
SARS-CoV-2 Reinfection Is a New Challenge for the Effectiveness of Global Vaccination Campaign: A Systematic Review of Cases Reported in Literature



Abstract
:1. Introduction
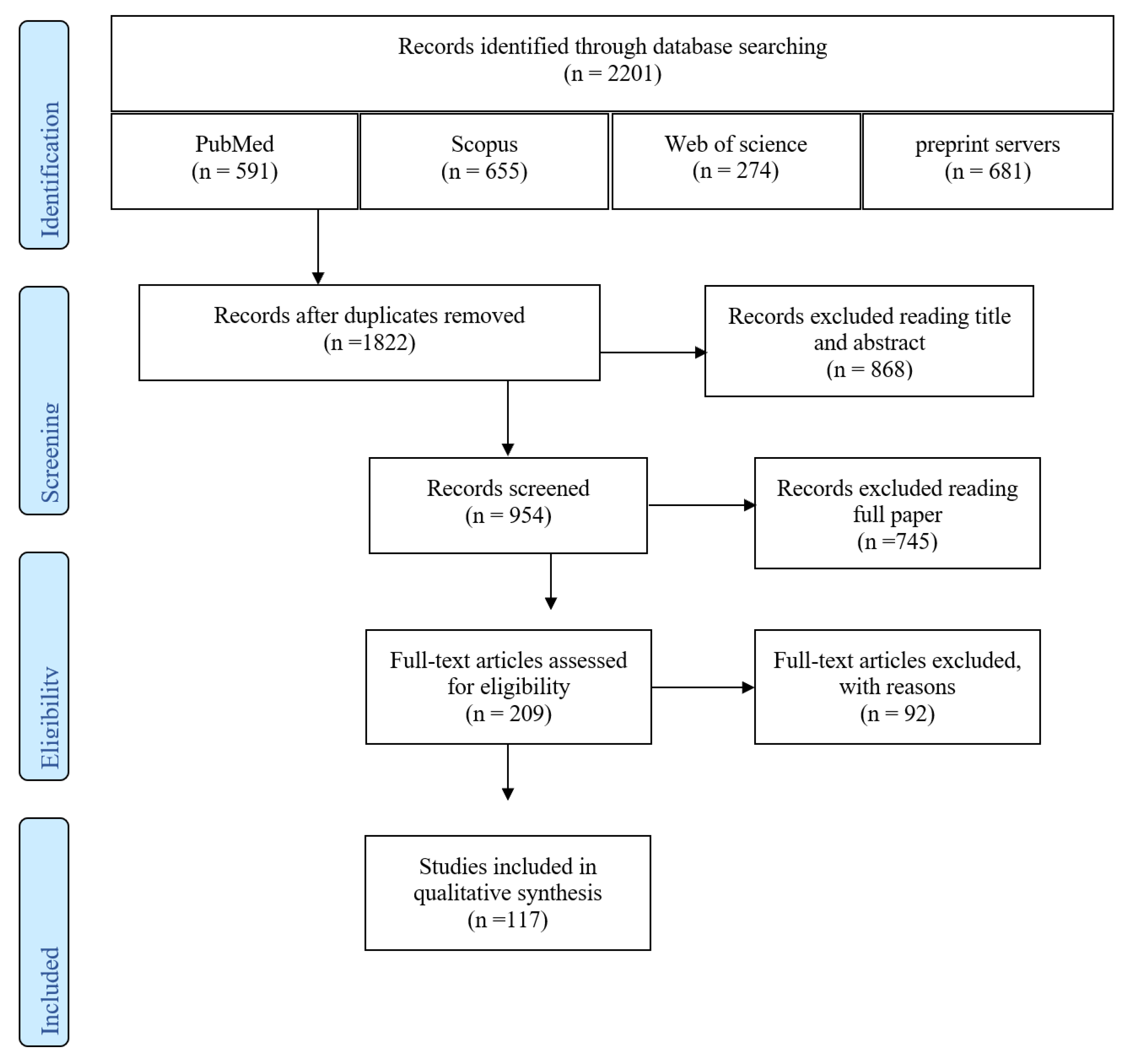
2. Materials and Methods
2.1. Data Sources
2.2. Study Selection
2.3. Data Extraction
2.4. Quality and Risk of Bias Assessment
3. Results
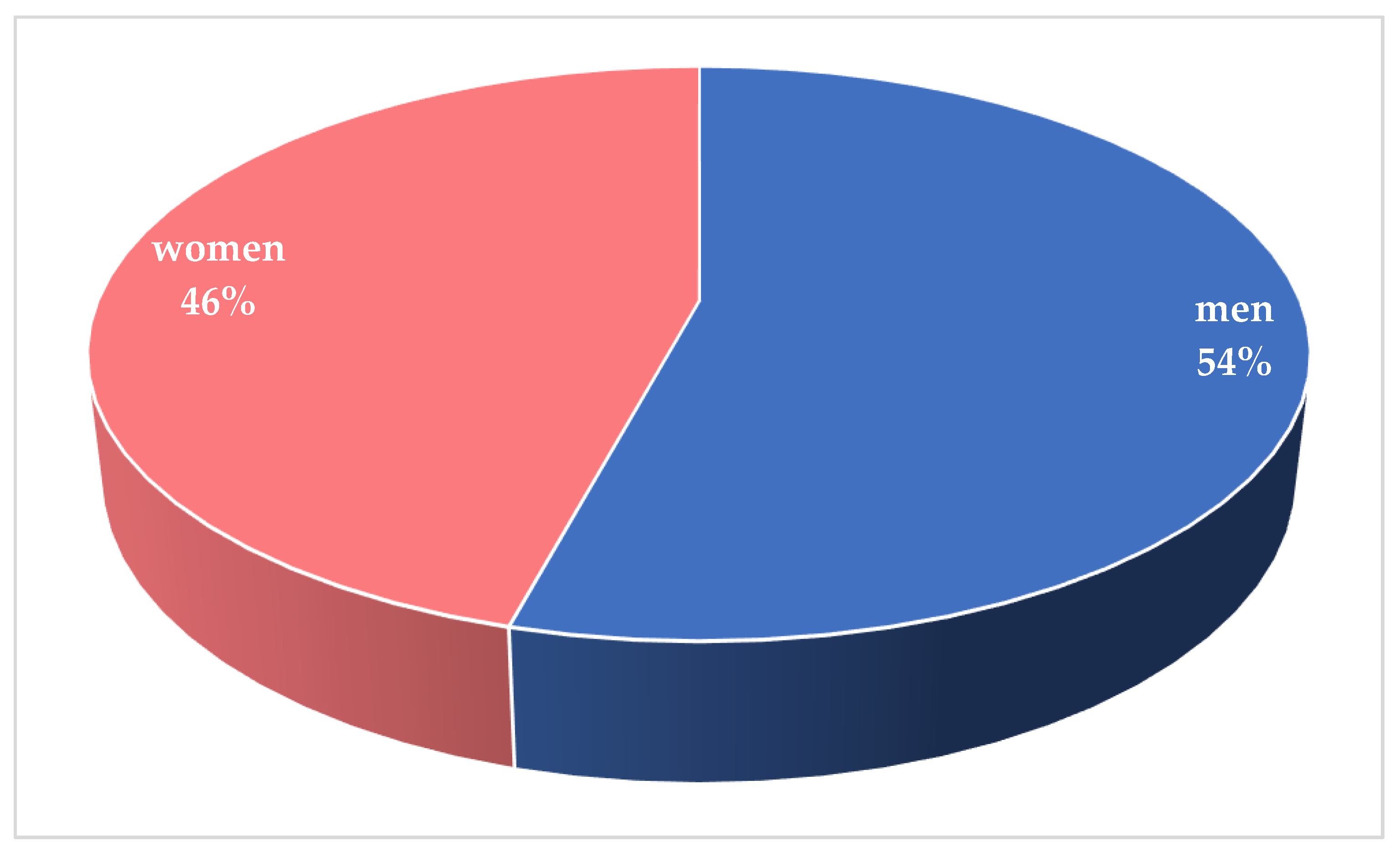
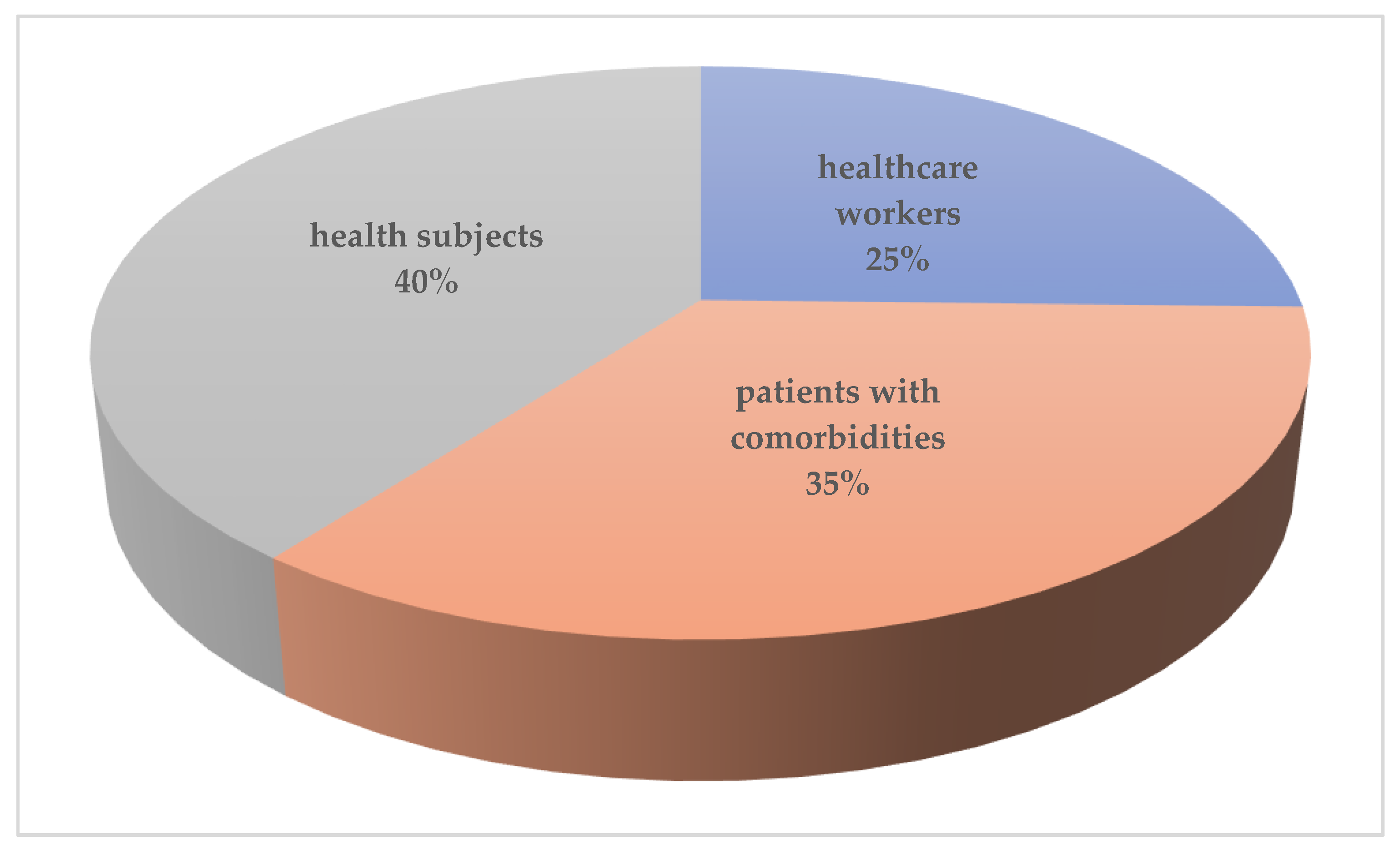
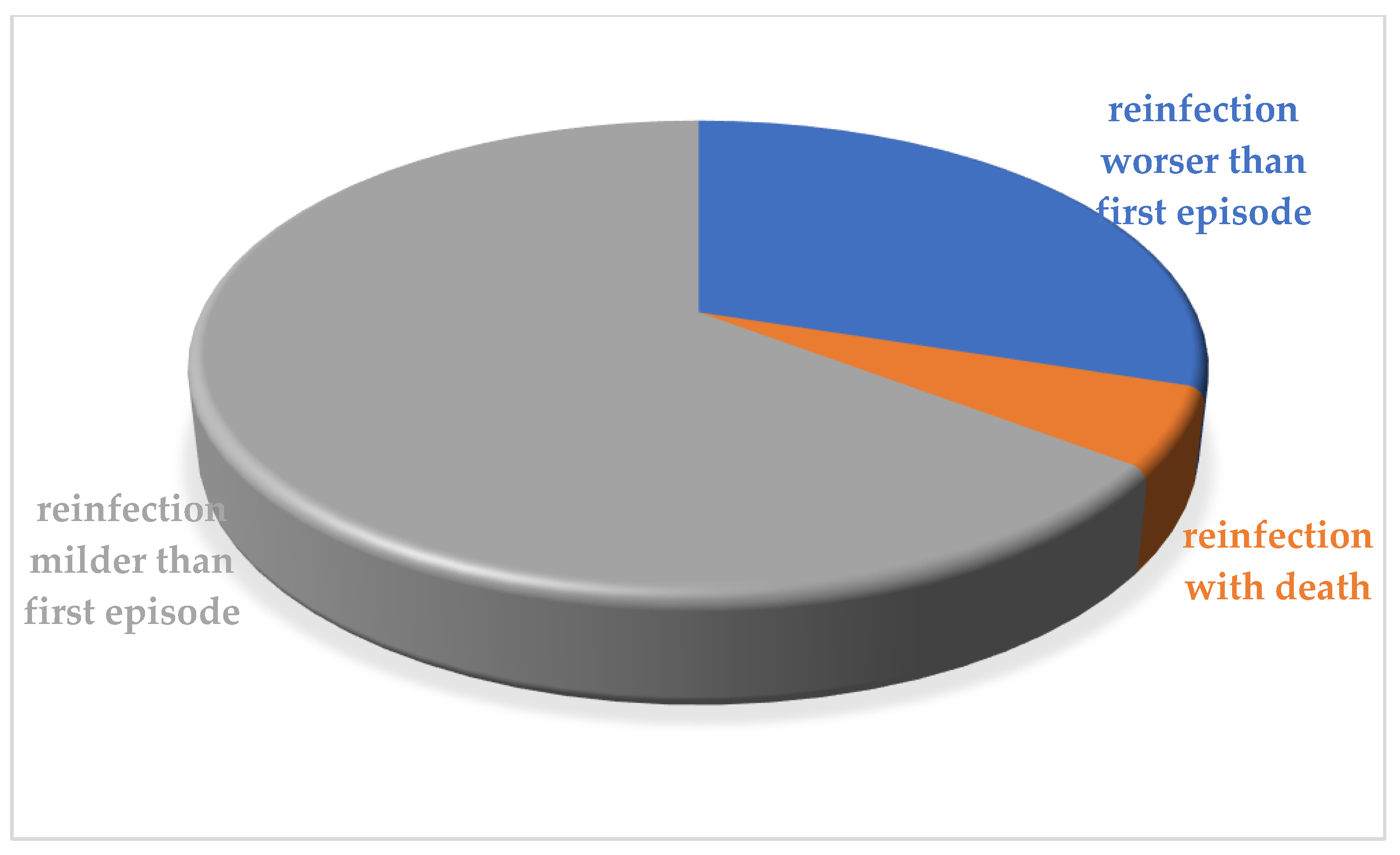
3.1. Demographic and Clinical Features of Reinfection Cases
3.2. Quality and Risk of Bias Assessment
4. Discussion
- (1)
- Infected cases with very mild symptoms or asymptomatic without any humoral immune response or elicited memory.
- (2)
- Infected cases with mild to moderate symptoms with low humoral immunity and low cellular immunity.
- (3)
- Infected cases with moderate or severe symptoms with highly activated humoral immunity and elicited memory.
- (4)
- Infected cases with moderate or severe symptoms with highly activated humoral immunity and low cellular immunity [175].
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef]
- Wang, C.; Horby, P.W.; Hayden, F.G.; Gao, G.F. A novel coronavirus outbreak of global health concern. Lancet 2020, 395, 470–473. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Rolling Updates on Corona Virus Disease (COVID-19). Health Emergencies. 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/events-as-they-happen (accessed on 1 October 2021).
- John Hopkins University. COVID-19 Dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU). Available online: https://coronavirus.jhu.edu/map.html (accessed on 17 October 2021).
- To, K.K.; Hung, I.F.; Ip, J.D.; Chu, A.W.; Chan, W.M.; Tam, A.R.; Fong, C.H.; Yuan, S.; Tsoi, H.W.; Ng, A.C.; et al. COVID-19 re-infection by a phylogenetically distinct SARS-coronavirus-2 strain confirmed by whole genome sequencing. Clin. Infect. Dis. 2020, ciaa1275. [Google Scholar] [CrossRef]
- Babiker, A.; Marvil, C.E.; Waggoner, J.J.; Collins, M.H.; Piantadosi, A. The Importance and Challenges of Identifying SARS-CoV-2 Reinfections. J. Clin. Microbiol. 2021, 59, e02769-20. [Google Scholar] [CrossRef]
- Edridge, A.W.D.; Kaczorowska, J.; Hoste, A.C.R.; Bakker, M.; Klein, M.; Loens, K.; Jebbink, M.F.; Matser, A.; Kinsella, C.M.; Rueda, P.; et al. Seasonal coronavirus protective immunity is short-lasting. Nat. Med. 2020, 26, 1691–1693. [Google Scholar] [CrossRef] [PubMed]
- Kiyuka, P.K.; Agoti, C.N.; Munywoki, P.K.; Njeru, R.; Bett, A.; Otieno, J.R.; Otieno, G.P.; Kamau, E.; Clark, T.G.; van der Hoek, L.; et al. Human Coronavirus NL63 Molecular Epidemiology and Evolutionary Patterns in Rural Coastal Kenya. J. Infect. Dis. 2018, 217, 1728–1739. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glezen, W.P.; Taber, L.H.; Frank, A.L.; Kasel, J.A. Risk of primary infection and reinfection with respiratory syncytial virus. Am. J. Dis. Child. 1986, 140, 543–546. [Google Scholar] [CrossRef] [PubMed]
- Perera, R.A.; Mok, C.K.; Tsang, O.T.; Lv, H.; Ko, R.L.; Wu, N.C.; Yuan, M.; Leung, W.S.; Chan, J.M.; Chik, T.S.; et al. Serological assays for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), March 2020. Eurosurveill 2020, 25, 2000421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hachim, A.; Kavian, N.; Cohen, C.A.; Chin, A.W.H.; Chu, D.K.W.; Mok, C.K.P.; Tsang, O.T.Y.; Yeung, Y.C.; Perera, R.; Poon, L.L.M.; et al. ORF8 and ORF3b antibodies are accurate serological markers of early and late SARS-CoV-2 infection. Nat. Immunol. 2020, 21, 1293–1301. [Google Scholar] [CrossRef]
- Addetia, A.; Crawford, K.H.D.; Dingens, A.; Zhu, H.; Roychoudhury, P.; Huang, M.L.; Jerome, K.R.; Bloom, J.D.; Greninger, A.L. Neutralizing Antibodies Correlate with Protection from SARS-CoV-2 in Humans during a Fishery Vessel Outbreak with a High Attack Rate. J. Clin. Microbiol. 2020, 58, e02107-20. [Google Scholar] [CrossRef]
- Sharma, R.; Sardar, S.; Mohammad Arshad, A.; Ata, F.; Zara, S.; Munir, W. A Patient with Asymptomatic SARS-CoV-2 Infection Who Presented 86 Days Later with COVID-19 Pneumonia Possibly Due to Reinfection with SARS-CoV-2. Am. J. Case Rep. 2020, 21, e927154. [Google Scholar] [CrossRef]
- Azkur, A.K.; Akdis, M.; Azkur, D.; Sokolowska, M.; van de Veen, W.; Bruggen, M.C.; O’Mahony, L.; Gao, Y.; Nadeau, K.; Akdis, C.A. Immune response to SARS-CoV-2 and mechanisms of immunopathological changes in COVID-19. Allergy 2020, 75, 1564–1581. [Google Scholar] [CrossRef]
- Long, Q.X.; Tang, X.J.; Shi, Q.L.; Li, Q.; Deng, H.J.; Yuan, J.; Hu, J.L.; Xu, W.; Zhang, Y.; Lv, F.J.; et al. Clinical and immunological assessment of asymptomatic SARS-CoV-2 infections. Nat. Med. 2020, 26, 1200–1204. [Google Scholar] [CrossRef]
- Amikishiyev, S.; Demir, E.; Aghamuradov, S.; Garayeva, N.; Artan, A.S.; Gul, A.; Turkmen, A. Reinfection with SARS-CoV-2 in a kidney transplant recipient. Transpl. Infect. Dis. 2021, 23, e13695. [Google Scholar] [CrossRef]
- Falahi, S.; Kenarkoohi, A. COVID-19 reinfection: Prolonged shedding or true reinfection? New Microbes New Infect. 2020, 38, 100812. [Google Scholar] [CrossRef] [PubMed]
- Xiao, A.T.; Tong, Y.X.; Gao, C.; Zhu, L.; Zhang, Y.J.; Zhang, S. Dynamic profile of RT-PCR findings from 301 COVID-19 patients in Wuhan, China: A descriptive study. J. Clin. Virol. 2020, 127, 104346. [Google Scholar] [CrossRef] [PubMed]
- Lan, L.; Xu, D.; Ye, G.; Xia, C.; Wang, S.; Li, Y.; Xu, H. Positive RT-PCR Test Results in Patients Recovered From COVID-19. JAMA 2020, 323, 1502–1503. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gombar, S.; Chang, M.; Hogan, C.A.; Zehnder, J.; Boyd, S.; Pinsky, B.A.; Shah, N.H. Persistent detection of SARS-CoV-2 RNA in patients and healthcare workers with COVID-19. J. Clin. Virol. 2020, 129, 104477. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Common Investigation Protocol for Investigating Suspected SARS-CoV-2 Reinfection. Available online: https://www.cdc.gov/coronavirus/2019-ncov/php/reinfection.html (accessed on 30 December 2020).
