
Influence of Auditory Integrative Training on Casein Kinase 2 and Its Impact on Behavioral and Social Interaction in Children with Autism Spectrum Disorder
 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Childhood Autism Rating Scale
2.2. Social Responsiveness Scale
2.3. The Short Sensory Profile
2.4. Measurement of Plasma Casein Kinase-2 (CK2)
2.5. Statistical Analysis
3. Results and Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Baio, J.; Wiggins, L.; Christensen, D.L.; Maenner, M.J.; Daniels, J.; Warren, Z.; Dowling, N.F. Prevalence of Autism Spectrum Disorder Among Children Aged 8 Years—Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2014. MMWR Surveill. Summ. 2018, 67, 1. [Google Scholar] [CrossRef] [PubMed]
- Brugha, T.S.; Spiers, N.; Bankart, J.; Cooper, S.A.; McManus, S.; Scott, F.J.; Smith, J.; Tyrer, F. Epidemiology of autism in adults across age groups and ability levels. Br. J. Psychiatry 2016, 209, 498–503. [Google Scholar] [CrossRef] [PubMed]
- Fernell, E.; Landgren, M.; Lindström, K.; Johnson, M.; Gillberg, C. Children and young people with neurodevelopmental problems: Support and efforts must be given even if not all diagnostic criteria are met. Lakartidningen 2013, 110, 1674. [Google Scholar] [PubMed]
- Narayanan, A.; Jacobson, M.P. Computational studies of protein regulation by post-translational phosphorylation. Curr. Opin. Struct. Biol. 2009, 19, 156–163. [Google Scholar] [CrossRef] [PubMed]
- Olsen, J.V.; Vermeulen, M.; Santamaria, A.; Kumar, C.; Miller, M.L.; Jensen, L.J.; Gnad, F.; Cox, J.; Jensen, T.S.; Nigg, E.A.; et al. Quantitative phosphoproteomics revealswidespread full phosphorylation site occupancy during mitosis. Sci. Signal. 2010, 3, ra3. [Google Scholar] [CrossRef] [PubMed]
- Ishii, A.; Nonaka, T.; Taniguchi, S.; Saito, T.; Arai, T.; Mann, D.; Iwatsubo, T.; Hisanaga, S.-I.; Goedert, M.; Hasegawa, M. Casein kinase 2 is the major enzyme in brain that phosphorylates Ser129 of human α-synuclein: Implication for α-synucleinopathies. FEBS Lett. 2007, 581, 4711–4717. [Google Scholar] [CrossRef]
- Götz, C.; Montenarh, M. Protein kinase CK2 in development and differentiation (Review). Biomed. Rep. 2017, 6, 127–133. [Google Scholar] [CrossRef]
