Non-Accidental Health Impacts of Wildfire Smoke

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Data Abstraction
3. Results
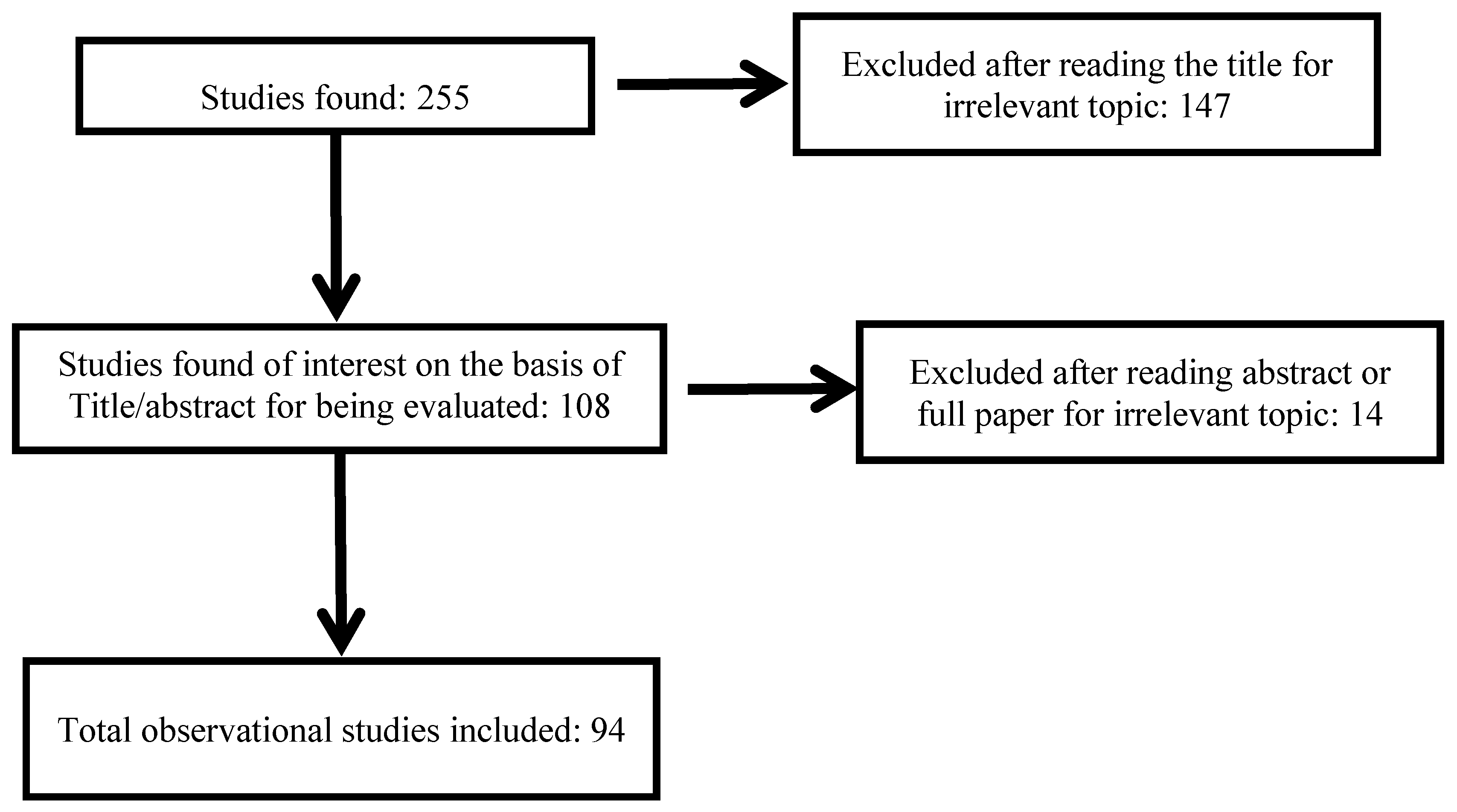
3.1. Study Selection
3.2. Wildfire Exposure Assessment
3.3. Study Design and Statistical Approaches to Evaluate Wildfire Health Effects
3.4. Non-Accidental Health Effects Related to Wildfire
3.4.1. Non-Accidental Health Effects at the Population Level

{kind=link}
{kind=link}
| Location | Authors | Study Period | Population | Health Outcomes | Exposure Assessment/Analytical Methodology | Findings |
|---|---|---|---|---|---|---|
| Sydney | Morgan et al. 2010 [24] | 1994–2002 | All causes mortality, Respiratory mortality and cardiovascular mortality, respiratory diseases admissions | Monitoring stations using TEOM instruments in 8 monitoring sites | PM10 was associated with small increase in all causes mortality at lag0 (0.80% CI : −0.24% to 1.86%) but not associated with respiratory mortality or cardiovascular mortality | |
| Denver | Vedal and Duton [36] | 2 days fire in Denver 9 June and 18 June 2002 | Denver population area (2 millions) | All-cause mortality data for 2001 and 2002 | PM was obtained from daily air pollution from network of monitoring sites for Colorado | 9 June 2002: PM10 and PM2.5 peak of 1 h concentration: 372 and 200 mg/m3, respectively 18 June 2002: PM10 and PM2.5 peak of 1 h concentration: 316 and 200 mg/m3, respectively No perceptible increases in daily mortality could be attributed to the increase PM concentrations from wildfire |
| Kuala Lampur | Sastry et al. 2002 [37] | April and November 1997 | Population of Kuala Lumpur (2.5 millions) | All-cause mortality data from 1994–1997 | Daily measurement from Malaysian Meteorological Bureau | PM10 > 210 µg/m3 is associated with increase of total non-trauma mortality (relative risk = 1.72 for 65–74) |
| Sydney | Johnston et al. 2011 [31] | 1997–2004 | Population of Sydney | All-cause mortality data from the Australian Bureau of Statistics | Events were defined as days for which the 24 h city-wide concentration of PM10 exceeded the 99th percentile | A recent study conducted by Johnston and colleagues in Sydney looked at the effects of bushfires between 1994 and 2007 and mortality. This study revealed that a 5% increase in non-accidental mortality at lag of 1 day (OR 1.05 (95% CI: 1.00–1.10)) was observed on days of high air pollution from bushfire smoke |
| Location | StudyAuthors | Study Period | Population | Health Outcomes | Exposure Assessment/Analytical Methodology | Findings |
|---|---|---|---|---|---|---|
| North Carolina | Rappold et al. 2011 [18] | June 2008 | Population of 42 North Carolina counties | Respiratory diseases | Use Aerosol Optical Depth (AOD) measured by satellite GEOS | In the counties exposed significant increase in cumulative RR for asthma (RR = 1.65 (95% CI: 1.25–2.1)), COPD (RR = 1.73 (95% CI: 1.06–2.83)) and pneumonia and acute bronchitis (RR = 1.59 (95% CI: 1.07–2.34)) |
| Emergency departments visits | AOD scale from 0–2, high density of plume if AOD > 1.25 | ED visits of all respiratory diagnosis were elevated in the exposed counties (RR = 1.66 (95% CI: 1.38–1.91)) | ||||
| Counties with 25% of areas with AOD > 1.25 were defined as exposed to the smoke plume for each day in high-expose window | Significant increase for Emergency department visits for cardiopulmonary symptoms (RR = 1.23 (95% CI: 1.06–1.43)) and heart failure (RR = 1.37 (95% CI: 1.01–1.85)) | |||||
| Southern California | Kunzli et al. 2006 [16] | October 2003 | 873 high school students and 551 elementary-school children from 16 communities in California | Respiratory diseases | Webmail questionnaire to assess smoke exposure and occurrence of symptoms | Prevalence rates of reported outcomes were much higher among individuals with asthma |
| Medication usage | Exposure duration were quantified by the number of days of exposure during the two weeks (not at all, 1–2 d, 3–5 d, 6–10 d, all days) | Dry cough, medication and physician visits were more frequently reported by parents of elementary school children. High school students report eye symptoms | ||||
| Physician visits | Six or more days of fire smell was significantly associated with all outcomes | |||||
| Six days or more of fire smell is associated with more than four-fold higher rates of eyes symptoms, 3 fold dry cough and sneezing 2 for cold, sore throat, wet cough, medication use, physician visits and missed school due symptoms | ||||||
| Southern California | Mirabelli et al. 2009 [17] | October 2003 | 465 high school students from 12 communities | Respiratory diseases | Webmail questionnaire assess smoke exposure and the occurrence of symptoms | Forty percent (186 of 465) of population reported the odor of wildfire smoke at home |
| Log-binomial regression to evaluate associations between smoke exposure and fire-related health symptoms | Increase respiratory and eye symptoms with increasing frequency of wildfire smoke exposure | |||||
| Ratio of maximum midexpiratory flow to forced vital capacity as marker of airway size | ||||||