- Qureshi, A.I.; Baskett, W.I.; Huang, W.; Lobanova, I.; Naqvi, S.H.; Shyu, C.R. Re-infection with SARS-CoV-2 in Patients Undergoing Serial Laboratory Testing. Clin. Infect. Dis. 2021. [Google Scholar] [CrossRef]
- Leidi, A.; Koegler, F.; Dumont, R.; Dubos, R.; Zaballa, M.E.; Piumatti, G.; Coen, M.; Berner, A.; Darbellay Farhoumand, P.; Vetter, P.; et al. Risk of reinfection after seroconversion to SARS-CoV-2: A population-based propensity-score matched cohort study. Clin. Infect. Dis. 2021. [Google Scholar] [CrossRef]
- Breathnach, A.S.; Riley, P.A.; Cotter, M.P.; Houston, A.C.; Habibi, M.S.; Planche, T.D. Prior COVID-19 significantly reduces the risk of subsequent infection, but reinfections are seen after eight months. J. Infect. 2021, 82, e11–e12. [Google Scholar] [CrossRef] [PubMed]
- Bongiovanni, M.; Marra, A.M.; Bini, F.; Bodini, B.D.; Carlo, D.D.; Giuliani, G. COVID-19 reinfection in healthcare workers: A case series. J. Infect. 2021, 82, e4–e5. [Google Scholar] [CrossRef]
- Vitale, J.; Mumoli, N.; Clerici, P.; De Paschale, M.; Evangelista, I.; Cei, M.; Mazzone, A. Assessment of SARS-CoV-2 Reinfection 1 Year After Primary Infection in a Population in Lombardy, Italy. JAMA Intern. Med. 2021, 181, 1407–1408. [Google Scholar] [CrossRef]
- Tillett, R.L.; Sevinsky, J.R.; Hartley, P.D.; Kerwin, H.; Crawford, N.; Gorzalski, A.; Laverdure, C.; Verma, S.C.; Rossetto, C.C.; Jackson, D.; et al. Genomic evidence for reinfection with SARS-CoV-2: A case study. Lancet Infect. Dis. 2021, 21, 52–58. [Google Scholar] [CrossRef]
- Prado-Vivar, B.; Becerra-Wong, M.; Guadalupe, J.J.; Marquez, S.; Gutierrez, B.; Rojas-Silva, P.; Grunauer, M.; Trueba, G.; Barragan, V.; Cardenas, P. A case of SARS-CoV-2 reinfection in Ecuador. Lancet Infect. Dis. 2021, 21, e142. [Google Scholar] [CrossRef]
- Van Elslande, J.; Vermeersch, P.; Vandervoort, K.; Wawina-Bokalanga, T.; Vanmechelen, B.; Wollants, E.; Laenen, L.; Andre, E.; Van Ranst, M.; Lagrou, K.; et al. Symptomatic Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Reinfection by a Phylogenetically Distinct Strain. Clin. Infect. Dis. 2021, 73, 354–356. [Google Scholar] [CrossRef]
- Goldman, J.D.; Wang, K.; Roltgen, K.; Nielsen, S.C.A.; Roach, J.C.; Naccache, S.N.; Yang, F.; Wirz, O.F.; Yost, K.E.; Lee, J.Y.; et al. Reinfection with SARS-CoV-2 and Failure of Humoral Immunity: A case report. medRxiv 2020. [Google Scholar] [CrossRef]
- Klein, J.; Brito, A.F.; Trubin, P.; Lu, P.; Wong, P.; Alpert, T.; Pena-Hernandez, M.A.; Haynes, W.; Kamath, K.; Liu, F.; et al. Case Study: Longitudinal immune profiling of a SARS-CoV-2 reinfection in a solid organ transplant recipient. medRxiv 2021. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Investigative Criteria for Suspected Cases of SARS-CoV-2 Reinfection (ICR). Available online: https://www.cdc.gov/coronavirus/2019-ncov/php/invest-criteria.html (accessed on 2 July 2021).
- Murad, M.H.; Sultan, S.; Haffar, S.; Bazerbachi, F. Methodological quality and synthesis of case series and case reports. BMJ Evid. Based Med. 2018, 23, 60–63. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Clinical Management of Severe Acute Respiratory Infection When COVID-19 Is Suspected: Interim Guidance. 13 March 2020. Available online: https://www.who.int/docs/default-source/coronaviruse/clinical-management-of-novel-cov.pdf?sfvrsn=bc7da517_2 (accessed on 26 May 2020).
- Abu-Raddad, L.J.; Chemaitelly, H.; Malek, J.A.; Ahmed, A.A.; Mohamoud, Y.A.; Younuskunju, S.; Ayoub, H.H.; Al Kanaani, Z.; Al Khal, A.; Al Kuwari, E.; et al. Assessment of the risk of SARS-CoV-2 reinfection in an intense re-exposure setting. Clin. Infect. Dis. 2020, 73, e1830–e1840. [Google Scholar] [CrossRef] [PubMed]
- Adrielle Dos Santos, L.; Filho, P.G.G.; Silva, A.M.F.; Santos, J.V.G.; Santos, D.S.; Aquino, M.M.; de Jesus, R.M.; Almeida, M.L.D.; da Silva, J.S.; Altmann, D.M.; et al. Recurrent COVID-19 including evidence of reinfection and enhanced severity in thirty Brazilian healthcare workers. J. Infect. 2021, 82, 399–406. [Google Scholar] [CrossRef]
- Aguilar-Shea, A.L.; Gutierrez-Martin-Arroyo, J.; Vacas-Cordoba, M.; Gallardo-Mayo, C. Reinfection by SARS-CoV-2: The first one in a family reported in Spain. Med. Clin. 2021. [Google Scholar] [CrossRef]
- Ahmadian, S.; Fathizadeh, H.; Shabestari Khiabani, S.; Asgharzadeh, M.; Kafil, H.S. COVID-19 reinfection in a healthcare worker after exposure with high dose of virus: A case report. Clin. Case Rep. 2021, 9, e04257. [Google Scholar] [CrossRef]
- Ahmed, A.; Sana, F.; Ikram, A.; Yousaf, S.; Khan, A. Reinfection or relapse of COVID-19 in health care workers; case series of 2 patients from Pakistan. New Microbes New Infect. 2021, 42, 100896. [Google Scholar] [CrossRef]
- Ak, R.; Yilmaz, E.; Seyhan, A.U.; Doganay, F. Recurrence of COVID-19 Documented with RT-PCR. J. Coll. Physicians Surg. Pak. 2021, 30, S26–S28. [Google Scholar] [CrossRef]
- Aldossary, B.; Hassan, A.; Moussa, M.; Alsaif, H.S.; Alfaraj, D. Fulminant hepatic failure in a patient testing re-positive for SARS-CoV-2: A case report. Int. J. Emerg. Med. 2021, 14, 24. [Google Scholar] [CrossRef]
- Ali, A.M.; Ali, K.M.; Fatah, M.H.; Tawfeeq, H.M.; Rostam, H.M. SARS-CoV-2 Reinfection in Patients Negative for Immunoglobulin G Following Recovery from COVID-19. New Microbes New Infect. 2021, 43, 100926. [Google Scholar] [CrossRef] [PubMed]
- AlFehaidi, A.; Ahmad, S.A.; Hamed, E. SARS-CoV-2 re-infection: A case report from Qatar. J. Infect. 2021, 82, 414–451. [Google Scholar] [CrossRef]
- Alshukairi, A.N.; El-Kafrawy, S.A.; Dada, A.; Yasir, M.; Yamani, A.H.; Saeedi, M.F.; Aljohaney, A.; AlJohani, N.I.; Bahaudden, H.A.; Alam, I.; et al. Re-infection with different SARS-CoV-2 clade and prolonged viral shedding in a patient with hematopoietic stem cell transplantation: SARS-CoV-2 Re-infection with different clade. Int. J. Infect. Dis. 2021, 110, 267–271. [Google Scholar] [CrossRef] [PubMed]
- Amorim, M.R.; Souza, W.M.; Barros, A.C.G., Jr.; Toledo-Teixeira, D.A.; Dos-Santos, K.B.; Simeoni, C.L.; Parise, P.L.; Vieira, A.; Forato, J.; Claro, I.M.; et al. Respiratory Viral Shedding in Healthcare Workers Reinfected with SARS-CoV-2, Brazil, 2020. Emerg. Infect. Dis. 2021, 27, 1737–1740. [Google Scholar] [CrossRef]
- Arteaga-Livias, K.; Panduro-Correa, V.; Pinzas-Acosta, K.; Perez-Abad, L.; Pecho-Silva, S.; Espinoza-Sanchez, F.; Damaso-Mata, B.; Rodriguez-Morales, A.J. COVID-19 reinfection? A suspected case in a Peruvian patient. Travel Med. Infect. Dis. 2021, 39, 101947. [Google Scholar] [CrossRef]
- Atici, S.; Ek, O.F.; Yildiz, M.S.; Sikgenc, M.M.; Guzel, E.; Soysal, A. Symptomatic recurrence of SARS-CoV-2 infection in healthcare workers recovered from COVID-19. J. Infect. Dev. Ctries. 2021, 15, 69–72. [Google Scholar] [CrossRef]
- Awada, H.; Nassereldine, H.; Hajj Ali, A. Severe acute respiratory syndrome coronavirus 2 reinfection in a coronavirus disease 2019 recovered young adult: A case report. J. Med. Case Rep. 2021, 15, 382. [Google Scholar] [CrossRef]
- Bader, N.; Khattab, M.; Farah, F. Severe reinfection with severe acute respiratory syndrome coronavirus 2 in a nursing home resident: A case report. J. Med. Case Rep. 2021, 15, 392. [Google Scholar] [CrossRef]
- Baiswar, S.; Mittal, R.; Tiwary, T.; Jinnur, P. Re-Positive SARS-CoV-2 With Respiratory Failure and Cerebrovascular Accident: Is This a Reinfection? Cureus 2021, 13, e15825. [Google Scholar] [CrossRef]
- Bellesso, M.; Bruniera, F.R.; Trunkel, A.T.; Nicodemo, I.P. Second COVID-19 infection in a patient with multiple myeloma in Brazil—Reinfection or reactivation? Hematol. Transfus. Cell Ther. 2021, 43, 109–111. [Google Scholar] [CrossRef]
- Bongiovanni, M. COVID-19 re-infection in an healthcare worker. J. Med. Virol. 2020, 93, 4058–4059. [Google Scholar] [CrossRef]
- Bonifacio, L.P.; Pereira, A.P.S.; Araujo, D.; Balbao, V.; Fonseca, B.; Passos, A.D.C.; Bellissimo-Rodrigues, F. Are SARS-CoV-2 reinfection and Covid-19 recurrence possible? a case report from Brazil. Rev. Soc. Bras. Med. Trop. 2020, 53, e20200619. [Google Scholar] [CrossRef] [PubMed]
- Borgogna, C.; De Andrea, M.; Griffante, G.; Lai, A.; Bergna, A.; Galli, M.; Zehender, G.; Castello, L.; Ravanini, P.; Cattrini, C.; et al. SARS-CoV-2 reinfection in a cancer patient with a defective neutralizing humoral response. J. Med. Virol. 2021, 93, 6444–6446. [Google Scholar] [CrossRef]
- Brehm, T.T.; Pfefferle, S.; von Possel, R.; Kobbe, R.; Norz, D.; Schmiedel, S.; Grundhoff, A.; Olearo, F.; Emmerich, P.; Robitaille, A.; et al. SARS-CoV-2 Reinfection in a Healthcare Worker Despite the Presence of Detectable Neutralizing Antibodies. Viruses 2021, 13, 661. [Google Scholar] [CrossRef] [PubMed]
- Buddingh, E.P.; Vossen, A.; Lamb, H.J.; van der Palen, R.L.F.; Brinkman, D.M.C. Reinfection With Severe Acute Respiratory Syndrome Coronavirus 2 Without Recurrence of Multisystem Inflammatory Syndrome in Children. Pediatr. Infect. Dis. J. 2021. [Google Scholar] [CrossRef] [PubMed]
- Caralis, P. Case Reports of COVID 19 Recurrence. J. Prim. Care Community Health 2021, 12, 2150132720982752. [Google Scholar] [CrossRef]
- Cavanaugh, A.M.; Thoroughman, D.; Miranda, H.; Spicer, K. Suspected Recurrent SARS-CoV-2 Infections Among Residents of a Skilled Nursing Facility During a Second COVID-19 Outbreak—Kentucky, July-November 2020. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 273–277. [Google Scholar] [CrossRef] [PubMed]
- Colson, P.; Finaud, M.; Levy, N.; Lagier, J.C.; Raoult, D. Evidence of SARS-CoV-2 re-infection with a different genotype. J. Infect. 2021, 82, 84–123. [Google Scholar] [CrossRef] [PubMed]
- Das, P.; Satter, S.M.; Ross, A.G.; Abdullah, Z.; Nazneen, A.; Sultana, R.; Rimi, N.A.; Chowdhury, K.; Alam, R.; Parveen, S.; et al. A Case Series Describing the Recurrence of COVID-19 in Patients Who Recovered from Initial Illness in Bangladesh. Trop. Med. Infect. Dis. 2021, 6, 41. [Google Scholar] [CrossRef]
- Daw, M.A.; Daw, A.M.; Miftah, M.M.; El-Bouzedi, A.; Ahmed, M.O.; Libyan Study Group of COVID-19. Familial Clustering and Reinfection With 2019 Novel Coronavirus (COVID-19, SARS-CoV-2) in the Libyan Community. Disaster Med. Public Health Prep. 2021, 1–3. [Google Scholar] [CrossRef]
- de Brito, C.A.A.; Lima, P.M.A.; de Brito, M.C.M.; de Oliveira, D.B. Second Episode of COVID-19 in Health Professionals: Report of Two Cases. Int. Med. Case Rep. J. 2020, 13, 471–475. [Google Scholar] [CrossRef]
- Diaz, Y.; Ortiz, A.; Weeden, A.; Castillo, D.; Gonzalez, C.; Moreno, B.; Martinez-Montero, M.; Castillo, M.; Vasquez, G.; Saenz, L.; et al. SARS-CoV-2 reinfection with a virus harboring mutation in the Spike and the Nucleocapsid proteins in Panama. Int. J. Infect. Dis. 2021, 108, 588–591. [Google Scholar] [CrossRef]
- Dimeglio, C.; Herin, F.; Miedouge, M.; Martin-Blondel, G.; Soulat, J.M.; Izopet, J. Protection of healthcare workers against SARS-CoV-2 reinfection. Clin. Infect. Dis. 2021. [Google Scholar] [CrossRef]
- Dobano, C.; Ramirez-Morros, A.; Alonso, S.; Vidal-Alaball, J.; Ruiz-Olalla, G.; Vidal, M.; Rubio, R.; Cascant, E.; Parras, D.; Rodrigo Melero, N.; et al. Persistence and baseline determinants of seropositivity and reinfection rates in health care workers up to 12.5 months after COVID-19. BMC Med. 2021, 19, 155. [Google Scholar] [CrossRef]
- Duggan, N.M.; Ludy, S.M.; Shannon, B.C.; Reisner, A.T.; Wilcox, S.R. Is novel coronavirus 2019 reinfection possible? Interpreting dynamic SARSCoV-2 test results through a case report. Am. J. Emerg. Med. 2020, 39, 256.e1–256.e3. [Google Scholar] [CrossRef] [PubMed]
- Elzein, F.; Ibrahim, A.; Alshahrani, F.; Mahrous, M.; Murshid, E.; Aldhehyan, T.; Almutiri, G.; Altowairqi, M.; Ahmed, M.; Alsaeed, M.; et al. Reinfection, recurrence, or delayed presentation of COVID-19? Case series and review of the literature. J. Infect. Public Health 2021, 14, 474–477. [Google Scholar] [CrossRef] [PubMed]
- Fageeh, H.; Alshehri, A.; Fageeh, H.; Bizzoca, M.E.; Lo Muzio, L.; Quadri, M.F.A. Re-infection of SARS-CoV-2: A case in a young dental healthcare worker. J. Infect. Public Health 2021, 14, 685–688. [Google Scholar] [CrossRef] [PubMed]
- Fabianova, K.; Kyncl, J.; Vlckova, I.; Jirincova, H.; Kostalova, J.; Liptakova, M.; Orlikova, H.; Sebestova, H.; Limberkova, R.; Mackova, B.; et al. COVID-19 reinfections. Epidemiol. Mikrobiol. Imunol. 2021, 70, 62–67. [Google Scholar] [PubMed]
- Fernandes, A.C.; Figueiredo, R. SARS-CoV-2 reinfection: A case report from Portugal. Rev. Soc. Bras. Med. Trop. 2021, 54, e0002-2021. [Google Scholar] [CrossRef] [PubMed]
- Ferrante, L.; Livas, S.; Steinmetz, W.A.; Almeida, A.C.L.; Leao, J.; Vassao, R.C.; Tupinambas, U.; Fearnside, P.M.; Duczmal, L.H. The First Case of Immunity Loss and SARS-CoV-2 Reinfection by the Same Virus Lineage in Amazonia. J. Racial Ethn. Health Disparities 2021, 8, 821–823. [Google Scholar] [CrossRef]
- Fintelman-Rodrigues, N.; da Silva, A.P.D.; Dos Santos, M.C.; Saraiva, F.B.; Ferreira, M.A.; Gesto, J.; Rodrigues, D.A.S.; Vale, A.M.; de Azevedo, I.G.; Soares, V.C.; et al. Genetic Evidence and Host Immune Response in Persons Reinfected with SARS-CoV-2, Brazil. Emerg. Infect. Dis. 2021, 27, 1446–1453. [Google Scholar] [CrossRef]
- Fonseca, V.; de Jesus, R.; Adelino, T.; Reis, A.B.; de Souza, B.B.; Ribeiro, A.A.; Guimaraes, N.R.; Livorati, M.; Neto, D.F.L.; Kato, R.B.; et al. Genomic evidence of SARS-CoV-2 reinfection case with the emerging B.1.2 variant in Brazil. J. Infect. 2021, 5126. [Google Scholar] [CrossRef]
- Garduno-Orbe, B.; Sanchez-Rebolledo, J.M.; Cortes-Rafael, M.; Garcia-Jimenez, Y.; Perez-Ortiz, M.; Mendiola-Pastrana, I.R.; Lopez-Ortiz, E.; Lopez-Ortiz, G. SARS-CoV-2 Reinfection among Healthcare Workers in Mexico: Case Report and Literature Review. Medicina (Kaunas) 2021, 57, 442. [Google Scholar] [CrossRef]
- Garg, J.; Agarwal, J.; Das, A.; Sen, M. Recurrent COVID-19 infection in a health care worker: A case report. J. Med. Case Rep. 2021, 15, 363. [Google Scholar] [CrossRef]
- Garvey, M.I.; Casey, A.L.; Wilkinson, M.A.C.; Ratcliffe, L.; McMurray, C.; Stockton, J.; Holden, E.; Osman, H.; Loman, N.J. Details of SARS-CoV-2 reinfections at a major UK tertiary centre. J. Infect. 2021, 82, e29–e30. [Google Scholar] [CrossRef] [PubMed]
- Goel, N.; Jain, D.; Haddad, D.B. Coronavirus Disease-19 and Re-infection: Unknown of the Unknown. Saudi J. Kidney Dis. Transpl. 2021, 32, 261–264. [Google Scholar] [CrossRef] [PubMed]
- Gulati, K.; Prendecki, M.; Clarke, C.; Willicombe, M.; McAdoo, S. COVID-19 Reinfection in a Patient Receiving Immunosuppressive Treatment for Antineutrophil Cytoplasmic Antibody-Associated Vasculitis. Arthritis Rheumatol. 2021, 73, 1091–1092. [Google Scholar] [CrossRef] [PubMed]
- Gupta, V.; Bhoyar, R.C.; Jain, A.; Srivastava, S.; Upadhayay, R.; Imran, M.; Jolly, B.; Divakar, M.K.; Sharma, D.; Sehgal, P.; et al. Asymptomatic reinfection in two healthcare workers from India with genetically distinct SARS-CoV-2. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Habadi, M.I.; Balla Abdalla, T.H.; Hamza, N.; Al-Gedeei, A. COVID-19 Reinfection. Cureus 2021, 13, e12730. [Google Scholar] [CrossRef] [PubMed]
- Hanif, M.; Haider, M.A.; Ali, M.J.; Naz, S.; Sundas, F. Reinfection of COVID-19 in Pakistan: A First Case Report. Cureus 2020, 12, e11176. [Google Scholar] [CrossRef] [PubMed]
- Harrington, D.; Kele, B.; Pereira, S.; Couto-Parada, X.; Riddell, A.; Forbes, S.; Dobbie, H.; Cutino-Moguel, T. Confirmed Reinfection with SARS-CoV-2 Variant VOC-202012/01. Clin. Infect. Dis. 2021. [Google Scholar] [CrossRef] [PubMed]
