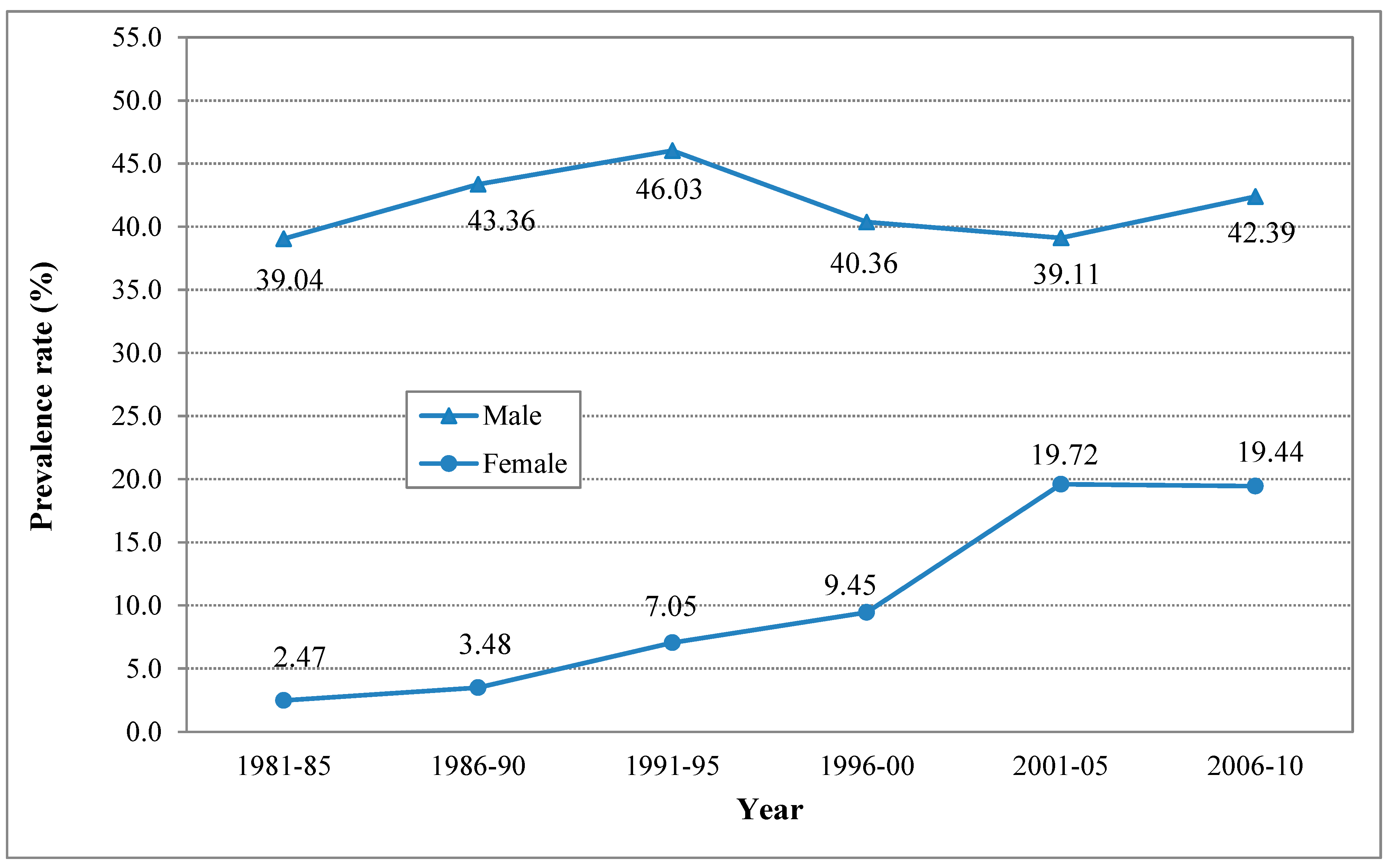
3.2. The Estimated Levels of and Time Trends in Lifetime Smoking

{kind=link}
{kind=link}
{kind=link}
| Gender | Time Period | Sample Weighted Method | Random Effect Method |
|---|---|---|---|
| (Year) | Prevalence Rate (95% CI) | Prevalence Rate (95% CI) | |
| Male | 1980–1985 | 39.48 (38.16, 40.81) | 39.04 (37.72, 40.36) |
| 1986–2000 | 39.71 (39.04, 40.37) | 43.36 (42.69, 44.03) | |
| 1991–1995 | 49.48 (48.50, 50.46) | 46.03 (45.05, 47.01) | |
| 1996–2000 | 42.24 (41.60, 42.88) | 40.36 (39.73, 41.00) | |
| 2001–2005 | 41.62 (41.32, 41.93) | 39.11 (38.81, 39.41) | |
| 2006–2010 | 42.27 (41.75, 42.80) | 42.39 (41.87, 42.92) | |
| Female | 1980–1985 | 4.45 (3.49, 5.41) | 2.47 (1.75, 3.19) |
| 1986–2000 | 4.10 (3.83, 4.38) | 3.48 (3.23, 3.73) | |