- Lettieri, A.; Borgo, C.; Zanieri, L.; D’amore, C.; Oleari, R.; Paganoni, A.; Pinna, L.A.; Cariboni, A.; Salvi, M. Protein Kinase CK2 Subunits Differentially Perturb the Adhesion and Migration of GN11 Cells: A Model of Immature Migrating Neurons. Int. J. Mol. Sci. 2019, 20, 5951. [Google Scholar] [CrossRef]
- Rebholz, H.; Nishi, A.; Liebscher, S.; Nairn, A.C.; Flajolet, M.; Greengard, P. CK2 Negatively Regulates G S Signaling. Proc. Natl. Acad. Sci. USA 2009, 106, 14096–14101. [Google Scholar] [CrossRef]
- Soto, D.; Pancetti, F.; Marengo, J.J.; Sandoval, M.; Sandoval, R.; Orrego, F.; Wyneken, U. Protein Kinase CK2 in Postsynaptic Densities: Phosphorylation of PSD-95/SAP90 and NMDA Receptor Regulation. Biochem. Biophys. Res. Commun. 2004, 322, 542–550. [Google Scholar] [CrossRef]
- Girault, J.A.; Hemmings, H.C., Jr.; Zorn, S.H.; Gustafson, E.L.; Greengard, P. Characterization in mammalian brain of a DARPP-32 serine kinase identical to casein kinase II. J. Neurochem. 1990, 55, 1772–1783. [Google Scholar] [CrossRef]
- Castello, J.; Ragnauth, A.; Friedman, E.; Rebholz, H. CK2—An emerging target for neurological and psychiatric disorders. Pharmaceuticals 2017, 10, 7. [Google Scholar] [CrossRef] [PubMed]
- Montenarh, M.; Götz, C. Protein Kinase CK2 and Ion Channels (Review). Biomed. Rep. 2020, 13, 55. [Google Scholar] [CrossRef] [PubMed]
- Castello, J.; LeFrancois, B.; Flajolet, M.; Greengard, P.; Friedman, E.; Rebholz, H. CK2 Regulates 5-HT4 Receptor Signaling and Modulates Depressive-like Behavior. Mol. Psychiatry 2018, 23, 872–882. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, T.; Yanagi, S. Psychiatric behaviors associated with cytoskeletal defects in radial neuronal migration. Cell. Mol. Life Sci. 2017, 74, 3533–3552. [Google Scholar] [CrossRef]
- Wegiel, J.; Kuchna, I.; Nowicki, K.; Imaki, H.; Wegiel, J.; Marchi, E.; Ma, S.Y.; Chauhan, A.; Chauhan, V.; Bobrowicz, T.W.; et al. The neuropathology of autism: Defects of neurogenesis and neuronal migration, and dysplastic changes. Acta Neuropathol. 2010, 119, 755–770. [Google Scholar] [CrossRef]
- Provenzano, G.; Chelini, G.; Bozzi, Y. Genetic control of social behavior: Lessons from mutant mice. Behav. Brain Res. 2017, 325, 237–250. [Google Scholar] [CrossRef]
- Ferguson, B.R.; Gao, W.J. Pv interneurons: Critical regulators of E/I balance for prefrontal cortex-dependent behavior and psychiatric disorders. Front. Neural Circuits 2018, 12, 37. [Google Scholar] [CrossRef]
