The Impact of the FIFA 11+ Training Program on Injury Prevention in Football Players: A Systematic Review


 ,
, 
Abstract
:1. Introduction
2. Material and Methods
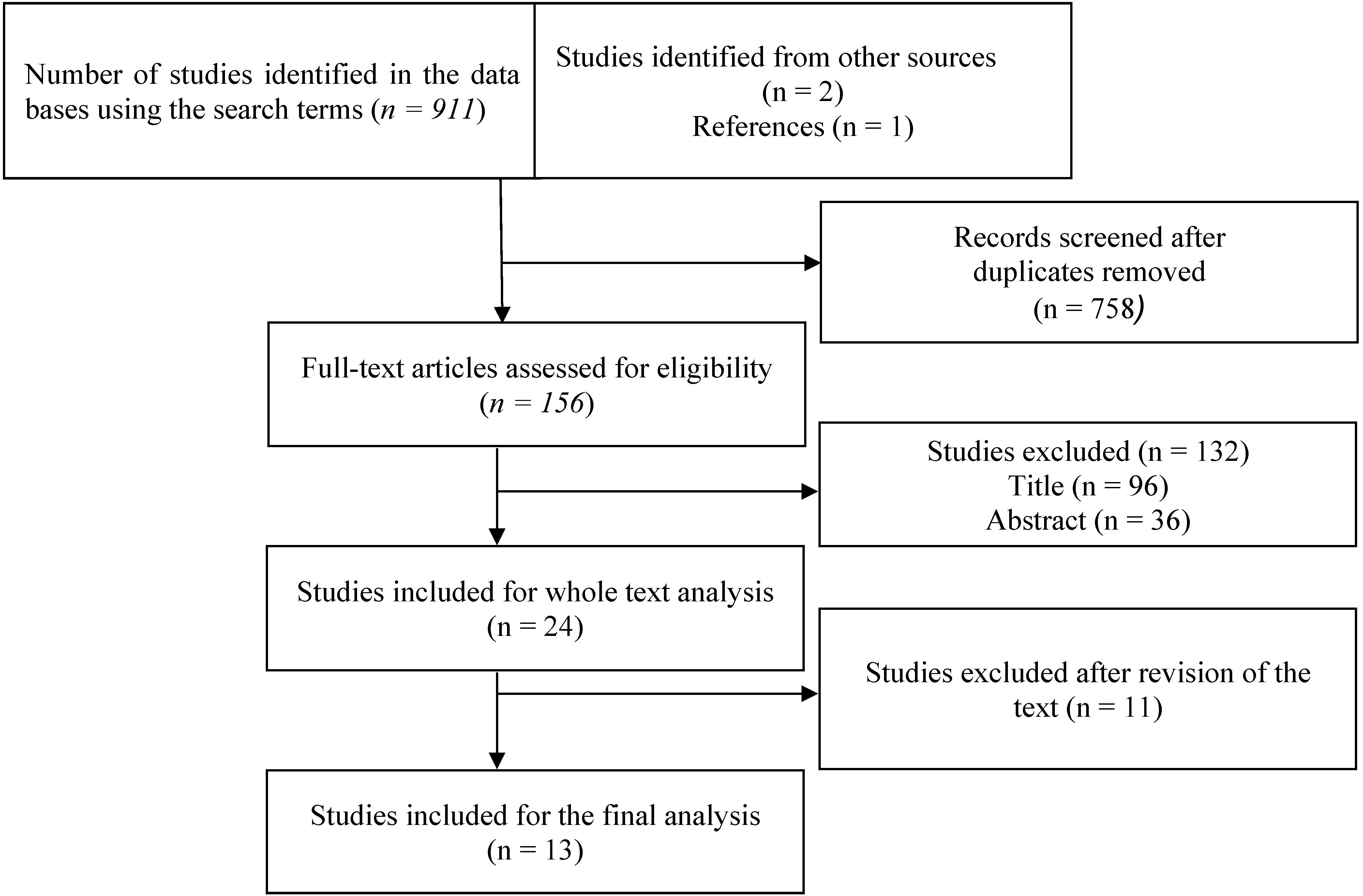
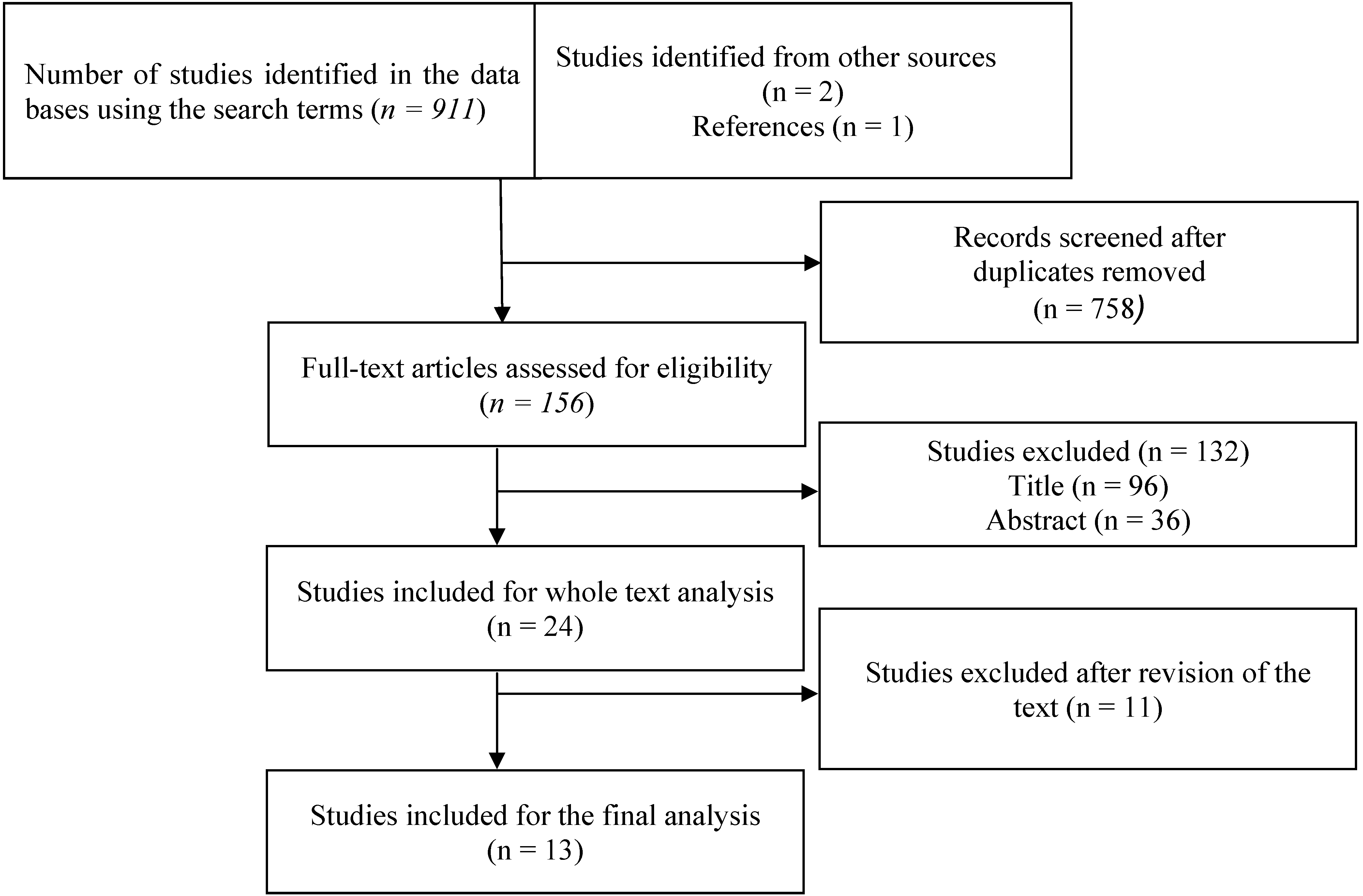
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria

{kind=link}
| PICO Indicators | Results according PICO |
|---|---|
| Design | Clinical trials and observational studies (cohort and case-control designs) |
| Population | Participants (both male and female) without restriction to a particular age (adolescents, sport players and amateur) |
| Intervention | FIFA 11+ |
| Comparisons | Conventional or no warm up |
| Outcome measures | Injury-Incidence rate |
| Neuromuscular performance changes | |
| Cost-effectiveness | |
| Compliance and method of delivery |
2.3. Quality Assessment of the Studies
3. Results
| Source, Year | Participants | Design | Outcomes | Duration, Frequency and Intensity of the Intervention. Period of Implementation | Results |
|---|---|---|---|---|---|
| Hammes et al. [29], 2014 | Male veteran football players (n = 265), mean age 45 years | Randomized controlled trial | Player exposure hours and injuries | Duration: 20 min; Frequency: once/week for 9 months | No significant difference was found between intervention and control group in overall injury incidence (incidence rate ratio (IRR: 0.91 (0.64–1.48); p = 0.89). Only severe injuries reached statistical significance with higher incidence in the control group (IRR: 0.46 (0.21–0.97), p = 0.04) |
| Grooms et al. [30], 2013 | Male collegiate football players (n = 41) 18–25 years-of-age | Cohort study | Lower extremity injury risk and time lost to lower extremity injury | Duration: 20 min; Frequency: 5–6 times/week for 2 seasons | The intervention season had reductions in the relative risk (RR) of lower extremity injury of 72% (RR 1 = 0.28; 95% CI 2 0.09–0.85) and time lost to lower extremity injury compared to the previous non-intervention season |
| Steffen et al. [31], 2013 | Female youth football players (n = 226) 13–18 years-of-age | Randomized controlled trial | Incidence of all injuries; Neuromuscular performance tests included the Star Excursion Balance Test (SEBT), single-leg balance, triple hop and jumping-over-a-bar | Duration: 20 min; Frequency: 2–3 times/week for 4.5 months | Compared to players with low adherence, players with high adherence to the 11+ had a 57% lower injury risk (RR = 0.43; 95% CI 0.19–1.00). However, after adjusting for covariates, this between group difference was not statistically significant RR = 0.44; 95% CI 0.18–1.06) |