| 1991–1995 | 8.00 (7.43, 8.58) | 7.05 (6.51, 7.60) | |
| 1996–2000 | 11.17 (10.74, 11.61) | 9.45 (9.04, 9.85) | |
| 2001–2005 | 20.33 (20.08, 20.57) | 19.72 (19.38, 19.86) | |
| 2006–2010 | 20.31 (19.89, 20.73) | 19.44 (19.02, 19.86) |
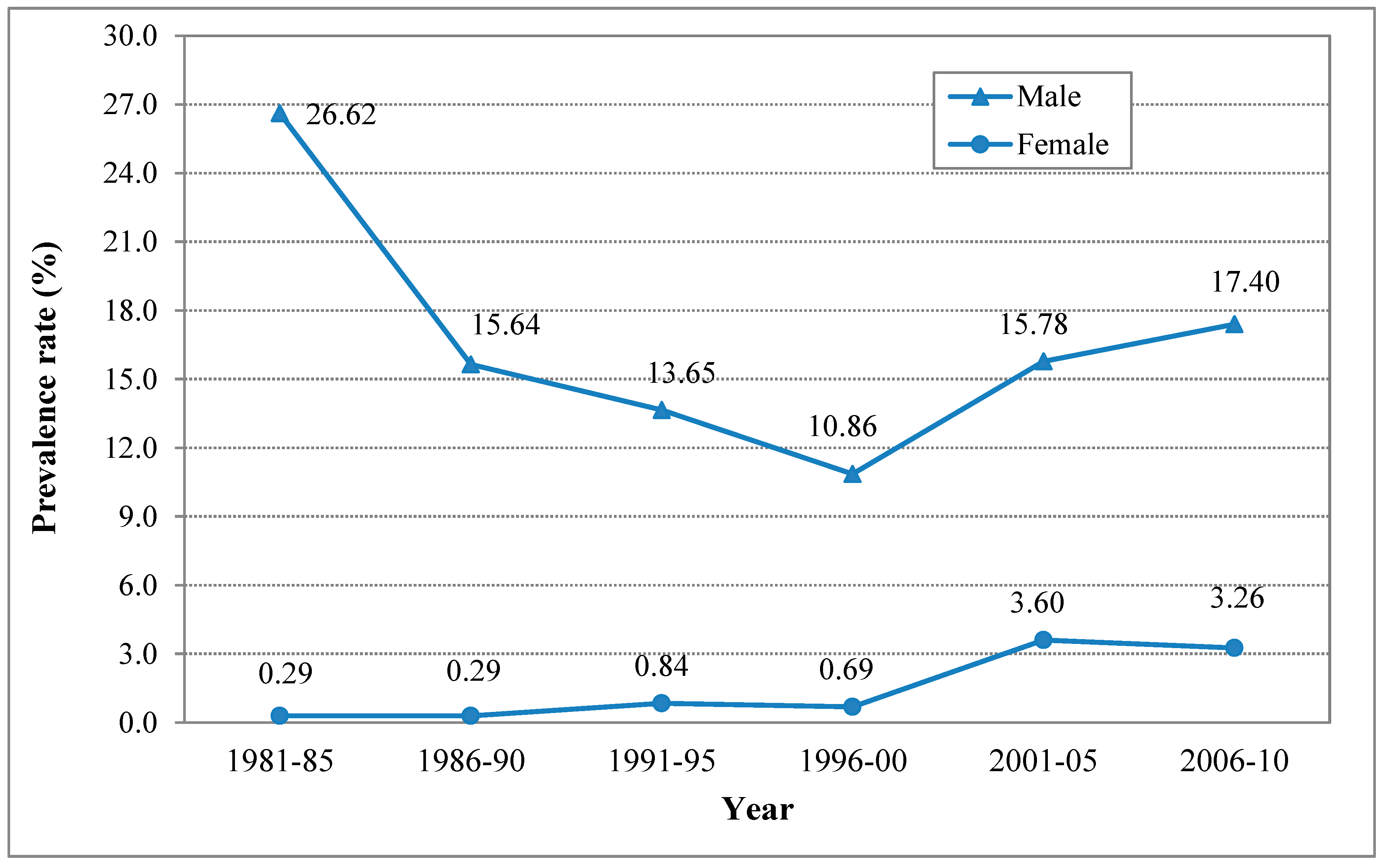
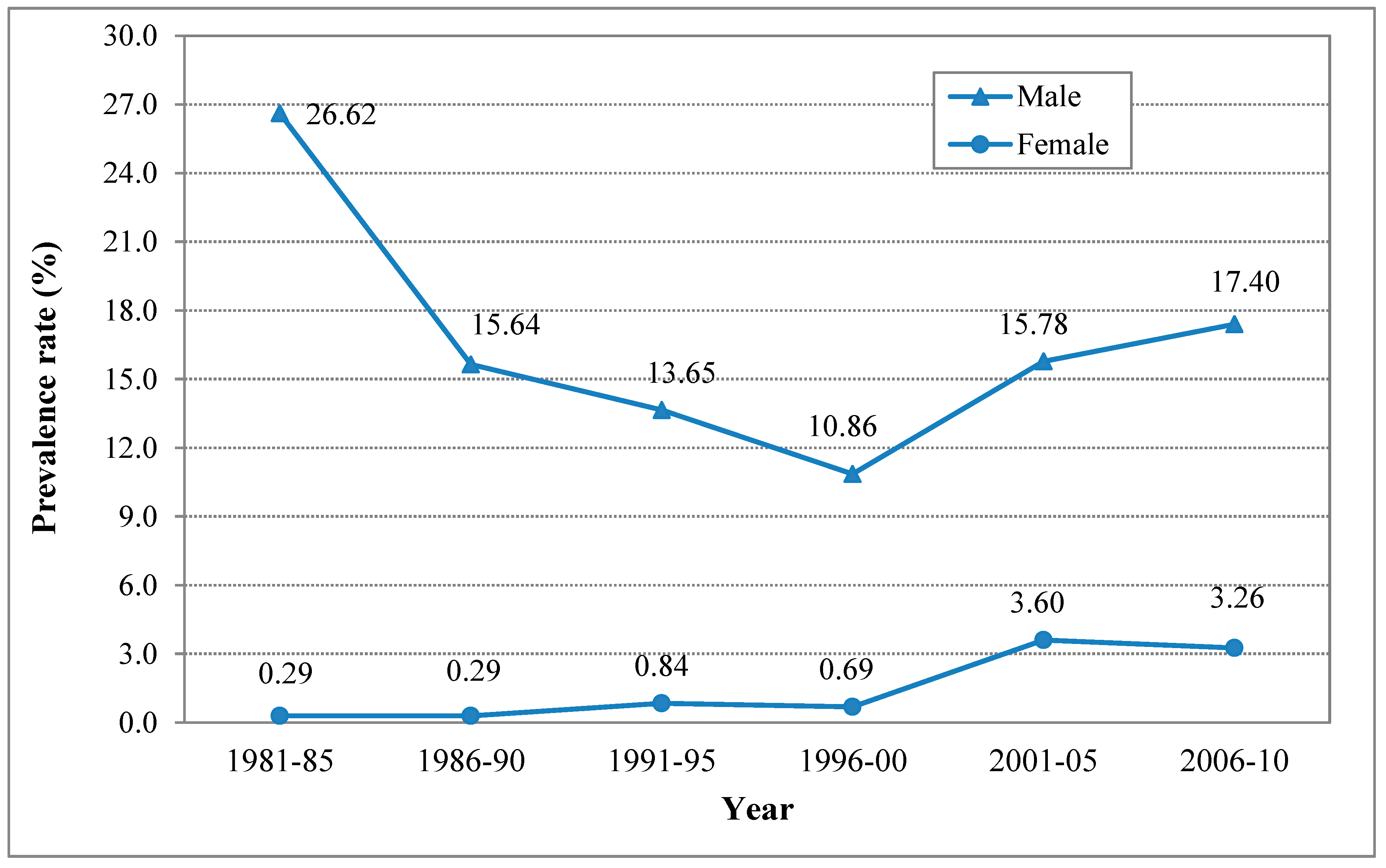
3.3. The Estimated Levels of and Time Trends in Current (30-Day) Smoking
| Gender | Time Period | Sample Weighted Method | Random Effect Method |
|---|---|---|---|
| (Year) | Prevalence Rate (95% CI) | Prevalence Rate (95% CI) | |
| Male | 1981–1985 | 26.95 (25.75, 28.15) | 26.62 (25.42, 27.81) |
| 1986–1990 | 12.54 (12.04, 13.04) | 15.64 (15.09, 16.19) | |
| 1991–1995 | 14.04 (13.36, 14.72) | 13.65 (12.97, 14.32) | |
| 1996–2000 | 10.35 (9.96, 10.75) | 10.86 (10.46, 11.26) | |
