Serum Lipid Profiles, Lipid Ratios and Chronic Kidney Disease in a Chinese Population

Abstract
:1. Introduction
2. Experimental Section
2.1. Study Population
2.2. Ethics Statement
2.3. Serum Lipid Profiles and Lipid-Related Ratios
2.4. Determination of CKD
2.5. Data Collection
2.6. Data Analysis
3. Results
3.1. Clinical Characteristics of Study Population (Table 1)

{kind=link}
{kind=link}
{kind=link}
| Total | Male | Female | P value | |
|---|---|---|---|---|
| n = 1834 | n = 679 | n = 1155 | ||
| Clinical Characteristics | ||||
| Age (Years) | 53 ± 15 | 53 ± 15 | 53 ± 14 | 0.29 |
| Waist circumference(cm) | 83 ± 10 | 86 ± 10 | 81 ± 10 | <0.001 |
| History of Hypertension (%) | 372 (20.28) | 166 (24.45) | 206 (17.84) | 0.001 |
| History of Diabetes (%) | 115 (6.27) | 48 (7.07) | 67 (5.80) | 0.29 |
| History of Coronary heart disease (%) | 42 (2.29) | 23 (3.39) | 19 (1.65) | 0.27 |
| Current smoker (%) | 223 (12.16) | 214 (31.52) | 9 (0.78) | <0.001 |
| Current alcohol use (%) | 106 (5.78) | 94 (13.84) | 12 (1.04) | <0.001 |
| Education attainment High school or above (%) | 761 (41.49) | 344 (50.66) | 417 (36.10) | 0.92 |
| Physical inactivity (%) | 1013 (55.23) | 374 (55.08) | 639 (55.32) | <0.001 |
| Systolic blood pressure (mmHg) | 129 ± 20 | 130 ± 19 | 127 ± 21 | 0.003 |
| Diastolic blood pressure (mmHg) | 78 ± 11 | 80 ± 11 | 77 ± 11 | <0.001 |
| Serum lipids | ||||
| Cholesterol (mmol/L) | 5.39 ± 1.03 | 5.34 ± 0.99 | 5.42 ± 1.05 | 0.09 |
| LDL (mmol/L) | 3.18 ± 0.91 | 3.14 ± 0.92 | 3.20 ± 0.90 | 0.19 |
| HDL (mmol/L) | 1.54 ± 0.33 | 1.44 ± 0.31 | 1.60 ± 0.32 | <0.001 |
| Triglyceride (mmol/L) | 0.65 (0.32–1.98) | 1.37 (0.97–2.17) | 1.15 (0.83–1.61) | <0.001 |
| LDL/HDL ratio | 2.09 (1.67–2.59) | 2.22 (1.81–2.76) | 2.00 (1.60–2.48) | <0.001 |
| TG/HDL ratio | 0.83 (0.53–1.35) | 1.03 (0.63–1.68) | 0.73 (0.48–1.17) | <0.001 |
| TC/HDL ratio | 3.58 (3.01–4.15) | 3.83 (3.23–4.38) | 3.45 (2.92–3.99) | <0.001 |
| Other labratory | ||||
| Serum creatitine (umol/L) | 73 ± 17 | 87 ± 15 | 65 ± 11 | <0.001 |
| eGFR( mL/min/1.73m2) | 99 ± 22 | 92 ± 20 | 104 ± 22 | <0.001 |