| Soligard et al. [25], 2010 | Young female football players (n = 1.055) 13–17 years-of-age | Cohort study | Compliance, injury incidence | Duration: 20 min; Frequency: 1.3 times/week for 10 months | Coaches who had previously utilized injury prevention training coached teams with a 46% lower risk of injury (OR = 0.54; 95% CI 0.33–0.87). Compared with players with intermediate compliance, players with high compliance with the program had a 35% lower risk of all injuries (RR = 0.65; 95% CI 0.46–0.91) |
| Soligard et al. [27], 2008 | Young female football players (n = 2.729) 13–17 years-of-age | Randomized controlled trial | Lower extremity injuries (foot, ankle, lower leg, knee, thigh, groin, and hip) | Duration: 20 min; Frequency: 3 times/week for 8 months | In the intervention group there was a significantly lower risk of injuries overall (RR = 0.68; 95% CI 0.48–0.98), lower risk of overuse injuries (RR = 0.47, 95% CI 0.26–0.85) and lower risk of severe injuries (RR = 0.55, 95% CI 0.36–0.83) compared to the control group |
| Steffen et al. [28], 2008 | Young female football players (n = 396) 13–17 years-of-age | Randomized controlled trial | Injury incidence and type | Duration: 20 min; Frequency: once/week for 8 months | No effect of the intervention on injury incidence |
| Source, Year | Participants | Design | Outcome | Duration, Frequency and Intensity of the Intervention. Period of Implementation | Results |
|---|---|---|---|---|---|
| Bizzini et al. [23], 2013 | Male amateur football players (n = 20), mean age 25.5 years | Cohort study. ACUTE effects | Acute effects of the FIFA 11+ on performance in 20-m sprints, agility t-test, counter- movement jump, squat jump, star excursion balance test and stiffness, quadriceps maximal isometric strength (MVC) and rate of force development (RFD) | Duration: 20 min | Statistically significant changes were found for all the performance variables with the exception of quadriceps MVC and RFD. Significant increases in resting oxygen uptake, core temperature and blood lactate |
| Impellizzeri et al. [24], 2013 | Male amateur football players (n = 81), mean age 24 years | Randomized controlled trial | Primary: Dynamic balance: Time-to-stabilization, star excursion balance test, eccentric/concentric flexors strength, core-stability test, vertical jump, 20-m sprint, agility t-test | Duration: 20 min; Frequency: 3 times/week for 9 weeks | Statistically significant improvement in time-to-stabilization (−2.8%; 90% CI −4.4–−1.2) and core-stability (−8.9%, 90% CI −14.6–−3.1) in the intervention group compared to the control group. Meaningful but non-significant improvements were observed in eccentric and concentric flexor strength |