- Bozzi, Y.; Provenzano, G.; Casarosa, S. Neurobiological bases of autism–epilepsy comorbidity: A focus on excitation/inhibition imbalance. Eur. J. Neurosci. 2018, 47, 534–548. [Google Scholar] [CrossRef]
- Gao, Z.; Lee, P.; Stafford, J.M.; Von Schimmelmann, M.; Schaefer, A.; Reinberg, D. An AUTS2–Polycomb complex activates gene expression in the CNS. Nature 2014, 516, 349–354. [Google Scholar] [CrossRef]
- Hori, K.; Shimaoka, K.; Hoshino, M. AUTS2 Gene: Keys to Understanding the Pathogenesis of Neurodevelopmental Disorders. Cells 2022, 11, 11. [Google Scholar] [CrossRef] [PubMed]
- Okur, V.; Cho, M.T.; Henderson, L.; Retterer, K.; Schneider, M.; Sattler, S.; Niyazov, D.; Azage, M.; Smith, S.; Picker, J.; et al. De novo mutations in CSNK2A1 are associated with neurodevelopmental abnormalities and dysmorphic features. Hum. Genet. 2016, 135, 699–705. [Google Scholar] [CrossRef] [PubMed]
- Gold, N.B.; Li, D.; Chassevent, A.; Kaiser, F.J.; Parenti, I.; Strom, T.M.; Ramos, F.J.; Puisac, B.; Pié, J.; McWalter, K.; et al. Heterozygous de novo variants in CSNK1G1 are associated with syndromic developmental delay and autism spectrum disorder. Clin. Genet. 2020, 98, 571–576. [Google Scholar] [CrossRef] [PubMed]
- Okochi, M.; Walter, J.; Koyama, A.; Nakajo, S.; Baba, M.; Iwatsubo, T.; Meijer, L.; Kahle, P.J.; Haass, C. Constitutive Phosphorylation of the Parkinson’s Disease Associated α-Synuclein. J. Biol. Chem. 2000, 275, 390–397. [Google Scholar] [CrossRef] [PubMed]
- Oueslati, A. Implication of Alpha-Synuclein Phosphorylation at S129 in Synucleinopathies: What Have We Learned in the Last Decade? J. Park. Dis. 2016, 6, 39–51. [Google Scholar] [CrossRef] [PubMed]
- Al-Mazidi, S.; Al-Ayadhi, L.Y. Plasma Levels of Alpha and Gamma Synucleins in Autism Spectrum Disorder: An Indicator of Severity. Med. Princ. Pract. 2021, 30, 160–167. [Google Scholar] [CrossRef]
- El-Ansary, A.; Alhakbany, M.; Aldbass, A.; Qasem, H.; Al-Mazidi, S.; Bhat, R.S.; Al-Ayadhi, L. Alpha-Synuclein, cyclooxygenase-2 and prostaglandins-EP2 receptors as neuroinflammatory biomarkers of autism spectrum disorders: Use of combined ROC curves to increase their diagnostic values. Lipids Health Dis. 2021, 20, 155. [Google Scholar] [CrossRef]
- Raghavan, K.; Dedeepiya, V.D.; Ikewaki, N.; Sonoda, T.; Iwasaki, M.; Preethy, S.; Abraham, S.J. Improvement of behavioural pattern and alpha-synuclein levels in autism spectrum disorder after consumption of a beta-glucan food supplement in a randomised, parallel-group pilot clinical study. BMJ Neurol. Open 2022, 4, e000203. [Google Scholar] [CrossRef]