- Hayes, B.; Stanley, J.; Peppers, B.P. COVID-19 Recurrence Without Seroconversion in a Patient With Mannose-Binding Lectin Deficiency. Allergy Rhinol. (Providence) 2021, 12, 21526567211024140. [Google Scholar] [CrossRef]
- Hunsinger, D.H.P.; Kutti Sridharan, D.G.; Rokkam, D.; Fantry, D.L.E. COVID-19 Reinfection in An Immunosuppressed Patient Without An Antibody Response. Am. J. Med. Sci. 2021, 362, 103. [Google Scholar] [CrossRef]
- Hussein, N.R.; Musa, D.H.; Saleem, Z.S.M.; Naqid, I.A.; Ibrahim, N. Possible COVID-19 reinfection case in Duhok City, Kurdistan: A case report. J. Fam. Med. Prim. Care 2021, 10, 2035–2037. [Google Scholar] [CrossRef]
- Hussein, N.R.; Rashad, B.H.; Almizori, L.A.; Yousif, S.S.; Sadeeq, A.T.; Abdulkareem, Y.R.; Mahmood, A.M.; Salih, Z.K. The Risk of SARS-CoV-2 Reinfection in Duhok city, Kurdistan Region of Iraq. Mediterr. J. Hematol. Infect. Dis. 2021, 13, e2021035. [Google Scholar] [CrossRef]
- Ibrahim, M.; Vegel, A.; Niu, A.; Panse, K.; Chen, R.; Safah, H.; Socola, F.; Luk, A.; Saba, N.S. Reinfection versus failure of viral clearance in a COVID-19 patient with hematologic malignancy. Leuk. Res. 2021, 101, 106514. [Google Scholar] [CrossRef]
- Inada, M.; Ishikane, M.; Terada, M.; Matsunaga, A.; Maeda, K.; Tsuchiya, K.; Miura, K.; Sairenji, Y.; Kinoshita, N.; Ujiie, M.; et al. Asymptomatic COVID-19 re-infection in a Japanese male by elevated half-maximal inhibitory concentration (IC50) of neutralizing antibodies. J. Infect. Chemother. 2021, 27, 1063–1067. [Google Scholar] [CrossRef] [PubMed]
- Jain, A.; Kaur, J.; Rai, A.K.; Pandey, A.K. Anosmia: A Clinical Indicator of COVID-19 Reinfection. Ear Nose Throat J. 2021, 100, 180S–181S. [Google Scholar] [CrossRef] [PubMed]
- Kapoor, R.; Nair, R.K.; Nayan, N.; Bhalla, S.; Singh, J. Reinfection or Reactivation of Coronavirus-19 in Patients with Hematologic Malignancies: Case Report Series. SN Compr. Clin. Med. 2021, 3, 670–674. [Google Scholar] [CrossRef] [PubMed]
- Krishna, V.N.; Ahmad, M.; Overton, E.T.; Jain, G. Recurrent COVID-19 in Hemodialysis: A Case Report of 2 Possible Reinfections. Kidney Med. 2021, 3, 447–450. [Google Scholar] [CrossRef]
- Kulkarni, O.; Narreddy, S.; Zaveri, L.; Kalal, I.G.; Tallapaka, K.B.; Sowpati, D.T. Evidence of SARS-CoV-2 reinfection without mutations in Spike protein. Clin. Infect. Dis. 2021, 73, e1239–e1241. [Google Scholar] [CrossRef]
- Larson, D.; Brodniak, S.L.; Voegtly, L.J.; Cer, R.Z.; Glang, L.A.; Malagon, F.J.; Long, K.A.; Potocki, R.; Smith, D.R.; Lanteri, C.; et al. A Case of Early Re-infection with SARS-CoV-2. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Lechien, J.R.; Chiesa-Estomba, C.M.; Vaira, L.A.; Saussez, S.; Hans, S. COVID-19 Reinfection and Second Episodes of Olfactory and Gustatory Dysfunctions: Report of First Cases. Ear Nose Throat J. 2020, 145561320970105. [Google Scholar] [CrossRef]
- Lee, J.S.; Kim, S.Y.; Kim, T.S.; Hong, K.H.; Ryoo, N.H.; Lee, J.; Park, J.H.; Cho, S.I.; Kim, M.J.; Kim, Y.G.; et al. Evidence of Severe Acute Respiratory Syndrome Coronavirus 2 Reinfection After Recovery from Mild Coronavirus Disease 2019. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Leung, S.; Hossain, N. Recurrence and Recovery of COVID-19 in an Older Adult Patient with Multiple Comorbidities: A Case Report. Gerontology 2021, 67, 445–448. [Google Scholar] [CrossRef]
- Luciani, M.; Bentivegna, E.; Spuntarelli, V.; Lamberti, P.A.; Cacioli, G.; Del Porto, F.; Sesti, G.; Martelletti, P.; De Biase, L. Recurrent COVID-19 pneumonia in the course of chemotherapy: Consequence of a weakened immune system? J. Med. Virol. 2021, 93, 1882–1884. [Google Scholar] [CrossRef]
- Mahajan, N.N.; Gajbhiye, R.K.; Lokhande, P.D.; Bahirat, S.; Modi, D.; Mathe, A.M.; Bharmal, R.; Rathi, S.; Mohite, S.C.; Tilve, A. Clinical Presentation of Cases with SARS-CoV-2 Reinfection/ Reactivation. J. Assoc. Physicians India 2021, 69, 16–18. [Google Scholar] [PubMed]
- Marquez, L.; Koy, T.; Spinler, J.K.; Luna, R.A.; Tocco, L.; Fasciano, L.; Dunn, J.; Campbell, J.R. Reinfection with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) B.1.1.7 variant in an immunocompromised adolescent. Infect. Control. Hosp. Epidemiol 2021, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Massanella, M.; Martin-Urda, A.; Mateu, L.; Marin, T.; Aldas, I.; Riveira-Munoz, E.; Kipelainen, A.; Jimenez-Moyano, E.; Rodriguez de la Concepcion, M.L.; Avila-Nieto, C.; et al. Critical Presentation of a Severe Acute Respiratory Syndrome Coronavirus 2 Reinfection: A Case Report. Open Forum Infect. Dis. 2021, 8, ofab329. [Google Scholar] [CrossRef] [PubMed]
- Mohseni, M.; Albus, M.; Kaminski, A.; Harrison, M.F. A Case of COVID-19 Re-Infection in a Liver Transplant Patient. Cureus 2021, 13, e14916. [Google Scholar] [CrossRef] [PubMed]
- Mulder, M.; van der Vegt, D.; Oude Munnink, B.B.; GeurtsvanKessel, C.H.; van de Bovenkamp, J.; Sikkema, R.S.; Jacobs, E.M.G.; Koopmans, M.P.G.; Wegdam-Blans, M.C.A. Reinfection of SARS-CoV-2 in an immunocompromised patient: A case report. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Munoz Mendoza, J.; Alcaide, M.L. COVID-19 in a patient with end-stage renal disease on chronic in-center hemodialysis after evidence of SARS-CoV-2 IgG antibodies. Reinfection or inaccuracy of antibody testing. IDCases 2020, 22, e00943. [Google Scholar] [CrossRef]
- Nachmias, V.; Fusman, R.; Mann, S.; Koren, G. The first case of documented Covid-19 reinfection in Israel. IDCases 2020, 22, e00970. [Google Scholar] [CrossRef]
- Naveca, F.; da Costa, C.; Nascimento, V.; Souza, V.; Corado, A.; Nascimento, F.; Costa, A.; Duarte, D.; Silva, G.; Mejía, M.; et al. Three SARS-CoV-2 reinfection cases by the new Variant of Concern (VOC) P.1/501Y.V3. Res. Sq. 2021. [Google Scholar] [CrossRef]
- Nazir, N.; Ahirwar, A.; Jain, S. Reinfection in a healthcare worker with COVID-19 in a hospital in North India. Anaesth. Pain Intensive Care 2020, 24, 572–573. [Google Scholar] [CrossRef]
- Nicholson, E.G.; Avadhanula, V.; Fragoso, S.; Stroh, R.; Ye, X.; Bond, N.; Santarcangelo, P.; Stroh, J.; Piedra, P.A. SARS-CoV-2 re-infection versus prolonged shedding: A case series. Influenza Other Respir Viruses 2021. [Google Scholar] [CrossRef]
- Nonaka, C.K.V.; Franco, M.M.; Graf, T.; de Lorenzo Barcia, C.A.; de Avila Mendonca, R.N.; de Sousa, K.A.F.; Neiva, L.M.C.; Fosenca, V.; Mendes, A.V.A.; de Aguiar, R.S.; et al. Genomic Evidence of SARS-CoV-2 Reinfection Involving E484K Spike Mutation, Brazil. Emerg. Infect. Dis. 2021, 27, 1522–1524. [Google Scholar] [CrossRef]
- Novoa, W.; Miller, H.; Mattar, S.; Faccini-Martinez, A.A.; Rivero, R.; Serrano-Coll, H. A first probable case of SARS-CoV-2 reinfection in Colombia. Ann. Clin. Microbiol. Antimicrob. 2021, 20, 7. [Google Scholar] [CrossRef]
- Ozaras, R.; Ozdogru, I.; Yilmaz, A.A. Coronavirus disease 2019 re-infection: First report from Turkey. New Microbes New Infect. 2020, 38, 100774. [Google Scholar] [CrossRef] [PubMed]
- Pow, T.; Allen, S.; Brailovsky, Y.; Darki, A. Acute submassive pulmonary embolism after SARS-CoV-2 infection: A case report of reinfection or prolonged hypercoagulable state. Eur. Heart J. Case Rep. 2021, 5, ytab103. [Google Scholar] [CrossRef] [PubMed]
- Quiroga, B.; Fernandez Ramos, A.; Delgado Arroyo, A. COVID-19 reinfection in a kidney transplant recipient, time for rethinking? Nefrologia 2021. [Google Scholar] [CrossRef] [PubMed]
- Ramirez, J.D.; Munoz, M.; Ballesteros, N.; Patino, L.H.; Castaneda, S.; Rincon, C.A.; Mendez, C.; Oliveros, C.; Perez, J.; Marquez, E.K.; et al. Phylogenomic Evidence of Reinfection and Persistence of SARS-CoV-2: First Report from Colombia. Vaccines 2021, 9, 282. [Google Scholar] [CrossRef] [PubMed]
- Rani, P.R.; Imran, M.; Lakshmi, J.V.; Jolly, B.; Jain, A.; Surekha, A.; Senthivel, V.; Chandrasekhar, P.; Divakar, M.K.; Srinivasulu, D.; et al. Symptomatic reinfection of SARS-CoV-2 with spike protein variant N440K associated with immune escape. J. Med. Virol. 2021, 93, 4163–4165. [Google Scholar] [CrossRef] [PubMed]
- Resende, P.C.; Bezerra, J.F.; Teixeira Vasconcelos, R.H.; Arantes, I.; Appolinario, L.; Mendonca, A.C.; Paixao, A.C.; Duarte, A.C.; Silva, T.; Rocha, A.S.; et al. Severe Acute Respiratory Syndrome Coronavirus 2 P.2 Lineage Associated with Reinfection Case, Brazil, June-October 2020. Emerg. Infect. Dis. 2021, 27, 1789–1794. [Google Scholar] [CrossRef]
- Rodriguez-Espinosa, D.; Broseta Monzo, J.J.; Casals, Q.; Pineiro, G.J.; Rodas, L.; Vera, M.; Maduell, F. Fatal SARS-CoV-2 reinfection in an immunosuppressed patient on hemodialysis. J. Nephrol. 2021, 34, 1041–1043. [Google Scholar] [CrossRef]
- Romano, C.M.; Felix, A.C.; Paula, A.V.; Jesus, J.G.; Andrade, P.S.; Candido, D.; Oliveira, F.M.; Ribeiro, A.C.; Silva, F.C.D.; Inemami, M.; et al. SARS-CoV-2 reinfection caused by the P.1 lineage in Araraquara city, Sao Paulo State, Brazil. Rev. Inst. Med. Trop. Sao Paulo 2021, 63, e36. [Google Scholar] [CrossRef] [PubMed]
- Salcin, S.; Fontem, F. Recurrent SARS-CoV-2 infection resulting in acute respiratory distress syndrome and development of pulmonary hypertension: A case report. Respir. Med. Case Rep. 2021, 33, 101314. [Google Scholar] [CrossRef] [PubMed]
- Salehi-Vaziri, M.; Omrani, M.D.; Pouriayevali, M.H.; Fotouhi, F.; Banifazl, M.; Farahmand, B.; Sadat Larijani, M.; Ahmadi, Z.; Fereydouni, Z.; Tavakoli, M.; et al. SARS-CoV-2 presented moderately during two episodes of the infection with lack of antibody responses. Virus Res. 2021, 299, 198421. [Google Scholar] [CrossRef] [PubMed]
- Salehi-Vaziri, M.; Jalali, T.; Farahmand, B.; Fotouhi, F.; Banifazl, M.; Pouriayevali, M.H.; Sadat Larijani, M.; Afzali, N.; Ramezani, A. Clinical characteristics of SARS-CoV-2 by re-infection vs. reactivation: A case series from Iran. Eur J. Clin. Microbiol. Infect. Dis. 2021, 40, 1713–1719. [Google Scholar] [CrossRef]
- Salzer, H.J.F. Emerging COVID-19 reinfection four months after primary SARS-CoV-2 infection. Wien. Med. Wochenschr. 2021. [Google Scholar] [CrossRef]
- Sanyang, B.; Kanteh, A.; Usuf, E.; Nadjm, B.; Jarju, S.; Bah, A.; Bojang, A.; Grey-Johnson, M.; Jones, J.C.; Gai, A.; et al. COVID-19 reinfections in The Gambia by phylogenetically distinct SARS-CoV-2 variants-first two confirmed events in west Africa. Lancet Glob. Health 2021, 9, e905–e907. [Google Scholar] [CrossRef]
- Scarpati, G.; Piazza, O.; Pagliano, P.; Rizzo, F. COVID-19: A confirmed case of reinfection in a nurse. BMJ Case Rep. 2021, 14, e244507. [Google Scholar] [CrossRef]
- Selhorst, P.; Van Ierssel, S.; Michiels, J.; Marien, J.; Bartholomeeusen, K.; Dirinck, E.; Vandamme, S.; Jansens, H.; Arien, K.K. Symptomatic SARS-CoV-2 reinfection of a health care worker in a Belgian nosocomial outbreak despite primary neutralizing antibody response. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Selvaraj, V.; Herman, K.; Dapaah-Afriyie, K. Severe, Symptomatic Reinfection in a Patient with COVID-19. R I Med. J. 2020, 103, 24–26. [Google Scholar]
- Sen, M.K.; Gupta, N.; Yadav, S.R.; Kumar, R.; Singh, B.; Ish, P. Contentious Issue in Recurrent COVID-19 Infection: Reactivation or Reinfection. Turk. Thorac. J. 2020, 21, 463–466. [Google Scholar] [CrossRef]
- Sevillano, G.; Ortega-Paredes, D.; Loaiza, K.; Zurita-Salinas, C.; Zurita, J. Evidence of SARS-CoV-2 reinfection within the same clade in Ecuador: A case study. Int. J. Infect. Dis. 2021, 108, 53–56. [Google Scholar] [CrossRef]
- Shastri, J.; Parikh, S.; Agrawal, S.; Chatterjee, N.; Pathak, M.; Chaudhary, S.; Sharma, C.; Kanakan, A.; Vivekanand, A.; Srinivasa Vasudevan, J.; et al. Clinical, Serological, Whole Genome Sequence Analyses to Confirm SARS-CoV-2 Reinfection in Patients From Mumbai, India. Front. Med. (Lausanne) 2021, 8, 631769. [Google Scholar] [CrossRef]
- Shoar, S.; Khavandi, S.; Tabibzadeh, E.; Khavandi, S.; Naderan, M.; Shoar, N. Recurrent coronavirus diseases 19 (COVID-19): A different presentation from the first episode. Clin. Case Rep. 2021, 9, 2149–2152. [Google Scholar] [CrossRef]
- Sicsic, I., Jr.; Chacon, A.R.; Zaw, M.; Ascher, K.; Abreu, A.; Chediak, A. A case of SARS-CoV-2 reinfection in a patient with obstructive sleep apnea managed with telemedicine. BMJ Case Rep. 2021, 14, e240496. [Google Scholar] [CrossRef]
- Siqueira, J.D.; Goes, L.R.; Alves, B.M.; da Silva, A.C.P.; de Carvalho, P.S.; Cicala, C.; Arthos, J.; Viola, J.P.B.; Soares, M.A. Distinguishing SARS-CoV-2 bonafide re-infection from pre-existing minor variant reactivation. Infect. Genet. Evol. 2021, 90, 104772. [Google Scholar] [CrossRef]
- Silva, M.S.D.; Demoliner, M.; Hansen, A.W.; Gularte, J.S.; Silveira, F.; Heldt, F.H.; Filippi, M.; Pereira, V.; Silva, F.P.D.; Mallmann, L.; et al. Early detection of SARS-CoV-2 P.1 variant in Southern Brazil and reinfection of the same patient by P.2. Rev. Inst. Med. Trop. Sao Paulo 2021, 63, e58. [Google Scholar] [CrossRef]
- Staub, T.; Arendt, V.; Lasso de la Vega, E.C.; Braquet, P.; Michaux, C.; Kohnen, M.; Tsobo, C.; Abdelrahman, T.; Wienecke-Baldacchino, A.; Francois, J.H. Case series of four re-infections with a SARS-CoV-2 B.1.351 variant, Luxembourg, February 2021. Euro Surveill 2021, 26, 2100423. [Google Scholar] [CrossRef] [PubMed]
- Takeda, C.F.V.; de Almeida, M.M.; Gomes, R.G.D.; Souza, T.C.; Mota, M.A.D.; Cavalcanti, L.P.D.; Colares, J.K.B. Case Report: Recurrent Clinical Symptoms of COVID-19 in Healthcare Professionals: A Series of Cases from Brazil. Am. J. Trop. Med. Hyg. 2020, 103, 1993–1996. [Google Scholar] [CrossRef] [PubMed]
- Tang, C.Y.; Wang, Y.; McElroy, J.A.; Li, T.; Hammer, R.; Ritter, D.; Lidl, G.M.; Webby, R.; Hang, J.; Wan, X.F. Reinfection with two genetically distinct SARS-CoV-2 viruses within 19 days. J. Med. Virol. 2021, 93, 5700–5703. [Google Scholar] [CrossRef] [PubMed]
- Tuan, J.; Spichler-Moffarah, A.; Ogbuagu, O. A new positive SARS-CoV-2 test months after severe COVID-19 illness: Reinfection or intermittent viral shedding? BMJ Case Rep. 2021, 14, e240531. [Google Scholar] [CrossRef] [PubMed]
- Teka, I.A.; BenHasan, M.H.; Alkershini, A.A.; Alatresh, O.K.; Abulifa, T.A.; Lembagga, H.A.; Alhudiri, I.M.; Elzagheid, A. Reinfection with SARS-CoV-2: A case report from Libya. Travel Med. Infect. Dis. 2021, 41, 102040. [Google Scholar] [CrossRef]
- To, K.K.; Hung, I.F.; Chan, K.H.; Yuan, S.; To, W.K.; Tsang, D.N.; Cheng, V.C.; Chen, Z.; Kok, K.H.; Yuen, K.Y. Serum Antibody Profile of a Patient With Coronavirus Disease 2019 Reinfection. Clin. Infect. Dis. 2021, 72, e659–e662. [Google Scholar] [CrossRef] [PubMed]
- Chan, P.K.S.; Lui, G.; Hachim, A.; Ko, R.L.W.; Boon, S.S.; Li, T.; Kavian, N.; Luk, F.; Chen, Z.; Yau, E.M.; et al. Serologic Responses in Healthy Adult with SARS-CoV-2 Reinfection, Hong Kong, August 2020. Emerg. Infect. Dis. 2020, 26, 3076–3078. [Google Scholar] [CrossRef] [PubMed]
- Tomkins-Tinch, C.H.; Daly, J.S.; Gladden-Young, A.; Theodoropoulos, N.M.; Madaio, M.P.; Yu, N.; Vanguri, V.K.; Siddle, K.J.; Adams, G.; Krasilnikova, L.A.; et al. SARS-CoV-2 Reinfection in a Liver Transplant Recipient. Ann. Intern. Med. 2021, 174, 1178–1180. [Google Scholar] [CrossRef]
- Tomassini, S.; Kotecha, D.; Bird, P.W.; Folwell, A.; Biju, S.; Tang, J.W. Setting the criteria for SARS-CoV-2 reinfection—Six possible cases. J. Infect. 2021, 82, 282–327. [Google Scholar] [CrossRef] [PubMed]
- Torres, D.A.; Ribeiro, L.; Riello, A.; Horovitz, D.D.G.; Pinto, L.F.R.; Croda, J. Reinfection of COVID-19 after 3 months with a distinct and more aggressive clinical presentation: Case report. J. Med. Virol. 2020, 93, 1857–1859. [Google Scholar] [CrossRef] [PubMed]