| Nakase et al. [33], 2013 | Healthy male volunteers (n = 10), mean age: 19 years | Explorative study. ACUTE effects | Acute effect of FIFA 11+ on fluorodeoxy-glucose (FDG) uptake of muscle tissue per unit volume (marker of muscle glucose intake and activation) | Duration: 20 min | Significantly higher FDG accumulation in the rectus abdominus, gluteus medius and gluteus minimus muscles following the FIFA 11+ than in a non-exercising control group |
| Daneshjoo et al. [34], 2012 | Young male professional football players (n = 36), mean age 19 years | Randomized controlled trial | Chronic effect of FIFA 11+ on concentric hamstrings:quadriceps ratio (Conventional strength ratio (CSR)), Eccentric hamstrings: concentric quadriceps ratio (Dynamic control ratio (DCR)), and fast:slow speed ratio (FSR) (net peak torque at 300°∙s−1/net peaktorque at 60°∙s−1) of the hamstrings and quadriceps | Duration: 20 min; Frequency: 3 times/week for 2 months | Significant increases in DCR in the dominant and non-dominant limb were observed after the 11+ training. In the non-dominant limb, significant improvements were observed in the CSR at 60°∙s−1 (but not at 180°∙s−1 or 300°∙s−1) and in the FSR of the quadriceps (but not in the hamstrings) |
| Daneshjoo et al. [34], 2012 | Under 21 year-old football players (n = 36), mean age 19 years | Randomized controlled trial | Joint positioning (proprioception) at 30°, 45° and 60° knee flexion. Stork stand test (Static balance) and SEBT (Dynamic balance) | Duration: 20 min; Frequency: 3 times/week for 2 months | Compared to control players who maintained normal activities The program significantly improved joint proprioception at 45° and 60° of knee flexion in the dominant leg and static and dynamic balance |
| Brito et al., [26], 2010 | Sub-elitemale football players (n = 20), mean age 22 years | Cohort study | Isokinetic hamstrings and quadriceps peak torque (PT) | Duration: 20 min; Frequency: 3 times/week for 10 weeks | Hamstrings PT in the non-dominant limb significantly increased by 14.6%, 15.0% and 14.3% during the above contractions/velocities, respectively. In the dominant limb, the concentric PT of the quadriceps increased by 6.9% at 60∙s−1, and 8.3% at 180∙s−1, whereas that of the hamstrings increased by 20.4% at 60∙s−1. The training program significantly increased the Hcon: Qcon ratio at 60∙s−1 by 14.8% and the Hecc: Qcon ratio by 13.8% in the non-dominant limb |
| Source, year | Participants | Design | Outcome | Duration, Frequency and Intensity of the Intervention. Period of Implementation | Results |
|---|---|---|---|---|---|