| ACR (mg/g) | 8.49 (5.75–14.23) | 9.54 (6.63–15.56) | 6.81 (4.59–11.46) | <0.001 |
| Fasting glucose (mmo/L) | 5.01 ± 1.19 | 5.07 ± 1.26 | 4.98 ± 1.14 | 0.10 |
| Serum C-reactive protein (mg/L) | 0.99 (0.46–2.37) | 1.01 (0.49–2.63) | 0.98 (0.44–2.25) | 0.17 |
| CKD | 235 (12.81) | 83 (12.22) | 152 (13.16) | 0.56 |
| Dyslipidemia | 1474 (80.37) | 556 (81.89) | 918 (79.48) | 0.21 |
3.2. Association of Serum Lipids, Lipid Ratios with CKD in Male and Female Subjects (Table 2)
| Men | Women | |||||||
|---|---|---|---|---|---|---|---|---|
| Unadjusted | Adjusted * | Unadjusted | Adjusted * | |||||
| OR (95% CI) | P value | OR (95% CI) | P value | OR (95% CI) | P value | OR (95% CI) | P value | |
| TC (one SD) | 1.29 (1.03–1.61) | 0.03 | 1.21 (0.91–1.62) | 0.19 | 1.27 (1.08–1.50) | 0.004 | 0.97 (0.79–1.20) | 0.79 |
| HDL (one SD) | 1.17 (0.94–1.44) | 0.16 | 1.20 (0.91–1.59) | 0.19 | 0.99 (0.84–1.18) | 0.94 | 1.12 (0.93–1.36) | 0.22 |
| LDL (one SD) | 0.97 (0.77–1.23) | 0.80 | 0.89 (0.67–1.18) | 0.40 | 1.18 (1.00–1.40) | 0.054 | 0.92 (0.75–1.13) | 0.44 |
| Log-triglyceride (one SD) | 1.53 (1.23–1.91) | <0.001 | 1.39 (1.03–1.87) | 0.03 | 1.44 (1.22–1.69) | <0.001 | 1.03 (0.83–1.28) | 0.82 |
| Log-TG/HDL (one SD) | 1.44 (1.14–1.82) | 0.002 | 1.30 (0.95–1.77) | 0.10 | 1.39 (1.17–1.64) | <0.001 | 0.98 (0.78–1.22) | 0.83 |
| Log-TC/HDL (one SD) | 1.13 (0.90–1.43) | 0.31 | 1.03 (0.76–1.40) | 0.84 | 1.29 (1.08–1.54) | 0.005 | 0.84 (0.67–1.06) | 0.14 |
| Log-LDL/HDL (one SD) | 0.93 (0.74–1.17) | 0.52 | 0.83 (0.64–1.09) | 0.18 | 1.22 (1.02–1.46) | 0.03 | 0.86 (0.69–1.07) | 0.18 |
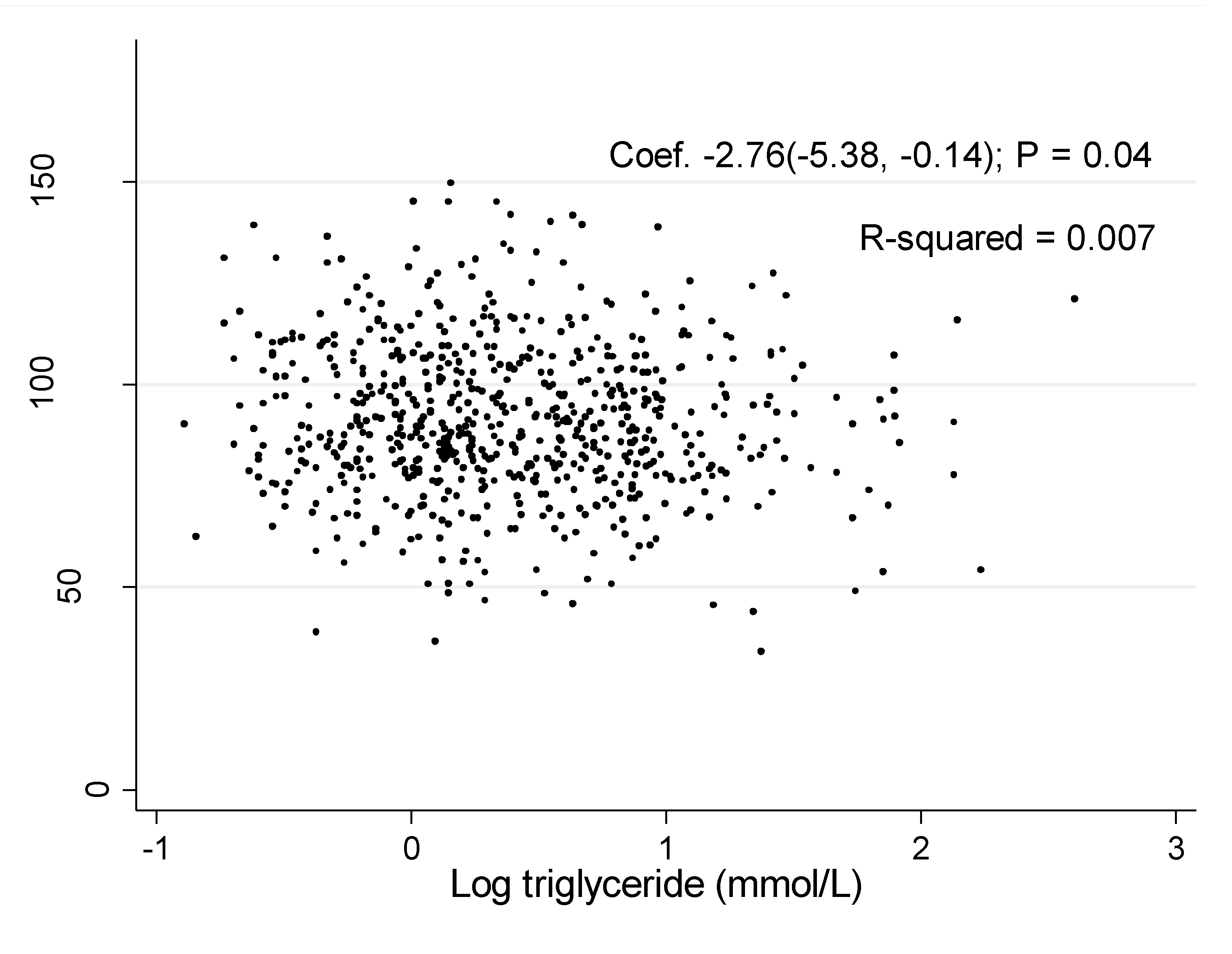
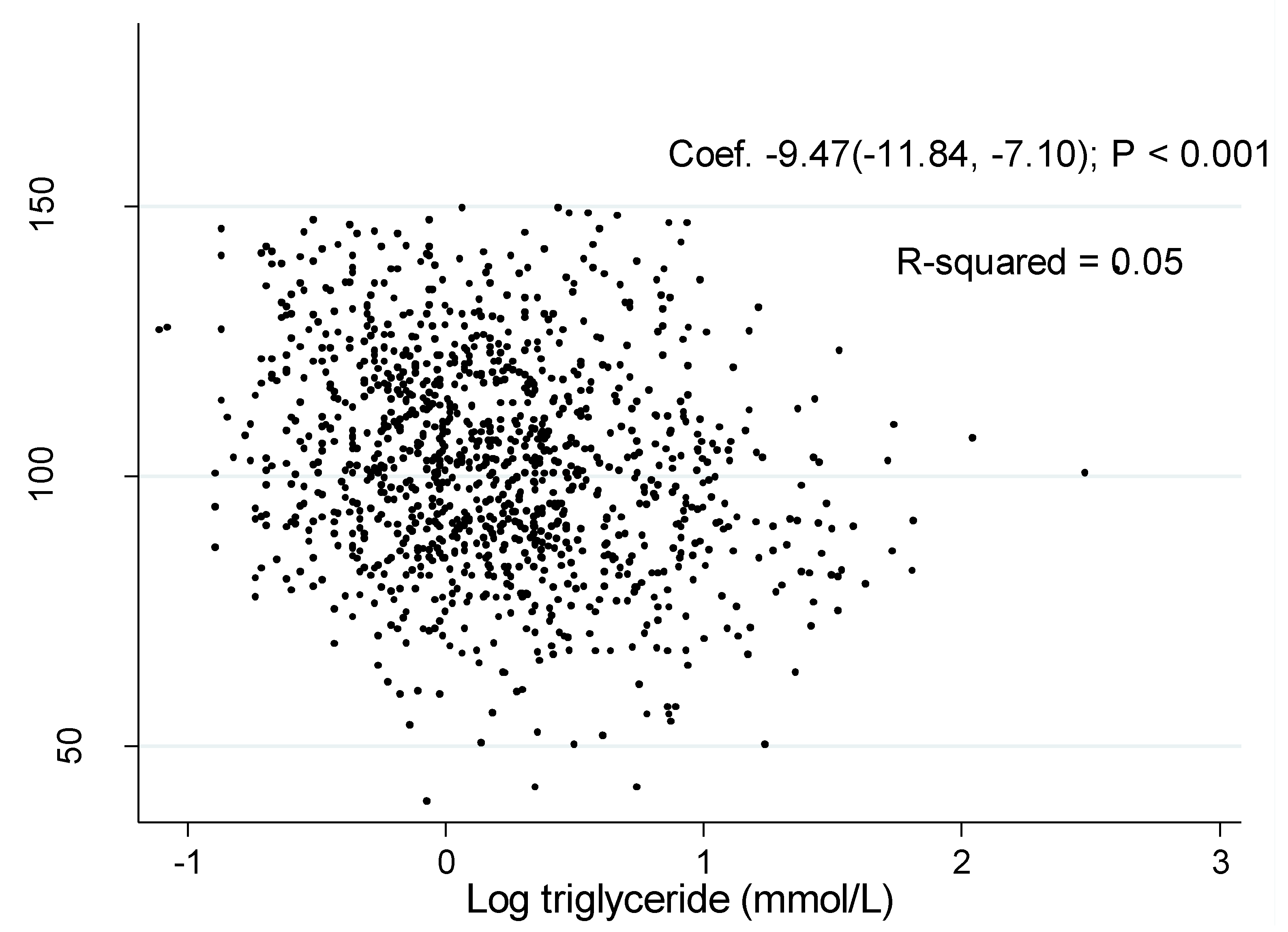
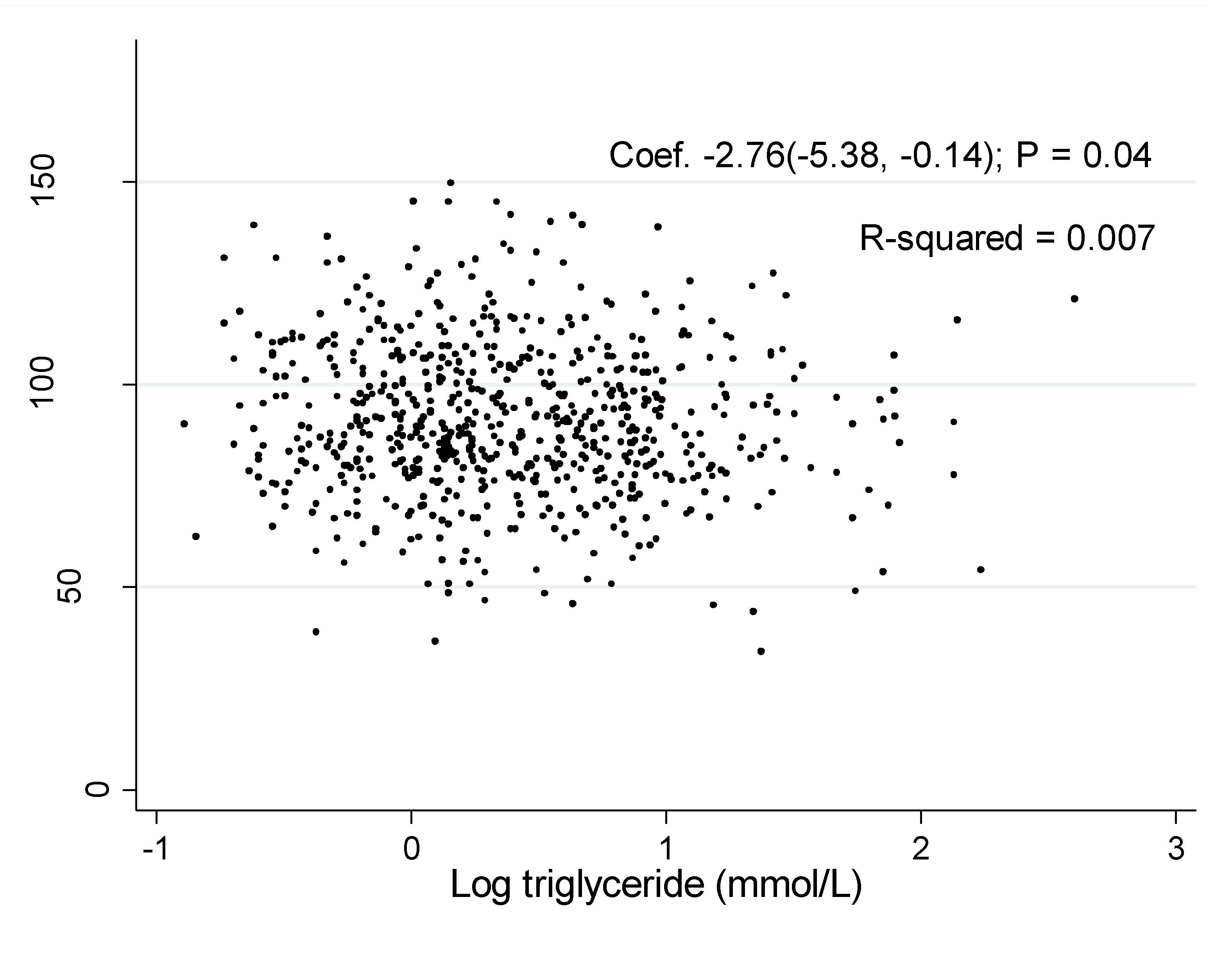
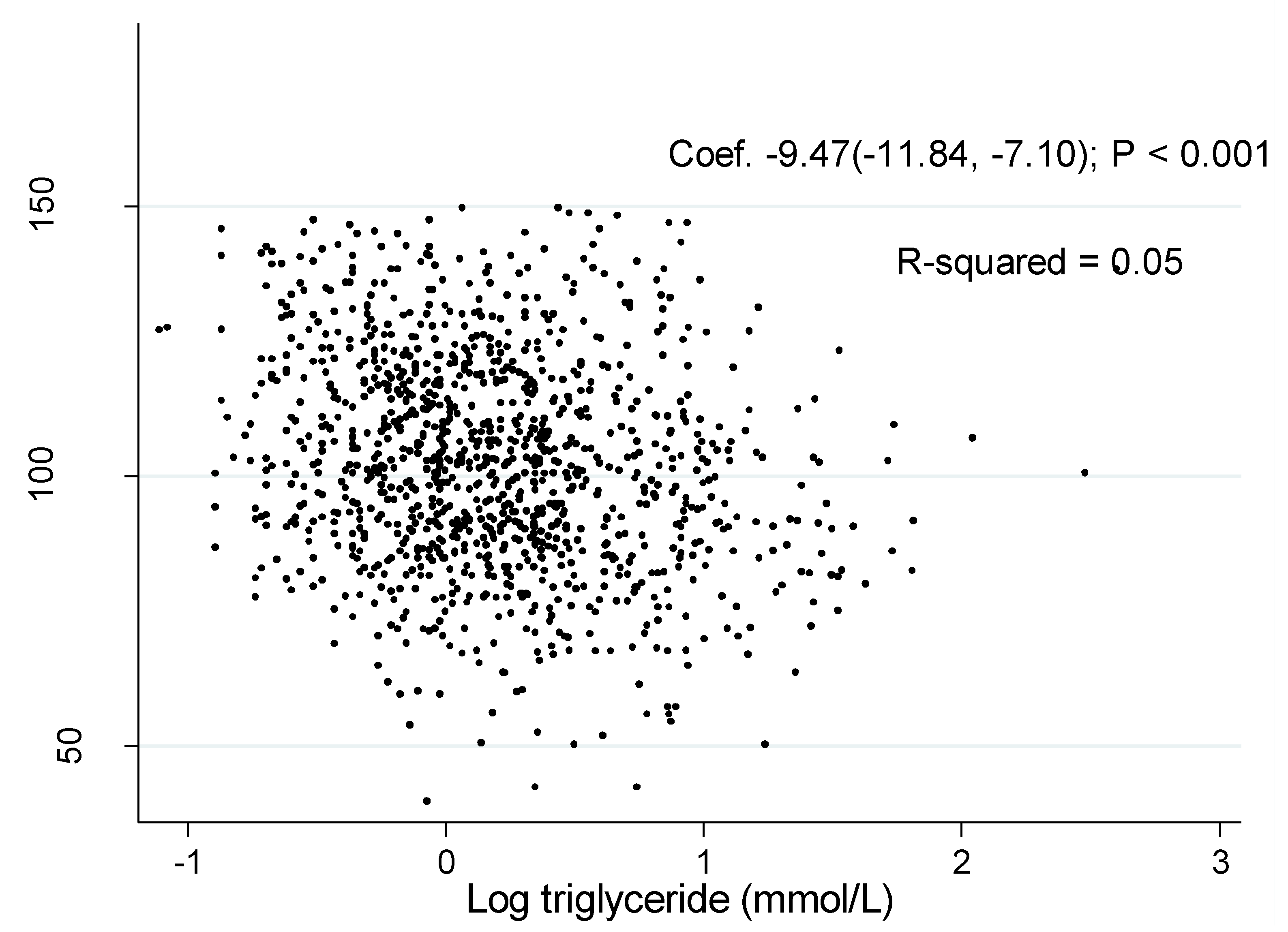
3.3. Correlation of eGFR or ACR with Serum Lipids and Lipid Ratios
| Men | Women | |||||||
|---|---|---|---|---|---|---|---|---|
| eGFR | ACR | eGFR | ACR | |||||
| Coefficient * (95% CI) | P value | Coefficient * (95% CI) | P value | Coefficient * (95% CI) | P value | Coefficient * (95% CI) | P value | |