| 2001–2005 | 19.40 (19.15, 19.64) | 15.78 (15.56, 16.01) | |
| 2006–2010 | 19.51 (19.09, 19.93) | 17.40 (17.00, 17.80) | |
| Female | 1981–1985 | 0.29 (0.06, 0.51) | 0.29 (0.06, 0.51) |
| 1986–2000 | 0.47 (0.37, 0.58) | 0.29 (0.20, 0.37) | |
| 1991–1995 | 0.89 (0.68, 1.09) | 0.84 (0.64, 1.04) | |
| 1996–2000 | 1.25 (1.10, 1.41) | 0.69 (0.58, 0.80) | |
| 2001–2005 | 4.41 (4.29, 4.54) | 3.60 (3.49, 3.72) | |
| 2006–2010 | 4.89 (4.66, 5.12) | 3.26 (3.08, 3.45) |
4. Discussion
4.1. A Growing Number of Adolescent Smokers in China
4.2. Changing Gender Pattern in Cigarette Smoking
4.3. Implications for Tobacco Control
5. Conclusions
Supplementary Files
Supplementary File 1Acknowledgments
Author Contributions
Conflicts of Interest
References
- World Health Organization (WHO). WHO Report on the Global Tobacco Epidemic. The MPOWER Package. Available online: http://whqlibdoc.who.int/publications/2009/9789241563918_eng_full.pdf (accessed on 20 August 2012).
- Ji, C.; Chen, T.; Song, Y.; Hu, P.; Xing, Y.; Zhang, L. Smoking status of high school and college students in China. Chin. J. Sch. Health 2009, 30, 109–111. [Google Scholar]
- Gu, D.; Tanika, N.K.; Wu, X.; Chen, J.; Jonathan, M.S.; Huang, J.; Zhu, M.; Chen, J.; Chen, C.; Duan, X.; Michael, J.K.; He, J. Mortality attributable to smoking in China. N. Engl. J. Med. 2009, 360, 150–159. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health of the People’s Republic of China. The 2008 Reports of Tobacco Control in China; Community Health and Maternal and Child Health Division, The Chinese Ministry of Health: Beijing, China, 2008.