| Three Provinces of Netherlands (Groningen, Friesland and Drenthe) | Greven et al. 2011 [20] | 12 months | 1330 firefighters | General respiratory symptoms | Questionnaire web-based version of European community Respiratory Health Survey questionnaire, added question to identify the number of incidents, the type, the onset, and the duration of symptoms and possible exposure during the incident | OR of general respiratory symptoms were estimated between 1.2 (95% CI: 1.0–1.4) and 1.4 (95% CI: 1.2–1.7) per 25 firesAn inhalation incident is strongly associated with the presents respiratory symptomsOR between 1.7 (95% CI: 1.1–2.7) and 3.0 (95% CI: 1.9–4.7). |
| Atopy and bronchial hyper-responsiveness | ||||||
| Brazilian Amazon Region | Ignotti et al. 2010 [32] | 2004–2005 | Population of Brazilian amazon region | Rates of respiratory hospitalization among children, elderly and intermediate age group and due to childbirth | Annual hours (AH%) of PM2.5 > 80 µg/m3 AH = (sum of hours with PM2.5 > 80 µg/m3/sum hours PM2.5 is measured in the year) × 100 Use of a coupled aerosol and gas transport model to estimate atmospheric emission Use of satellite observations of fires to obtain several gas and aerosols particles from biomass burnings | 1% of increase of the exposure indicator was associated to an increase of 8% of child hospitalization (children < 5 years), 10% increase in hospitalization of elderly, 5% increase of the intermediate age group |
| Singapore | Emmanuel et al. 2000 [38] | 1997 | Respiratory diseases | PM10, PM2.5, and other compounds( nitrogen dioxide, ozone, CO) were measured by 15 stations located through the Island linked via public telephone network to a central control station | Air quality was into the unhealthy range (PSI > 100) on 12 days, the highest PSI was 138.94% of particles observed were PM2.5 Haze from the Indonesian forest fire was responsible of 30% increase in outpatient attendances | |
| Outpatient attendances, accident and emergencies, inpatient care, mortality data | Increase in PM10 levels from 50 µg/m3 to 150 µg/m3 was significantly associated with increase of 12% of upper respiratory tract illness, 19% asthma and 26% rhinitis No significant increase in hospitalization or mortality due to the smoke haze | |||||
| Victoria, Australia | Tham et al. 2009 [39] | 2002–2003 | Hospital admissions, emergency attendances, air quality and meteorological data | Air pollution from the Aplington air quality monitoring station which had the most complete data and was located away from the coast freeways and industrial settings | Daily levels PM10 were strongly associated with respiratory emergency department attendances (p < 0.001) No association with hospital admissions (p = 0.06) After adjusting for confounding effects of maximum temperature and relative humidity, the strongest associations were observed between PM10 and daily respiratory emergency department attendances in Melbourne (RR = 1.018, 95% CI: 1.004–1.033, p = 0.01) | |
| Vilnius | Ovadnevaite et al. 2006 [40] | August–September 2002 | The population of Vilnius | Respiratory diseases, bronchial asthma | Air pollution data from Vilnius monitoring network | Significant increase of average hourly values of PM10, NO2, CO and SO2 during several episodes in 2002 |
| Australia | Reisen et al. 2011 [41] | 2005–2008 | 130 firefighters | Air toxics within the breathing zone of firefighters | One-way analyses of variance, Student t-tests | 30% of firefighters had a high exposure risk i.e., exposure to hazardous substance, CO, RP, and formaldehyde exceeds the occupational exposure standard (OES) to 5% to 20% of time, 6% had a very high exposure risk i.e., exposure to hazardous substance exceeds OES for more than 20% of time |
| CO values were Log-transformed in all tests to meet the assumption of normal distribution of variables | The majority of firefighters (60%) were exposed in low to moderate levels | |||||
| Galice, Spain | Caamano-Isorna et al. 2011 [21] | 2006 | 156 municipalities | Consumption drugs for anxiolytics-hypnotics and drugs for obstructive airway disease (DOADs) for respiratory health | Additive model for time series analysis | Higher consumption of DOADs among pensioners during the months after the wildfires |
| Sydney | Jalaludin et al. 2000 [15] | January 1994 | Children with a reported history of wheezing in the previous 12 months (32 children recruited) | Peak expiratory flow rates (PEFR) | Generalized estimating equation models | After adjusting for the wildfire period and potential confounders, there was no significant association between mean PM10 and PEFR Children without bronchial hyperactivity had a significant negative association between PEFR and PM10 |
| Southern California | Delfino et al. 2009 [13] | October 2003 | n = 40,856 (hospital admissions) | Respiratroy admissions, cardiovascular admissions | Generalised estimating equation models for Poisson data | Average increases of 70 µg/m3 PM2.5 during heavy smoke conditions was associated with 34% increase asthma admissions |