| Total Cholesterol | −0.82 (−2.30–0.67) | 0.28 | −0.03 (−0.10–0.03) | 0.31 | −1.45 (−2.76–−0.15) | 0.03 | −0.02 (−0.07–0.03) | 0.43 |
| HDL | −0.01 (−4.84– 4.84) | 1.00 | 0.06 (−0.15–0.28) | 0.55 | 0.17 (−1.05–1.39) | 0.79 | 0.03 (−0.02–0.08) | 0.18 |
| LDL | 0.30 (−1.28–1.88) | 0.71 | −0.08 (−0.15–−0.01 | 0.02 | −0.74 (−2.03–0.55) | 0.26 | −0.03 (−0.08–0.02) | 0.25 |
| Log-triglyceride | −4.89 (−7.61–−2.17) | <0.001 | 0.003 (−0.12–0.12) | 0.96 | −1.78 (−3.14–−0.43) | 0.01 | 0.005 (−0.05–0.06) | 0.86 |
| Log-TG/HDL | −4.04 (−6.53–−1.65) | 0.001 | −0.005 (−0.11–0.10) | 0.94 | −1.57 (−2.92–−0.22) | 0.03 | −0.006 (−0.06–0.05) | 0.83 |
| Log-TC/HDL | −5.65 (−12.64–1.35) | 0.11 | −0.21 (−0.51–0.10) | 0.19 | −1.53 (−2.87–−0.18) | 0.03 | −0.05 (−0.10–0.005) | 0.08 |
| Log-LDL/HDL | 0.42 (−3.70–4.55) | 0.84 | −0.25 (−0.43–−0.07) | 0.007 | −0.64 (−1.93–0.65) | 0.33 | −0.03 (−0.08–0.02) | 0.22 |
4. Discussion
5. Conclusions
Acknowledgments
Authors Contributions
Conflicts of Interest
References
- Miller, M.; Stone, N.J.; Ballantyne, C.; Bittner, V.; Criqui, M.H.; Ginsberg, H.N.; Goldberg, A.C.; Howard, W.J.; Jacobson, M.S.; Kris-Etherton, P.M.; et al. Triglycerides and cardiovascular disease: A scientific statement from the American Heart Association. Circulation 2011, 123, 2292–2333. [Google Scholar] [CrossRef]
- Kurella, M.; Lo, J.C.; Chertow, G.M. Metabolic syndrome and the risk for chronic kidney disease among nondiabetic adults. J. Am. Soc. Nephrol. 2005, 16, 2134–2140. [Google Scholar] [CrossRef]
- Kang, H.T.; Shim, J.Y.; Lee, Y.J.; Lee, J.E.; Linton, J.A.; Kim, J.K.; Lee, H.R. Association between the ratio of triglycerides to high-density lipoprotein cholesterol and chronic kidney diseasein Korean adults: The 2005 Korean national hHealth and nutrition examination survey. Kidney Blood Press. Res. 2011, 34, 173–179. [Google Scholar] [CrossRef]
- Kim, J.Y.; Kang, H.T.; Lee, H.R.; Lee, Y.J.; Shim, J.Y. Comparison of lipid-related ratios for prediction of chronic kidney disease stage 3 or more in Korean adults. J. Korean Med. Sci. 2012, 27, 1524–1594. [Google Scholar] [CrossRef]