- Warren, C.W.; Riley, L.; Asma, S.; Eriksen, M.P.; Green, L.; Blanton, C.; Loo, C.; Batchelor, S.; Yach, D. Tobacco use by youth: A surveillance report from the global youth tobacco survey project. Bull. WHO 2000, 78, 868–876. [Google Scholar] [PubMed]
- Cochran, M.M.; Brassard, J.A. Child development and personal social networks. Child. Dev. 1979, 50, 601–616. [Google Scholar] [CrossRef]
- Blair, C.; Raver, C.C. Child development in the context of adversity: Experiential canalization of brain and behavior. Amer. Psychol. 2012, 67, 309–318. [Google Scholar] [CrossRef]
- Olivia, M.M.; Marcus, R.M.; Ute, L. Visual attention to health warnings on plain tobacco packaging in adolescent smokers and non-smokers. Addict. Biol. 2012. [Google Scholar] [CrossRef]
- O’Dell, L.E. NICO-TEEN: Neural substrates that mediate adolescent tobacco abuse. Neuropsychopharmacology 2011, 36, 356–357. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Jacques-Tiura, A. Smoking initiation associated with specific periods in the life course from birth to young adulthood: Data from the national longitudinal survey of youth 1997. Amer. J. Public Health 2014, 104, 119–126. [Google Scholar] [CrossRef]
- Preventing Tobacco Use among Youth and Young Adults: A Report of the Surgeon General; Office on Smoking and Health, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, U.S. Department of Health and Human Services: Atlanta, GA, USA, 2012.
- Hesketh, T.; Ding, Q.J.; Tomkins, A. Smoking among youths in China. Amer. J. Public Health 2001, 91, 1653–1655. [Google Scholar] [CrossRef]
- WHO Western Pacific Region. China and the WHO Framework Convention on Tobacco Control (WHO FCTC). Available online: http://www2.wpro.who.int/china/media_centre/news/BN20110107.htm (accessed on 7 January 2011).
- Chen, X.; Li, Y.; Unger, J.B.; Gong, J.; Johnson, C.A.; Guo, Q. Hazard of smoking initiation by age among adolescents in Wuhan, China. Prev. Med. 2001, 32, 437–445. [Google Scholar] [CrossRef] [PubMed]
- Wong, X.; Hong, S.; Chen, D.; Zhang, M.; Chen, B.; Tian, B. The 1984 national prevalence survey of smoking. People Health Press: Beijing, China, 1987. [Google Scholar]
- Yang, G.; Ma, J.; Chen, A.P.; Brown, S.; Taylor, C.E.; Samet, J.M. Smoking among adolescents in China: 1998 survey findings. Int. J. Epidemiol. 2004, 33, 1103–1110. [Google Scholar] [CrossRef] [PubMed]
- Yan, J.; Zhang, T. Smoking among middle school students in Huairou district of Beijing city. Occup. Health 2011, 27, 1085–1087. [Google Scholar]
- Wang, S.; Zhang, Z. Tobacco use status and KAP survey among 1446 middle school students in a district of Beijing. Chin. J. Sch. Health 2011, 32, 646–651. [Google Scholar]
- Li, J.; Li, X.; Peng, N. Analysis of smoking behavior and its related factors among adolescents in certain districts of Shanghai. Chin. J. Sch. Dr. 2005, 19, 111–114. [Google Scholar]
- Unger, J.B.; Li, Y.; Chen, X.; Xia, J.; Sun, A.Z.; Guo, Q.; Tan, S.; Gong, J.; Sun, P.; Liu, C.H.; Chou, C.P.; Zheng, H.; Anderson Johnson, C. Adolescent smoking in Wuhan, China: Baseline data from the Wuhan smoking prevention trial. Amer. J. Prev. Med. 2001, 21, 162–169. [Google Scholar] [CrossRef]
- Tao, F.B.; Huang, K.; Gao, M.; Su, P.Y. Smoking and subjective life qualities in middle school students. Chin. J. Epidemiol. 2006, 27, 132–136. [Google Scholar]
- Wen, X.; Chen, W.; Qian, Z.; Muscat, J.E.; Lu, C.; Ling, W. Differences in students’ smoking-related knowledge, attitudes, and behaviors among public, factory, and private secondary schools in Guangzhou, China. J. Sch. Health 2008, 78, 46–53. [Google Scholar] [CrossRef] [PubMed]
