
The Extent, Nature and Environmental Health Implications of Cottage Industries in Johannesburg, South Africa


Abstract
:1. Introduction

{kind=link}
| Toxic Metal | Cottage Industry | Health Effect |
|---|---|---|
| Lead | Electrical appliance repair [8,9] Hairdressing [10] Car repairs [11,12,13] Welding [11] Spray painting [14,15] Scrap metal recycling [8,16] Metal jewelry making [17] | Ill health effects include headache, irritability, abdominal pain, fatigue, nausea, vomiting, problems with intellectual development, convulsions, coma, renal failure, death, hypertension, cognitive impairment, tremor of the hands, excitability, memory loss, insomnia [18,19], cardiac conduction disturbances [20]. Children in particular are susceptible to the ill health effects of lead exposure due to their permeable blood-brain barrier and high gastrointestinal uptake. Children may be affected by behavioural disturbances, learning and concentration difficulties [19]. |
| Mercury | Electrical appliance repair [8,9] | Injury to the lungs and the neurological system, anxiety [18,19]. |
| Arsenic | Electrical appliance repair [8,9] | Skin hyperpigmentation, skin cancer, cancers of the liver, lungs and bladder, diabetes, blood vessel damage, and peripheral nerve damage (presenting as numbness or tingling in hands and feet) [18,19,21]. |
| Cadmium | Electrical appliance repair [8,9] Welding [22] Spray painting [14] Metal jewelry making [17] | Chronic lung disease [8], kidney dysfunction [23] and osteoporosis [24]. |