| Sao Paulo State Brazil | Abrex et al. 2007 [30] | 23 March 2003–27 July 2004 | Population admitted for asthma in main hospital of Araraquara | Asthma hospital admissions | Time series analysis | Asthma hospital admission during burning period were 50% higher than those observed during the non-burning period (p < 0.001) |
| Generalized linear Poisson regression models | ||||||
| Brisbane | Chen et al. 2006 [23] | 1 July 1997–31 December 2000 | Patients admitted in Brisbane | Respiratory hospital admissions | generalized linear model with negative binomial distribution | An increase of PM10 from low (<15 µg/m3) to high level (>20 µg/m) level, is accompanied by an increase of 19% in respiratory hospital admissions for wildfire days vs. 13% for background days |
| Indonesia | Kunii et al. 2002 [42] | 29 September–7 October 1997 | n = 543 | Respiratory diseases | 8 monitoring sites between Jakarta (Java) and Jambi (Sumatra) were used to air quality measurements, Health effects measured by a face to face structured interview | Concentration of CO and PM10: very unhealthy and hazardous levels |
| Kuching, Malaisia | Mott et al. 2005 [35] | 1 January 1995–31 December 1998, fire period 1 Augst–31 October 1997 | Population of Kuching region in Malaysia (7 hospitals) | Hospitalizations, all causes, respiratory admissions, cardiovasuclar admissions | Comparison of health outcomes in the wildfire period or post-fire period basing on forecasting estimates established from a historical baseline period of 1 January 1995 through 31 July 1997 | Increase respiratory hospitalizations specifically for patients with COPD and asthma patients |
| Australia | Morgan et al. 2010 [24] | 1994–2002 | Respiratory diseases, respiratory mortality and cardiovascular mortality, respiratory diseases admissions | Monitoring stations using TEOM instruments in 8 monitoring sites | A 10 µg/m3 increase in wildfire PM10 is associated with: 1.24% (95% CI 0.22% to 2.27%) increase in all respiratory diseases admissions (at lag 0) 3.8% (1.4 to 6.26) increase in COPD admissions at lag 25.02 (1.77 to 8.37) increase in adult asthma at lag (0) | |
| Darwin, Australia | Hanigan et al. 2008 [43] | April–November 1995–2005 | Respiratory diseases admissions | Daily PM10 exposure level is determined using the visibility data to build a predictive model | An increase of 10 µg/m3 in same-day estimated PM10 was associated with 4.81% (95% CI: −1.04%–11.1%) increase in total respiratory admissions | |
| A strong association of wildfire PM10 and respiratory admission among indigenous people than non-indigenous people (15.02%, 95% CI: 3.73%–27.54% vs. 0.67%, 95% CI: 7.55%–9.6%) | ||||||
| Central Florida | Sorenson et al. 1999 [44] | June–July 1998 | All ages | Emergency room visits, hospital admissions | descriptive statistics | Increased emergency-room visits and hospital admissions for asthma and bronchitis during fire period relative to same period in previous year |
| Malaysia | Brauer, 1998 [45] | All ages | Outpatient visits | Not specified | Increased visits for asthma, upper respiratory tract symptoms, and rhinitis during vegetation fire episode periods of elevated, PM10 in Malaysia | |
| Singapore | Chew et al. 1995 [46] | Children less than 12 years old | Emergency room visits | Multiple regression analysis | Increased asthma visits with PM10 during episode of exposure to biomass burning emissions in Singapore | |
| Denver | Sutherland et al. 2005 [47] | June–July 2002 | Adult with COPD | Symptoms | Standard descriptive statistics, repeated measurements ANOVA | Significant increase in symptom index (dyspnea, cough, chest tightness, wheezing, sputum production) on two days of elevated PM2.5 (65 μg/m3) relative to control days (14 μg/m3). Days of elevated PM attributed to fire smoke by satellite imaging |
| Kelowna and Kamloops Regions British Columbia | Moore et al. 2006 [48] | 2003 | All ages | Physician visits for respiratory, cardiovascular, and mental illness | Particulate matter obtained from monitoring network of the BC Ministry of Water | A 46% to 78% increase in physician visits for respiratory illness during a 3-week forest fire period in Kelowna, British Columbia |
| Malaysia | Hisham-Hashim et al. 1998 [49] | 1997 | Children | Lung function | Not specified | Decreased lung function in children during vegetation fire episode compared to preepisode measurements |
| Malaysia | Tan et al. 2000 [50] | 1997 | Adult military recruits | Blood markers of inflammation | Not specified | Bone marrow stimulated to release immature polymorphonuclear leukocytes into blood during period of exposure to forest fire smoke relative to period following smoke exposure |
| Isfahan rural areas, Iran | Golshan et al. 2002 [51] | 1–80 years olds | Adults | Asthma medication, lung function, asthmatic and other respiratory symptoms | physician-administered health questionnaire, physical examinations and spirometry in symptomatic cases | Increased prevalence of respiratory symptoms and various asthma indicators, decreased lung function post-rice stubble burning period relative to period prior to burning in three communities in Iran |