- Turner, J.R. Intestinal mucosal barrier function in health and disease. Nat. Rev. Immunol. 2009, 9, 799–809. [Google Scholar] [CrossRef]
- Shen, L.; Weber, C.R.; Raleigh, D.R.; Yu, D.; Turner, J.R. Tight Junction Pore and Leak Pathways: A Dynamic Duo. Annu. Rev. Physiol. 2011, 73, 283–309. [Google Scholar] [CrossRef]
- Dörfel, M.J.; Westphal, J.K.; Bellmann, C.; Krug, S.M.; Cording, J.; Mittag, S.; Tauber, R.; Fromm, M.; Blasig, I.E.; Huber, O. CK2-dependent phosphorylation of occludin regulates the interaction with ZO-proteins and tight junction integrity. Cell Commun. Signal. 2013, 11, 40. [Google Scholar] [CrossRef] [PubMed]
- Liu, D.; Marie, J.C.; Pelletier, A.L.; Song, Z.; Ben-Khemis, M.; Boudiaf, K.; Pintard, C.; Leger, T.; Terrier, S.; Chevreux, G.; et al. Protein Kinase CK2 Acts as a Molecular Brake to Control NADPH Oxidase 1 Activation and Colon Inflammation. Cell. Mol. Gastroenterol. Hepatol. 2022, 13, 1073–1093. [Google Scholar] [CrossRef] [PubMed]
- Paul, R. Interventions to Improve Communication in Autism. Child Adolesc. Psychiatr. Clin. North Am. 2008, 17, 835–856. [Google Scholar] [CrossRef] [PubMed]
- Sinha, Y.; Silove, N.; Hayen, A.; Williams, K. Auditory integration training and other sound therapies for autism spectrum disorders (ASD). Cochrane Database Syst. Rev. 2011, 2011, CD003681. [Google Scholar] [CrossRef]
- Rotschafer, S.E. Auditory Discrimination in Autism Spectrum Disorder. Front. Neurosci. 2021, 15, 651209. [Google Scholar] [CrossRef]
- Ventola, P.E.; Kleinman, J.; Pandey, J.; Barton, M.; Allen, S.; Green, J.; Robins, D.; Fein, D. Agreement Among Four Diagnostic Instruments for Autism Spectrum Disorders in Toddlers. J. Autism Dev. Disord. 2006, 36, 839–847. [Google Scholar] [CrossRef]
- Constantino, J.N.; Davis, S.A.; Todd, R.D.; Schindler, M.K.; Gross, M.M.; Brophy, S.L.; Reich, W. Validation of a Brief Quantitative Measure of Autistic Traits: Comparison of the Social Responsiveness Scale with the Autism Diagnostic Interview-Revised. J. Autism Dev. Disord. 2003, 33, 427–433. [Google Scholar] [CrossRef]
- Dunn, W.; Daniels, D.B. Initial Development of the Infant/Toddler Sensory Profile. J. Early Interv. 2022, 25, 27–41. [Google Scholar] [CrossRef]