- Fang, H.; Ding, Y.; Li, N. Survey on adolescents’ knowledge, attitude, and behavior about smoking in Xi’an. Chin. J. Health Educ. 2008, 24, 19–20. [Google Scholar]
- Zhang, M.; Liang, Z.; Zhou, Y.; Yang, N. Survey on the status of smoking among 2569 middle school students of Thibetan in Lhasa city. Chin. Sch. Dr. 1990, 4, 20–22. [Google Scholar]
- Zhu, Y.; Zhang, T.; Wang, X.; Gao, H.; Chen, J.; Shen, Y. Survey on smoking behavior among junior high school students in 6 district of Ningbo. Chin. J. Prev. Med. 2011, 45, 464–466. [Google Scholar]
- Borenstein, M.; Hedges, L.V.; Higgins, P.T.; Rothstein, H.R. A basic introduction to fixed-effect and random-effects models for meta-analysis. Res. Synth. Method. 2010, 1, 97–111. [Google Scholar] [CrossRef]
- Liu, X. Survey on the status of smoking among 2144 middle school students in Nanzhao county. Sch. Health 1986, 7, 28–30. [Google Scholar]
- Wang, T.; Liu, M. Survey on cigarrete smoking situation of middle school students in Anshan city. Sch. Health 1988, 9, 6–7. [Google Scholar]
- Department of School Health, Sanitation Antiepidemic Station. The analysis of smoking habit among 2300 middle school students in urban and rural aeras, Guansu. Sch. Health 1986, 7, 25–27. [Google Scholar]
- U.S. Centers for Disease Control and Prevention. Cigarette use among high school students—The United States, 1991–2009. MMWR 2010, 59, 797–800. [Google Scholar]
- Rodu, B.; Cole, P. Smoking prevalence: A comparison of two American surveys. Public Health 2009, 123, 598–601. [Google Scholar] [CrossRef] [PubMed]
- Warren, C.W.; Jones, N.R.; Peruga, A.; Chauvin, J.; Baptiste, J.; Silva, V.C.; Awa, F.; Ssouros, A.; Rahman, K.; Fishburn, B. Global youth tobacco surveillance, 2000–2007. MMWR 2008, 57, 1–21. [Google Scholar] [PubMed]
- Giovino, G.A.; Mirza, S.A.; Samet, J.M.; Gupta, P.C.; Jarvis, M.J.; Bhala, N.; Peto, R.; Zatonski, W.; Hsia, J.; Morton, J.; et al. Tobacco use in 3 billion individuals from 16 countries: An analysis of nationally respresentative cross-sectional household surveys. Lancet 2012, 380, 668–679. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Hsia, J.; Yang, G. Prevalence of smoking in China in 2010. N. Engl. J. Med. 2011, 364, 2469–2470. [Google Scholar] [CrossRef] [PubMed]
- Gfroerer, J.; Wright, D.; Kopstein, A. Prevelence of youth substance use: The impact of methodological differences between two national surveys. Drug Alcohol Depend. 1997, 47, 19–30. [Google Scholar] [CrossRef] [PubMed]
- Yang, G. 1996 National Prevalence Survey of Smoking Pattern; China Science and Technology Press: Beijing, China, 1997. [Google Scholar]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.; Altman, D.G. Measuring inconsistency in meta-analysis. BMJ 2003, 327, 577–560. [Google Scholar] [CrossRef] [PubMed]
- Anderson, J.C.; Palmer, P.H.; Chou, C.P.; Pang, Z.; Zhou, D.; Dong, L.; Xiang, H.; Yang, P.; Xu, H.; Wang, J.; et al. Tobacco use among youth and adults in Mainland China: The China seven cities study. Public Health 2006, 120, 1156–1169. [Google Scholar] [CrossRef] [PubMed]
- Hu, P.; Ji, C.; Song, Y. Comparison of cigarette smoking among adolescents in Beijing and Yunnan province: Data from Chinese national youth risk behaviors surveillance. Chin. J. Sch. Health 2011, 32, 394–396. [Google Scholar]
- Guidelines for the conduct of tobacco smoking surveys of the general population: Report of a WHO meeting held in the general population. In Proceedings of the WHO Meeting, Helsinki, Finland, 29 November–4 December 1982; World Health Organisation: Geneva, Switzerland.