- Jiang, L.; Liang, Y.; Qiu, B.; Wang, F.; Duan, X.; Yang, X.; Yang, J.; Huang, W.; Wang, N. Metabolic syndrome and chronic kidney disease in a rural Chinese population. Clin. Chim. Acta. 2011, 412, 1983–1988. [Google Scholar] [CrossRef]
- Cheng, H.T.; Huang, J.W.; Chiang, C.K.; Yen, C.J.; Hung, K.Y.; Wu, K.D. Metabolic syndrome and insulin resistance as risk factors for development of chronic kidney disease and rapid decline in renal function in elderly. J. Clin. Endocrinol. Metab. 2012, 97, 1268–1276. [Google Scholar] [CrossRef]
- Chen, S.Y.; Chen, Y.M.; Liu, X.Y.; Li, M.; Wu, B.D.; Li, Y.Q.; Liang, Y.; Shao, X.; Holthöfer, H.; Zou, H. Association of insulin resistance with chronic kidney disease in non-diabetic subjects with normal weight. Plos One 2013, 8. [Google Scholar] [CrossRef]
- Liu, C.; Sempos, R.; Donahue, J.; Dorn, J.; Trevisan, M.; Grundy, S.M. Non-high-density lipoprotein and very-low-density lipoprotein cholesterol and their risk predictive values in coronary heart disease. Am. J. Cardiol. 2006, 98, 1363–1368. [Google Scholar] [CrossRef]
- Eliasson, B.; Cederholm, J.; Eeg-Olofsson, K.; Svensson, A.M.; Zethelius, B.; Gudbjörnsdottir, S. Clinical usefulness of different lipid measures for prediction of coronary heart disease intype 2 diabetes: A report from the Swedish national diabetes register. Diabetes Care 2011, 34, 2095–2100. [Google Scholar] [CrossRef]
- Joint Committee for Developing Chinese guidelines on prevention and treatment of dyslipidemia in adults. Chinese guidelines on prevention and treatment of dyslipidemia in adults. (In Chinese)Chin. J. Cardiol. 2007, 35, 390–419. [Google Scholar]
- Ma, Y.C.; Zuo, L.; Chen, J.H.; Luo, Q.; Yu, X.Q.; Li, Y.; Xu, J.; Huang, S.; Wang, L.; Huang, W. Modified glomerular filtration rate estimating equation for Chinese patients with chronic kidney disease. J. Am. Soc. Nephrol. 2006, 17, 2937–2944. [Google Scholar] [CrossRef]
- Kidney Disease: Improving Global Outcomes (KDIGO). KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. KidneyInt. Suppl. 2013, 3, S1–S150. [Google Scholar]