- Ul-Haq, Z.; Khan, A.; Fazid, S.; Noor, F.; Yousafzai, Y.M.; Sherin, A. First documented reinfection of SARS-COV-2 in second wave from Pakistan. J. Ayub. Med. Coll. Abbottabad 2020, 32 (Suppl. 1), S704–S705. [Google Scholar]
- Vetter, P.; Cordey, S.; Schibler, M.; Vieux, L.; Despres, L.; Laubscher, F.; Andrey, D.O.; Martischang, R.; Harbarth, S.; Cuvelier, C.; et al. Clinical, virological and immunological features of a mild case of SARS-CoV-2 re-infection. Clin. Microbiol. Infect. 2021, 27, 791.e1–791.e4. [Google Scholar] [CrossRef]
- Vora, T.; Vora, P.; Vora, F.; Sharma, K.; Desai, H.D. Symptomatic reinfection with COVID-19: A first from Western India. J. Fam. Med. Prim. Care 2021, 10, 1496–1498. [Google Scholar] [CrossRef]
- West, J.; Everden, S.; Nikitas, N. A case of COVID-19 reinfection in the UK. Clin. Med. (Lond) 2021, 21, e52–e53. [Google Scholar] [CrossRef]
- Yeleti, R.; Guglin, M.; Saleem, K.; Adigopula, S.V.; Sinha, A.; Upadhyay, S.; Everett, J.E.; Ballut, K.; Uppuluri, S.; Rao, R.A. Fulminant myocarditis: COVID or not COVID? Reinfection or co-infection? Future Cardiol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Yu, A.L.F.; Liphaus, B.L.; Ferreira, P.M.; Tanamachi, A.T.; Masuda, E.T.; Trevisan, C.M.; Lucas, P.C.C.; Bugno, A.; Carvalhanas, T. SARS-CoV-2 reinfection: Report of two cases in Southeast Brazil. Rev. Inst. Med. Trop. Sao Paulo 2021, 63, e50. [Google Scholar] [CrossRef] [PubMed]
- Zare, F.; Teimouri, M.; Khosravi, A.; Rohani-Rasaf, M.; Chaman, R.; Hosseinzadeh, A.; Jamali Atergeleh, H.; Binesh, E.; Emamian, M.H. COVID-19 re-infection in Shahroud, Iran: A follow-up study. Epidemiol. Infect. 2021, 149, e159. [Google Scholar] [CrossRef] [PubMed]
- Zhang, K.; Yiu-Nam Lau, J.; Yang, L.; Ma, Z. SARS-CoV-2 reinfection in two patients who have recovered from COVID-19. Precis. Clin. Med. 2020, 3, 292–293. [Google Scholar] [CrossRef]
- Zucman, N.; Uhel, F.; Descamps, D.; Roux, D.; Ricard, J.D. Severe reinfection with South African SARS-CoV-2 variant 501Y.V2: A case report. Clin. Infect. Dis. 2021. [Google Scholar] [CrossRef]
- Tirado, S.M.; Yoon, K.J. Antibody-dependent enhancement of virus infection and disease. Viral Immunol. 2003, 16, 69–86. [Google Scholar] [CrossRef]
- Yahav, D.; Yelin, D.; Eckerle, I.; Eberhardt, C.S.; Wang, J.; Cao, B.; Kaiser, L. Definitions for coronavirus disease 2019 reinfection, relapse and PCR re-positivity. Clin. Microbiol. Infect. 2021, 27, 315–318. [Google Scholar] [CrossRef]
- Xiao, A.T.; Tong, Y.X.; Zhang, S. False negative of RT-PCR and prolonged nucleic acid conversion in COVID-19: Rather than recurrence. J. Med. Virol. 2020, 92, 1755–1756. [Google Scholar] [CrossRef] [Green Version]
- Wang, W.; Xu, Y.; Gao, R.; Lu, R.; Han, K.; Wu, G.; Tan, W. Detection of SARS-CoV-2 in Different Types of Clinical Specimens. JAMA 2020, 323, 1843–1844. [Google Scholar] [CrossRef] [Green Version]
- Chaturvedi, R.; Naidu, R.; Sheth, S.; Chakravarthy, K. Efficacy of Serology Testing in Predicting Reinfection in Patients With SARS-CoV-2. Disaster Med. Public Health Prep. 2020, 15, e29–e31. [Google Scholar] [CrossRef]
- Atkinson, B.; Petersen, E. SARS-CoV-2 shedding and infectivity. Lancet 2020, 395, 1339–1340. [Google Scholar] [CrossRef]
- Anonymous. COVID-19 reinfection: Are we ready for winter? EBioMedicine 2020, 62, 103173. [Google Scholar] [CrossRef] [PubMed]
- Gousseff, M.; Penot, P.; Gallay, L.; Batisse, D.; Benech, N.; Bouiller, K.; Collarino, R.; Conrad, A.; Slama, D.; Joseph, C.; et al. Clinical recurrences of COVID-19 symptoms after recovery: Viral relapse, reinfection or inflammatory rebound? J. Infect. 2020, 81, 816–846. [Google Scholar] [CrossRef] [PubMed]
- Turner, J.S.; Day, A.; Alsoussi, W.B.; Liu, Z.; O’Halloran, J.A.; Presti, R.M.; Patterson, B.K.; Whelan, S.P.J.; Ellebedy, A.H.; Mudd, P.A. SARS-CoV-2 Viral RNA Shedding for More Than 87 Days in an Individual With an Impaired CD8+ T Cell Response. Front. Immunol. 2020, 11, 618402. [Google Scholar] [CrossRef] [PubMed]
- Raveendran, A.V. COVID-19 re-infection: Diagnostic challenges and proposed diagnostic criteria. Diabetes Metab. Syndr. 2021, 15, 645–648. [Google Scholar] [CrossRef]
- Pilz, S.; Chakeri, A.; Ioannidis, J.P.; Richter, L.; Theiler-Schwetz, V.; Trummer, C.; Krause, R.; Allerberger, F. SARS-CoV-2 re-infection risk in Austria. Eur. J. Clin. Investig. 2021, 51, e13520. [Google Scholar] [CrossRef] [PubMed]
- Sui, J.; Li, W.; Roberts, A.; Matthews, L.J.; Murakami, A.; Vogel, L.; Wong, S.K.; Subbarao, K.; Farzan, M.; Marasco, W.A. Evaluation of human monoclonal antibody 80R for immunoprophylaxis of severe acute respiratory syndrome by an animal study, epitope mapping, and analysis of spike variants. J. Virol. 2005, 79, 5900–5906. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, J.; Yuan, Q.; Wang, H.; Liu, W.; Liao, X.; Su, Y.; Wang, X.; Yuan, J.; Li, T.; Li, J.; et al. Antibody Responses to SARS-CoV-2 in Patients With Novel Coronavirus Disease 2019. Clin. Infect. Dis. 2020, 71, 2027–2034. [Google Scholar] [CrossRef]
- Del Fante, C.; Franchini, M.; Baldanti, F.; Percivalle, E.; Glingani, C.; Marano, G.; Mengoli, C.; Mortellaro, C.; Viarengo, G.; Perotti, C.; et al. A retrospective study assessing the characteristics of COVID-19 convalescent plasma donors and donations. Transfusion 2020, 61, 830–838. [Google Scholar] [CrossRef] [PubMed]
- Long, Q.X.; Liu, B.Z.; Deng, H.J.; Wu, G.C.; Deng, K.; Chen, Y.K.; Liao, P.; Qiu, J.F.; Lin, Y.; Cai, X.F.; et al. Antibody responses to SARS-CoV-2 in patients with COVID-19. Nat. Med. 2020, 26, 845–848. [Google Scholar] [CrossRef]
- Cassaniti, I.; Novazzi, F.; Giardina, F.; Salinaro, F.; Sachs, M.; Perlini, S.; Bruno, R.; Mojoli, F.; Baldanti, F.; Members of the San Matteo Pavia, C.-T.F. Performance of VivaDiag COVID-19 IgM/IgG Rapid Test is inadequate for diagnosis of COVID-19 in acute patients referring to emergency room department. J. Med. Virol 2020, 92, 1724–1727. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bichara, C.; Amoras, E.; Vaz, G.; Bichara, C.; Amaral, I.; Vallinoto, A. Persistence of Anti-SARS-CoV-2 IgM Antibody up to 8 Months Post-COVID-19. Case Rep. Clin. Med. 2021, 10, 227–231. [Google Scholar] [CrossRef]
- Sethuraman, N.; Jeremiah, S.S.; Ryo, A. Interpreting Diagnostic Tests for SARS-CoV-2. JAMA 2020, 323, 2249–2251. [Google Scholar] [CrossRef]
- Channappanavar, R.; Fett, C.; Zhao, J.; Meyerholz, D.K.; Perlman, S. Virus-specific memory CD8 T cells provide substantial protection from lethal severe acute respiratory syndrome coronavirus infection. J. Virol. 2014, 88, 11034–11044. [Google Scholar] [CrossRef] [Green Version]
- Sherina, N.; Piralla, A.; Du, L.; Wan, H.; Kumagai-Braesh, M.; Andréll, J.; Braesch-Andersen, S.; Cassaniti, I.; Percivalle, E.; Sarasini, A.; et al. Persistence of SARS-CoV-2 specific B- and T-cell responses in convalescent COVID-19 patients 6-8 months after the infection. BioRxiv 2020. [Google Scholar] [CrossRef]
- Enjuanes, L.; Zuniga, S.; Castano-Rodriguez, C.; Gutierrez-Alvarez, J.; Canton, J.; Sola, I. Molecular Basis of Coronavirus Virulence and Vaccine Development. Adv. Virus Res. 2016, 96, 245–286. [Google Scholar] [CrossRef]
- Figueiredo-Campos, P.; Blankenhaus, B.; Mota, C.; Gomes, A.; Serrano, M.; Ariotti, S.; Costa, C.; Nunes-Cabaco, H.; Mendes, A.M.; Gaspar, P.; et al. Seroprevalence of anti-SARS-CoV-2 antibodies in COVID-19 patients and healthy volunteers up to 6 months post disease onset. Eur. J. Immunol. 2020, 50, 2025–2040. [Google Scholar] [CrossRef]
- Krishna, E.; Pathak, V.K.; Prasad, R.; Jose, H.; Kumar, M.M. COVID-19 reinfection: Linked Possibilities and future outlook. J. Fam. Med. Prim. Care 2020, 9, 5445–5449. [Google Scholar] [CrossRef]
- Khoshkam, Z.; Aftabi, Y.; Stenvinkel, P.; Paige Lawrence, B.; Rezaei, M.H.; Ichihara, G.; Fereidouni, S. Recovery scenario and immunity in COVID-19 disease: A new strategy to predict the potential of reinfection. J. Adv. Res. 2021, 31, 49–60. [Google Scholar] [CrossRef] [PubMed]
- Prevost, J.; Finzi, A. The great escape? SARS-CoV-2 variants evading neutralizing responses. Cell Host Microbe 2021, 29, 322–324. [Google Scholar] [CrossRef] [PubMed]
- Guallar, M.P.; Meirino, R.; Donat-Vargas, C.; Corral, O.; Jouve, N.; Soriano, V. Inoculum at the time of SARS-CoV-2 exposure and risk of disease severity. Int. J. Infect. Dis. 2020, 97, 290–292. [Google Scholar] [CrossRef] [PubMed]
- Arvin, A.M.; Fink, K.; Schmid, M.A.; Cathcart, A.; Spreafico, R.; Havenar-Daughton, C.; Lanzavecchia, A.; Corti, D.; Virgin, H.W. A perspective on potential antibody-dependent enhancement of SARS-CoV-2. Nature 2020, 584, 353–363. [Google Scholar] [CrossRef]
- Negro, F. Is antibody-dependent enhancement playing a role in COVID-19 pathogenesis? Swiss Med. Wkly. 2020, 150, w20249. [Google Scholar] [CrossRef] [PubMed]
- Peron, J.P.S.; Nakaya, H. Susceptibility of the Elderly to SARS-CoV-2 Infection: ACE-2 Overexpression, Shedding, and Antibody-dependent Enhancement (ADE). Clinics (Sao Paulo) 2020, 75, e1912. [Google Scholar] [CrossRef] [PubMed]
- Ulrich, H.; Pillat, M.M.; Tarnok, A. Dengue Fever, COVID-19 (SARS-CoV-2), and Antibody-Dependent Enhancement (ADE): A Perspective. Cytom. A 2020, 97, 662–667. [Google Scholar] [CrossRef] [PubMed]
- Wan, Y.; Shang, J.; Sun, S.; Tai, W.; Chen, J.; Geng, Q.; He, L.; Chen, Y.; Wu, J.; Shi, Z.; et al. Molecular Mechanism for Antibody-Dependent Enhancement of Coronavirus Entry. J. Virol. 2020, 94, e02015-19. [Google Scholar] [CrossRef] [Green Version]
- Wen, J.; Cheng, Y.; Ling, R.; Dai, Y.; Huang, B.; Huang, W.; Zhang, S.; Jiang, Y. Antibody-dependent enhancement of coronavirus. Int. J. Infect. Dis. 2020, 100, 483–489. [Google Scholar] [CrossRef]
- Yager, E.J. Antibody-dependent enhancement and COVID-19: Moving toward acquittal. Clin. Immunol. 2020, 217, 108496. [Google Scholar] [CrossRef]
- Bournazos, S.; Gupta, A.; Ravetch, J.V. The role of IgG Fc receptors in antibody-dependent enhancement. Nat. Rev. Immunol. 2020, 20, 633–643. [Google Scholar] [CrossRef]
- Eroshenko, N.; Gill, T.; Keaveney, M.K.; Church, G.M.; Trevejo, J.M.; Rajaniemi, H. Implications of antibody-dependent enhancement of infection for SARS-CoV-2 countermeasures. Nat. Biotechnol. 2020, 38, 789–791. [Google Scholar] [CrossRef]
- Fleming, A.B.; Raabe, V. Current studies of convalescent plasma therapy for COVID-19 may underestimate risk of antibody-dependent enhancement. J. Clin. Virol. 2020, 127, 104388. [Google Scholar] [CrossRef]
- Kumar, R.; Gupta, N.; Kodan, P.; Mittal, A.; Soneja, M.; Wig, N. Is there antibody-dependent enhancement in SARS Coronavirus 2? J. Fam. Med. Prim. Care 2020, 9, 2589–2590. [Google Scholar] [CrossRef]
- Nechipurenko, Y.D.; Anashkina, A.A.; Matveeva, O.V. Change of Antigenic Determinants of SARS-CoV-2 Virus S-Protein as a Possible Cause of Antibody-Dependent Enhancement of Virus Infection and Cytokine Storm. Biophysics (Oxford) 2020, 65, 703–709. [Google Scholar] [CrossRef] [PubMed]
- Yip, M.S.; Leung, N.H.; Cheung, C.Y.; Li, P.H.; Lee, H.H.; Daeron, M.; Peiris, J.S.; Bruzzone, R.; Jaume, M. Antibody-dependent infection of human macrophages by severe acute respiratory syndrome coronavirus. Virol. J. 2014, 11, 82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, W.S.; Wheatley, A.K.; Kent, S.J.; DeKosky, B.J. Antibody-dependent enhancement and SARS-CoV-2 vaccines and therapies. Nat. Microbiol. 2020, 5, 1185–1191. [Google Scholar] [CrossRef] [PubMed]
- Kabir, K.M.A.; Tanimoto, J. Cost-efficiency analysis of voluntary vaccination against n-serovar diseases using antibody-dependent enhancement: A game approach. J. Theor. Biol. 2020, 503, 110379. [Google Scholar] [CrossRef]
- Kadkhoda, K. Severe acute respiratory syndrome coronavirus 2, original antigenic sin, and antibody-dependent enhancement: Ménage à trois. Curr. Opin. Rheumatol. 2020, 32, 458–461. [Google Scholar] [CrossRef]
- Karthik, K.; Senthilkumar, T.M.A.; Udhayavel, S.; Raj, G.D. Role of antibody-dependent enhancement (ADE) in the virulence of SARS-CoV-2 and its mitigation strategies for the development of vaccines and immunotherapies to counter COVID-19. Hum. Vaccines Immunother. 2020, 16, 3055–3060. [Google Scholar] [CrossRef]
- Cohen, J.I.; Burbelo, P.D. Reinfection with SARS-CoV-2: Implications for Vaccines. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Gudbjartsson, D.F.; Norddahl, G.L.; Melsted, P.; Gunnarsdottir, K.; Holm, H.; Eythorsson, E.; Arnthorsson, A.O.; Helgason, D.; Bjarnadottir, K.; Ingvarsson, R.F.; et al. Humoral Immune Response to SARS-CoV-2 in Iceland. N. Engl. J. Med. 2020, 383, 1724–1734. [Google Scholar] [CrossRef] [PubMed]
- Iyer, A.S.; Jones, F.K.; Nodoushani, A.; Kelly, M.; Becker, M.; Slater, D.; Mills, R.; Teng, E.; Kamruzzaman, M.; Garcia-Beltran, W.F.; et al. Persistence and decay of human antibody responses to the receptor binding domain of SARS-CoV-2 spike protein in COVID-19 patients. Sci. Immunol. 2020, 5, eabe0367. [Google Scholar] [CrossRef]
- Weisblum, Y.; Schmidt, F.; Zhang, F.; DaSilva, J.; Poston, D.; Lorenzi, J.C.; Muecksch, F.; Rutkowska, M.; Hoffmann, H.H.; Michailidis, E.; et al. Escape from neutralizing antibodies by SARS-CoV-2 spike protein variants. Elife 2020, 9, e61312. [Google Scholar] [CrossRef]
- Choudhary, M.C.; Crain, C.R.; Qiu, X.; Hanage, W.; Li, J.Z. SARS-CoV-2 Sequence Characteristics of COVID-19 Persistence and Reinfection. Clin. Infect. Dis. 2021. [Google Scholar] [CrossRef]
- Ulhaq, Z.S.; Soraya, G.V.; Indriana, K. Breakthrough COVID-19 case after full-dose administration of CoronaVac vaccine. Indian J. Med. Microbiol. 2021. [Google Scholar] [CrossRef]
- Hacisuleyman, E.; Hale, C.; Saito, Y.; Blachere, N.E.; Bergh, M.; Conlon, E.G.; Schaefer-Babajew, D.J.; DaSilva, J.; Muecksch, F.; Gaebler, C.; et al. Vaccine Breakthrough Infections with SARS-CoV-2 Variants. N. Engl. J. Med. 2021, 384, 2212–2218. [Google Scholar] [CrossRef] [PubMed]
- Dyer, O. Covid-19: Chinese vaccines may need changes to improve efficacy, admits official. BMJ 2021, 373, n969. [Google Scholar] [CrossRef]
- Angel, Y.; Spitzer, A.; Henig, O.; Saiag, E.; Sprecher, E.; Padova, H.; Ben-Ami, R. Association Between Vaccination With BNT162b2 and Incidence of Symptomatic and Asymptomatic SARS-CoV-2 Infections Among Health Care Workers. JAMA 2021, 325, 2457–2465. [Google Scholar] [CrossRef] [PubMed]
- Osterholm, M.T.; Kelley, N.S.; Sommer, A.; Belongia, E.A. Efficacy and effectiveness of influenza vaccines: A systematic review and meta-analysis. Lancet Infect. Dis. 2012, 12, 36–44. [Google Scholar] [CrossRef]
- Roy, S. COVID-19 Reinfection: Myth or Truth? SN Compr. Clin. Med. 2020, 2, 710–713. [Google Scholar] [CrossRef]
- Cavanaugh, A.M.; Spicer, K.B.; Thoroughman, D.; Glick, C.; Winter, K. Reduced Risk of Reinfection with SARS-CoV-2 After COVID-19 Vaccination—Kentucky, May-June 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1081–1083. [Google Scholar] [CrossRef] [PubMed]
- Al-Tawfiq, J.A.; Rabaan, A.A.; Al-Omari, A.; Al Mutair, A.; Al-Qahtani, M.; Tirupathi, R. Learning from SARS and MERS: COVID-19 reinfection where do we stand? Travel Med. Infect. Dis. 2021, 41, 102024. [Google Scholar] [CrossRef]
- Bizzoca, M.E.; Campisi, G.; Lo Muzio, L. An innovative risk-scoring system of dental procedures and safety protocols in the COVID-19 era. BMC Oral Health 2020, 20, 301. [Google Scholar] [CrossRef]
