A Simple Microbiological Tool to Evaluate the Effect of Environmental Health Interventions on Hand Contamination

Abstract
:
1. Introduction
2. Experimental Section
2.1. Study Settings and Populations
2.1.1. India (Recontamination Study and Cross Sectional Study)
2.1.2. Mozambique (Cross Sectional Study)
2.2. Microbiological Sampling and Processing
2.3. Statistical Analysis
3. Results and Discussion
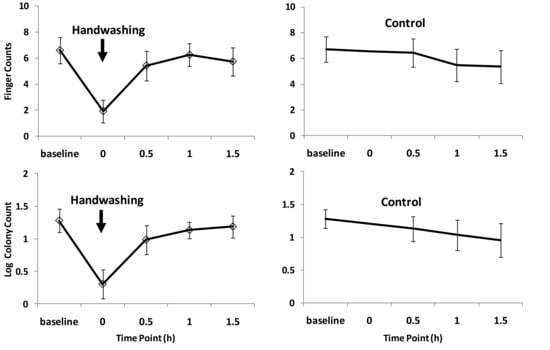
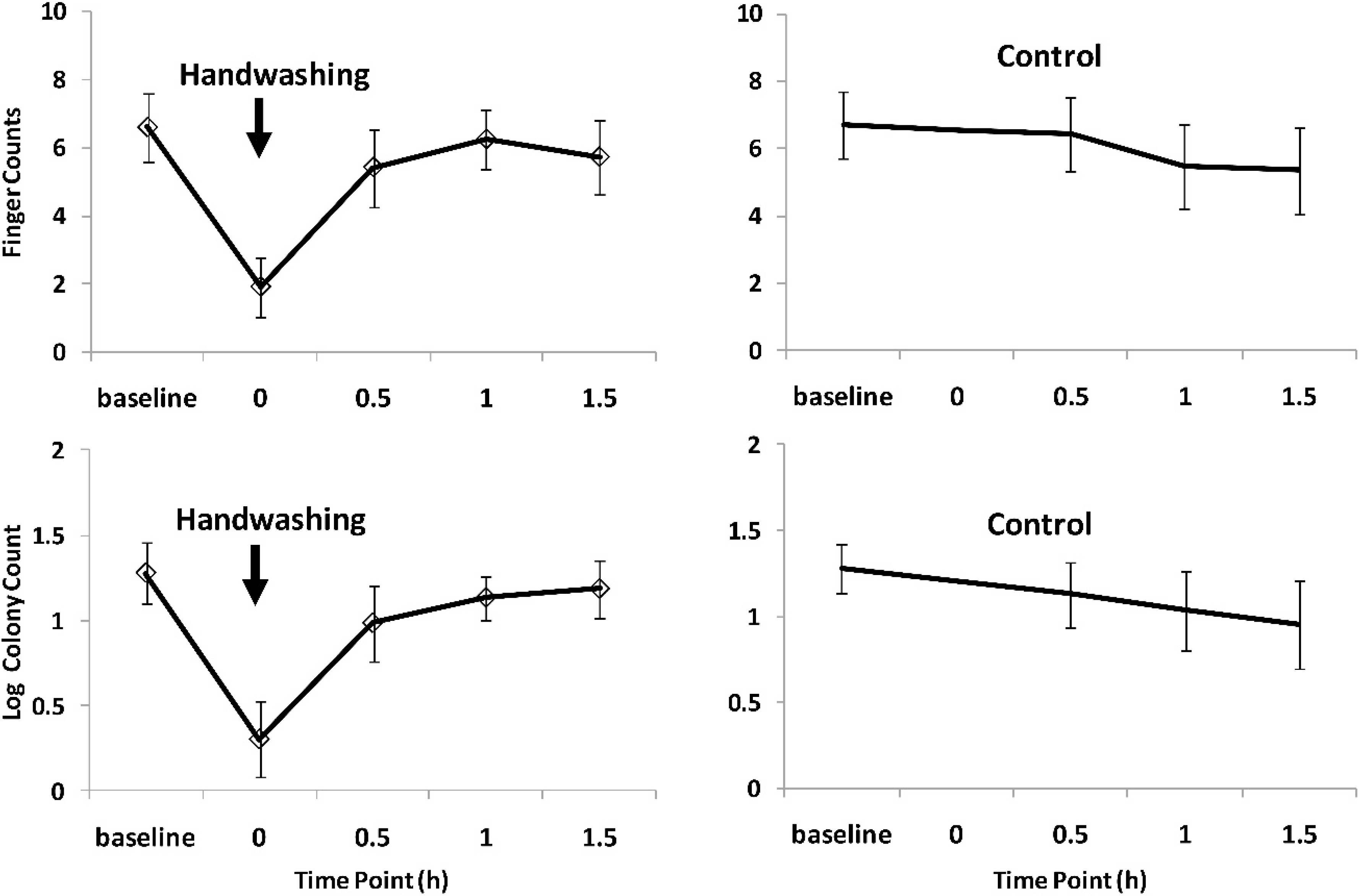
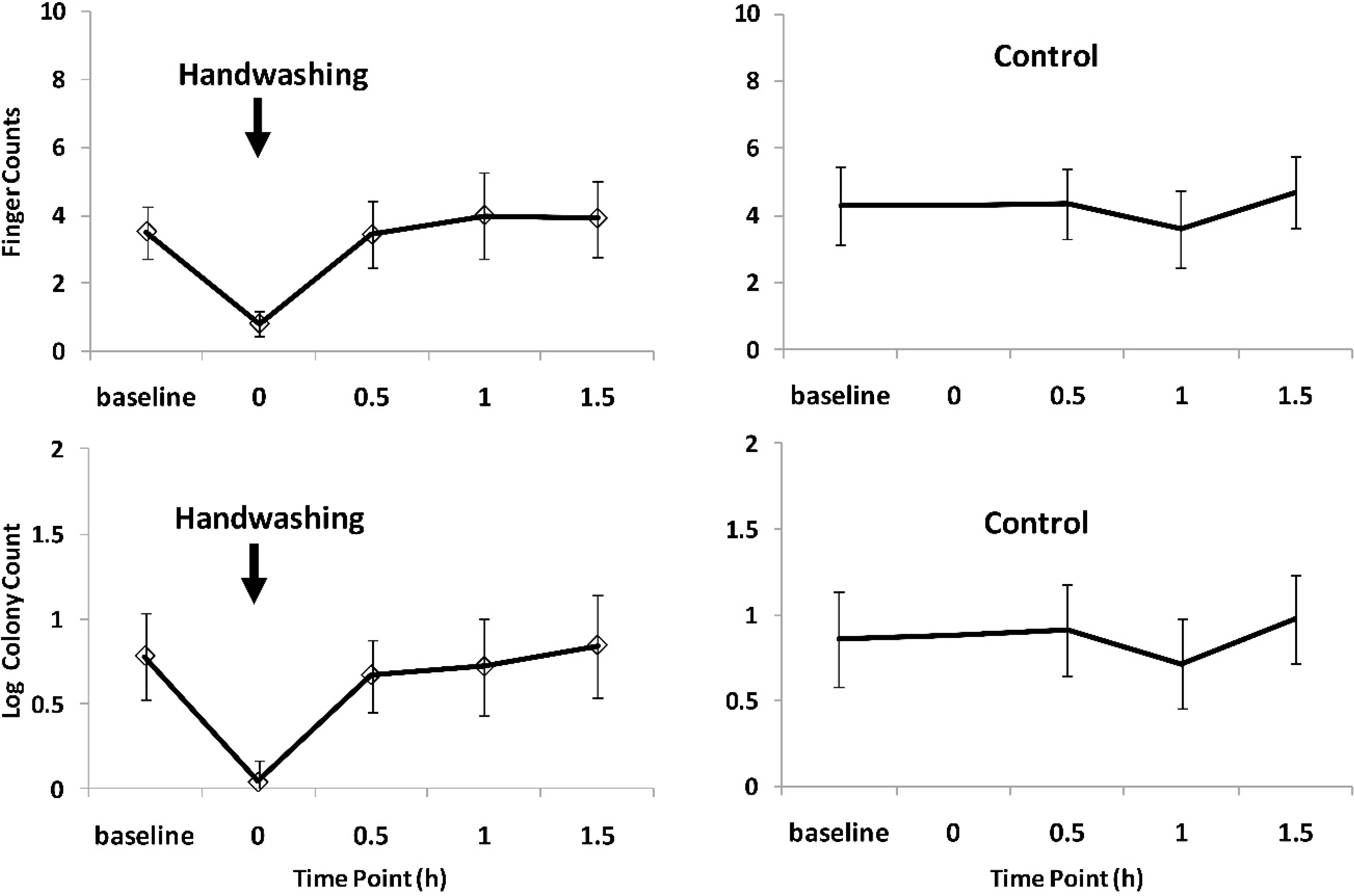
3.1. Longitudinal Recontamination Study

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Time Point | Difference in Mean Finger Counts and Mean Log Colony Counts between Hand Washing and Control ( p-Value) * | |||
|---|---|---|---|---|
| Enterococcus FC | Enterococcus LogCC | E. coli FC | E. coli LogCC | |
| Baseline | −0.87 (0.89) | −0.002 (0.98) | −0.78 (0.11) | −0.08 (0.63) |
| 0.5 h | −0.96 (0.19) | −0.15 (0.26) | −0.72 (0.32) | −0.22 (0.19) |
| 1 h | 0.80 (0.29) | 0.10 (0.43) | 0.52 (0.54) | 0.02 (0.92) |
| 1.5 h | 0.43 (0.59) | 0.23 (0.10) | −0.52 (0.49) | −0.11 (0.57) |
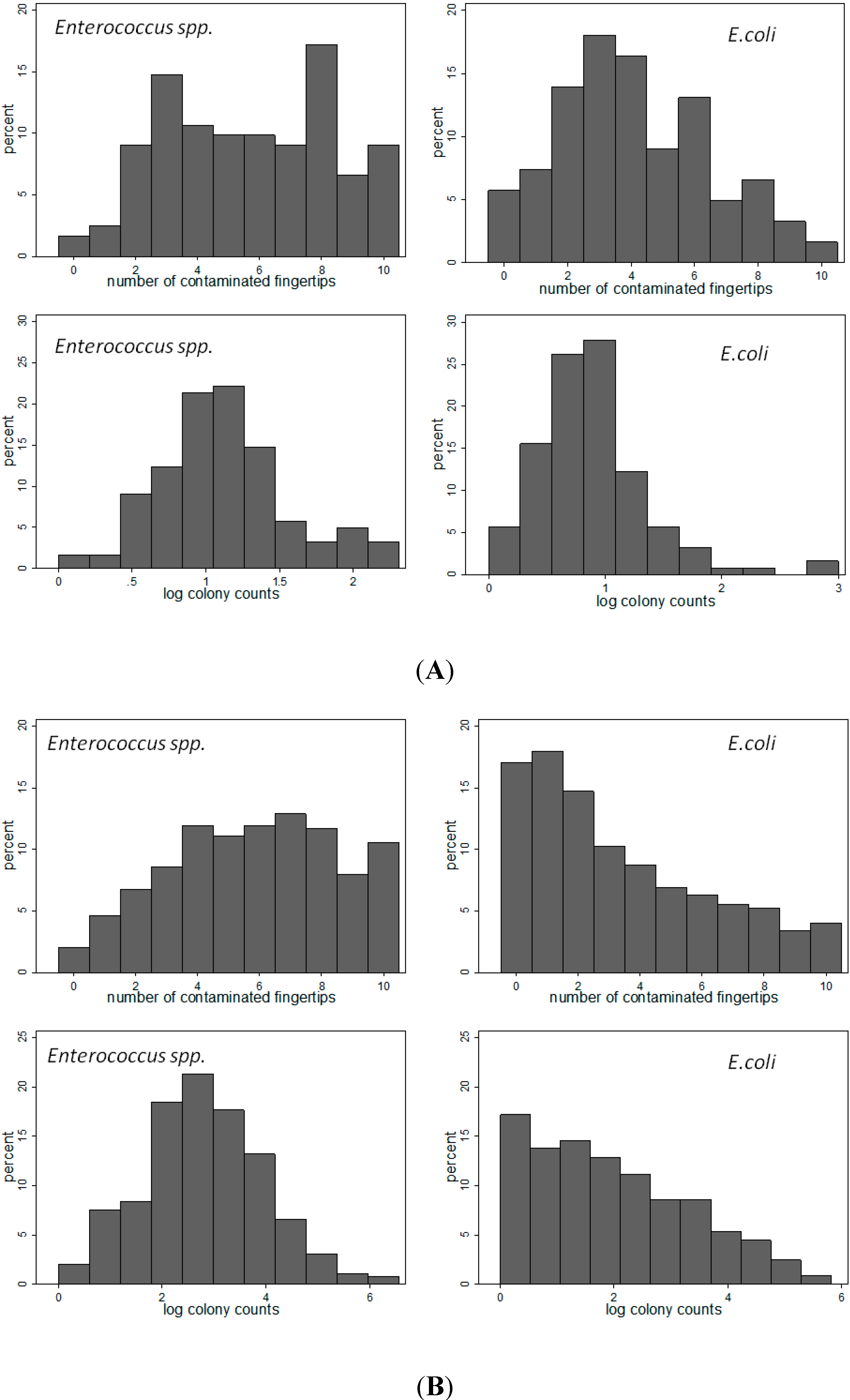
3.2. Cross Sectional Study India
| Person/Activity | N | No. of Fingers Contaminated | Log Colony Count | ||||
|---|---|---|---|---|---|---|---|
| Difference * | 95% CI | P | Difference ** | 95% CI | P | ||
| Enterococcus spp. | |||||||
| Person | |||||||
| Male (reference) | 23 | - | - | - | - | ||
| Mother of young child | 65 | 1.45 | 0.11/2.74 | 0.033 | 0.26 | 0.04/0.51 | 0.036 |
| Grandmother | 34 | 0.34 | −1.15/1.91 | 0.654 | 0.11 | −0.18/0.35 | 0.383 |
| Activity | |||||||