2. Methods
2.1. Data Collection
2.2. Procedure
2.3. Data Analysis
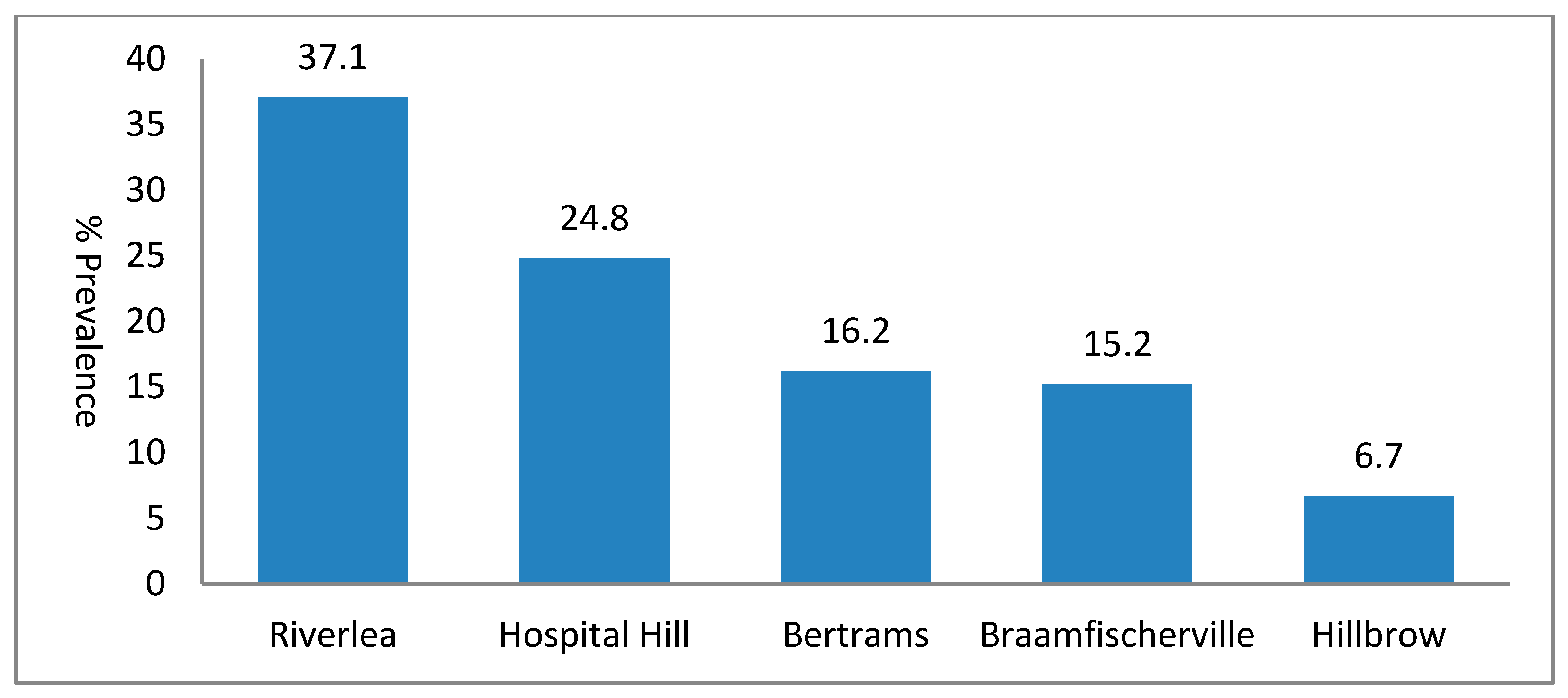
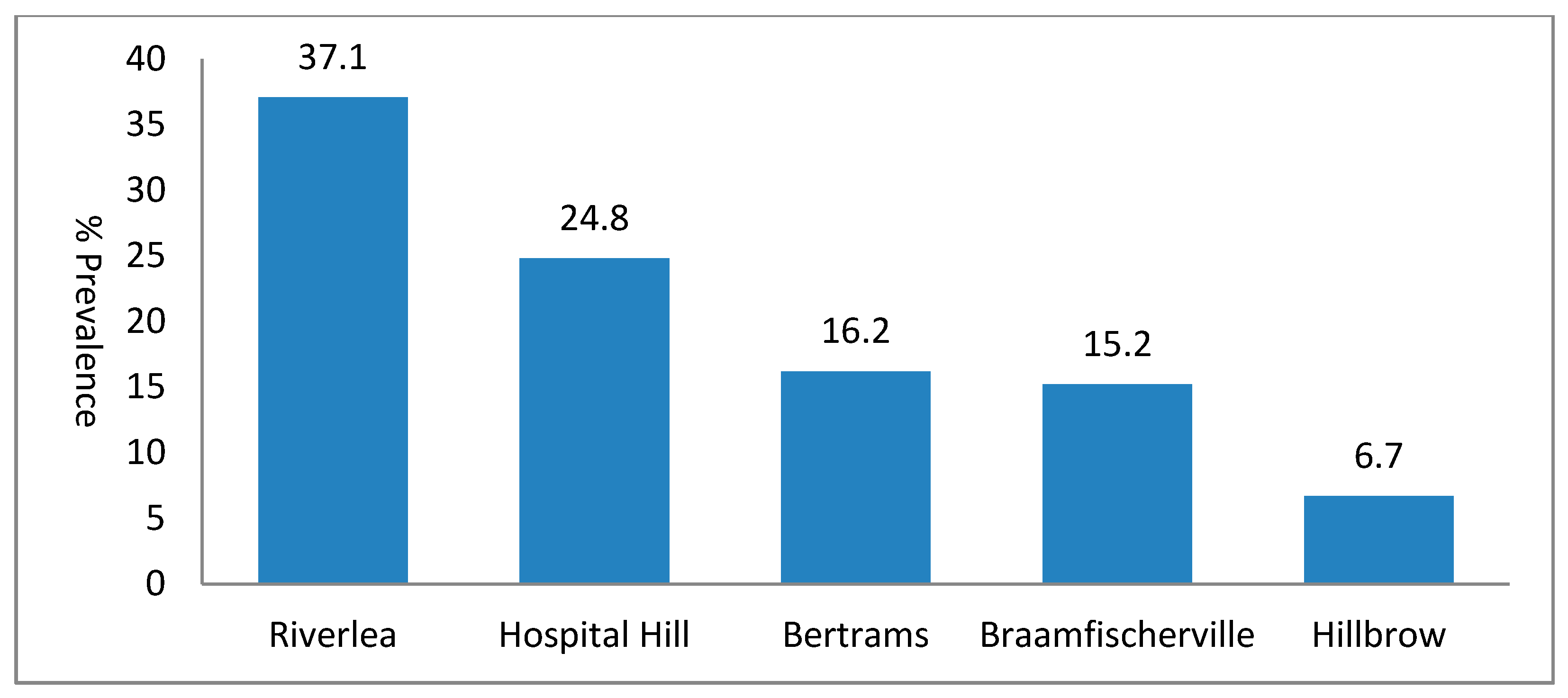
3. Results
Prevalence and Types of Cottage Industries
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- McCann, M. Hazards in cottage industries in developing countries. Amer. J. Ind. Med. 1996, 30, 125–129. [Google Scholar]
- Chen, M.; Sebstad, J.; O#x2019;Connell, L. Counting the invisible workforce: The case of homebased workers. World Dev. 1999, 27, 603–610. [Google Scholar]
- Hiralal, K. The “invisible” workers of the informal economy—A case study of home-based workers in Kwazulu/Natal, South Africa. J. Soc. Sci. 2010, 23, 29–37. [Google Scholar]
- Knishkowy, B.; Baker, E.L. Transmission of occupational disease to family contacts. Amer. J. Ind. Med. 1986, 9, 543–550. [Google Scholar]
- Tong, S.; von Schirnding, Y.E.; Prapamontol, T. Environmental lead exposure: A public health problem of global dimensions. Bull. WHO 2000, 78, 1068–1077. [Google Scholar]
- Stein, J.; Schettler, T.; Wallinga, D.; Valenti, M. In harm’s way: Toxic threats to child development. Dev. Behav. Pediatr. 2002, 23, S13–S22. [Google Scholar]
- Horton, L.M.; Mortensen, M.E.; Iossifova, Y.; Wald, M.M.; Burgess, P. What do we know of childhood exposures to metals (arsenic, cadmium, lead, and mercury) in emerging market countries? Int. J. Pediatr. 2013. Available online: http://dx.doi.org/10.1155/2013/872596 (accessed on 15 September 2014).