- Al-Ayadhi, L.; Al-Drees, A.; Al-Arfaj, A. Effectiveness of Auditory Integration Therapy in Autism Spectrum Disorders--Prospective Study. Autism Insights 2013, 5, 13–20. [Google Scholar] [CrossRef]
- Perrin, J.M.; Coury, D.L.; Hyman, S.L.; Cole, L.; Reynolds, A.M.; Clemons, T. Complementary and Alternative Medicine Use in a Large Pediatric Autism Sample. Pediatrics 2012, 130 (Suppl. S2), S77–S82. [Google Scholar] [CrossRef]
- El-Ansary, A.; Hassan, W.M.; Daghestani, M.; Al-Ayadhi, L.; Ben Bacha, A. Preliminary evaluation of a novel nine-biomarker profile for the prediction of autism spectrum disorder. PLoS ONE 2020, 15, e0227626. [Google Scholar] [CrossRef] [PubMed]
- Heuer, L.S.; Croen, L.A.; Jones, K.L.; Yoshida, C.K.; Hansen, R.L.; Yolken, R.; Zerbo, O.; DeLorenze, G.; Kharrazi, M.; Ashwood, P.; et al. An Exploratory Examination of Neonatal Cytokines and Chemokines as Predictors of Autism Risk: The Early Markers for Autism Study. Biol. Psychiatry 2019, 86, 255–264. [Google Scholar] [CrossRef] [PubMed]
- Frye, R.E.; Melnyk, S.; Macfabe, D.F. Unique acyl-carnitine profiles are potential biomarkers for acquired mitochondrial disease in autism spectrum disorder. Transl. Psychiatry 2013, 3, e220. [Google Scholar] [CrossRef]
- Al-Ayadhi, L.; Zayed, N.; Bhat, R.S.; Moubayed, N.M.S.; Al-Muammar, M.N.; El-Ansary, A. The use of biomarkers associated with leaky gut as a diagnostic tool for early intervention in autism spectrum disorder: A systematic review. Gut Pathog. 2021, 13, 54. [Google Scholar] [CrossRef]
- Montanari, M.; Martella, G.; Bonsi, P.; Meringolo, M. Autism Spectrum Disorder: Focus on Glutamatergic Neurotransmission. Int. J. Mol. Sci. 2022, 23, 3861. [Google Scholar] [CrossRef] [PubMed]
- Caia, J.; Ding, L.; Zhang, J.S.; Xue, J.; Wang, L.Z. Elevated plasma levels of glutamate in children with autism spectrum disorders. NeuroReport 2016, 27, 272–276. [Google Scholar] [CrossRef] [PubMed]
- Tilleux, S.; Hermans, E. Neuroinflammation and regulation of glial glutamate uptake in neurological disorders. J. Neurosci. Res. 2007, 85, 2059–2070. [Google Scholar] [CrossRef]
- Domercq, M.; Perez-Samartin, A.; Aparicio, D.; Alberdi, E.; Pampliega, O.; Matute, C. P2X7 receptors mediate ischemic damage to oligodendrocytes. Glia 2009, 58, 730–740. [Google Scholar] [CrossRef]