- Molarius, A.; Seidell, J.C.; Sans, S.; Tuomilehto, J.; Kuulasmaa, K. Waist and hip circumferences, and waist-hip ratio in 19 populations of the WHO MONICA Project. Int. J. Obes. Relat. Metab. Disord. 1999, 23, 116–125. [Google Scholar]
- Wheeler, D.C.; Fernando, R.L.; Gillett, M.P.; Zaruba, J.; Persaud, J.; Kingstone, D.; Varghese, Z.; Moorhead, J.F. Characterisation of the binding of low-density lipoproteins to cultured rat mesangial cells. Nephrol. Dial. Transpl. 1991, 6, 701–708. [Google Scholar] [CrossRef]
- Al-Shebeb, T.; Frohlich, J.; Magil, A.B. Glomerular disease in hypercholesterolemic guinea pigs: A pathogenetic study. Kidney Int. 1988, 33, 498–507. [Google Scholar] [CrossRef]
- Neverov, N.I.; Kaysen, G.A.; Nuccitelli, R.; Weiss, R.H. HDL causes mesangial cell mitogenesis through a tyrosine kinase-dependent receptor mechanism. J. Am. Soc. Nephrol. 1997, 8, 1247–1256. [Google Scholar]
- Hattori, M.; Nikolic-Paterson, D.J.; Miyazaki, K.; Isbel, N.M.; Lan, H.Y.; Atkins, R.C.; Kawaguchi, H.; Ito, K. Mechanisms of glomerular macrophage infiltration in lipid-induced renal injury. Kidney Int. Suppl. 1999, 71, S47–S50. [Google Scholar]
- Dominguez, J.H.; Tang, N.; Xu, W.; Evan, A.P.; Siakotos, A.N.; Agarwal, R.; Walsh, J.; Deeg, M.; Pratt, H.J.; March, K.L.; et al. Studies of renal injury III: Lipid-induced nephropathy in type II diabetes. Kidney Int. 2000, 57, 92–104. [Google Scholar] [CrossRef]
- Muntner, P.; Coresh, J.; Smith, J.C.; Eckfeldt, J.; Klag, M.J. Plasma lipids and risk of developing renal dysfunction: The atherosclerosis risk in communities study. Kidney Int. 2000, 58, 293–301. [Google Scholar] [CrossRef]
- Maddox, D.A.; Alavi, F.K.; Santella, R.N.; Zawada, E.T., Jr. Prevention of obesity-linked renal disease: Age-dependent effects of dietary food restriction. Kidney Int. 2002, 62, 208–219. [Google Scholar] [CrossRef]
- Abrass, C.K. Cellular lipid metabolism and the role of lipids in progressive renal disease. Am. J. Nephrol. 2004, 24, 46–53. [Google Scholar] [CrossRef]
- Trevisan, R.; Dodesini, A.R.; Lepore, G. Lipids and renal disease. J. Am. Soc. Nephrol. 2006, 17, S145–S147. [Google Scholar] [CrossRef]