- Occupational Safety and Health Administration (OSHA). Guidance for the Identification and Control of Safety and Health Hazards in Metal Scrap Recycling. 2008. Available online: http://www.osha.gov (accessed on 15 January 2015). [Google Scholar]
- Hazardous Substances in E-Waste. Available online: http://ewasteguide.info/ (accessed on 4 June 2014).
- Mielke, H.W.; Taylor, M.D.; Gonzales, C.R.; Smith, M.K.; Daniels, P.V.; Buckner, A.V. Lead-based hair coloring products: Too hazardous for household use. J. Amer. Pharm. Assoc. 1997, 37, 85–89. [Google Scholar]
- Clausen, J.; Rastogi, S.C. Heavy metal pollution among autoworkers. I. Lead. Brit. J. Ind. Med. 1977, 34, 208–215. [Google Scholar]
- Öktem, F.; Arslan, M.K.; Dündar, B.; Delibas, N.; Gültepe, M.; Ilhan, I.E. Renal effects and erythrocyte oxidative stress in long-term low-level lead-exposed adolescent workers in auto repair workshops. Arch. Toxicol. 2004, 78, 681–687. [Google Scholar]
- Babalola, O.O.; Ojo, L.O.; Aderemi, M.O. Lead levels in some biological samples of auto-mechanics in Abeokuta, Nigeria. Indian J. Biochem. Biophys. 2005, 42, 401–403. [Google Scholar]
- Vitayavirasuk, B.; Junhom, S.; Tantisaeranee, P. Exposure to lead, cadmium and chromium among spray painters in automobile body repair shops. J. Occup. Health 2005, 47, 518–522. [Google Scholar]
- Tahir, H.; JahanZeb, Q.; Sultan, M. Assessment of heavy metal exposure around auto body refinishing shops. Afr. J. Biotechnol. 2010, 9, 7862–7869. [Google Scholar]
- Department of Labor and Industries. Preventing Lead Poisoning in Scrap Metal Recycling. Available online: http://www.lni.wa.gov/safety/research/files/lead_scrap.pdf (accessed on 16 January 2015).
- Gonzales, M.; Shah, V.; Bobelu, A.; Qualls, C.; Natachu, K.; Bobelu, J.; Jamon, E.; Neha, D.; Paine, S.; Zager, P. Concentrations of surface-dust metals in Native American jewelry-making homes in Zuni Pueblo, New Mexico. Arch. Environ. Health 2004, 59, 245–249. [Google Scholar]
- Hu, H. Human health and heavy metals exposure. In Life Support; McCally, M., Ed.; The Environment and Human Health, MIT Press: Cambridge, MA, USA, 2002. [Google Scholar]
- Järup, L. Hazards of heavy metal contamination. Brit. Med. Bull. 2003, 68, 167–182. [Google Scholar]
- Cheng, Y.; Schwartz, J.; Vokonas, P.S.; Weiss, S.T.; Aro, A.; Hu, H. Electrocardiographic conduction disturbances in association with low-level lead exposure (the Normative Aging Study). Amer. J. Cardiol. 1998, 82, 594–599. [Google Scholar]
- Çöl, M.; Çöl, C.; Soran, A.; Sayli, B.S.; Öztürk, S. Arsenic-related Bowen’s Disease, palmar keratosis, and skin cancer. Environ. Health Perspect. 1999, 107, 687–689. [Google Scholar]
- Clausen, J.; Rastogi, S.C. Heavy metal pollution among autoworkers. II. Cadmium, chromium, copper, manganese, and nickel. Brit. J. Ind. Med. 1977, 34, 216–220. [Google Scholar]
- Järup, L.; Hellström, L.; Alfvén, T.; Carlsson, M.D.; Grubb, A.; Persson, B.; Pettersson, C.; Spång, G.; Schütz, A.; Elinder, C.G. Low level exposure to cadmium and early kidney damage: The OSCAR study. Occup. Environ. Med. 2000, 57, 668–672. [Google Scholar]
- Alfvén, T.; Elinder, C-G.; Carlsson, M.G.; Grubb, A.; Hellström, L.; Persson, B.; Pettersson, C.; Spång, B.; Schütz, A.; Järup, L. Low-level cadmium exposure and osteoporosis. J. Bone Miner. Res. 2000, 15, 1579–1586. [Google Scholar]
- Mathee, A. Indicators of Health Environment and Development: Longitudinal Study in Johannesburg, 2006–2008; Environmental & Health Research Unit, South African Medical Research Council: Johannesburg, South Africa, 2009. Available online: http://www.mrc.ac.za/environmenthealth/head0608.pdf (accessed on 4 June 2014).