- Pampliega, O.; Domercq, M.; Soria, F.N.; Villoslada, P.; Rodríguez-Antigüedad, A.; Matute, C. Increased expression of cystine/glutamate antiporter in multiple sclerosis. J. Neuroinflammation 2011, 8, 63. [Google Scholar] [CrossRef]
- El-Ansary, A.K.; Ben Bacha, A.G.; Al-Ayadhi, L.Y. Proinflammatory and proapoptotic markers in relation to mono and di-cations in plasma of autistic patients from Saudi Arabia. J. Neuroinflammation 2011, 8, 142. [Google Scholar] [CrossRef]
- Axtell, R.C.; Xu, L.; Barnum, S.R.; Raman, C. CD5-CK2 Binding/Activation-Deficient Mice Are Resistant to Experimental Autoimmune Encephalomyelitis: Protection Is Associated with Diminished Populations of IL-17-Expressing T Cells in the Central Nervous System. J. Immunol. 2006, 177, 8542–8549. [Google Scholar] [CrossRef] [PubMed]
- Sestero, C.M.; McGuire, D.J.; De Sarno, P.; Brantley, E.C.; Soldevila, G.; Axtell, R.C.; Raman, C. CD5-Dependent CK2 Activation Pathway Regulates Threshold for T Cell Anergy. J. Immunol. 2012, 189, 2918–2930. [Google Scholar] [CrossRef] [PubMed]
- Mier-Aguilar, C.A.; Cashman, K.S.; Raman, C.; Soldevila, G. CD5-CK2 Signaling Modulates Erk Activation and Thymocyte Survival. PLoS ONE 2016, 11, e0168155. [Google Scholar] [CrossRef] [PubMed]
- Ulges, A.; Witsch, E.J.; Pramanik, G.; Klein, M.; Birkner, K.; Bühler, U.; Wasser, B.; Luessi, F.; Stergiou, N.; Dietzen, S.; et al. Protein kinase CK2 governs the molecular decision between encephalitogenic T H 17 cell and T reg cell development. Proc. Natl. Acad. Sci. USA 2016, 113, 10145–10150. [Google Scholar] [CrossRef] [PubMed]
- Canedo-Antelo, M.; Serrano, M.P.; Manterola, A.; Ruiz, A.; Llavero, F.; Mato, S.; Zugaza, J.L.; Pérez-Cerdá, F.; Matute, C.; Sánchez-Gómez, M.V. Inhibition of Casein Kinase 2 Protects Oligodendrocytes from Excitotoxicity by Attenuating JNK/p53 Signaling Cascade. Front. Mol. Neurosci. 2018, 11, 333. [Google Scholar] [CrossRef]
- Hafizi, S.; Tabatabaei, D.; Lai, M.-C. Review of Clinical Studies Targeting Inflammatory Pathways for Individuals with Autism. Front. Psychiatry 2019, 10, 849. [Google Scholar] [CrossRef]
- Tsilioni, I.; Taliou, A.; Francis, K.; Theoharides, T.C. Children with autism spectrum disorders, who improved with a luteolin-containing dietary formulation, show reduced serum levels of TNF and IL-6. Transl. Psychiatry 2015, 5, e647. [Google Scholar] [CrossRef]