| Darwin, Australia) | Johnston et al. 2002 [52] | April–31 October 2000 | All Ages | Emergency room visits | Mean atmospheric concentration PM10 per cubic metre per 24-h period | Increased asthma visits associated with PM10, especially for concentrations exceeding 40 μg/m3 |
| California | Duclos et al. 1990 [53] | August 1987 | All ages | Emergency room visits | descriptive statistics | Increased respiratory visits in communities exposed to fire smoke |
3.4.1.1. All-Cause and Cardiorespiratory Mortality
3.4.1.2. Cardiorespiratory Morbidity
3.4.1.3. Wildfire Exposure during Pregnancy and Birth Weight
3.4.1.4. Subclinical Effects
3.4.1.4.1. Animal Models
3.4.1.4.2. Human Beings and Firefighters
3.4.1.4.3. Exposure Trials
3.4.2. Wildfire Health Effects in Firefighters and Mechanisms
4. Public Awareness
5. Discussion
6. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Lipsett, M.; Materna, B.; Lyon Stone, S.; Therriault, S.; Blaisdell, R.; Cook, J. Wildfire Smoke—A Guide for Public Health Officials; California Department of Public Health: Sacramento, CA, USA; U.S. Environmental Protection Agency: Washington, DC, USA; California Office of Environmental Health Hazard Assessment: Sacramento, CA, USA; Missoula County Health Department: Missoula, MT, USA; California Air Resources Board: Sacramento, CA, USA, 2008. [Google Scholar]
- European Commission. Forest Fires in Europe 2010; Institute for Environment and Sustainability: Ispra, Italy, 2010. [Google Scholar]
- Ottmar, R.D. Smoke source characteristics. In Smoke Management Guide for Prescribed and Wildland Fire, 2001 ed.; Hardy, C.C., Ottmar, R.D., Peterson, J.L., Core, J.E., Seamon, P., Eds.; National Wildfire Coordinating Group, Fire Use Working Team: Boise, ID, USA, 2001; pp. 89–105. [Google Scholar]
- Gyawali, M.; Arnott, W.P.; Lewis, K.; Moosmüller, H. In situ aerosol optics in Reno, NV, 5 USA during and after the summer 2008 California wildfires and the influence of absorbing and non-absorbing organic coatings on spectral light absorption. Atmos. Chem. Phys. 2009, 9, 8007–8015. [Google Scholar] [CrossRef]
- WHO Regional Office for Europe. Health Risks of Particulate Matter from Long-Range Transboundary Air Pollution; European Centre for Environment and Health: Bonn, Germany, 2006. [Google Scholar]
- WHO Regional Office for Europe. Health Effects of Particulate Matter; WHO: Copenhagen, Denmark, 2013. [Google Scholar]
- World Health Organization. Health Guidelines for Vegetation Fire Events; United Nations Environment Programme; WHO: Geneva, Swizerland, 1999. [Google Scholar]
- Dennekamp, M.; Abramson, M.J. The effects of bushfire smoke on respiratory health. Respirology 2011, 16, 198–209. [Google Scholar] [CrossRef] [PubMed]
- U.S. Environmental Protection Agency. National ambient air quality standards for particulate matter. Fed. Register 2013, 78, 3086–3287. [Google Scholar]
- Malilay, J. A Review of Factors Affecting the Human Health Impacts of Air Pollutants from Forest Fires; WHO: Geneva, Switzerland; UNEP: Nairobi, Kenya; WMO: Geneva, Switzerland, 1999; pp. 255–270. [Google Scholar]
- Youssouf, H.; Lioussec, C.; Roblouc, L.; Assamoic, E.M.; Salonend, R.O.; Maesanoa, C.; Banerjeea, S.; Annesi-Maesano, I. Quantifying wildfires exposure for investigating health-related effects. Atmos. Environ. 2014, 97, 239–251. [Google Scholar] [CrossRef]
- Finlay, S.E.; Moffat, A.; Gazzard, R.; Baker, D.; Murray, V. Health impacts of wildfires. PLoS Curr. 2012, 4. [Google Scholar] [CrossRef]
- Delfino, R.J.; Brummel, S.; Wu, J.; Stern, H.; Ostro, B.; Lipsett, M.; Winer, A.; Street, D.H.; Zhang, L.; Tjoa, T.; et al. The relationship of respiratory and cardiovascular hospital admissions to the Southern California wildfires of 2003. Occup. Environ. Med. 2009, 66, 189–197. [Google Scholar] [CrossRef] [PubMed]
- Henderson, S.B.; Johnston, F.H. Measures of forest fire smoke exposure and their associations with respiratory health outcomes. Curr. Opin. Allergy Clin. Immunol. 2012, 12, 221–227. [Google Scholar] [CrossRef] [PubMed]
- Jalaludin, B.; Smith, M.; O’Toole, B.; Leeder, S. Acute effects of bushfires on peak expiratory flow rates in children with wheeze: A time series analysis. Aust. N. Z. J. Public Health 2000, 24, 174–177. [Google Scholar] [CrossRef] [PubMed]
- Künzli, N.; Avol, E.; Wu, J.; Gauderman, W.J.; Rappaport, E.; Millstein, J.; Bennion, J.; McConnell, R.; Gilliland, F.D.; Berhane, K.; et al. Health effects of the 2003 Southern California wildfires on children. Amer. J. Respir. Crit. Care Med. 2006, 174, 1221–1228. [Google Scholar] [CrossRef]
- Mirabelli, M.C.; ünzli, N.; Avol, E.; Gilliland, F.D.; Gauderman, W.J.; McConnell, R.; Peters, J.M. Respiratory symptoms following wildfire smoke exposure: Airway size as a susceptibility factor. Epidemiology 2009, 20, 451–459. [Google Scholar] [CrossRef] [PubMed]
- Rappold, A.G.; Stone, S.L.; Cascio, W.E.; Neas, L.M.; Kilaru, V.J.; Carraway, M.S.; Szykman, J.J.; Ising, A.; Cleve, W.E.; Meredith, J.T.; et al. Peat bog wildfire smoke exposure in rural North Carolina is associated with cardiopulmonary emergency department visits assessed through syndromic surveillance. Environ. Health Perspect. 2011, 119, 1415–1420. [Google Scholar] [CrossRef] [PubMed]