- Bizzoca, M.E.; Campisi, G.; Lo Muzio, L. Covid-19 Pandemic: What Changes for Dentists and Oral Medicine Experts? A Narrative Review and Novel Approaches to Infection Containment. Int. J. Environ. Res. Public Health 2020, 17, 3793. [Google Scholar] [CrossRef]
- Campisi, G.; Bazzano, M.; Mauceri, R.; Panzarella, V.; Di Fede, O.; Bizzoca, M.E.; Lo Muzio, L. The patient-doctor relationship: New insights in light of the current Ministerial recommendations regarding Phase 2 of the COVID-19 pandemic. Minerva Stomatol. 2020, 69, 251–255. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Investigative Criteria | Laboratory Evidence |
|---|---|
| Best evidence Differing clades as defined in Nextstrain and GISAID of SARS-CoV-2 between the first and second infection, ideally coupled with other evidence of actual infection (e.g., high viral titers in each sample or positive for subgenomic mRNA, and culture) |
with a symptomatic second episode and no obvious alternate etiology for COVID-19-like symptoms or close contact with a person known to have laboratory-confirmed COVID-19 | Moderate evidence >2 nucleotide differences per month * in consensus between sequences that meet quality metrics above, ideally coupled with other evidence of actual infection (e.g., high viral titers in each sample or positive for subgenomic mRNA, and culture) |
| Poor evidence but possible ≤2 nucleotide differences per month * in consensus between sequences that meet quality metrics above or >2 nucleotide differences per month * in consensus between sequences that do not meet quality metrics above, ideally coupled with other evidence of actual infection (e.g., high viral titers in each sample or positive for subgenomic mRNA, and culture) |
| Authors | Year | Patient Country | Patient | Interval Time between 1 Infection and Reinfection | Viral Genome Sequence | COVID-19 | Symptoms | Antibody after First Infection or Reinfection |
|---|---|---|---|---|---|---|---|---|
| 2021 | Qatar | 25–29-year-old man | 46 | 9 SNVs compared to initial infection strain, including D614G | Mild | N/A | N/A |
| Mild | N/A | |||||||
| 2021 | Qatar | 40–44-year-old man | 71 | 11 SNVs compared to initial infection strain, including D614G | Mild | N/A | N/A |
| Mild | N/A | |||||||
| 2021 | Qatar | 45–49-year-old woman | 88 | 3 SNVs compared to initial infection strain, including D614G | Mild | N/A | ROCHE elecsys antiSARS-CoV-2 negative at time of reinfection |
| Mild | N/A | |||||||
| 2021 | Qatar | 25–29-year-old woman | 55 | 1 SNVs compared to initial infection strain, including D614G | Mild | N/A | N/A |
| Mild | N/A | |||||||
| 2021 | Brazil | 44-year-old healthcare man with systemic arterial hypertension, obesity | 53 | 20A | Mild | Dry cough, dyspnea, dysgeusia, diarrhea, asthenia, sneezing/runny nose | N/A |
| Clade B.1.1.28 | Worse | Dry cough, dyspnea, fever, myalgia, asthenia, arthralgia, headache, nausea/vomiting, sneezing/runny nose, severe respiratory symptoms and was admitted to ICU, dying after 20 days of symptoms | ||||||
| 2021 | Spain | 39-year-old healthcare man | 290 | N/A | Mild | Sore throat, fever, general malaise, nasal congestion, tachycardia, chest pain, loss of smell and taste | Rapid antibody test: positive |
| 201/501Y.V1.Britain variant B.1.17 | Milder | Sore throat, slight general malaise, nasal congestion, tiredness | Rapid antibody test: positive | |||||
| 2021 | Iran | 36-year-old healthcare man | 60 | N/A | Mild | Lethargy, fatigue, shortness of breath, headache, fever, chills | N/A |
| Milder | Eye infection, fever, fatigue, shortness of breath, muscle pain | |||||||
| 2021 | Pakistan | Healthcare worker man | 118 | N/A | Mild | Arthralgia, weakness, anosmia, ageusia | N/A |
| Milder | Fever, sore throat, dry cough | |||||||
| 2021 | Pakistan | Healthcare worker man | 86 | N/A | Mild | Fever, sore throat | N/A |
| Milder | Sinusitis | |||||||
| 2021 | Pakistan | 40-year-old male | 94 | N/A | Mild | Fever | N/A |
| Worse | Sore throat, cough, diarrhea | |||||||
| 2021 | Bahrain | 47-year-old woman without comorbidities | 60 | N/A | Mild | Mild respiratory tract symptoms | N/A |
| Worse | Abdominal pain, fulminant hepatic failure > death | |||||||
| 2020 | Iran | 20s year age range, male | 89 ** | N/A | Mild | Fever, myalgia | 6.7 IgG (s/ca) after recovery |
| Worse | Fever, myalgia, cough, loss of taste, loss of smell | |||||||
| 2020 | Iran | 30s year age range, female | 55 ** | N/A | Mild | Fever, myalgia | 10.3 IgG (s/ca) after recovery |
| Worse | Fever, loss of taste and smell, myalgia, cough | |||||||
| 2020 | Iran | 40s year age range, male | 55 ** | N/A | Mild | Fever, myalgia | 15.5 IgG (s/ca) after recovery |
| Mild | Fever, myalgia, cough | |||||||
| 2020 | Iran | 50s year age range, male | 46 ** | N/A | Mild | Fever, myalgia | 10.3 IgG (s/ca) after recovery |
| Worse | Fever, loss of taste and smell, myalgia, cough | |||||||
| 2020 | Iran | 50s year age range, female | 53 ** | N/A | Mild | Fever, loss of taste and smell | 5.35 IgG (s/ca) after recovery |
| Milder | Fever, myalgia, cough | |||||||
| 2020 | Iran | 40s year age range, male | 76 ** | N/A | Mild | Fever, myalgia | 7.22 IgG (s/ca) after recovery |
| Worse | Fever, loss of taste and smell, myalgia, cough | |||||||
| 2020 | Iran | 40s year age range, female | 45 ** | N/A | Mild | Fever, myalgia | 11.2 IgG (s/ca) after recovery |
| Worse | Fever, loss of taste and smell, myalgia, cough | |||||||
| 2020 | Iran | 40s year age range, male | 50 ** | N/A | Mild | Fever, loss of taste and smell, myalgia | 12.51 IgG (s/ca) after recovery |
| Mild | Fever, loss of taste and smell, myalgia, cough | |||||||
| 2020 | Iran | 40s year age range, male | 62 ** | N/A | Mild | Fever, cough | 7.11 IgG (s/ca) after recovery |
| Worse | Fever, loss of taste and smell, myalgia, cough | |||||||
| 2020 | Iran | 40s year age range, female | 49 ** | N/A | Mild | Fever | 8.37 IgG (s/ca) after recovery |
| Worse | Fever, loss of taste and smell, myalgia | |||||||
| 2020 | Iran | 40s year age range, male | 72 ** | N/A | Mild | Fever | 5.11 IgG (s/ca) after recovery |
| Worse | Fever, loss of taste and smell, myalgia, cough | |||||||
| 2020 | Iran | 30s year age range, male | 59 ** | N/A | Mild | Fever, loss of taste and smell, myalgia | 6.3 IgG (s/ca) after recovery |
| Mild | Fever, loss of taste and smell, myalgia, cough | |||||||
| 2020 | Iran | 50s year age range, male | 53 ** | N/A | Mild | Fever, myalgia | 9.3 IgG (s/ca) after recovery |
| Worse | Fever, loss of taste and smell, myalgia, cough | |||||||
| 2020 | Iran | 20s year age range, male | 49 ** | N/A | Mild | Fever, myalgia | 7.25 IgG (s/ca) after recovery |
| Worse | Fever, loss of taste and smell, myalgia, cough | |||||||
| 2020 | Iran | 40s year age range, female | 52 ** | N/A | Mild | Fever, myalgia | 6.21 IgG (s/ca) after recovery |
| Worse | Loss of taste and smell, myalgia | |||||||
| 2020 | Iran | 20s year age range, female | 54 ** | N/A | Mild | Fever | 11.9 IgG (s/ca) after recovery |
| Mild | Fever, cough | |||||||
| 2020 | Iran | 30s year age range, male | 138 ** | N/A | Moderate | Fever, loss of taste and smell, myalgia, cough | 2.08 IgG (s/ca) after recovery |
| Asymptomatic | Asymptomatic | |||||||
| 2020 | Qatar | 46-year-old woman with mild asthma | 80 | N/A | Mild | Sore throat | N/A |
| Moderate | Chest pain, fever, sore throat, body pain, cough, mild dyspnea | |||||||
| 2021 | Saudi Arabia | 51-year-old woman with autologous hematopoietic stem cell transplantation for follicular non-Hodgkin lymphoma | 160 | 19B | Mild | Fever, cough, malaise, and headache | Negative COVID-19 serology after 1st infection and reinfection |
| 20B | Mild | Fever and dyspnea | ||||||
| 2021 | Turkey | 34-year-old man with chronic glomerulonephritis | >150 | N/A | Mild | Asymptomatic | N/A |
| Worse | Cough, fever, bilateral infiltrates at computed chest tomography | |||||||
| 2021 | Brazil | 35-year-old healthcare worker woman | 55 | N/A | Mild | Fever, headache, chills, sneezing, coryza, myalgia | N/A |
| Mild | Headache, nasal congestion, odynophagia, ageusia, anosmia | |||||||
| 2021 | Brazil | 61-year-old healthcare worker woman with chronic bronchitis | 170 | N/A | Mild | Headache, cough, myalgia, odynophagia, coryza, diarrhea, ageusia | N/A |
| Mild | Cough, myalgia, odynophagia, anosmia, diarrhea | |||||||
| 2021 | Brazil | 40-year-old healthcare worker woman | 131 | N/A | Mild | Nasal congestion, coryza, cough, ageusia | N/A |
| Mild | Odynophagia, sneezing, coryza, diarrhea, ageusia, anosmia | |||||||
| 2021 | Brazil | 40-year-old healthcare worker woman | 148 | N/A | Mild | Fever, headache, myalgia, coryza, dry cough, vomiting, malaise | N/A |
| Mild | Odynophagia, dry cough, myalgia, malaise, coryza, headache | |||||||
| 2021 | Peru | 42-year-old healthcare worker woman | 107 | N/A | Mild with home management | Odynophagia, headache, malaise, rhinorrhea, ageusia, anosmia, cough | IgM and IgG+ |
| Worse with home management | Chest pain, productive cough, anosmia, pneumonia | |||||||
| 2021 | Turkey | 46-year-old healthcare worker man | 114 | N/A | Moderate | Fever, sore throat, headache, cough, weakness, nausea and diarrhea, bilateral ground glass opacities and peribronchial thickening predominating on the right lung | N/A |
| Mild | Sore throat, fever, headache, myalgia, weakness and nausea | |||||||
| 2021 | Turkey | 47-year-old healthcare worker woman | 128 | N/A | Mild | Myalgia, headache and abdominal pain started without fever and cough | N/A |
| Worse | Sore throat, headache and myalgia, fever, cough and mild respiratory symptoms, ground glass opacities and subpleural nodule on the left lung base consistent with COVID-19 on chest CT imagine | |||||||
| 2021 | Lebanon | 27-year-old man | 56 | N/A | Mild | Fever, chills, diffuse arthralgia, myalgia, headache, back pain | N/A |
| Milder | Fever, headache | |||||||
| 2021 | USA | 73-year-old man with obesity, chronic obstructive pulmonary disease, pancreatic insufficiency, type II diabetes mellitus | 60 | N/A | Mild | Shortness of breath | N/A |
| Worse | Dyspnea, fevers, confusion with worsening clinical situation and intubation | |||||||
| 2021 | USA | 28-year-old male with diabetes mellitus type 1, hypertension, and end-stage renal disease on hemodialysis with multiple past admissions for diabetic ketoacidosis and uncontrolled hypertension | 122 | N/A | Mild | Nausea and vomiting | N/A |
| Worse | Headaches and altered mental status, left-hand weakness. The patient became unresponsive and was intubated for airway protection > cerebrovascular accident | |||||||
| 2021 | Brazil | 76-year-old female with end-stage kidney disease related to lambda light chain multiple myeloma | 126 | N/A | Moderate | Hip pain, confusion, respiratory distress | N/A |
| Worse | Dyspnea, acute respiratory failure, hypoxemia > death | |||||||
| 2020 | Italy | 48-year-old nurse female | 90 | N/A | Mild | Dry cough, mild fever | LIASON ® SARS-CoV-2 S1/S2 IgG+ 30 Au/mL |
| Asymptomatic | Asymptomatic | IgG+ 102.9 Au/mL | ||||||
| 2020 | Brazil | 24-year-old white female without comorbidities | 76 | N/A | Mild with complete resolution at home within 10 days | Headache, malaise, adynamia, feverish sensation, sore throat, nasal congestion | N/A |
| Worse with home resolution in 12 days, headache and hyposmia for 63 days | Malaise, myalgia, severe headache, fatigue, weakness, feverish sensation, sore throat, anosmia, dysgeusia, diarrhea, coughing | IgG/IgM– at NAAT+IgG/IgM+ 28 days after NAAT+ | ||||||
| 2021 | Italy | 52-year-old man with transitional cell carcinoma of the renal pelvis | 110 | Clade 20B and Pangolin lineage B.1.1 | Mild | Cough, fever | |
| Clade 20A and Pangolin lineage B.1 | Milder | Fever | Very low levels of IgG anti-SARS-CoV-2 Spike protein, positive IgG anti-SARS-CoV-2 N protein | |||||
| 2021 | Germany | 27-year-old female nurse | 282 | HH-24.I (19A) | Mild | Fever, chills, dyspnea | IgG anti-SARS-CoV-2 Spike protein: 40 AU/mL in July 2020, 15 AU/mL in September 2020 |
| HH-24.II (20EU1) with differences in 21 positions, including 2 typical variations in spike proteins A222V and D614G | Milder | Dry cough, mild rhinorrhea | IgG anti-SARS-CoV-2 Spike protein: 97 AU/mL on 29 December | |||||
| 2021 | The Netherlands | 16-year-old girl | 390 | Classic | Moderate | High fever, mild conjunctivitis, malaise, chest pain, coughing, abdominal pain and diarrhea. She was diagnosed with myocarditis, shock and had high inflammatory parameters. | IgG SARS-CoV-2 was negative (Abbott SARS-CoV-2 IgG; Abbott Laboratories) |
| B.1.1.7 variant (UK variant), | Mild | Mild respiratory symptoms | ||||||
| 2021 | USA | 60 with diabetes | 72 | N/A | Mild | Acute renal failure | |
| Milder | Fatigue | |||||||
| 2021 | USA | 27 with psoriatic arthritis | 79 | N/A | Mild | Fever, flu-like | IgG+ |
| Milder | Fatigue, loss taste | |||||||
| 2021 | USA | 33 year-old woman with allergic rhinitis | 172 | N/A | Mild | Fever, cough, diarrhea | IgG+ |
| Milder | Fever headache | |||||||
| 2021 | USA | 71 with renal/liver transplant HIV, diabetes | 93 | N/A | Moderate | Fever, pneumonia, respiratory insufficiency | |
| Asymptomatic | Asymptomatic | |||||||
| 2021 | USA | 72 with pulmonary/cardiac sarcoidosis | 111 | N/A | Mild | Dyspnea, fatigue, headache | |
| Milder | Fatigue | |||||||
| 2021 | USA | M (80–89 years old) | 101 | N/A | Asymptomatic | asymptomatic | N/A |
| Mild | Lethargy, decreased appetite, dry cough for 14 days | |||||||
| 2021 | USA | F (80–89 years old) | 103 | N/A | Asymptomatic | asymptomatic | N/A |
| Worse | Congestion, respiratory failure and death | |||||||
| 2021 | USA | F (60–69 years old) | 109 | N/A | Mild | nausea | N/A |
| Mild | Cough, sore throat, loss of appetite, malaise, muscle aches for 17 days | |||||||
| 2021 | USA | F (70–79 years old) | 109 | N/A | Mild | Gastrointestinal symptoms for 17 days | N/A |
| Milder | Loss of appetite, malaise for 12 days | |||||||
| 2021 | USA | Female (90–99 years old) | 110 | N/A | Asymptomatic | asymptomatic | N/A |
| Mild | Cough, loss of appetite, malaise, muscle aches for 6 days | |||||||
| 2021 | France | 70-year-old man | 105 | Clade 20A | Moderate | Fever, cough | IgG+ on D26 |
| 20A.E2, 34 nucleotide differences | Asymptomatic, during a systematic screening | Asymptomatic | ||||||
| 2021 | Bangladesh | A 35–49-year-old man with hypertension | 98 | N/A | Mild | Fever, cough | |
| Milder | Fever, cough, cold | |||||||
| 2021 | Bangladesh | A 35–49-year-old researcher woman | 92 | N/A | Mild | Malaise | |
| Milder | Sore throat, fever, cough, headache | |||||||
| 2021 | Bangladesh | 35–49 hypertensive physician | 94 | N/A | Mild | Fever, headache, sore throat | |
| Mild | Fever, cold, low oxygen saturation | |||||||
| 2021 | Bangladesh | 35–49 man with asthma | 93 | N/A | Mild | Fever | |
| Mild | Fever, cough | |||||||
| 2021 | Bangladesh | 35–49-year-old health worker woman with hypertension, hypothyroidism | 131 | N/A | Mild | Fever, cough | |
| Worse | Chest pain, headache, sore throat, hospitalized | |||||||
| 2021 | Libya | 52-year-old healthy male | 72 | N/A | Mild | Cough, sore throat, fever, myalgias, headache | N/A |
| Worse | Fever, cough, shortness of breath, gastrointestinal symptoms | |||||||
| 2020 | Brazil | 40-year-old male doctor | 46 | N/A | Moderate | Fever, cough, sore throat, fatigue, myalgia, headache, diarrhea | IgG and IgM– 42 days after 1 infection |
| Moderate | Fever, cough, sore throat, fatigue, myalgia, headache, diarrhea, anosmia and dysgeusia | IgG and IgM– | ||||||