- Bertolino, B.; Crupi, R.; Impellizzeri, D.; Bruschetta, G.; Cordaro, M.; Siracusa, R.; Cuzzocrea, S. Beneficial Effects of Co-Ultramicronized Palmitoylethanolamide/Luteolin in a Mouse Model of Autism and in a Case Report of Autism. CNS Neurosci. Ther. 2017, 23, 87–98. [Google Scholar] [CrossRef]
- Williams, Z.J.; Failla, M.D.; Gotham, K.O.; Woynaroski, T.G.; Cascio, C. Psychometric Evaluation of the Short Sensory Profile in Youth with Autism Spectrum Disorder. J. Autism Dev. Disord. 2018, 48, 4231–4249. [Google Scholar] [CrossRef]
- Raleigh, D.R.; Boe, D.M.; Yu, D.; Weber, C.R.; Marchiando, A.M.; Bradford, E.M.; Wang, Y.; Wu, L.; Schneeberger, E.E.; Shen, L.; et al. Occludin S408 phosphorylation regulates tight junction protein interactions and barrier function. J. Cell Biol. 2011, 193, 565–582. [Google Scholar] [CrossRef]
- White, A.; McGlone, A.; Gomez-Pastor, R. Protein Kinase CK2 and Its Potential Role as a Therapeutic Target in Huntington’s Disease. Biomedicines 2022, 10, 1979. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Min. | Max. | Median | Percent Change | p Value | |
|---|---|---|---|---|---|
| Before | 0.406 | 5.317 | 2.447 | 100.00% | |
| Immediately after | 0.462 | 5.476 | 1.984 | 81.08% | 0.049 |
| 1 month after | 0.533 | 4.36 | 2.104 | 85.98% | 0.052 |
| 3 months after | 0.127 | 5.851 | 2.032 | 83.04% | 0.046 |
| CARS | Min. | Max. | Mean ± S.D. | Percent Change | p Value |
|---|---|---|---|---|---|
| Before | 22 | 52 | 36.84 ± 10.95 | 100.00% | |
| 1 month after | 23 | 38 | 29.81 ± 6.24 | 80.92% | 0.003 |
| 3 months after | 22 | 37 | 29.36 ± 6.06 | 79.70% | 0.008 |
| SRS | Min. | Max. | Mean ± S.D. | Percent Change | p Value |
|---|---|---|---|---|---|
| Before | 138 | 203 | 179.42 ± 19.48 | 100.00% | |
| 1 month after | 78 | 218 | 168.23 ± 32.14 | 93.76% | 0.002 |
| 3 months after | 54 | 171 | 142.88 ± 27.23 | 79.64% | 0.001 |
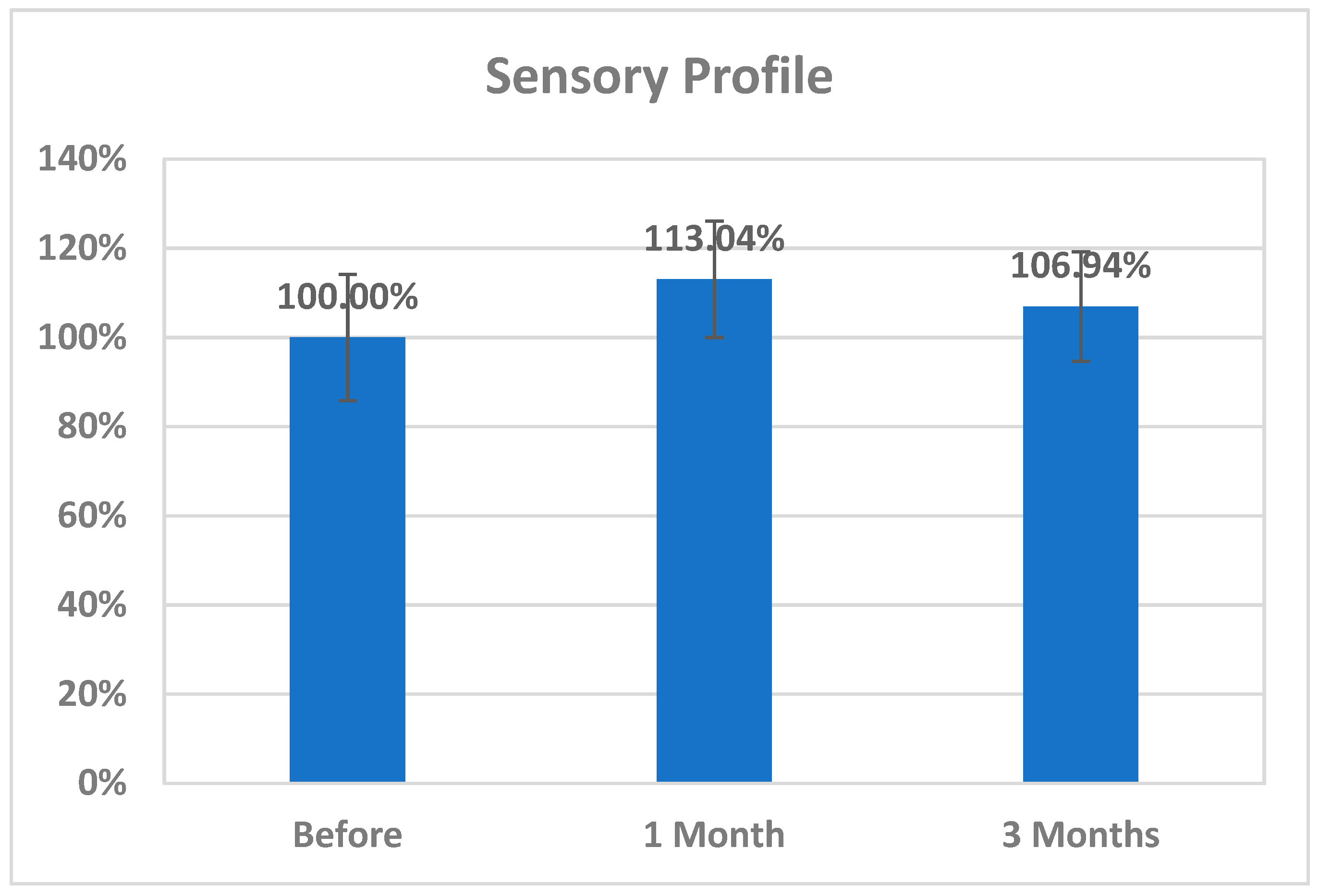
| Sensory Profile | Min. | Max. | Mean ± S.D. | Percent Change | p Value |
|---|---|---|---|---|---|
| Before | 87 | 190 | 144.56 ± 35.08 | 100.00% | |
| 1 month after | 129 | 190 | 163.40 ± 20.85 | 113.04% | 0.223 |
| 3 months after | 112 | 190 | 154.59 ± 23.25 | 106.94% | 0.612 |
| GI Symptoms | Before | One Month | Three Months |
|---|---|---|---|
| Vomiting after eating | 5 | 0 | 0 |
| Reflux bloating | 15 | 11 | 13 |
| Diarrhea | 8 | 1 | 1 |
| Constipation | 17 | 1 | 0 |
| Colic | 22 | 2 | 0 |