| Steffen et al. [32], 2013 | Female youth football players (n = 226) 13–18 years-of-age | Randomized controlled trial | Comparison of different delivery methods of FIFA 11+ on adherence among female youth football teams | Duration: 20 min; Frequency: 3 times/week for 4 months | Following a workshop delivery of the FIFA 11+ by coaches who had attended a workshop was equally successful with or without the additional field involvement of a physio-therapist. Proper education of coaches during an extensive preseason workshop followed by supervised delivery by these coaches resulted in significantly higher team adherence than an unsupervised delivery of the FIFA 11+ |
| Soligard et al. [25], 2010 | Young female football players (n = 1.055), 13–17 years-of-age | Cohort study | Interaction between compliance with program and injury incidence | Duration: 20 min; Frequency: 2 times/week for 8 months | Compared with players with intermediate compliance, players with high compliance with the program had a 35% lower risk of all injuries (RR = 0.65; 95% CI 0.46–0.91) |
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Federation International of Football Association (FIFA). FIFA Big Count 2006: 270 Million People Active in Football; FIFA Communications Division Information Services: Zurich, Switzerland, 2007. [Google Scholar]
- Junge, A.; Dvorak, J. Soccer injuries: A review on incidence and prevention. Sport. Med. 2004, 34, 929–938. [Google Scholar] [CrossRef]
- Woods, C.; Hawkins, R.; Hulse, M.; Hodson, A. The football association medical research programme: An audit of injuries in professional football—Analysis of preseason injuries. Brit. J. Sport. Med. 2002, 36, 436–441. [Google Scholar] [CrossRef]
- Junge, A.; Lamprecht, M.; Stamm, H.; Hasler, H.; Bizzini, M.; Tschopp, M.; Reuter, H.; Wyss, H.; Chilvers, C.; Dvorak, J. Countrywide campaign to prevent soccer injuries in Swiss amateur players. Amer. J. Sport. Med. 2011, 36, 57–63. [Google Scholar] [CrossRef]
- Letsellast Model 2008; Consumer Safety Institute: Amsterdam, the Netherlands; Erasmus Medical Center: Rotterdam, the Netherlands, 2010. (in Dutch)
- Faude, O.; Rößler, R.; Junge, A. Football injuries in children and adolescent players: Are there clues for prevention? Sport. Med. 2013, 43, 819–837. [Google Scholar] [CrossRef]
- Majewski, M.; Susanne, H.; Klaus, S. Epidemiology of athletic knee injuries: A 10-year study. Knee 2006, 13, 184–188. [Google Scholar] [CrossRef] [PubMed]
- Krustrup, P.; Hansen, P.R.; Andersen, L.J.; Jakobsen, M.D.; Sundstrup, E.; Randers, M.B.; Christiansen, L.; Helge, E.W.; Pedersen, M.T.; Søgaard, P.; et al. Long-term musculoskeletal and cardiac health effects of recreational football and running for premenopausal women. Scand. J. Med. Sci. Sports 2010, 20, S80–S89. [Google Scholar]