- Ravid, M.; Brosh, D.; Ravid-Safran, D.; Levy, Z.; Rachmani, R. Main risk factors for nephropathy in type 2 diabetes mellitus are plasma cholesterol levels, mean blood pressure, and hyperglycemia. Arch. Intern. Med. 1998, 158, 998–1004. [Google Scholar] [CrossRef]
- Samuelsson, O.; Attman, P.O.; Knight-Gibson, C.; Larsson, R.; Mulec, H.; Weiss, L.; Alaupovic, P. Complex apolipoprotein B-containing lipoprotein particles are associated with a higher rate of progression of human chronic renal insufficiency. J. Am. Soc. Nephrol. 1998, 9, 1482–1488. [Google Scholar]
- Austin, M.A.; Hokanson, J.E. Epidemiology of triglycerides, small dense low-density lipoprotein, and lipoprotein (a) as risk factors for coronary heart disease. Med. Clin. North Am. 1994, 78, 99–115. [Google Scholar]
- Austin, M.A.; Breslow, J.L.; Hennekens, C.H.; Buring, J.L.; Willett, W.C.; Krauss, R.M. Low density lipoprotein subclass pattern and risk of myocardial infarction. JAMA 1988, 260, 1917–1921. [Google Scholar] [CrossRef]
- Tornvall, P.; Karpe, F.; Carlson, L.A.; Hamsten, A. Relationships of low density lipoprotein subfractions to angiographically defined coronary heart disease in young survivors of myocardial infarction. Atherosclerosis 1991, 90, 67–80. [Google Scholar] [CrossRef]
- Campos, H.; Genest, J.J., Jr; Blijlevens, E.; McNamara, J.R.; Jenner, J.L.; Ordovas, J.M.; Wilson, P.M.; Schaefer, E.J. Low density lipoprotein particle size and coronary artery disease. Arterioscler. Thromb. 1992, 12, 187–195. [Google Scholar]
- Coresh, J.; Kwiterovich, P.O., Jr; Smith, H.H.; Bachorik, P.S. Association of plasma triglyceride concentration and LDL particle diameter, density, and chemical composition with premature coronary artery disease in men and women. J. Lipid. Res. 1993, 34, 1687–1697. [Google Scholar]
- Lamarche, B.; Lemieux, I.; Després, J.P. The small, dense LDL phenotype and the risk of coronary heart disease: epidemiology, patho-physiology and therapeutic aspects. Diabetes Metab. 1999, 25, 199–211. [Google Scholar]