- Naeher, L.P.; Brauer, M.; Lipsett, M.; Zelikoff, J.T.; Simpson, C.D.; Koenig, J.Q.; Smith, K.R. Woodsmoke health effects: A review. Inhal. Toxicol. 2007, 19, 67–106. [Google Scholar]
- Greven, F.E.; Rooyackers, J.M.; Kerstjens, H.A.; Heederik, D.J. Respiratory symptoms in firefighters. Amer. J. Ind. Med. 2011, 54, 350–355. [Google Scholar] [CrossRef]
- Caamano-Isorna, F.; Figueiras, A.; Sastre, I.; Montes-Martínez, A.; Taracido, M.; Piñeiro-Lamas, M. Respiratory and mental health effects of wildfires: An ecological study in Galician municipalities (north-west Spain). Environ. Health 2011, 10. [Google Scholar] [CrossRef]
- Kolbe, A.; Gilchrist, K.L. An extreme bushfire smoke pollution event: health impacts and public health challenges. N. S. W. Public Health Bull. 2009, 20, 19–23. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Verrall, K.; Tong, S. Air particulate pollution due to bushfires and respiratory hospital admissions in Brisbane, Australia. Int. J. Environ. Health Res. 2006, 16, 181–191. [Google Scholar] [CrossRef] [PubMed]
- Morgan, G.; Sheppeard, V.; Khalaj, B.; Ayyar, A.; Lincoln, D.; Jalaludin, B.; Beard, J.; Corbett, S.; Lumley, T. Effects of bushfire smoke on daily mortality and hospital admissions in Sydney, Australia. Epidemiology 2010, 21, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Van Donkelaar, A.; Martin, R.V.; Brauer, M.; Kahn, R.; Levy, R.; Verduzco, C.; Villeneuve, P.J. Global estimates of ambient fine particulate matter concentrations from satellite-based aerosol optical depth: Development and application. Environ. Health Perspect. 2010, 118, 847–855. [Google Scholar] [CrossRef] [PubMed]
- Hodzic, A.; Madronich, S.; Bohn, B.; Massie, S.; Menut, L.; Wiedinmyer, C. Wildfire particulate matter in Europe during summer 2003: Meso-scale modeling of smoke emissions, transport and radiative effects. Atmos. Chem. Phys. 2007, 7, 4043–4064. [Google Scholar] [CrossRef]
- Liousse, C.; Guillaume, B.; Grégoire, J.M.; Mallet, M.; Galy, C.; Pont, V.; Akpo, A.; Bedou, M.; Castéra, P.; Dungall, L.; et al. Updated African biomass burning emission inventories in the framework of the AMMA-IDAF program, with an evaluation of combustion aerosols. Atmos. Chem. Phys. 2010, 10, 9631–9646. [Google Scholar] [CrossRef]
- Betchley, C.; Koenig, J.Q.; van Belle, G.; Checkoway, H.; Reinhardt, T. Pulmonary function and respiratory symptoms in forest firefighters. Amer. J. Ind. Med. 1997, 31, 503–509. [Google Scholar] [CrossRef]
- Analitis, A.; Georgiadis, I.; Katsouyanni, K. Forest fires are associated with elevated mortality in a dense urban setting. Occup. Environ. Med. 2012, 69, 158–162. [Google Scholar] [CrossRef] [PubMed]
- Arbex, M.A.; Martins, L.C.; de Oliveira, R.C.; Pereira, L.A.; Arbex, F.F.; Cançado, J.E.; Saldiva, P.H.; Braga, A.L. Air pollution from biomass burning and asthma hospital admissions in a sugar cane plantation area in Brazil. J. Epidemiol. Community Health 2007, 61, 395–400. [Google Scholar] [CrossRef] [PubMed]
- Johnston, F.; Hanigan, I.; Henderson, S.; Morgan, G.; Bowman, D. Extreme air pollution events from bushfires and dust storms and their association with mortality in Sydney, Australia 1994–2007. Environ. Res. 2011, 111, 811–816. [Google Scholar] [CrossRef] [PubMed]
- Ignotti, E.; Valente, J.G.; Longo, K.M.; Freitas, S.R.; de Souza Hacon, S.; Netto, P.A. Impact on human health of particulate matter emitted from burnings in the Brazilian Amazon region. Rev. Saúde Públ. 2010, 44, 121–130. [Google Scholar] [CrossRef]
- Gasparrini, A. Distributed lag linear and non-linear models in R: The package dlnm. J Stat. Softw 2011, 43, 1–20. [Google Scholar] [PubMed]
- Fowler, C.T. Human health impacts of forest fires in the southern United States: A literature review. J. Ecol. Anthropol. 2003, 7, 39–63. [Google Scholar] [CrossRef]
- Mott, J.A.; Mannino, D.M.; Alverson, C.J.; Kiyu, A.; Hashim, J.; Lee, T.; Falter, K.; Redd, S.C. Cardiorespiratory hospitalizations associated with smoke exposure during the 1997, southeast Asian forest fires. Int. J. Hyg. Environ. Health 2005, 208, 75–85. [Google Scholar] [CrossRef] [PubMed]
- Vedal, S.; Dutton, S.J. Wildfire air pollution and daily mortality in a large urban area. Environ. Res. 2006, 102, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Sastry, N. Forest fires, air pollution, and mortality in southeast Asia. Demography 2002, 39, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Emmanuel, S.C. Impact to lung health of haze from forest fires: The Singapore experience. Respirology 2000, 5, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Tham, R.; Erbas, B.; Akram, M.; Dennekamp, M.; Abramson, M.J. The impact of smoke on respiratory hospital outcomes during the 2002–2003 bushfire season, Victoria, Australia. Respirology 2009, 14, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Ovadnevaitė, J.; Kvietkus, K.; Maršalka, A. 2002 summer fires in Lithuania: Impact on the Vilnius city air quality and the inhabitants health. Sci. Total Environ. 2006, 356, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Reisen, F.; Hansen, D.; Meyer, C.P.M. Exposure to bushfire smoke during prescribed burns and wildfires: Firefighters’ exposure risks and options. Environ. Int. 2011, 37, 314–321. [Google Scholar] [CrossRef] [PubMed]