| 2021 | Panama | 36-year-old man without comorbidities | 181 | A.2.4 | Mild | Myalgia, chest pain, fever, cephalea, rhinorrhea, hyposmia, ageusia | |
| A.2.5 containing Spike mutations D614G and L452R | Milder | Cephalea, myalgia, rhinorrhea | ||||||
| 2021 | France | 25-year-old female healthcare worker | >90 | N/A | Asymptomatic | Asymptomatic | No neutralizing antibodies |
| Moderate | Fever, rhinorrhea, dyspnea, chest pain, dysgeusia, anosmia, asthenia, myalgia, eye pain, pharyngitis; not hospitalized | Yes, neutralizing antibodies | ||||||
| 2021 | France | 40-year-old female healthcare worker | >90 | N/A | Asymptomatic | Asymptomatic | No neutralizing antibodies |
| Asymptomatic | Asymptomatic | No neutralizing antibodies | ||||||
| 2021 | France | 46-year-old female healthcare worker | >90 | N/A | Moderate | Fever, rhinorrhea, cough, dyspnea, chest pain, intestinal disorders, dysgeusia, anosmia, asthenia, headache, myalgia, not hospitalized | Yes, neutralizing antibodies |
| Mild | Fever, cough, dyspnea, chest pain, headache, asthenia, myalgia, pharyngitis; not hospitalized | Yes, neutralizing antibodies | ||||||
| 2021 | France | 31-year-old male healthcare worker | >90 | N/A | Mild | Anosmia; not hospitalized | Yes, neutralizing antibodies |
| Asymptomatic | Asymptomatic | Yes, neutralizing antibodies | ||||||
| 2021 | France | 50-year-old female healthcare worker | >90 | N/A | Asymptomatic | Asymptomatic | Yes, neutralizing antibodies |
| Mild | Cough, headache; not hospitalized | Yes, neutralizing antibodies | ||||||
| 2021 | Spain | 29-year-old female healthcare worker | 212 | N/A | Mild | 60 days | Seronegative after 1st infection, seroconverted after re-infection |
| Mild | 70 days | |||||||
| 2021 | Spain | 41-year-old female healthcare worker | 154 | N/A | Mild | 61 days | Seronegative after 1st infection, seroconverted after re-infection |
| Milder | ||||||||
| 2021 | Spain | 58-year-old female healthcare worker | 58 | N/A | Mild | 3 days | Unknow after 1st infection, seropositive after reinfection |
| Mild | 3 days | |||||||
| 2021 | Spain | 44-year-old female healthcare worker | 211 | N/A | Mild | 11 days | Seropositive after 1st infection with antibody low-level |
| Asymptomatic | Asymptomatic | |||||||
| 2020 | USA | 82-year-old male with Parkinson, insulin-dependent diabetes, chronic kidney disease, hypertension | 48 | N/A | Severe with intubation | Fever, shortness of breath, hypoxia, pneumonia | N/A |
| Severe without intubation | Fever, hypoxia, hypotension, tachycardia, pneumonia | |||||||
| 2021 | Saudi Arabia | 51-year-old man without comorbidities | 58 | Asymptomatic | Asymptomatic | 7.04 SARS-CoV-2 IgG (Abbot) during second admission | |
| Worse | Fever, cough, generalized weakness, and shortness of breath, bilateral diffuse patchy airspace disease while a CT scan revealed bilateral patchy 4 central and peripheral ground glass opacities most likely related to COVID-19 | |||||||
| 2021 | Saudi Arabia | 55-year-old man with relapsed NHL | 31 | Mild | Mild | 0.01 SARS-CoV-2 IgG (Abbot) index negative during second admission | |
| Worse | High grade fever, dry cough, sore throat, tachycardia and (SPO2) 93% on room air | |||||||
| 2021 | Saudi Arabia | 60-year-old man with diabetes mellitus, hypertension, ischemic heart disease | 27 | Mild | Mild | N/A | |
| Milder | Cough, shortness of breath | |||||||
| 2021 | Saudi Arabia | 48-year-old woman with metastatic breast cancer | 85 | Moderate | Pneumonia | N/A | |
| Mild | Fever, shortness of breath | |||||||
| 2021 | Saudi Arabia | 24-year-old male dental student | 90 | N/A | Mild | Sore throat, cough, headache, nausea, diarrhea, loss of taste and smell, insomnia, loss of appetite, and fatigue, fear and anxiety, increased insomnia, and increased body ache | N/A |
| Mild | Coughing, body ache, loss of taste and smell, and diarrhea symptoms were slightly less severe, the patient was less anxious and slept well. Fever | |||||||
| 2021 | Czech Republic | 60-year-old man with diabetes | 177 | N/A | Mild | Mild—long term care facility | N/A |
| Moderate | Mild—hospitalized | |||||||
| 2021 | Czech Republic | 75-year-old man with diabetes, cardiovascular disease | 102 | N/A | Mild | Mild—long term care facility | N/A |
| Severe | Mild—hospitalized | |||||||
| 2021 | Czech Republic | 72-year-old man with malignity | 205 | N/A | Mild | Mild—home | N/A |
| Mild | Mild—home | |||||||
| 2021 | Czech Republic | 62-year-old woman with asthma | 137 | N/A | Mild | Mild—home | N/A |
| Mild | Mild—home | |||||||
| 2021 | Czech Republic | 57-year-old woman without comorbidities | 203 | N/A | Mild | Mild—home | N/A |
| Mild | Mild—home | |||||||
| 2021 | Czech Republic | 56-year-old woman without comorbidities | 216 | N/A | Mild | Mild—home | N/A |
| Mild | Mild—home | |||||||
| 2021 | Czech Republic | 55-year-old man without comorbidities | 212 | N/A | Mild | Mild—home | N/A |
| Mild | Mild—home | |||||||
| 2021 | Czech Republic | 53-year-old man without comorbidities | 214 | N/A | Mild | Mild—home | N/A |
| Mild | Mild—home | |||||||
| 2021 | Czech Republic | 50-year-old woman with malignity | 197 | N/A | Mild | Mild—home | N/A |
| Mild | Mild—home | |||||||
| 2021 | Czech Republic | 49-year-old woman without comorbidities | 195 | N/A | Mild | Mild—home | N/A |
| Mild | Mild—home | |||||||
| 2021 | Czech Republic | 49-year-old woman without comorbidities | 200 | N/A | Mild | Mild—home | N/A |
| Mild | Mild—home | |||||||
| 2021 | Czech Republic | 47-year-old man without comorbidities | 141 | N/A | Mild | Mild—home | N/A |
| Moderate | Mild—home | |||||||
| 2021 | Czech Republic | 47-year-old man without comorbidities | 206 | N/A | Mild | Mild—home | N/A |
| Mild | Mild—home | |||||||
| 2021 | Czech Republic | 46-year-old man without comorbidities | 154 | N/A | Mild | Mild—home | N/A |
| Mild | Mild—home | |||||||
| 2021 | Czech Republic | 46-year-old woman without comorbidities | 231 | N/A | Mild | Mild—home | N/A |
| Mild | Mild—home | |||||||
| 2021 | Czech Republic | 45-year-old woman without comorbidities | 101 | N/A | Mild | Mild—home | N/A |
| Mild | Mild—home | |||||||
| 2021 | Czech Republic | 45-year-old woman with diabetes, chronic pulmonary disease, allergy | 196 | N/A | Mild | Mild—home | N/A |
| Mild | Mild—home | |||||||
| 2021 | Czech Republic | 45-year-old woman with cardiovascular disease | 211 | N/A | Mild | Mild—home | N/A |
| Mild | Mild—home | |||||||
| 2021 | Czech Republic | 44-year-old woman with hypertension | 169 | N/A | Mild | Mild—home | N/A |
| Mild | Mild—home | |||||||
| 2021 | Czech Republic | 44-year-old man without comorbidities | 224 | N/A | Mild | Mild—home | N/A |
| Mild | Mild—home | |||||||
| 2021 | Czech Republic | 42-year-old woman without comorbidities | 206 | N/A | Mild | Mild—home | N/A |
| Mild | Mild—home | |||||||
| 2021 | Czech Republic | 39-year-old woman without comorbidities | 229 | N/A | Mild | Mild—home | N/A |
| Mild | Mild—home | |||||||
| 2021 | Czech Republic | 34-year-old man without comorbidities | 158 | N/A | Mild | Mild—home | N/A |
| Mild | Mild—home | |||||||
| 2021 | Czech Republic | 30-year-old woman without comorbidities | 219 | N/A | Mild | Mild—home | N/A |
| Mild | Mild—home | |||||||
| 2021 | Czech Republic | 29-year-old woman without comorbidities | 139 | N/A | Mild | Mild—home | N/A |
| Mild | Mild—home | |||||||
| 2021 | Czech Republic | 27-year-old woman without comorbidities | 172 | N/A | Mild | Mild—home | N/A |
| Mild | Mild—home | |||||||
| 2021 | Czech Republic | 27-year-old woman without comorbidities | 215 | N/A | Mild | Mild—home | N/A |
| Mild | Mild—home | |||||||
| 2021 | Czech Republic | 25-year-old man without comorbidities | 222 | N/A | Mild | Mild—home | N/A |
| Mild | Mild—home | |||||||
| 2021 | Portugal | 28-year-old man with asthma | 285 | N/A | Mild | Fever, chills, sneezing | N/A |
| Worse | Fever, tiredness, productive cough, frontal headache, dizziness, dark urine, dysuria | |||||||
| 2021 | Brazil | 24-year-old woman without comorbidities | 109 | N/A | Asymptomatic | Asymptomatic | No IgG antibodies after first infection |
| P1 variant | Worse | Headache, sore throat, odynophagia, nasal congestion, tiredness, fatigue, chest pain, lack of appetite, hypertension, tachycardia | ||||||
| 2021 | Brazil | 54-year-old man without comorbidities | 65 | N/A | Mild | Headache | IgM, IgA, IgG detected <1:4 |
| Clade 20B | Worse | Fever, dry cough, tiredness, body ache, anosmia, ageusia | IgM, IgA, IgG detected 1:128 | |||||
| 2021 | Brazil | 57-year-old woman with discoid lupus erythematous | 61 | Clade 19A | Mild | Mild diarrhea | IgM, IgA, IgG detected <1:4 |
| Clade 20B | Worse | Fever, diarrhea, headache, body ache, anosmia, ageusia | IgM, IgA, IgG detected 1:32 | |||||
| 2021 | Brazil | 34-year-old man without comorbidities | 64 | Clade 20B | Mild | Asymptomatic | IgM, IgA, IgG detected <1:4 |
| Clade 20B | Worse | Fever, nausea, tiredness, headache, body ache | IgM, IgA, IgG detected 1.64 | |||||
| 2021 | Brazil | 34-year-old woman without comorbidities | 60 | N/A | Mild | Mild diarrhea | IgM, IgA, IgG detected <1:4 |
| Clade 20B | Worse | Dry cough, diarrhea, tiredness, headache, body ache, anosmia, ageusia | IgM, IgA, IgG detected 1:64 | |||||
| 2021 | Brazil | 29-year-old health care worker man without comorbidities | 225 | B.1.1.28 Spike D614G | Mild | Fever, myalgia cough, sore throat, diarrhea | IgG negative 180 days after the 1st infection |
| B,1,2 Spike D614G | Mild | Again symptoms | ||||||
| 2021 | Mexico | 40-year-old healthcare worker woman with hypertension, smoking | 134 | N/A | Moderate | Fever, dry cough, nasal drainage, dyspnea, myalgia, arthralgia, headache, anosmia, dysgeusia, decreased oxygen saturation up to 84%, maculopapular rash on the upper and lower limbs, chest, face, neck | |
| Worse | Sneezing, runny nose, myalgia, arthralgia, fever, dry cough, headache, dyspnea, emphysema of the right lung | |||||||
| 2021 | Mexico | 49-year-old health care worker woman with hypothyroidism | 129 | N/A | Mild | Nasal congestion, myalgia, arthralgia, chills, headache, dry cough, dysgeusia, anosmia, maculopapular exanthema, insomnia | |
| Mild | Headache, dry cough, odynophagia, myalgia, dyspnea, conjunctivitis | |||||||
| 2021 | Mexico | 53-year-old health care worker man without comorbidities | 107 | N/A | Mild | Fever, dyspnea, pneumonia | |
| Mild | Fever, chills, anosmia, dysgeusia dry cough, rhinorrhea, general malaise, chest pain, | |||||||
| 2021 | Mexico | 52-year-old health care worker man without comorbidities | 82 | N/A | Mild | Odynophagia, dry cough, nasopharyngeal exudate | |
| Worse | Myalgias, arthralgias, dry cough, dyspnea, odynophagia, pneumonia> intensive care for hypoxia | |||||||
| 2021 | India | 30-year-old health care worker man without comorbidities | 90 | N/A | Mild | Fever | 30 days after initial diagnosis IgG antibody negativity |
| Worse | Fever, severe myalgia, anosmia, loss of taste | 30 days after reinfection diagnosis IgG antibody positivity | ||||||
| 2021 | UK | 92-year-old man with dementia | 207 | 1st wave | Moderate | Pyrexia, dry cough, shortness of breath, bilateral pneumonia | |
| B.1.177 (Spain variant) | Moderate | Lethargy, persistent cough, pyrexia, pneumonia | ||||||
| 2021 | UK | 84-year-old man with dementia and Paget’s disease | 224 | 1st wave | Mild | Lethargy, confusion, headache, fatigue | |
| B.1.177 (Spain variant) | Mild | Positive | ||||||
| 2021 | UK | 59-year-old man with end stage renal failure | 236 | 1st wave | Mild | Cough, fluctuating temperature | |
| B.1.1.7 (Kent variant) | none | None | ||||||
| 2021 | USA | 59-year-old man with end stage renal failure and hemodialysis | 59 | N/A | Moderate | Cough, fever, pneumonia > hospitalization | |
| Milder | Cough, shortness of breath, >hospitalization | SARS-CoV-2 IgG antibody positive after re-infection | ||||||
| 2020 | USA (Washington) | Sexagenarian (age between 60 and 69) with emphysema and hypertension | 140 | Clade 19B | Severe | Fever, chills, productive cough, dyspnea, chest pain | |
| Clade 20A harboring the spike variant D614G | Severe, but milder than first | Dyspnea, dry cough, weakness | RBD, spike and NC IgG, spike IgM, NC IgA+ on D14 of reinfection | |||||
| 2021 | UK | 61-year-old south Asian with immunosuppression for ANCA-associated vasculitis | 180 | N/A | Severe | Dry cough, dyspnea, fever, myalgia, kidney dysfunction, pneumonia | N/A |
| Moderate | Fever, myalgia, dyspnea, pneumonia | |||||||
| 2020 | India | 25-year-old male healthcare worker | 108 | 9 SNVs compared to initial infection (19A first infection–20A second infection) | Asymptomatic | Asymptomatic | N/A |
| Asymptomatic | Asymptomatic with higher viral load | |||||||
| 2020 | India | 28-year-old female healthcare worker | 111 | 10 SNVs compared to initial infection; mutation 22882T > G (S:N440K) within the receptor binding domain found in the second episode | Asymptomatic | Asymptomatic | N/A |
| Asymptomatic | Asymptomatic with higher viral load | |||||||
| 2021 | SAU | 44-year-old woman healthcare worker | 108 | N/A | Moderate | Fever, chills, severe sore throat, fatigue | N/A |
| Moderate | Severe persistent productive cough, runny nose, loss of smell, partial loss of taste | |||||||
| 2021 | SAU | 35-year-old heavy male smoker | 94 | N/A | Asymptomatic | Asymptomatic | N/A |
| Worse | Fever, cough, body ache, abdominal pain, loss of taste | |||||||
| 2020 | Pakistan | 58-year-old cardiac surgeon male without comorbidities | 55 | N/A | Hospitalized for 30 days | Fatigue, headache, sore throat, pneumonia | N/A |
| Hospitalized for 14 days | Fever >39 °C, headache, muscle aches | |||||||
| 2021 | UK | 78-year-old man with type 2 diabetes mellitus, diabetic nephropathy, chronic obstructive pulmonary diseases, sleep apnea, ischemic heart disease | 250 | Lineage B.2 with no mutations in the S region | Discharged home | Mild illness | SARS-CoV-2 antibodies (using the Roche anti-SARS-CoV-2 IgM/IgG assay detecting antibodies targeting viral nucleocapsid “N” antigen) were detectable on 6 occasions between 4 June 2020 and 13 November 2020 with no evidence of antibody waning seen |
| Variant VOC-20201/01 of lineage B.1.1.7 with 18 amino acid replacement and deletions in the S region | Emergency intubation, worse | Shortness breath, severe hypoxia, pneumonia, myocardial infarction | ||||||
| 2021 | USA | 30-year-old female healthcare worker with idiopathic thrombocytopenic purpura, pancreatitis, GERD, anxiety, recurrent pneumonia | 183 | N/A | Mild | Fever, fatigue, sore throat, nasal congestion, dry cough, chest tightness | After 1st infection anti-SARS-CoV-2 IgG were negative |
| Mild | Headaches, fever, sinus congestion | After 2nd infection anti-SARS-CoV-2 IgG were positive | ||||||
| 2021 | USA | 81-year-old woman with immunosuppression for rheumatoid arthritis | 62 | N/A | Mild | Altered mental status, | N/A |
| Moderate | Cough, shortness of breath, oxygen requirement | |||||||
| 2021 | Iraq | 39-year-old man with hypertension | 112 | N/A | Moderate | Fever, dry cough, hypoxemia | SARS-CoV-2 2 months after discharge |
| Mild | Fever, not hypoxemia | |||||||
| 2021 | Iraq | 32-year-old man | 82 | N/A | Mild | Myalgia, fever | N/A |
| Mild | Myalgia | |||||||
| 2021 | Iraq | 40-year-old man | 50 | N/A | Severe | Fever, loss of smell, myalgia, dyspnea | N/A |
| Mild | Fever, sore throat | |||||||
| 2021 | Iraq | 46-year-old man | 74 | N/A | Mild | Fever, dry cough | N/A |