- Austin, M.A.; King, M.C.; Vranizan, K.M.; Krauss, R.M. Atherogenic lipoprotein phenotype. A proposed genetic marker for coronary heart disease risk. Circulation 1990, 82, 495–506. [Google Scholar] [CrossRef]
- Bhalodkar, N.C.; Blum, S.; Enas, E.A. Accuracy of the ratio of triglycerides to high-density lipoprotein cholesterol for predicting low-density lipoprotein cholesterol particle sizes, phenotype B, and particle concentrations among Asian Indians. Am. J. Cardiol. 2006, 97, 1007–1009. [Google Scholar] [CrossRef]
- Fan, X.; Liu, E.Y.; Hoffman, V.P.; Potts, A.J.; Sharma, B.; Henderson, D.C. Triglyceride/high-density lipoprotein cholesterol ratio: A surrogate to predict insulin resistance and low-density lipoprotein cholesterol particle size in nondiabetic patients with schizophrenia. J. Clin. Psychiatry 2011, 72, 806–812. [Google Scholar] [CrossRef]
- Onat, A.; Can, G.; Kaya, H.; Hergenç, G. “Atherogenic index of plasma” (log10 triglyceride/high-density lipoprotein-cholesterol) predicts high blood pressure, diabetes, and vascular events. Clin. Lipidol. 2010, 4, 89–98. [Google Scholar] [CrossRef]
- Shepherd, J.; Kastelein, J.J.; Bittner, V.; Deedwania, P.; Breazna, A.; Dobson, S.; Zuckerman, A.; Wenger, N.K.; For the Treating to New Targets Investigators. Effect of intensive lipid lowering with atorvastatin on renal function in patients with coronary heart disease: the Treating to New Targets (TNT) study. Am. J. Kidney Dis. 1998, 32, S142–S156. [Google Scholar]
- Athyros, V.G.; Mikhailidis, D.P.; Papageorgiou, A.A.; Symeonidis, A.N.; Pehlivanidis, A.N.; Bouloukos, V.I.; Elisaf, M. The effect of statins versus untreated dyslipidaemia on renal function in patients with coronary heart disease. A subgroup analysis of the Greek atorvastatin and coronary heart disease evaluation (GREACE) study. J. Clin. Pathol. 2004, 57, 728–734. [Google Scholar] [CrossRef]
- Bianchi, S.; Bigazzi, R.; Caiazza, A.; Campese, V.M. A controlled, prospective study of the effects of atorvastatin on proteinuria and progression of kidney disease. Clin. J. Am. Soc. Nephrol. 2007, 2, 1131–1139. [Google Scholar] [CrossRef]