- Kunii, O.; Kanagawa, S.; Yajima, I.; Hisamatsu, Y.; Yamamura, S.; Amagai, T.; Ismail, I.T. The 1997 haze disaster in Indonesia: Its air quality and health effects. Arch. Environ. Health. 2002, 57, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Hanigan, I.C.; Johnston, F.H.; Morgan, G.G. Vegetation fire smoke, indigenous status and cardio-respiratory hospital admissions in Darwin, Australia, 1996–2005: A time-series study. Environ. Health 2008, 7. [Google Scholar] [CrossRef]
- Sorensen, B.; Fuss, M.; Mulla, Z.; Bigler, W.; Wiersma, S.; Hopkins, R. Surveillance of morbidity during wildfires—Central florida, 1998. MMWR 1999, 48, 78–79. [Google Scholar] [PubMed]
- Brauer, M. Health Impacts of Biomass Air Pollution; Regional Offices for Southeast Asia and the Western Pacific, World Health Organization: Kuala Lumpour, Malesia, 1998. [Google Scholar]
- Chew, F.T.; Ooi, B.C.; Hui, J.K.; Saharom, R.; Goh, D.Y.; Lee, B.W. Singapore’s haze and acute asthma in children. Lancet 1995, 346. [Google Scholar] [CrossRef]
- Sutherland, E.R.; Make, B.J.; Vedal, S.; Zhang, L.; Dutton, S.J.; Murphy, J.R.; Silkoff, P.E. Wildfire smoke and respiratory symptoms in patients with chronic obstructive pulmonary disease. J. Allergy Clin. Immunol. 2005, 115, 420–422. [Google Scholar] [CrossRef] [PubMed]
- Moore, D.; Copes, R.; Fisk, R.; Joy, R.; Chan, K.; Brauer, M. Population health effects of air quality changes due to forest fires in British Columbia in 2003: Estimates from physician-visit billing data. Can. J. Public Health 2006, 97, 105–108. [Google Scholar] [PubMed]
- Hisham-Hashim, J.; Hashim, Z.; Jalaludin, J.; Lubis, S.H.; Hashim, R. Respiratory function of elementary school children exposed to the 1997 Kuala Lumpur haze. Epidemiology 1998, 9. [Google Scholar] [CrossRef]
- Tan, W.C.; Qiu, D.; Liam, B.L.; Ng, T.P.; Lee, S.H.; van Eeden, S.F.; D’Yachkova, Y.; Hogg, J.C. The human bone marrow response to acute air pollution caused by forest fires. Amer. J. Respir. Crit. Care Med. 2000, 161, 1213–1217. [Google Scholar] [CrossRef]
- Golshan, M.; Faghihi, M.; Roushan-Zamir, T.; Masood Marandi, M.; Esteki, B.; Dadvand, P.; Farahmand-Far, H.; Rahmati, S.; Islami, F. Early effects of burning rice farm residues on respiratory symptoms of villagers in suburbs of Isfahan, Iran. Int. J. Environ. Health Res. 2002, 12, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Johnston, F.H.; Kavanagh, A.M.; Bowman, D.M.; Scott, R.K. Exposure to bushfire smoke and asthma: an ecological study. Med. J. Aust. 2002, 176, 535–538. [Google Scholar] [PubMed]
- Duclos, P.; Sanderson, L.M.; Lipsett, M. The 1987 forest fire disaster in California: Assessment of emergency room visits. Arch. Environ. Health 1990, 45, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Haenninen, O. Challenges in estimating the health effects of biomass smoke—Response to Sverre Vedal and Steven J. Dutton: Wildfire air pollution and daily mortality in a large urban area—Commentary. Environ. Res. 2008, 106, 423–424. [Google Scholar] [CrossRef] [PubMed]
- Hanninen, O.O.; Salonen, R.O.; Koistinen, K.; Lanki, T.; Barregard, L.; Jantunen, M. Population exposure to fine particles and estimated excess mortality in Finland from an east European wildfire episode. J. Expo. Sci. Environ. Epidemiol. 2009, 19, 414–422. [Google Scholar] [CrossRef] [PubMed]
- Johnston, F.H.; Henderson, S.B.; Chen, Y.; Randerson, J.T.; Marlier, M.; Defries, R.S.; Kinney, P.; Bowman, D.M.; Brauer, M. Estimated global mortality attributable to smoke from landscape fires. Environ. Health Perspect. 2012, 120, 695–701. [Google Scholar] [CrossRef] [PubMed]
- Aditama, T.Y. Impact of haze from forest fire to respiratory health: Indonesian experience. Respirology 2000, 5, 169–174. [Google Scholar] [CrossRef] [PubMed]
- Frankenberg, E.; McKee, D.; Thomas, D. Health consequences of forest fires in Indonesia. Demography 2005, 42, 109–129. [Google Scholar] [CrossRef] [PubMed]
- Yao, J.; Brauer, M.; Henderson, S.B. Evaluation of a wildfire smoke forecasting system as a tool for public health protection. Environ. Health Perspect. 2013, 121, 1142–1147. [Google Scholar] [PubMed]
- Elliott, C.T.; Henderson, S.B.; Wan, V. Time series analysis of fine particulate matter and asthma reliever dispensations in populations affected by forest fires. Environ. Health 2013, 12. [Google Scholar] [CrossRef]
- Henderson, S.B.; Brauer, M.; Macnab, Y.C.; Kennedy, S.M. Three measures of forest fire smoke exposure and their associations with respiratory and cardiovascular health outcomes in a population-based cohort. Environ. Health Perspect. 2011, 119, 1266–1271. [Google Scholar] [CrossRef] [PubMed]