- Randers, M.B.; Nielsen, J.J.; Krustrup, B.R.; Sundstrup, E.; Jakobsen, M.D.; Nybo, L.; Dvorak, J.; Bangsbo, J.; Krustrup, P. Positive performance and health effects of a football training program over 12 weeks can be maintained over a 1-year period with reduced training frequency. Scand. J. Med. Sci. Sports 2010, 20, S80–S89. [Google Scholar] [CrossRef]
- Alentorn-Geli, E.; Myer, G.D.; Silvers, H.J.; Samitier, G.; Romero, D.; Lázaro-Haro, C.; Cugat, R. Prevention of non-contact anterior cruciate ligament injuries in soccer players. Part 1: Mechanisms of injury and underlying risk factors. Knee Surg. Sports Traumatol. Arthrosc. 2009, 17, 705–729. [Google Scholar] [CrossRef] [PubMed]
- Mendiguchia, J.; Alentorn-Geli, E.; Brughelli, M. Hamstring strain injuries: Are we heading in the right direction? Brit. J. Sport. Med. 2012, 46, 81–85. [Google Scholar] [CrossRef]
- McHugh, M.P. Injury prevention in professional sports: protecting your investments. Scand. J. Med. Sci. Sports 2009, 19, 751–752. [Google Scholar] [CrossRef] [PubMed]
- Dvorak, J.; Junge, A.; Chomiak, J.; Graf-Baumann, T.; Peterson, L.; Rosch, D.; Hodgson, R. Risk factor analysis for injuries in football players. Possibilities for a prevention program. Amer. J. Sport. Med. 2000, 28, S69–S74. [Google Scholar]
- Ekstrand, J.; Gillquist, J.; Liljedahl, S.O. Prevention of soccer injuries. Supervision by doctor and physiotherapist. Amer. J. Sport. Med. 1983, 11, 116–120. [Google Scholar] [CrossRef]
- Krist, M.R.; van Beijsterveldt, A.M.; Backx, F.J.; de Wit, G.A. Preventive exercises reduced injury-related costs among adult male amateur soccer players: A cluster-randomised trial. J. Physiother. 2013, 59, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Verhagen, E.A. Costing an injury prevention program in amateur adult soccer. Clin. J. Sport. Med. 2013, 23, 500–501. [Google Scholar] [CrossRef] [PubMed]
- Gatterer, H.; Ruedl, G.; Faulhaber, M.; Regele, M.; Burtscher, M. Effects of the performance level and the FIFA “The 11” injury prevention program on the injury rate in Italian male amateur soccer players. J. Sports Med. Phys. Fitness. 2012, 52, 80–84. [Google Scholar] [PubMed]
- Van Beijsterveldt, A.M.; van de Port, I.G.; Krist, M.R.; Schmikli, S.L.; Stubbe, J.H.; Frederiks, J.E.; Backx, F.J. Effectiveness of an injury prevention programme for adult male amateur soccer players: A cluster-randomised controlled trial. Brit. J. Sports Med. 2012, 46, 1114–1118. [Google Scholar] [CrossRef]
- Kilding, A.E.; Tunstall, H.; Kuzmic, D. Suitability of FIFA’s “The 11” training programme for young football players—Impact on physical performance. J. Sport. Sci. Med. 2008, 7, 320–326. [Google Scholar]
- De Morton, N. The PEDro scale is a valid measure of the methodological quality of clinical trials: A demographic study. Aust. J. Physiother. 2009, 55, 129–133. [Google Scholar] [CrossRef] [PubMed]