- Koren, M.J.; Davidson, M.H.; Wilson, D.J.; Fayyad, R.S.; Zuckerman, A.; Reed, D.P.; ALLIANCE Investigators. Focused atorvastatin therapy in managed-care patients with coronary heart disease and CKD. Am. J. Kidney Dis. 2009, 53, 741–750. [Google Scholar]
- National Cholesterol Education Program (NCEP) Expert Panel on Detection Ea, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third report of the national cholesterol education program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult Treatment Panel III) final report. Circulation 2002, 106, 3143–3421. [Google Scholar]
- Kasiske, B. Hyperlipidemia in patients with chronic renal disease. Am. J. Kidney Dis. 1998, 32, S142–S156. [Google Scholar] [CrossRef]
- Wanner, C. Importance of hyperlipidaemia and therapy in renal patients. Nephrol. Dial. Transpl. 2000, 15, 92–96. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Zhang, L.; Yuan, Z.; Chen, W.; Chen, S.; Liu, X.; Liang, Y.; Shao, X.; Zou, H. Serum Lipid Profiles, Lipid Ratios and Chronic Kidney Disease in a Chinese Population. Int. J. Environ. Res. Public Health 2014, 11, 7622-7635. https://doi.org/10.3390/ijerph110807622
Zhang L, Yuan Z, Chen W, Chen S, Liu X, Liang Y, Shao X, Zou H. Serum Lipid Profiles, Lipid Ratios and Chronic Kidney Disease in a Chinese Population. International Journal of Environmental Research and Public Health. 2014; 11(8):7622-7635. https://doi.org/10.3390/ijerph110807622
Chicago/Turabian StyleZhang, Liying, Zhiyong Yuan, Wu Chen, Shanying Chen, Xinyu Liu, Yan Liang, Xiaofei Shao, and Hequn Zou. 2014. "Serum Lipid Profiles, Lipid Ratios and Chronic Kidney Disease in a Chinese Population" International Journal of Environmental Research and Public Health 11, no. 8: 7622-7635. https://doi.org/10.3390/ijerph110807622
APA StyleZhang, L., Yuan, Z., Chen, W., Chen, S., Liu, X., Liang, Y., Shao, X., & Zou, H. (2014). Serum Lipid Profiles, Lipid Ratios and Chronic Kidney Disease in a Chinese Population. International Journal of Environmental Research and Public Health, 11(8), 7622-7635. https://doi.org/10.3390/ijerph110807622