- Long, W.; Tate, R.B.; Neuman, M.; Manfreda, J.; Becker, A.B.; Anthonisen, N.R. Respiratory symptoms in a susceptible population due to burning of agricultural residue. Chest 1998, 113, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Johnston, F.H.; Bailie, R.S.; Pilotto, L.S.; Hanigan, I.C. Ambient biomass smoke and cardio-respiratory hospital admissions in Darwin, Australia. BMC Public Health 2007, 7. [Google Scholar] [CrossRef]
- Crabbe, H. Risk of respiratory and cardiovascular hospitalisation with exposure to bushfire particulates: New evidence from Darwin, Australia. Environ. Geochem. Health 2012, 34, 697–709. [Google Scholar] [CrossRef] [PubMed]
- Martin, K.L.; Hanigan, I.C.; Morgan, G.G.; Henderson, S.B.; Johnston, F.H. Air pollution from bushfires and their association with hospital admissions in Sydney, Newcastle and Wollongong, Australia 1994–2007. Aust. N. Z. J. Public Health 2013, 37, 238–243. [Google Scholar] [CrossRef] [PubMed]
- Thelen, B.; French, N.F.N.; Koziol, B.W.; Billmire, M.; Owen, R.C.; Johnson, J.; Ginsberg, M.; Loboda, T.; Wu, S. Modeling acute respiratory illness during the 2007 San Diego wildland fires using a coupled emissions-transport system and generalized additive modeling. Environ. Health 2013, 12. [Google Scholar] [CrossRef]
- Allen, R.W.; Carlsten, C.; Karlen, B.; Leckie, S.; van Eeden, S.; Vedal, S.; Wong, I.; Brauer, M. An air filter intervention study of endothelial function among healthy adults in a woodsmoke-impacted community. Amer. J. Respir. Crit. Care Med. 2011, 183, 1222–1230. [Google Scholar] [CrossRef]
- Forchhammer, L.; Møller, P.; Riddervold, I.S.; Bønløkke, J.; Massling, A.; Sigsgaard, T.; Loft, S. Controlled human wood smoke exposure: Oxidative stress, inflammation and microvascular function. Part Fibre Toxicol. 2012, 9. [Google Scholar] [CrossRef]
- Ghio, A.J.; Soukup, J.M.; Case, M.; Dailey, L.A.; Richards, J.; Berntsen, J.; Devlin, R.B.; Stone, S.; Rappold, A. Exposure to wood smoke particles produces inflammation in healthy volunteers. Occup. Environ. Med. 2012, 69, 170–175. [Google Scholar] [CrossRef] [PubMed]
- Riddervold, I.S.; Bønløkke, J.H.; Mølhave, L.; Massling, A.; Jensen, B.; Grønborg, T.K.; Bossi, R.; Forchhammer, L.; Kjærgaard, S.K.; Sigsgaard, T.; et al. Wood smoke in a controlled exposure experiment with human volunteers. Inhal. Toxicol. 2011, 23, 277–288. [Google Scholar] [CrossRef] [PubMed]
- Holstius, D.M.; Reid, C.E.; Jesdale, B.M.; Morello-Frosch, R. Birth weight following pregnancy during the 2003 Southern California wildfires. Environ. Health Perspect. 2012, 120, 1340–1345. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R. Followup in Southern California: Decreased birth weight following prenatal wildfire smoke exposure. Environ. Health Perspect. 2012, 120. [Google Scholar] [CrossRef]
- Williams, K.M.; Franzi, L.M.; Last, J.A. Cell-specific oxidative stress and cytotoxicity after wildfire coarse particulate matter instillation into mouse lung. Toxicol. Appl. Pharmacol. 2013, 266, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Wegesser, T.C.; Pinkerton, K.E.; Last, J.A. California wildfires of 2008: Coarse and fine particulate matter toxicity. Environ. Health Perspect. 2009, 117, 893–897. [Google Scholar] [CrossRef] [PubMed]
- Huttunen, K.; Siponen, T.; Salonen, I.; Yli-Tuomi, T.; Aurela, M.; Dufva, H.; Hillamo, R.; Linkola, E.; Pekkanen, J.; Pennanen, A.; et al. Low-level exposure to ambient particulate matter is associated with systemic inflammation in ischemic heart disease patients. Environ. Res. 2012, 116, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Reinhardt, T.E.; Ottmar, R.D. Baseline measurements of smoke exposure among wildland firefighters. J. Occup. Environ. Hyg. 2004, 1, 593–606. [Google Scholar] [CrossRef] [PubMed]
- Aisbett, B.; Wolkow, A.; Sprajcer, M.; Ferguson, S.A. “Awake, smoky, and hot”: Providing an evidence-base for managing the risks associated with occupational stressors encountered by wildland firefighters. Appl. Ergon. 2012, 43, 916–925. [Google Scholar] [CrossRef] [PubMed]
- Swiston, J.R.; Davidson, W.; Attridge, S.; Li, G.T.; Brauer, M.; van Eeden, S.F. Wood smoke exposure induces a pulmonary and systemic inflammatory response in firefighters. Eur. Respir. J. 2008, 32, 129–138. [Google Scholar] [CrossRef] [PubMed]
- Hejl, A.M.; Adetona, O.; Diaz-Sanchez, D.; Carter, J.D.; Commodore, A.A.; Rathbun, S.L.; Naeher, L.P. Inflammatory effects of woodsmoke exposure among wildland firefighters working at prescribed burns at the Savannah River Site, SC. J. Occup. Environ. Hyg. 2013, 10, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Brotherhood, J.R.; Budd, G.M.; Jeffery, S.E.; Hendrie, A.L.; Beasley, F.A.; Costin, B.P.; Wu, Z.E. Fire fighters’ exposure to carbon monoxide during Australian bushfires. Amer. Ind. Hyg. Assoc. J. 1990, 51, 234–240. [Google Scholar] [CrossRef]
- Leonard, S.S.; Castranova, V.; Chen, B.T.; Schwegler-Berry, D.; Hoover, M.; Piacitelli, C.; Gaughan, D.M. Particle size-dependent radical generation from wildland fire smoke. Toxicology 2007, 236, 103–113. [Google Scholar] [CrossRef] [PubMed]