- Public Health Resource Unit. Critical Appraisal Skills Programme (CASP). Available online: http://www.phru.nhs.uk/ Pages/PHD/CASP.htm (accessed on 8 August 2008).
- Daneshjoo, A.; Mokhtar, A.H.; Rahnama, N.; Yusof, A. The effects of injury preventive warm-up programs on knee strength ratio in young male professional soccer players. PLoS One 2012, 7. [Google Scholar] [CrossRef]
- Bizzini, M.; Impellizzeri, F.M.; Dvorak, J.; Bortolan, L.; Schena, F.; Modena, R.; Junge, A. Physiological and performance responses to the “FIFA 11+” (part 1): Is it an appropriate warm-up? J. Sport. Sci. 2013, 31, 1481–1490. [Google Scholar] [CrossRef]
- Impellizzeri, F.M.; Bizzini, M.; Dvorak, J.; Pellegrini, B.; Schena, F.; Junge, A. Physiological and performance responses to the FIFA 11+ (Part 2): A randomised controlled trial on the training effects. J. Sport. Sci. 2013, 31, 1491–1502. [Google Scholar] [CrossRef]
- Soligard, T.; Nilstad, A.; Steffen, K.; Myklebust, G.; Holme, I.; Dvorak, J.; Bahr, R.; Andersen, T.E. Compliance with a comprehensive warm-up programme to prevent injuries in youth football. Brit. J. Sport. Med. 2010, 44, 787–793. [Google Scholar] [CrossRef]
- Brito, J.; Figueiredo, P.; Fernandes, L.; Seabra, A.; Soares, J.M.; Krustrup, P.; Rebelo, A. Isokinetic strength effects of FIFA’s “the 11+” injury prevention training programme. Isokinet. Exerc. Sci. 2010, 18, 211–215. [Google Scholar]
- Soligard, T.; Myklebust, G.; Steffen, K.; Holme, I.; Silvers, H.; Bizzini, M.; Junge, A.; Dvorak, J.; Bahr, R.; Andersen, T.E. Comprehensive warm-up programme to prevent injuries in young female footballers: cluster randomised controlled trial. BMJ 2008, 337. [Google Scholar] [CrossRef]
- Steffen, K.; Myklebust, G.; Olsen, O.E.; Holme, I.; Bahr, R. Preventing injuries in female youth football—A cluster-randomized controlled trial. Scand. J. Med. Sci. Sports 2008, 18, 605–614. [Google Scholar] [CrossRef] [PubMed]
- Hammes, D.; Aus der Fünten, K.; Kaiser, S.; Frisen, E.; Bizzini, M.; Meyer, T. Injury prevention in male veteran football players—A randomised controlled trial using “FIFA 11+”. J. Sport. Sci. 2014. [Google Scholar] [CrossRef]
- Grooms, D.R.; Palmer, T.; Onate, J.A.; Myer, G.; Grindstaff, T. Comprehensive soccer-specific warm-up and lower extremity injury in collegiate male soccer players. J. Athl. Training 2013, 48, 782–789. [Google Scholar] [CrossRef]
- Steffen, K.; Emery, C.A.; Romiti, M.; Kang, J.; Bizzini, M.; Dvorak, J.; Finch, C.F.; Meeuwisse, W.H. High adherence to a neuromuscular injury prevention programme (FIFA 11+) improves functional balance and reduces injury risk in Canadian youth female football players: A cluster randomized trial. Brit. J. Sport. Med. 2013, 47, 794–802. [Google Scholar] [CrossRef]