| None (reference) | 19 | - | - | - | - | - | |
| Child rearing | 37 | 2.35 | 0.87/3.83 | 0.002 | 0.28 | 0.02/0.52 | 0.031 |
| Food preparation | 12 | 2.41 | 1.07/3.74 | 0.000 | 0.54 | 0.17/0.92 | 0.004 |
| Soil contact | 24 | 0.77 | −0.62/2.15 | 0.276 | 0.06 | −0.18/0.30 | 0.645 |
| Contact with Agricultural products/crops | 6 | 1.36 | −0.21/2.92 | 0.090 | 0.24 | −0.24/0.71 | 0.325 |
| Animal contact | 10 | 1.36 | −0.52/3.25 | 0.156 | 0.17 | −0.24/0.58 | 0.409 |
| Other | 23 | 0.64 | −1.19/2.46 | 0.495 | 0.10 | −0.23/0.43 | 0.545 |
| Escherichia coli | |||||||
| Person | |||||||
| Male (reference) | 23 | - | - | - | - | ||
| Mother of young child | 65 | 0.61 | −0.48/1.82 | 0.328 | 0.08 | −0.12/0.37 | 0.534 |
| Grandmother | 34 | 0.73 | −0.66/2.12 | 0.287 | 0.19 | −0.13/0.49 | 0.210 |
| Activity | |||||||
| None (reference) | 19 | - | - | - | - | ||
| Child rearing | 37 | −0.05 | −1.39/1.30 | 0.947 | 0.10 | −0.22/0.42 | 0.542 |
| Food preparation | 12 | 1.62 | −0.28/3.51 | 0.095 | 2.20 | 1.97/2.42 | 0.000 |
| Soil contact | 24 | 0.78 | −0.59/2.16 | 0.264 | 0.14 | −0.04/0.32 | 0.129 |
| Contact with Agricultural products/crops | 6 | 2.83 | 0.26/5.41 | 0.031 | 2.28 | 2.11/2.45 | 0.000 |
| Animal contact | 10 | 1.15 | −0.56/2.86 | 0.188 | 0.27 | 0.001/0.54 | 0.050 |
| Other | 23 | −0.21 | −1.86/1.42 | 0.798 | 0.03 | −0.31/0.38 | 0.845 |
3.3. Cross Sectional Study Mozambique
| Risk Factor | N | No. of Fingers Contaminated | Log Colony Count | ||||
|---|---|---|---|---|---|---|---|
| Mean Counts | Difference * | p Value * | Mean Counts | Difference ** | p Value * | ||
| Enterococcus spp. | |||||||