- Van Eeden, S.F.; Tan, W.C.; Suwa, T.; Mukae, H.; Terashima, T.; Fujii, T.; Qui, D.; Vincent, R.; Hogg, J.C. Cytokines involved in the systemic inflammatory response induced by exposure to particulate matter air pollutants (PM10). Amer. J. Respir. Crit. Care Med. 2001, 164, 826–830. [Google Scholar] [CrossRef]
- Adetona, O.; Hall, D.B.; Naeher, L.P. Lung function changes in wildland firefighters working at prescribed burns. Inhal. Toxicol. 2011, 23, 835–841. [Google Scholar] [CrossRef] [PubMed]
- Soteriades, E.S.; Smith, D.L.; Tsismenakis, A.J.; Baur, D.M.; Kales, S.N. Cardiovascular disease in U.S. firefighters: A systematic review. Cardiol Rev. 2011, 19, 202–215. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Teehan, D.; Farioli, A.; Baur, D.M.; Smith, D.; Kales, S.N. Sudden cardiac death among firefighters ≤45 years of age in the United States. Amer. J. Cardiol. 2013, 112, 1962–1967. [Google Scholar] [CrossRef] [PubMed]
- Choi, B.; Schnall, P.L.; Dobson, M.; Garcia-Rivas, J.; Kim, H.; Zaldivar, F.; Israel, L.; Baker, D. Very long (>48 h) shifts and cardiovascular strain in firefighters: A theoretical framework. Ann. Occup. Environ. Med. 2014, 26. [Google Scholar] [CrossRef]
- De Vos, A.J.; Cook, A.; Devine, B.; Thompson, P.J.; Weinstein, P. Effect of protective filters on fire fighter respiratory health during simulated bushfire smoke exposure. Amer. J. Ind. Med. 2006, 49, 740–750. [Google Scholar] [CrossRef]
- Booze, T.F.; Reinhardt, T.E.; Quiring, S.J.; Ottmar, R.D. A screening-level assessment of the health risks of chronic smoke exposure for wildland firefighters. J. Occup. Environ. Hyg. 2004, 1, 296–305. [Google Scholar] [CrossRef] [PubMed]
- Aisbett, B.; Phillips, M.; Sargeant, M.; Gilbert, B.; Nichols, D. Fighting with fire—How bushfire suppression can impact on fire fighters’ health. Aust. Fam. Physician 2007, 36, 994–997. [Google Scholar] [PubMed]
- Edwards, R.; Johnson, M.; Dunn, K.H.; Naeher, L.P. Application of real-time particle sensors to help mitigate exposures of wildland firefighters. Arch. Environ. Occup. Health 2005, 60, 40–43. [Google Scholar] [CrossRef] [PubMed]
- Semenza, J.C.; Wilson, D.J.; Parra, J.; Bontempo, B.D.; Hart, M.; Sailor, D.J.; George, L.A. Public perception and behavior change in relationship to hot weather and air pollution. Environ. Res. 2008, 107, 401–411. [Google Scholar] [CrossRef] [PubMed]
- Sillanpää, M.; Saarikoski, S.; Hillamo, R.; Pennanen, A.; Makkonen, U.; Spolnik, Z.; van Grieken, R.; Koskentalo, T.; Salonen, R.O. Chemical composition, mass size distribution and source analysis of long-range transported wildfire smokes in Helsinki. Sci. Total Environ. 2005, 350, 119–135. [Google Scholar] [CrossRef] [PubMed]
- Dominici, F.; McDermott, A.; Zeger, S.L.; Samet, J.M. On the use of generalized additive models in time-series studies of air pollution and health. Amer. J. Epidemiol. 2002, 156, 193–203. [Google Scholar] [CrossRef]
- Kim, S.-Y.; Peel, J.L.; Hannigan, M.P.; Dutton, S.J.; Sheppard, L.; Clark, M.L.; Vedal, S. The temporal lag structure of short-term associations of fine particulate matter chemical constituents and cardiovascular and respiratory hospitalizations. Environ. Health Perspect. 2012, 120, 1094–1099. [Google Scholar] [CrossRef] [PubMed]
- Dominici, F.; Peng, R.D.; Bell, M.L.; Pham, L.; McDermott, A.; Zeger, S.L.; Samet, J.M. Fine particulate air pollution and hospital admission for cardiovascular and respiratory diseases. JAMA 2006, 295, 1127–1134. [Google Scholar] [CrossRef] [PubMed]
- Fraga, J.; Botelho, A.; Sá, A.; Costa, M.; Quaresma, M. The lag structure and the general effect of ozone exposure on pediatric respiratory morbidity. Int. J. Environ. Res. Public Health 2011, 8, 4013–4024. [Google Scholar] [CrossRef] [PubMed]
- Peng, R.D.; Dominici, F. Statistical Methods for Environmental Epidemiology with R: A Case Study in Air Pollution and Health Series; Springer: New York, NY, USA, 2008. [Google Scholar]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Youssouf, H.; Liousse, C.; Roblou, L.; Assamoi, E.-M.; Salonen, R.O.; Maesano, C.; Banerjee, S.; Annesi-Maesano, I. Non-Accidental Health Impacts of Wildfire Smoke. Int. J. Environ. Res. Public Health 2014, 11, 11772-11804. https://doi.org/10.3390/ijerph111111772
Youssouf H, Liousse C, Roblou L, Assamoi E-M, Salonen RO, Maesano C, Banerjee S, Annesi-Maesano I. Non-Accidental Health Impacts of Wildfire Smoke. International Journal of Environmental Research and Public Health. 2014; 11(11):11772-11804. https://doi.org/10.3390/ijerph111111772
Chicago/Turabian StyleYoussouf, Hassani, Catherine Liousse, Laurent Roblou, Eric-Michel Assamoi, Raimo O. Salonen, Cara Maesano, Soutrik Banerjee, and Isabella Annesi-Maesano. 2014. "Non-Accidental Health Impacts of Wildfire Smoke" International Journal of Environmental Research and Public Health 11, no. 11: 11772-11804. https://doi.org/10.3390/ijerph111111772
APA StyleYoussouf, H., Liousse, C., Roblou, L., Assamoi, E.-M., Salonen, R. O., Maesano, C., Banerjee, S., & Annesi-Maesano, I. (2014). Non-Accidental Health Impacts of Wildfire Smoke. International Journal of Environmental Research and Public Health, 11(11), 11772-11804. https://doi.org/10.3390/ijerph111111772