- Steffen, K.; Meeuwisse, W.H.; Romiti, M.; Kang, J.; McKay, C.; Bizzini, M.; Dvorak, J.; Finch, C.; Myklebust, G.; Emery, C.A. Evaluation of how different implementation strategies of an injury prevention programme (FIFA 11+) impact team adherence and injury risk in Canadian female youth football players: A cluster-randomised trial. Brit. J. Sport. Med. 2013, 47, 480–487. [Google Scholar] [CrossRef]
- Nakase, J.; Inaki, A.; Mochizuki, T.; Toratani, T.; Kosaka, M.; Ohashi, Y.; Taki, J.; Yahata, T.; Kinuya, S.; Tsuchiya, H. Whole body muscle activity during the FIFA 11+ program evaluated by positron emission tomography. PLoS One 2013, 8. [Google Scholar] [CrossRef] [PubMed]
- Daneshjoo, A.; Mokhtar, A.H.; Rahnama, N.; Yusof, A. The effects of comprehensive warm-up programs on proprioception, static and dynamic balance on male soccer players. PLoS One 2012, 7. [Google Scholar] [CrossRef]
- Zazulak, B.T.; Hewett, T.E.; Reeves, N.P.; Goldberg, B.; Cholewicki, J. Deficits in neuromuscular control of the trunk predict knee injury risk: A prospective biomechanical-epidemiologic study. Amer. J. Sport. Med. 2007, 35, 1123–1130. [Google Scholar] [CrossRef]
- Frank, B.; Bell, D.R.; Norcross, M.F.; Blackburn, J.T.; Goerger, B.M.; Padua, D.A. Trunk and hip biomechanics influence anterior cruciate loading mechanisms in physically active participants. Amer. J. Sport. Med. 2013, 41, 2676–2683. [Google Scholar] [CrossRef]
- Waldén, M.; Atroshi, I.; Magnusson, H.; Wagner, P.; Hägglund, M. Prevention of acute knee injuries in adolescent female football players: Cluster randomised controlled trial. BMJ 2012, 344. [Google Scholar] [CrossRef] [PubMed]
- Kirkendall, D.T.; Junge, A.; Dvorak, J. Prevention of football injuries. Asian J. Sport. Med. 2010, 1, 81–92. [Google Scholar]
- Gilchrist, J.; Mandelbaum, B.R.; Melancon, H.; Ryan, G.W.; Silvers, H.J.; Griffin, L.Y.; Watanabe, D.S.; Dick, R.W.; Dvorak, J. A randomized controlled trial to prevent non-contact anterior cruciate ligament injury in female collegiate soccer players. Amer. J. Sport. Med. 2008, 36, 1476–1483. [Google Scholar] [CrossRef]
- Kiani, A.; Hellquist, E.; Ahlqvist, K.; Gedeborg, R.; Michaelsson, K.; Byberg, L. Prevention of soccer-related knee injuries in teenaged girls. Arch. Intern. Med. 2010, 170, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Wingfield, K. Neuromuscular training to prevent knee injuries in adolescent female soccer players. Clin. J. Sport. Med. 2013, 23, 407–408. [Google Scholar] [CrossRef] [PubMed]
- Faude, O.; Junge, A.; Kindermann, W.; Dvorak, J. Risk factors for injuries in elite female soccer players. Brit. J. Sport. Med. 2006, 40, 785–790. [Google Scholar] [CrossRef]