- Labréche, F.; Forest, J.; Trottier, M.; Lalonde, M.; Simard, R. Characterization of chemical exposures in hairdressing salons. Appl. Occup. Environ. Hyg. 2003, 8, 1014–1021. [Google Scholar]
- Banks, E.C.; Ferretti, L.E.; Shucard, D.W. Effects of low-level lead exposure on cognitive function in children: A review of behavioural, neuropsychological and biological evidence. Neurotoxicology 1997, 18, 237–281. [Google Scholar]
- Haefliger, P.; Mathieu-Nolf, M.; Lociciro, S.; Ndiaye, C.; Coly, M.; Diouf, A.; Faye, A.L.; Sow, A.; Tempowski, J.; Pronczuk, J.; et al. Mass lead intoxication from informal used lead-acid battery recycling in Dakar, Senegal. Environ. Health Perspect. 2009, 117, 1535–1540. [Google Scholar]
- Nriagu, J.O. Toxic metal pollution in Africa. Sci. Total Environ. 1992, 121, 1–37. [Google Scholar]
- Suplido, M.L.; Ong, C.N. Lead exposure among small scale battery recyclers, automobile radiator mechanics, and their children in Manila, the Philippines. Environ. Res. 2000, 82, 231–238. [Google Scholar]
- Matte, T.D.; Fiqueroa, J.P.; Ostrowski, S.; Burr, G.; Jackson-Hunt, L.; Keenlyside, R.A.; Baker, E.L. Lead poisoning among household members exposed to lead-acid battery repair shops in Kingston, Jamaica. Int. J. Epidemiol. 1989, 18, 874–881. [Google Scholar]
- Paoliello, M.M.; de Capitani, E.M. Environmental contamination and human exposure to lead in Brazil. Rev. Environ. Contam. Toxicol. 2005, 184, 59–96. [Google Scholar]
- UNEP. Draft Final Review of Scientific Information on Lead; United Nations Environment Programme, Chemicals Branch: Geneva, Switzerland, 2008. Available online: http://www.chem.unep.ch/Pb_and_Cd/SR/Draft_final_reviews/Pb_Review/Final_UNEP_Lead_review_Nov_2008.pdf (accessed on 23 January 2015).
- Mathee, A.; Harpham, T.; Barnes, B.; Swart, A.; Naidoo, S.; de Wet, T.; Becker, P. Inequity in poverty: The emerging public health challenge in Johannesburg. Dev. Southern Afr. 2009, 26, 721–732. [Google Scholar]
- Kootbodien, T.; Mathee, A.; Naicker, N.; Moodley, N. Heavy metal contamination in a school vegetable garden in Johannesburg. S. Afr. Med. J. 2012, 102, 226–227. [Google Scholar]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Teare, J.; Kootbodien, T.; Naicker, N.; Mathee, A. The Extent, Nature and Environmental Health Implications of Cottage Industries in Johannesburg, South Africa. Int. J. Environ. Res. Public Health 2015, 12, 1894-1901. https://doi.org/10.3390/ijerph120201894
Teare J, Kootbodien T, Naicker N, Mathee A. The Extent, Nature and Environmental Health Implications of Cottage Industries in Johannesburg, South Africa. International Journal of Environmental Research and Public Health. 2015; 12(2):1894-1901. https://doi.org/10.3390/ijerph120201894
Chicago/Turabian StyleTeare, June, Tahira Kootbodien, Nisha Naicker, and Angela Mathee. 2015. "The Extent, Nature and Environmental Health Implications of Cottage Industries in Johannesburg, South Africa" International Journal of Environmental Research and Public Health 12, no. 2: 1894-1901. https://doi.org/10.3390/ijerph120201894
APA StyleTeare, J., Kootbodien, T., Naicker, N., & Mathee, A. (2015). The Extent, Nature and Environmental Health Implications of Cottage Industries in Johannesburg, South Africa. International Journal of Environmental Research and Public Health, 12(2), 1894-1901. https://doi.org/10.3390/ijerph120201894