| Neighbourhood ID | <0.001 | <0.001 | |||||
| 1 | 111 | 5.7 | ref | 2.7 | ref | ||
| 2 | 157 | 5.9 | 0.2 | 2.8 | 0.1 | ||
| 3 | 92 | 5.3 | −0.4 | 2.6 | −0.2 | ||
| 4 | 78 | 7.1 | 1.4 | 3.3 | 0.5 | ||
| 5 | 101 | 5.0 | −0.7 | 2.4 | −0.3 | ||
| 6 | 111 | 6.0 | 0.4 | 2.8 | 0.1 | ||
| Latrine type | |||||||
| Unimproved | 158 | 5.9 | ref | 2.9 | ref | ||
| Improved | 492 | 5.8 | −0.1 | 0.64 | 2.7 | −0.1 | 0.22 |
| Water tap | |||||||
| Out of compound | 277 | 5.9 | ref | 2.8 | ref | ||
| In compound | 373 | 5.7 | −0.2 | 0.44 | 2.8 | 0.0 | 0.71 |
| Highest education level in household | |||||||
| No secondary | 338 | 6.0 | ref | 2.9 | ref | ||
| Some secondary | 312 | 5.6 | −0.3 | 0.11 | 2.7 | −0.2 | 0.01 |
| Diarrhoea in HH in last 7 days | |||||||
| Yes | 124 | 5.6 | ref | 2.7 | ref | ||
| No | 526 | 5.8 | 0.2 | 0.42 | 2.8 | 0.1 | 0.49 |
| Escherichia coli | |||||||
| Neighbourhood ID | <0.001 | <0.001 | |||||
| 1 | 111 | 4.0 | ref | 2.2 | ref | ||
| 2 | 157 | 3.4 | −0.6 | 1.9 | −0.3 | ||
| 3 | 92 | 2.2 | −1.8 | 1.3 | −1.0 | ||
| 4 | 78 | 3.8 | −0.2 | 2.2 | 0.0 | ||
| 5 | 101 | 3.0 | −1.0 | 1.7 | −0.6 | ||
| 6 | 111 | 3.5 | −0.6 | 2.0 | −0.3 | ||
| Latrine type | |||||||
| Unimproved | 158 | 3.2 | ref | 1.8 | ref | ||
| Improved | 492 | 3.4 | 0.2 | 0.49 | 1.9 | 0.2 | 0.19 |
| Water tap | |||||||
| Out of compound | 277 | 3.4 | ref | 1.9 | ref | ||
| In compound | 373 | 3.3 | −0.1 | 0.63 | 1.9 | 0.0 | 0.93 |
| Highest education level in household | |||||||
| No secondary | 338 | 3.4 | ref | 1.9 | ref | ||
| Some secondary | 312 | 3.3 | −0.1 | 0.75 | 1.9 | −0.1 | 0.61 |
| Diarrhoea in HH in last 7 days | |||||||