- Hägglund, M.; Waldén, M.; Ekstrand, J. Injuries among male and female elite football players. Scand. J. Med. Sci. Sports 2009, 19, 819–827. [Google Scholar] [CrossRef] [PubMed]
- Chomiak, J.; Junge, A.; Peterson, L.; Dvorak, J. Severe injuries in football players: Influencing factors. Amer. J. Sport. Med. 2000, 28, S58–S68. [Google Scholar]
- Peterson, L.; Junge, A.; Chomiak, J.; Graf-Baumann, T.; Dvorak, J. Incidence of football injuries and complaints in different age groups and skill-level groups. Amer. J. Sport. Med 2000, 28, S51–S57. [Google Scholar]
- Orchard, J.W.; Waldén, M.; Hägglund, M.; Orchard, J.J.; Chivers, I.; Seward, H.; Ekstrand, J. Comparison of injury incidences between football teams playing in different climatic regions. J. Sport. Med. 2013, 4, 251–260. [Google Scholar]
- Padua, D.A.; DiStefano, L.J.; Marshall, S.W.; Beutler, A.I.; de la Motte, S.J.; DiStefano, M.J. Retention of movement pattern changes after a lower extremity injury prevention program is affected by program duration. Amer. J. Sport. Med. 2012, 40, 300–306. [Google Scholar] [CrossRef]
- Bizzini, M.; Junge, A.; Dvorak, J. Implementation of the FIFA 11+ football warm up program: How to approach and convince the football associations to invest in prevention. Brit. J. Sport. Med. 2013, 47, 803–806. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barengo, N.C.; Meneses-Echávez, J.F.; Ramírez-Vélez, R.; Cohen, D.D.; Tovar, G.; Bautista, J.E.C. The Impact of the FIFA 11+ Training Program on Injury Prevention in Football Players: A Systematic Review. Int. J. Environ. Res. Public Health 2014, 11, 11986-12000. https://doi.org/10.3390/ijerph111111986
Barengo NC, Meneses-Echávez JF, Ramírez-Vélez R, Cohen DD, Tovar G, Bautista JEC. The Impact of the FIFA 11+ Training Program on Injury Prevention in Football Players: A Systematic Review. International Journal of Environmental Research and Public Health. 2014; 11(11):11986-12000. https://doi.org/10.3390/ijerph111111986
Chicago/Turabian StyleBarengo, Noël C., José Francisco Meneses-Echávez, Robinson Ramírez-Vélez, Daniel Dylan Cohen, Gustavo Tovar, and Jorge Enrique Correa Bautista. 2014. "The Impact of the FIFA 11+ Training Program on Injury Prevention in Football Players: A Systematic Review" International Journal of Environmental Research and Public Health 11, no. 11: 11986-12000. https://doi.org/10.3390/ijerph111111986
APA StyleBarengo, N. C., Meneses-Echávez, J. F., Ramírez-Vélez, R., Cohen, D. D., Tovar, G., & Bautista, J. E. C. (2014). The Impact of the FIFA 11+ Training Program on Injury Prevention in Football Players: A Systematic Review. International Journal of Environmental Research and Public Health, 11(11), 11986-12000. https://doi.org/10.3390/ijerph111111986