- Chen, X.; Gong, J.; Li, H.; Zhou, D.; Yan, Y. Receptivity to pro-tobacco meida and cigarette smoking among vocational high school students in China. Int. J. Pschological Stud. 2014, 6, 7–18. [Google Scholar]
- Beaglehole, R.; Bonita, R.; Horton, R.; Adams, C.; Alleyne, G.; Asaria, P.; Baugh, V.; Bekedam, H.; Billo, N.; Casswell, S.; et al. Priority actions for the non-communicable disease crisis. Lancet 2011, 377, 1438–1447. [Google Scholar] [CrossRef] [PubMed]
- Ho, M.G.; Ma, S.; Chai, W.; Xia, W.; Yang, G.; Novotny, T.E. Smoking among rural and urban young women in China. Tob. Control 2010, 19, 13–18. [Google Scholar] [CrossRef] [PubMed]
- Weiss, J.W.; Spruijt-Metz, D.; Palmer, P.H.; Chou, C.P.; Johnson, C.A. Smoking among adolescents in China: An analysis based upon the meanings of smoking theory. Amer. J. Health Promot. 2006, 20, 171–178. [Google Scholar] [CrossRef]
- Sun, W.; Ling, T. Smoking behavior among adolescents in the city, suburbs, and rural areas of Shanghai. Amer. J. Health Promot. 1997, 11, 331–336. [Google Scholar] [CrossRef]
- Yan, Y.; Jacques-Tiura, A.J.; Chen, X.; Xie, N.; Chen, J.; Yang, N.; Gong, J.; MacDonell, K.K. Application of the protection motivation theory in predicting cigarette smoking among adolecents in China. Addict. Behav. 2014, 39, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Burns, D.M.; Johnston, L.D. Overview of recent changes in adolescent smoking behavior. In Changing Adolescent Smoking Prevalence Smoking and Tobacco Control Monograph 14; U.S. Department of Health and Human Services, National Institutes of Health, National Cancer Institute: Bethesda, MD, USA, 2001; pp. 1–8. [Google Scholar]
- Yang, L.; Sung, H.Y.; Mao, Z.; Hu, T.W.; Rao, K. Economic costs attributable to smoking in China: Update and an 8-year comparison, 2000–2008. Tob. Control 2011, 20, 266–272. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Ren, Y.; Lin, F.; MacDonell, K.; Jiang, Y. Exposure to school and community based prevention programs and reductions in cigarette smoking among adolescents in the United States, 2000–2008. Eval. Program Plann. 2012, 35, 321–328. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Han, J.; Chen, X. A Meta-Analysis of Cigarette Smoking Prevalence among Adolescents in China: 1981–2010. Int. J. Environ. Res. Public Health 2015, 12, 4617-4630. https://doi.org/10.3390/ijerph120504617
Han J, Chen X. A Meta-Analysis of Cigarette Smoking Prevalence among Adolescents in China: 1981–2010. International Journal of Environmental Research and Public Health. 2015; 12(5):4617-4630. https://doi.org/10.3390/ijerph120504617
Chicago/Turabian StyleHan, Juan, and Xinguang Chen. 2015. "A Meta-Analysis of Cigarette Smoking Prevalence among Adolescents in China: 1981–2010" International Journal of Environmental Research and Public Health 12, no. 5: 4617-4630. https://doi.org/10.3390/ijerph120504617
APA StyleHan, J., & Chen, X. (2015). A Meta-Analysis of Cigarette Smoking Prevalence among Adolescents in China: 1981–2010. International Journal of Environmental Research and Public Health, 12(5), 4617-4630. https://doi.org/10.3390/ijerph120504617