| Yes | 124 | 3.4 | ref | 1.9 | ref | ||
| No | 526 | 3.4 | 0 | 0.99 | 1.9 | 0.1 | 0.67 |
3.4. Discussion
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Curtis, V.; Cairncross, S.; Yonli, R. Domestic hygiene and diarrhoea—Pinpointing the problem. Trop. Med. Int. Health 2000, 5, 22–32. [Google Scholar] [PubMed]
- Curtis, V.; Schmidt, W.; Luby, S.; Florez, R.; Toure, O.; Biran, A. Hygiene: New hopes, new horizons. Lancet Infect. Dis. 2011, 11, 312–321. [Google Scholar] [CrossRef]
- Hunter, R.P.; MacDonald, A.M.; Carter, R.C. Water supply and health. PLoS Med. 2010, 7. [Google Scholar] [CrossRef] [Green Version]
- Mara, D.; Lane, J.; Scott, B.; Trouba, D. Sanitation and health. PLoS Med. 2010, 7. [Google Scholar] [CrossRef]
- Schmidt, W.P. The elusive effect of water and sanitation on the global burden of disease. Trop. Med. Int. Health 2014, 19, 522–527. [Google Scholar] [CrossRef] [PubMed]
- Luby, S.P.; Agboatwalla, M.; Billhimer, W.; Hoekstra, R.M. Field trial of a low cost method to evaluate hand cleanliness. Trop. Med. Int. Health 2007, 12, 765–771. [Google Scholar] [CrossRef]
- Pinfold, V.J.; Horan, N.J. Measuring the effect of a hygiene behaviour intervention by indicators of behaviour and diarrhoeal disease. Trans. R. Soc. Trop. Med. Hyg. 1996, 90, 366–371. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, M.W.; Tiwari, S.; Lorente, M.; Gichaba, C.M.; Wuertz, S. Identifying human and livestock sources of fecal contamination in Kenya with host-specific Bacteroidales assays. Water Res. 2009, 43, 4956–4966. [Google Scholar] [CrossRef]