| Moderate | Fever, sore throat, loss of taste and smell | |||||||
| 2021 | Iraq | 39-year-old man | 122 | N/A | Severe | Fever, dry cough, dyspnea | N/A |
| Mild | Fever, sore throat | |||||||
| 2021 | Iraq | 32-year-old woman | 174 | N/A | Mild | Fever, dry cough, loss of smell, sore throat | N/A |
| Mild | Fever, sore throat, myalgia | |||||||
| 2021 | Iraq | 44-year-old man with colon cancer | 51 | N/A | Mild | Fever, myalgia | N/A |
| Mild | Myalgia | |||||||
| 2021 | Iraq | 26-year-old woman | 84 | N/A | Mild | Headache, sweating, loss of taste | N/A |
| Mild | Headache, myalgia | |||||||
| 2021 | Iraq | 26-year-old woman | 84 | N/A | Mild | Headache, loss of taste | N/A |
| Moderate | Myalgia, cough, dyspnea | |||||||
| 2021 | Iraq | 36-year-old woman with diabetes | 51 | N/A | Mild | Sore throat, fever | N/A |
| Severe | Fever, myalgia, cough, dyspnea | |||||||
| 2021 | Iraq | 34-year-old man | 49 | N/A | Mild | Headache, fever | N/A |
| Severe | Myalgia, fever, headache, anorexia | |||||||
| 2021 | Iraq | 79-year-old woman with heart failure and hypertension | 58 | N/A | Severe | Fever, dyspnea | N/A |
| Severe | Cough, anorexia, fever | |||||||
| 2021 | USA | 59-year-old Caucasian male with Hodgkin lymphoma | 150 | N/A | Moderate | Shortness of breath, dry cough, tachycardia, oxygen desaturation to 85% | N/A |
| Moderate | Chills, worsening shortness of breath, productive cough, fever, tachycardia, hypoxemia | |||||||
| 2021 | Japan | 58-year-old with mild dyslipidemia | 105 | N/A | Moderate | Fever, bilateral pneumonia | After 1st episode IC50 of neutralizing antibodies anti-SARS-CoV-2 was 50.0 microg/mL |
| Asymptomatic | Asymptomatic | After 2nd episode IC50 of neutralizing antibodies anti-SARS-CoV-2 was 14.8 microg/mL | ||||||
| 2020 | India | 21-year-old female | 50 | N/A | Asymptomatic | Asymptomatic | N/A |
| mild | Complete loss of smell for 2 weeks | |||||||
| 2021 | India | 39-year-old male with multiple myeloma | 84 | N/A | Asymptomatic | Asymptomatic | N/A |
| Severe | High grade fever, chills, shortness of breath, bilateral pneunomia | |||||||
| 2021 | India | 33-year-old male with T cell acute lymphoblastic leukemia | 60 | N/A | Severe | Fever, cough, pneumonia | N/A |
| Severe | Headache, vomiting, high grade fever, pneumonia | |||||||
| 2021 | India | 26-year-old male with Philadelphia chromosome positive acute lymphoblastic leukemia | 91 | N/A | Asymptomatic | Asymptomatic | N/A |
| Moderate | Fever | |||||||
| 2021 | USA | 70-year-old man with hypertension, diabetes mellitus, coronary artery disease | 45 | N/A | Asymptomatic | Asymptomatic | COVID-19 IgG positive after 1st infection |
| Worse | Shortness of breath, cough, chest pain, myalgias | |||||||
| 2021 | USA | Late 50s woman with hypertension, hepatitis C, heart failure | 75 | N/A | Asymptomatic | Asymptomatic | N/A |
| Worse | Fever, myalgias, sore throat | |||||||
| 2021 | USA | 66-year-old man with bipolar disorder, end-stage renal disease due to lithium toxicity and renal transplantation | 210 | Clade B.1 | Mild | Fever, fatigue, dry cough | Failure of humoral immunity with defective response of the neutralizing antibodies after primary infection |
| Clade B.1.280 | Milder | Fatigue and nonproductive cough | ||||||
| 2021 | India | 61-year-old male healthcare worker | 75 | 20B clade | Asymptomatic | Asymptomatic | N/A |
| 20B clade with 10 variations | Mild | Cough, weakness | ||||||
| 2020 | USA (Virginia) | 42-year-old man military healthcare provider | 64 | Lineage B.1.26 | Moderate, clinical resolution in 10 days | Cough, fever, myalgias | |
| Lineage B.1.26 with several potential variations | Severe, worse | Fever, cough, shortness of breath, gastrointestinal symptoms, pneumonia | Spike IgG+ on D8 of reinfection | |||||
| 2020 | France | 42-year-old Parisian male | 7 months | N/A | Home-managed | Dyspnea, fever, headache, diarrhea, abdominal pain, ageusia, total less of smell | IgG 2 months after |
| Milder | Fever, nasal burning, total loss of taste and smell | |||||||
| 2020 | Spain | 38-year-old Spanish health care worker female | 6 months | N/A | Moderate—hospitalized for 7 days | Dyspnea, fever, headache, diarrhea, loss of smell | N/A |
| Milder | Fever, headache, new total loss of smell and taste | |||||||
| 2020 | South Korea | 21-year-old healthy woman | 26 | Clade V—found in Asia and Europe | Hospitalized with few symptoms | Sore throat | |
| Clade G—found in south Korea | Mild | Cough, sore throat | IgG+ | |||||
| 2021 | Italy | 41-year-old healthcare worker woman | 289 | 20B | Mild | Fever, arthralgia, headache, diarrhea, anosmia, ageusia | IgG positive after 1st infection and after 2nd infection |
| 20E (EU1) | Mild | Headache, sore throat, diarrhea | ||||||
| 2021 | UK | 55-year-old man with X-linked agammaglobulinemia | 56 | N/A | Moderate | Purulent sputum, fever, breathlessness, fever, headache, myalgia, chest tightness | N/A |
| Worse | Short of breath, fevers > death | |||||||
| 2020 | Italy | 69-year-old man, heavy smoker with classic Hodgkin’s lymphoma with mixed cellularity | 131 | N/A | Moderate with 3 months of hospitalization | Pneumonia, fever, diarrhea | IgG+ 50 days after hospitalization |
| Moderate with 64 days of hospitalization | Fever, dyspnea, anemia, leukopenia, pneumonia | N/A | ||||||
| 2021 | India | 33-year-old man | 90 | N/A | Mild | Sore throat | N/A |
| Worse | Influenza like Illness symptoms with breathing difficulty | |||||||
| 2021 | India | 27-year-old man | 69 | N/A | Asymptomatic | Asymptomatic | N/A |
| Worse | Fever, cough, myalgia | |||||||
| 2021 | India | 48-year-old woman | 97 | N/A | Mild | Myalgia | N/A |
| Mild | Myalgia | |||||||
| 2021 | India | 26-year-old woman | 55 | N/A | Mild | Fever, myalgia | N/A |
| Mild | Fever, sore throat, myalgia | |||||||
| 2021 | India | 25-year-old man | 89 | N/A | Mild | Fever, sore throat, myalgia and loss of smell and taste | N/A |
| Mild | Fever | |||||||
| 2021 | India | 31-year-old man | 70 | N/A | Asymptomatic | Asymptomatic | N/A |
| Worse | Myalgia | |||||||
| 2021 | India | 51-year-old woman | 157 | N/A | Asymptomatic | Asymptomatic | N/A |
| Worse | Myalgia, headache, pneumonia (25% lung involvement) | |||||||
| 2021 | USA | 16-year-old woman with end-stage renal disease | 90 | B.1.2 | Mild | Sore throat, fatigue, nasal congestion, rhinorrhea, dry cough | IgM+ and IgG− after the 2nd infection |
| B.1.1.7 | Milder | Leg pain, fatigue, swelling leg, fever | ||||||
| 2021 | Spain | 62-year-old male healthcare worker with previous history of mild asthma, hypertension, dyslipidemia, liver steatosis, hyperuricemia, and overweight (body mass index ≥ 30 kg/m2) | 158 | Mild | Fever of 38 °C, diarrhea, anosmia, dysgeusia, cough, intense asthenia, and arthromyalgia | After reinfection weak immune response, with marginal humoral and specific T-cell responses against SARS-CoV-2. All antibody isotypes tested as well as SARS-CoV-2 neutralizing antibodies increased sharply after day 8 post symptoms. A slight increase of T-cell responses was observed at day 19 after symptom onset | |
| B.1.79 (G) | Worse | Intense arthromyalgias, headache, fever, cough, and dyspnea > admitted to the emergency room for worsening dyspnea, cough, chills, fever 39 °C, myalgias, anosmia, and ageusia. His respiratory rate was 36 breaths/minute, his heart rate was 100 beats/minute, and he had bilateral inspiratory crackles. The chest radiograph showed bilateral alveolar-interstitial infiltrates | ||||||
| 2021 | USA | 53-year-old female with liver transplant in 2010 due to alcoholic cirrhosis, hypertension, hypothyroidism, anxiety, and chronic kidney disease | 90 | N/A | Severe | Encephalopathy due to her COVID-19 | N/A |
| Mild | Nausea, vomiting, diarrhea, and myalgias | |||||||
| 2020 | Denmark | 89-year-old immunocompromised woman (Waldestrom macroglobulinemia) | 59 | The 2 strains differed at 10 nucleotide positions in ORF1a (4), ORF1b (2), spike (2), ORF3A (1), M (1) genes | Hospitalized for 5 days | Fever, severe cough, persisting fatigue | IgM- |
| Worse | Fever, cough, dyspnea > death after 2 weeks | N/A | ||||||
| 2020 | USA | 51-year-old African American male with hypertension and hemodialysis history | 2 months | N/A | Asymptomatic | Positive for NAAT and IgG at a routine control during hemodialysis | IgM−, IgG+ |
| Severe, hospitalized with non-invasive positive pressure mechanical ventilation | Fever 38.3 °C, severe dyspnea, pneumonia | IgG+, IgM+, IgA+ | ||||||
| 2020 | Israel | 22-year-old woman without comorbidities | 111 | N/A | Mild with home back after 23 days | Fever, cough | |
| Asymptomatic | Tachycardia | IgG+ | ||||||
| 2021 | Brazil | 29-year-old | 281 | 20A | Mild | Fever, myalgia, cough, sore throat, nausea, and back pain | |
| 20J (P.1) | Mild | Fever, cough, sore throat, diarrhea, anosmia, ageusia, headache, runny nose, and resting pulse oximetry of 97% | ||||||
| 2021 | Brazil | 50-year-old | 153 | 20B | Mild | Fever, cough, and tiredness | |
| 20J (P.1) | Mild | Cough, headache, and runny nose | ||||||
| 2021 | Brazil | 40-year-old woman | 282 | 20A | Mild | Fever, headache, chest pain, and weakness | |
| 20J (P.1) | Mild | Sore throat and running nose | ||||||
| 2020 | India | 26-year-old man healthcare worker | 97 | N/A | Asymptomatic | Asymptomatic | N/A |
| Asymptomatic | Asymptomatic | |||||||
| 2021 | USA | 46-year-old man with hypertension, gastroesophageal reflux disease, plantar fasciitis | >90 | N/A | Mild | Fever, myalgias, sore throat, chills, headaches, nausea, shortness of breath | SARS-CoV−2 IgG testing 1st test: 1:4096 (BCM laboratory) |
| Asymptomatic | Asymptomatic | SARS-CoV−2 IgG testing 2nd test: 1:2048 (BCM laboratory) | ||||||
| 2021 | USA | 27-year-old woman | >90 | N/A | Mild | Congestion, fatigue, loss of taste, loss of smell, headache | N/A |
| Milder | Fever, chills, fatigue | |||||||
| 2021 | USA | 53-year-old man with hypertension, sleep apnea | >90 | N/A | Mild | Cough, congestion, loss of taste, loss of smell | SARS-CoV−2 IgG testing 1st test: 1:2048 (BCM laboratory) |
| Asymptomatic | Asymptomatic | SARS-CoV−2 IgG testing 2nd test: 1:1024 (BCM laboratory) | ||||||
| 2021 | USA | 66-year-old woman with diabetes mellitus, rheumatoid arthritis, systemic lupus erythematosus, congestive heart failure, renal disease, gout, hypertension | >90 | N/A | Mild | Fatigue | N/A |
| Asymptomatic | Asymptomatic | |||||||
| 2021 | USA | 73-year-old woman with hypertension, hyperlipidemia, depression | >90 | N/A | Mild | Congestion, sore throat, headache | N/A |
| Mild | Cough, shortness of breath, congestion, abdominal pain, nausea, vomiting, headache | |||||||
| 2021 | USA | 42-year-old woman with breast cancer | >90 | N/A | Mild | Cough, shortness of breath, fatigue, loss of taste, loss of smell, headache, fever | SARS-CoV−2 IgG testing 1st test: 1:4096 (BCM laboratory) |
| Asymptomatic | Asymptomatic | |||||||
| 2021 | USA | 36-year-old man | >90 | N/A | Mild | Cough, fatigue, nausea, loss of smell, fever | SARS-CoV−2 IgG testing 1st test: 1:4096 (BCM laboratory), 2nd test: 1:4096 (BCM laboratory) |
| Asymptomatic | Asymptomatic | |||||||
| 2021 | Brazil | 45-year-old woman | 147 | Lineage B.1.1.33 with S:G1219C mutation | Mild | Diarrhea, myalgia, asthenia, odynophagia for 7 days | N/A |
| Lineage P.2 (or B.1.1.28.2) with S:E484K mutation | Moderate | Headache, malaise, ageusia, muscle fatigue, insomnia, mild dyspnea, shortness of breath | ||||||
| 2021 | Colombia | 44-year-old male, healthcare worker | 103 | N/A | Asymptomatic | Asymptomatic | N/A |
| Moderate | Malaise, chills, headache, fever, odynophagia | |||||||
| 2020 | Turkey | 23-year-old woman | 116 | N/A | Hospitalized | Fever >39 °C, chills, fatigue, cough, headache, sore throat, muscle and joint pain | N/A |
| Recovered in 10 days | Fever 28.7 °C, chills, fatigue, loss of appetite, taste and smell loss, muscle and joint pain | IgG slightly positive | ||||||
| 2021 | USA | 40-year-old man | 89 | N/A | Mild | Fever, cough | N/A |
| Worse | Dyspnea, tachycardia > death | |||||||
| 2020 | Ecuador | 46-year-old man | 63 | Nextstrain 20A/GISAID B1.p9 lineage | Mild | Intense headache, drowsiness | IgM+ IgG− on D7 of initial infection |
| Nextstrain 19B/GISAID A.1.1 lineage; 18 mutations difference | Moderate | Odynophagia, nasal congestion, fever 39 °C, back pain, productive cough, dyspnea | IgM+ IgG+ on D28 | |||||
| 2021 | Spain | 60-year-old male, with chronic kidney disease (CKD) due to focal and segmental glomerulosclerosis that received his first kidney transplant 2004 | 149 | N/A | Mild | Cough and low-grade fever | Antibodies (IgM and IgG) for SARS-CoV2 resulted negative after reinfection |
| Worse | Respiratory fever and acute injury of the allograft function. A chest X-ray showed bilateral infiltrates with unilateral pleural effusion > death | |||||||
| 2021 | Colombia | 54-year-old woman with hypertension, gastritis, arthrosis | 33 | B.1 | Mild | Fever, cough, odynophagia, fatigue | N/A |
| B.1.1.269 | Milder | Fever, odynophagia | ||||||
| 2021 | India | 47-year-old man | 46 | 15 genetic variants with 22882T > G (Spike N440K) | Asymptomatic | Asymptomatic | N/A |
| 17 genetic variants with 22882T > G (Spike N440K) | Worse | Fever, cough, malaise | ||||||
| 2021 | Brazil | 37-year-old healthcare worker woman | 116 | B.1.1.33 | Mild | Headache, runny nose, diarrhea, myalgia | IgG+ after re-infection |
| VOI P.2 with mutation S-E484K | Mild | Headache, ageusia, anosmia, fatigue | ||||||
| 2021 | Spain | 76-year-old man with hypertension, biological aortic heart valve replacement, and end-stage kidney disease secondary to autosomal dominant polycystic kidney disease | 58 | Asymptomatic | Asymptomatic | IgG and IgM to SARS-CoV-2 tested negative after 1st and 2nd episode | |
| Worse | Fever, cough, and shortness of breath, bilateral pneumonia > death 18 days after admission | |||||||
| 2021 | Brazil | 26-year-old woman | 128 | Non-VOC virus | Mild | Dry cough, dizziness, headache, fatigue, stuffy nose, back pain, loss of taste, nausea, diarrhea | |
| VOC-virus P.1 variant | Mild | Dry cough, dizziness, headache, fatigue, diarrhea, joint pain legs, difficult breathing | ||||||
| 2021 | USA | 62-year-old woman with hypertension, hypothyroidism, chronic lower back pain | 90 | N/A | Hospitalized | Worsening shortness of breath, cough, hypoxia | N/A |
| Worse with intubation twice | Tachypnea, hypoxia, pneumonia | |||||||
| 2021 | Iran | 42-year-old man | 128 | 20G with 11 mutations | Mild | Cough, headache, severe diarrhea | IgG and IgM negative |
| 20G with 17 mutations | Mild | Body pain, shortness of breath, headache, anosmia | IgG and IgM negative | |||||
| 2021 | Iran | 32-year-old woman | 63 | N/A | Mild | Headache, sore throat, cough, fever | The antibody titration was achieved positive by the rapid test (sensitivity 72%, specificity: 76%) for IgM (At the time of second infection, IgG titration was assessed as 4.89 AU/mL which after two months turned to a significant raise (over ELISA reader standard range). |
| D614G mutation | Worse | Severe cough, fever, fatigue | ||||||
| 2021 | Iran | 54-year-old man | 156 | L139L non-synonymous mutation | Mild | Fatigue, anxiety, chest pain, cough, fever | IgM and IgG were detected in the first incidence, and he was being followed up to the second virus presentation. In the whole duration between two incidences, IgG test was positive. Antibody titration at the time of second infection showed that IgG level was 5.25 IU/mL which increased to 27.5 IU/mL after about 2 weeks. |