| Itchy skin | 12 | 1 | 1 |
| Rash | 6 | 0 | 0 |
| Irritability | 25 | 4 | 0 |
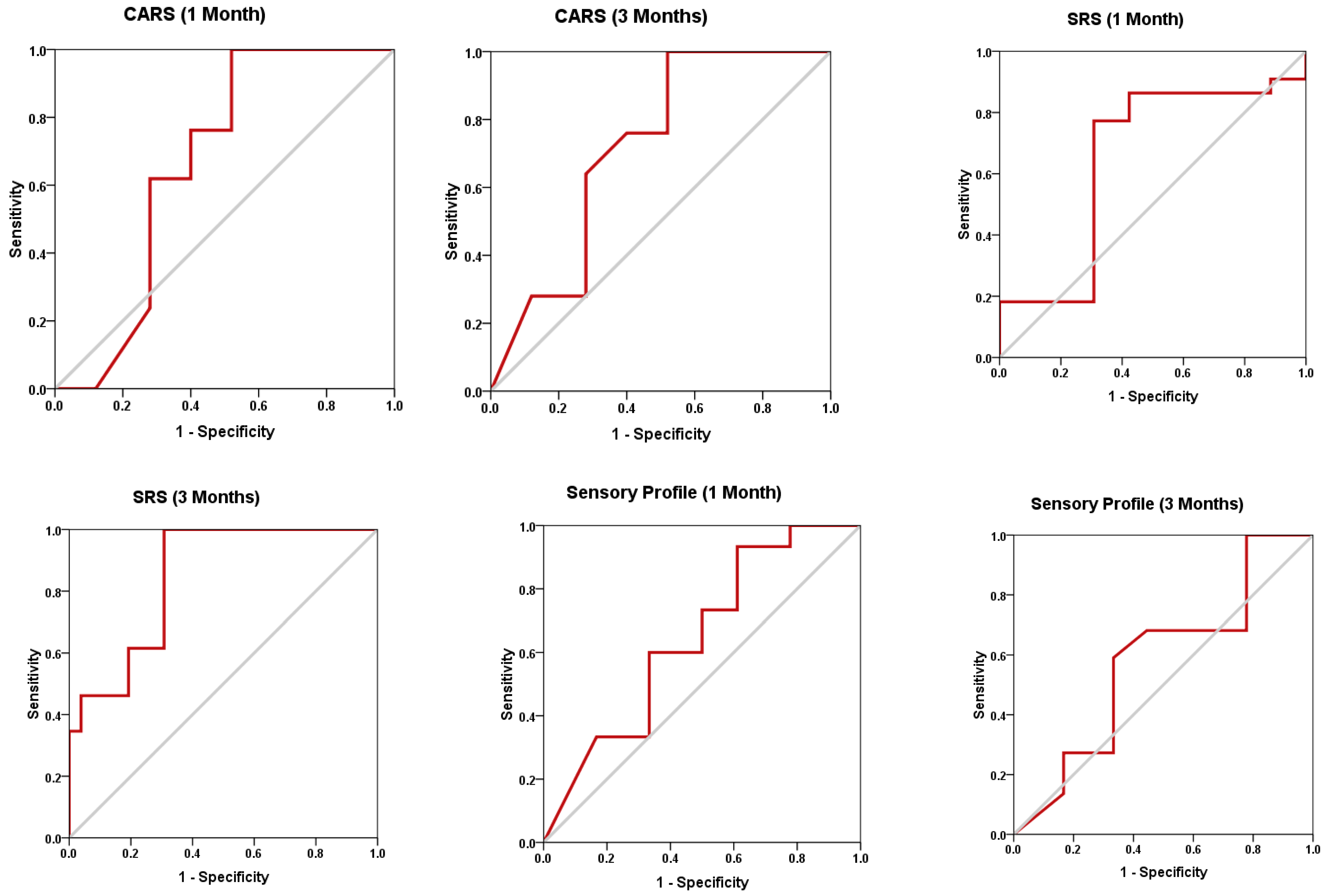
| Duration | AUC | Cut-Off Value | Sensitivity % | Specificity % | p Value | 95% CI |
|---|---|---|---|---|---|---|
| CK2 immediately after | 0.573 | 2.076 | 56.5% | 63.6% | 0.401 | 0.402–0.745 |
| CK2 1 month after | 0.564 | 2.327 | 70.0% | 54.5% | 0.481 | 0.386–0.741 |
| CK2 3 months after | 0.598 | 1.893 | 50.0% | 63.6% | 0.253 | 0.433–0.764 |
| SRS 1 month after | 0.649 | 180.000 | 77.3% | 69.2% | 0.079 | 0.481–0.816 |
| SRS 3 months after | 0.848 | 176.000 | 100.0% | 69.2% | 0.000 | 0.742–0.954 |
| CARS 1 month after | 0.665 | 39.000 | 100.0% | 48.0% | 0.056 | 0.500–0.830 |
| CARS 3 months after | 0.717 | 38.500 | 100.0% | 48.0% | 0.009 | 0.570–0.864 |
| Sensory Profile (1 month after) | 0.643 | 145.000 | 93.3% | 38.9% | 0.164 | 0.453–0.832 |
| Sensory Profile (3 months after) | 0.577 | 156.500 | 59.1% | 66.7% | 0.407 | 0.391–0.763 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Ayadhi, L.; Bhat, R.S.; Alghamdi, F.A.; Alhadlaq, A.S.; El-Ansary, A. Influence of Auditory Integrative Training on Casein Kinase 2 and Its Impact on Behavioral and Social Interaction in Children with Autism Spectrum Disorder. Curr. Issues Mol. Biol. 2023, 45, 4317-4330. https://doi.org/10.3390/cimb45050274
Al-Ayadhi L, Bhat RS, Alghamdi FA, Alhadlaq AS, El-Ansary A. Influence of Auditory Integrative Training on Casein Kinase 2 and Its Impact on Behavioral and Social Interaction in Children with Autism Spectrum Disorder. Current Issues in Molecular Biology. 2023; 45(5):4317-4330. https://doi.org/10.3390/cimb45050274
Chicago/Turabian StyleAl-Ayadhi, Laila, Ramesa Shafi Bhat, Farah Ali Alghamdi, Abdulmalik S. Alhadlaq, and Afaf El-Ansary. 2023. "Influence of Auditory Integrative Training on Casein Kinase 2 and Its Impact on Behavioral and Social Interaction in Children with Autism Spectrum Disorder" Current Issues in Molecular Biology 45, no. 5: 4317-4330. https://doi.org/10.3390/cimb45050274
APA StyleAl-Ayadhi, L., Bhat, R. S., Alghamdi, F. A., Alhadlaq, A. S., & El-Ansary, A. (2023). Influence of Auditory Integrative Training on Casein Kinase 2 and Its Impact on Behavioral and Social Interaction in Children with Autism Spectrum Disorder. Current Issues in Molecular Biology, 45(5), 4317-4330. https://doi.org/10.3390/cimb45050274