- Mattioli, M.C.; Pickering, A.J.; Gilsdorf, R.J.; Davis, J.; Boehm, A.B. Hands and water as vectors of diarrheal pathogens in Bagamoyo, Tanzania. Environ. Sci. Technol. 2013, 47, 355–363. [Google Scholar] [CrossRef]
- Pickering, A.J.; Davis, J.; Walters, S.P.; Horak, H.M.; Keymer, D.P.; Mushi, D.; Struckfaden, R.; Chynoweth, J.S.; Liu, J.; Blum, A.; et al. Hands, water, and health: Fecal contamination in Tanzanian communities with improved, non-networked water supplies. Environ. Sci. Technol. 2010, 44, 3267–3272. [Google Scholar] [CrossRef]
- Anuradha, P.; Devi, P.Y.; Prakash, M.S. Effect of handwashing agents on bacterial contamination. Indian J. Pediatr. 1999, 66, 7–10. [Google Scholar] [CrossRef] [PubMed]
- Hoque, B.A. Handwashing practices and challenges in Bangladesh. Int. J. Environ. Health Res. 2003, 13, S81–S87. [Google Scholar] [CrossRef] [PubMed]
- Hoque, A.B.; Briend, A. A comparison of local handwashing agents in Bangladesh. J. Trop. Med. Hyg. 1991, 94, 61–64. [Google Scholar] [PubMed]
- Hoque, B.A.; Mahalanabis, D.; Alam, M.J.; Islam, M.S. Post-defecation handwashing in Bangladesh: Practice and efficiency perspectives. Public Health 1995, 109, 15–24. [Google Scholar] [CrossRef]
- Hoque, B.A.; Mahalanabis, D.; Pelto, B.; Alam, M.J. Research methodology for developing efficient handwashing options: An example from Bangladesh. J. Trop. Med. Hyg. 1995, 98, 469–475. [Google Scholar]
- Kaltenthaler, C.E.; Drasar, B.S.; Potter, C.W. The use of microbiology in the study of hygiene behaviour. Microbios 1996, 88, 35–43. [Google Scholar] [PubMed]
- Burton, M.; Cobb, E.; Donachie, P.; Judah, G.; Curtis, V.; Schmidt, W.-P. The Effect of handwashing with water or soap on bacterial contamination of hands. Int. J. Environ. Res. Public Health 2011, 8, 97–104. [Google Scholar] [CrossRef]
- Dodrill, L.; Schmidt, W.-P.; Cobb, E.; Donachie, P.; Curtis, V.; Barra, M. Male commuters in north and south England: Risk factors for the presence of faecal bacteria on hands. BMC Public Health 2011, 11. [Google Scholar] [CrossRef]
- Judah, G.; Donach, P.; Cobb, E.; Schmidt, W.; Holland, M.; Curtis, V. Dirty hands: Bacteria of faecal origin on commuters’ hands. Epidemiol. Infect. 2010, 138, 409–414. [Google Scholar] [CrossRef] [PubMed]
- Pickering, A.J.; Julian, T.R.; Mamuya, S.; Boehm, A.B.; Davis, J. Bacterial hand contamination among Tanzanian mothers varies temporally and following household activities. Trop. Med. Int. Health 2011, 16, 233–239. [Google Scholar] [CrossRef]
- Pickering, A.J.; Julian, T.R.; Marks, S.J.; Mattioli, M.C.; Boehm, A.B.; Schwab, K.J.; Davis, J. Fecal Contamination and diarrheal pathogens on surfaces and in soils among Tanzanian households with and without improved sanitation. Environ. Sci. Technol. 2012, 46, 5736–5743. [Google Scholar] [CrossRef]
- Devamani, C. Bacterial Recontamination of Hands Following Handwashing and Associated Risk Factors in Rural Andhra Pradesh, India; University of London: London, UK, 2011. [Google Scholar]
- Reduction of Fecal Contamination of Street-Vended Beverages in Guatemala by A Simple System for Water Purification and Storage, Handwashing, and Beverage Storage. Available online: http://www2.wsp.org/scalinguphandwashing/enablingtechnologies/docs/36._closed_small__reservoir.pdf (accessed on 21 August 2014).
- Kotloff, K.L.; Nataro, J.P.; Blackwelder, W.C.; Nasrin, D.; Farag, T.H.; Panchalingam, S.; Wu, Y.; Sow, S.O.; Sur, D.; Breiman, R.F.; et al. Burden and aetiology of diarrhoeal disease in infants and young children in developing countries (the Global Enteric Multicenter Study, GEMS): A prospective, case-control study. Lancet 2013, 382, 209–222. [Google Scholar] [CrossRef]
- Alam, N.; Wojtyniak, B.; Henry, F.J.; Rahaman, M.M. Mothers’ personal and domestic hygiene and diarrhoea incidence in young children in rural Bangladesh. Int. J. Epidemiol. 1989, 18, 242–247. [Google Scholar] [CrossRef]
- Henry, J.F.; Rahim, Z. Transmission of diarrhoea in two crowded areas with different sanitary facilities in Dhaka, Bangladesh. J. Trop. Med. Hyg. 1990, 93, 121–126. [Google Scholar] [PubMed]
- Luby, S.P.; Halder, A.K.; Huda, T.; Unicomb, L.; Johnston, R.B. The effect of handwashing at recommended times with water alone and with soap on child diarrhea in rural Bangladesh: An observational study. PLoS Med. 2011, 8. [Google Scholar] [CrossRef]
- The Public and Domestic Domains in the Transmission of Disease. Available online: http://onlinelibrary.wiley.com/doi/10.1046/j.1365-3156.1996.d01-9.x/pdf (accessed on 20 February 1996).
- Genser, B.; Strina, A.; dos Santos, L.A.; Teles, C.A.; Prado, M.S.; Cairncross, S; Barreto, M.L. Impact of a city-wide sanitation intervention in a large urban centre on social, environmental and behavioural determinants of childhood diarrhoea: Analysis of two cohort studies. Int. J. Epidemiol. 2008, 37, 831–840. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Devamani, C.; Norman, G.; Schmidt, W.-P. A Simple Microbiological Tool to Evaluate the Effect of Environmental Health Interventions on Hand Contamination. Int. J. Environ. Res. Public Health 2014, 11, 11846-11859. https://doi.org/10.3390/ijerph111111846
Devamani C, Norman G, Schmidt W-P. A Simple Microbiological Tool to Evaluate the Effect of Environmental Health Interventions on Hand Contamination. International Journal of Environmental Research and Public Health. 2014; 11(11):11846-11859. https://doi.org/10.3390/ijerph111111846
Chicago/Turabian StyleDevamani, Carol, Guy Norman, and Wolf-Peter Schmidt. 2014. "A Simple Microbiological Tool to Evaluate the Effect of Environmental Health Interventions on Hand Contamination" International Journal of Environmental Research and Public Health 11, no. 11: 11846-11859. https://doi.org/10.3390/ijerph111111846
APA StyleDevamani, C., Norman, G., & Schmidt, W.-P. (2014). A Simple Microbiological Tool to Evaluate the Effect of Environmental Health Interventions on Hand Contamination. International Journal of Environmental Research and Public Health, 11(11), 11846-11859. https://doi.org/10.3390/ijerph111111846