| L139L non-synonymous mutation | Mild | Milder fatigue, chest pain, dizziness, diarrhea | ||||||
| 2021 | Iran | 42-year-old man | 111 | N/A | Mild | Shortness of breath, sore throat, shaking chills, pain, diarrhea | The IgG titration was 17.5 IU/mL which decreased to 6.5 IU/mL after almost 2 weeks. |
| D614G mutation | Mild | Similar to the first infection with severe diarrhea | ||||||
| 2021 | Austria | 95-year old man with dementia, hypertension, total thyroidectomy | 124 | N/A | Mild | Fever, leukopenia | N/A |
| Severe | Pneumonia | |||||||
| 2021 | Gambia | 31-year-old woman without comorbidities | 145 | B1 | Mild | Mild | |
| B1.1.74 | Mild | Mild | ||||||
| 2021 | Gambia | 36-year-old woman without comorbidities | 184 | B.1.235 | Asymptomatic | Asymptomatic | |
| B.1 | Worse | Mild | ||||||
| 2021 | Italy | 63-year-old healthcare man with type II diabetes, atrial fibrillation, chronic obstructive pulmonary disease | 299 | Clade 20A | Asymptomatic | Asymptomatic | |
| Clade 20E | Worse | Shortness of breath with rapid worsening of clinical presentation and recovering in intensive care unit > death | ||||||
| 2020 | Belgium | 39-year-old female immunocompetent healthcare worker | 185 | Different clades: 19A | Mild | Cough, dyspnea, headache, fever, general malaise | IgG+ |
| 20A | Milder | Dyspnea | IgM and IgG+ | |||||
| 2020 | USA | 70-year-old male with obesity, neuropathy, asthma, obstructive sleep apnea, hypertension | 7 months | N/A | Hospitalized | Worsening shortness of breath, tachypneic, mild, patchy mid and lower lung airspace disease bilaterally | SARS-CoV-2 IgG− |
| Hospitalized | Shortness of breath, fever, body aches, nausea, malaise | |||||||
| 2020 | India | 78-year-old man with coronary artery disease | 57 | N/A | Mild | Fever, cough for 2 days | N/A |
| Mild | Fever, cough, dyspnea for 1 day | |||||||
| 2021 | Ecuador | 28-year-old man | 102 | B.1.1 | Mild | Sore throat, cough, headache, nausea, diarrhea, anxiety, panic attack | IgM and IgG negative after 1st infection |
| Different in 27 nucleotides | Mild | Anosmia, ageusia, fever, headache | IgM and IgG negative after 2nd infection | |||||
| 2020 | Qatar | 57-year-old male with diabetes mellitus | 86 | N/A | Asymptomatic | Asymptomatic, screening for exposition to an infected work colleague | N/A |
| Symptomatic | Fever, myalgia, headache, productive cough | IgM and IgG+ | ||||||
| 2021 | India | 27-year-old male doctor | 66 | Lineage B.1 | Mild, 2 days of symptoms | Sore throat, nasal congestion, rhinitis | N/A |
| Lineage B with 7 differences | Mild, worse than initial (1 week) | Myalgia, fever, non-productive cough, fatigue | Abbott anti-NC IgG− on D5 of reinfection | |||||
| 2021 | India | 31-year-old male doctor | 65 | Lineage B.1.1 | Asymptomatic | Nothing | N/A |
| Lineage B.1.1 with 8SPSs in initial strain compared to reference not present in reinfection strain including D614G | Mild, worse than initial (2 days) | Myalgia, malaise | Abbott NC IgG− on D7 of reinfection | |||||
| 2021 | India | 27-year-old male doctor | 19 | Lineage B.1.1 | Asymptomatic | Asymptomatic—screening prior going home to visit parents | N/A |
| Lineage B.1.1 with 9 SNPs compared to reference not present in initial infection strain including D614G | Mild | Fever, headache, myalgia not productive cough | IgG/IgM/IgA− | |||||
| 2021 | India | 24-year-old woman nurse | 55 | Lineage B.1.1 | Mild, 5 days | Sore throat, rhinitis, myalgia | N/A |
| Lineage B.1.1 with 10SNPs compared to reference not present in initial infection strain including D614G | Mild, worse than initial—3 weeks | Fever, myalgia, rhinitis, sore throat, not productive cough, fatigue | IgG/IgM/IgA− | |||||
| 2021 | USA | 31-year-old healthcare worker man | 79 | N/A | Severe | Malaise, cough, shortness of breath, anosmia, =2 saturation to 88%, pneumonia | N/A |
| Milder | Malaise, aphthous gingival ulcer, desquamating palmar lesion, fever, myalgia | |||||||
| 2021 | USA | 69-year-old woman with asthma, hypercholesteremia, hypertension, OSA (obstructive sleep apnea) | 70 | N/A | Mild | Shortness of breath, dry cough, headache, fatigue, fevers | N/A |
| Moderate | Cough, fever, ageusia | |||||||
| 2021 | Brazil | 76-year-old woman with chronic renal failure and renal squamous cell carcinoma | 104 | 9 single nucleotide variations (SNVs) | Severe | Cough, fever, pneumonia | N/A |
| Worse | Cough, fever, pneumonia > death | |||||||
| 2021 | Brazil | 39-year-old man with chronic cardiovascular disease, diabetes mellitus | 101 | P.1 | Not reported | Not reported | N/A |
| P.2 | Worse | Dyspnea, fatigue, respiratory distress > intubated > death 12 days after the onset of symptoms | ||||||
| 2021 | France | Mid-20s healthcare worker man without comorbidities | >83 | November N/A | Asymptomatic | Asymptomatic | N/A |
| B1.351—identified in December 2020 in South Africa | Worse | Cough | ||||||
| 2021 | France | Mid-20s healthcare worker woman without comorbidities | 288 | April 2020—N/A | Mild | Fever, headache, chills, diarrhea, loss of taste and smell | N/A |
| B1.351 | Milder | Fever, headache, chills | ||||||
| 2021 | France | Late-20s healthcare worker woman without comorbidities | 90 | November 2020—N/A | Mild | Fever, muscle pain, headache, loss of taste and smell | N/A |
| B1.351 | Milder | Cough, muscle pain | ||||||
| 2020 | Brazil | 29-year-old man healthcare professional without comorbidities | 53 | N/A | Mild | Myalgia, fever | N/A |
| Mild | Fever, anosmia, loss of taste | |||||||
| 2020 | Brazil | 63-year-old man healthcare professional without comorbidities | 58 | N/A | Mild | Diarrhea, fever | N/A |
| Mild | Hypoxemia, fever | |||||||
| 2020 | Brazil | 40-year-old woman healthcare professional with ankylosing spondylitis and asthma | 70 | N/A | Moderate | Fever, Pneumonia, myalgia | Not specified |
| Mild | Anosmia, fever | |||||||
| 2020 | Brazil | 67-year-old man healthcare professional with obesity, apnea syndrome, rhinitis | 54 | N/A | Mild | Coryza, arthralgia | Not specified |
| Hospitalized with high-flow oxygen therapy | Hypoxia | |||||||
| 2020 | Brazil | 47-year-old man healthcare professional without comorbidities | 56 | N/A | Mild | Myalgia, fever | Not specified |
| Mild | Fever | |||||||
| 2020 | Brazil | 31-year-old man healthcare professional without comorbidities | 57 | N/A | Moderate | Hypoxemia, myalgia, diarrhea, fever | Not specified |
| Moderate | Hypoxemia, fever | |||||||
| 2021 | USA | Female in 20s with asthma, obesity, anxiety, depression | 19 | PANGOLIN A.3 lineage | Mild | Cough, chills, exertional dyspnea, sore throat, dizziness, rhinorrhea, fever | N/A |
| PANGOLIN B.1.1 lineage | Milder | |||||||
| Cough, fatigue, dyspnea | ||||||||
| 2021 | Iran | 15-year-old boy with acute myeloid leukemia M3 | 43 | N/A | Moderate | Cough, dyspnea, patchy infiltration in the left lung | IgG+ IgM− |
| Severe | Fever, neutropenia, cough, myalgia and shivering, O2 saturation at 75%, pneumonia | IgG− | ||||||
| 2021 | Libya | 18-year-old man | 80 | N/A | Mild | Fever, headache, sore throat, cough, shortness of breath, anosmia | IgG positive after re-infection |
| Worse | Fever, cough, muscle pain, dyspnea, hypoxia | |||||||
| 2020 | USA (Nevada) | 25-year-old man without comorbidities | 48 | Clade 20C | Mild | Sore throat, cough, headache, nausea, diarrhea | N/A |
| Clade 20C with 11SNP mutation | Severe with hospitalization | Fever, headache, dizziness, cough, nausea, diarrhea, hypoxia, shortness of breath | Roche Elecsys Anrti-SARS-CoV-2 IgM/IgG+ on D8 of reinfection | |||||
| 2020 | Hong Kong | A 33-year-old male | 142 | Nextstrain 19A/GISAID V/Pangolin lineage B.2 | Mild—hospitalized | Fever, headache, cough, sore throat | IgG negativity by ELISA or microsphere based antibody assay 10 days post symptom onset; IgG positivity but IgM negativity by indirect immunofluoresence assay; neutralizing antibody presence 10 days post-symptom onset with conventional and pseudovirus-based neutralization tests (VNTs) |
| Nextstrain 20A/GISAID G/Rambout B.1.79; 24 nucleotides difference | Asymptomatic, systematic screening | Asymptomatic | IgG negativity by ELISA or microsphere based antibody assay 1 day post-hospitalization, but positivity at day 5; absence of neutralizing antibodies by VNTs and IgM negativity by IFI assay and CLIA 1 day post-hospitalization; then positivation on day 3; neutralizing antibody detection on day 3; IgG detection by IFon day 3; high affinity IgG | |||||
| 2021 | USA | 61-year-old man with liver transplant due to chronic hepatitis B and C infections | 111 | Genome of 2nd episode differed by 11 to 12 single base substitutions | Mild | Fever, nausea, vomiting, cough | |
| Worse | Confusion, hallucination, lethargy, hypoxia | Anti-SARS-CoV-2 assay positive after 2nd episode | ||||||
| 2021 | UK | 93-year-old British male with multiple myeloma, cognitive impairment | 55 | N/A | 14 days—hospitalized | Lethargy, reduced appetite, diarrhea | |
| Cough, fever, dyspnea | Abbott Architect SARS-CoV-2 IgG+ on D58 | |||||||
| 2021 | UK | 82-year-old British male with atrial fibrillation, congestive cardiac failure, abdominal aortic aneurism, lung cancer, diabetes | 87 | N/A | Mild—hospitalized | Fever, cough, sore throat, dyspnea, hemoptysis, hypoxia | |
| Milder | Fever, cough, dyspnea | Abbott Architect SARS-CoV-2 IgG+ on D88. 92 | ||||||
| 2020 | Brazil | 36-year-old female medical doctor without comorbidities | 87 | N/A | Moderate | Rhinorrhea, sore throat, low fever, diarrhea, asthenia, mild headache, erythematous vesicles on her right calf, severe musculoskeletal pain of the lower limbs, hyperesthesia | IgG− 23 days after the onset, IgM/IgG− after 33 and 67 days from onset |
| Worse | Nasal obstruction, hyaline rhinorrhea, sudden and complete anosmia and ageusia, frontal headache and asthenia, pneumonia | IgG+ at the 20th day | ||||||
| 2021 | USA | 44-year-old Hispanic man with type 2 diabetes mellitus, obesity | 4 months | N/A | Severe with tracheostomy | Dyspnea, stridor, difficulty at breath, | IgG+ |
| Mild | Fever, respiratory decompensation | |||||||
| 2020 | Pakistan | 41-year-old healthcare worker man | 133 | N/A | Mild | Fever, oxygen saturation of 90–92%, bilateral lung infiltrates, mild shortness of breath, loss of taste, severe restlessness, insomnia, body-aches | SARS-CoV-2 antibodies: 1.97 |
| Milder | Fever, moderate shortness of breath, loss of smell, moderate restlessness, insomnia, body aches | SARS-CoV-2 antibodies: 0.08 | ||||||
| 2020 | Belgium | 51-year-old woman with asthma | 93 | Pangolin Lineage B.1.1 | Moderate with self-quarantine for 2 weeks | Headache, myalgia, fever, cough, chest pain, dyspnea; some persisting symptoms for 5 weeks | N/A |
| Lineage A; 11 nucleotide differences | Milder with resolution in 1 week | Headache, cough, fatigue, rhinitis | Roche nucleocapsid IgG+ on D7 of reinfection | |||||
| 2021 | Switzerland | 36-year-old female physician | 205 | Clade 20A | Mild | Asthenia, headache, slight memory loss | Positivity for anti-S1 IgG and anti-N Ig at 14th and at 30th days |
| Clade 20A.EU2 with non-synonymous mutation in the S (S477N) | Mild | Asthenia, shivering, rhinorrhea, anosmia, arthralgia, headache, exertional dyspnea for 10 days | Positivity for anti-S1 IgG and anti-N Ig | |||||
| 2021 | India | 58-year-old woman with hypertension, hypothyroidism | 120 | N/A | Mild | Fever, generalized body ache, running nose, soreness of throat | Total antibody and immunoglobulin G antibody test for COVID-19 were negative after first infection |
| Milder | Fever, generalized body ache, dry cough, throat pain | |||||||
| 2021 | India | 58-year-old woman with hypertension and hypothyroidism | 91 | N/A | Mild | Low-grade intermittent fever, generalized body ache, running nose and soreness of throat | N/A |
| Mild | Intermittent fever, generalized body ache, dry cough, and throat pain | |||||||
| 2021 | UK | 25-year-old male UK doctor | 17 | N/A | Mild | High-grade fevers, headache of 3-day duration, severe fatigue lasting 3 weeks | N/A |
| Milder | Fatigue, coryzal symptoms for 4 days | Rest at home | ||||||
| 2021 | USA | 25-year-old female medical student with vitiligo | 120 | N/A | Asymptomatic | Asymptomatic | IgG+ |
| Severe | Fever, abdominal pain, fatigue, vomiting and fulminant myocarditis with co-infection of parvovirus and SARS-CoV-2 | N/A | ||||||
| 2021 | Brazil | 41-year-old woman with gastroplasty history | 146 | B.1.1.33 lineage | Mild | Headache, myalgia, fatigue, fever, dry cough, shortness of breath, anosmia, loss of taste | N/A |
| B.1.1.28 lineage | Mild | Headache, myalgia, fatigue, fever, dry cough, shortness of breath, anosmia, loss of taste, diarrhea, loss of appetite, dizziness | ||||||
| 2021 | Brazil | 34-year-old healthcare worker woman with chronic respiratory disease | 173 | B.1.1.28 lineage | Mild | Fever, cough, odynophagia, dyspnea | N/A |
| P2 | Mild | Headache, running nose, fever, sore throat | ||||||
| 2021 | Iran | 50-year-old man | 230 | N/A | N/A | N/A | N/A |
| 2021 | Iran | 81-year-old woman | 234 | N/A | Moderate | N/A | N/A |
| Worse | Death for COVID-19 | |||||||
| 2021 | Iran | 42-year-old woman | 107 | N/A | N/A | N/A | N/A |
| 2021 | Iran | 27-year-old man | 115 | N/A | N/A | N/A | N/A |
| 2021 | Iran | 79-year-old man | 150 | N/A | Moderate | N/A | N/A |
| Worse | Death for COVID-19 | |||||||
| 2021 | Iran | 86-year-old man | 164 | N/A | Moderate | N/A | N/A |
| Worse | Death for COVID-19 | |||||||
| 2021 | Iran | 90-year-old woman | 130 | N/A | N/A | N/A | N/A |
| 2021 | Iran | 13-year-old woman | 124 | N/A | N/A | N/A | N/A |
| 2020 | China | 33-year-old female | 59 | N/A | Moderate—hospitalized for 16 days | Reduction of IgG+ to − | |
| Moderate | IgG+ | |||||||
| 2020 | China | 33-year-old female | 86 | N/A | Severe—hospitalized for 38 days | Reduction of IgG+ to weak+ | |
| Moderate | IgM+ and IgG+ | |||||||
| 2021 | South African | 58-year-old male with asthma | 120 | N/A | Mild | Dyspnea, fever | IgG+ |
| South African variant 501Y.V2 | Severe with intubation and mechanical ventilation | Dyspnea, fever, severe acute respiratory distress syndrome |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lo Muzio, L.; Ambosino, M.; Lo Muzio, E.; Quadri, M.F.A. SARS-CoV-2 Reinfection Is a New Challenge for the Effectiveness of Global Vaccination Campaign: A Systematic Review of Cases Reported in Literature. Int. J. Environ. Res. Public Health 2021, 18, 11001. https://doi.org/10.3390/ijerph182011001
Lo Muzio L, Ambosino M, Lo Muzio E, Quadri MFA. SARS-CoV-2 Reinfection Is a New Challenge for the Effectiveness of Global Vaccination Campaign: A Systematic Review of Cases Reported in Literature. International Journal of Environmental Research and Public Health. 2021; 18(20):11001. https://doi.org/10.3390/ijerph182011001
Chicago/Turabian StyleLo Muzio, Lorenzo, Mariateresa Ambosino, Eleonora Lo Muzio, and Mir Faeq Ali Quadri. 2021. "SARS-CoV-2 Reinfection Is a New Challenge for the Effectiveness of Global Vaccination Campaign: A Systematic Review of Cases Reported in Literature" International Journal of Environmental Research and Public Health 18, no. 20: 11001. https://doi.org/10.3390/ijerph182011001
APA StyleLo Muzio, L., Ambosino, M., Lo Muzio, E., & Quadri, M. F. A. (2021). SARS-CoV-2 Reinfection Is a New Challenge for the Effectiveness of Global Vaccination Campaign: A Systematic Review of Cases Reported in Literature. International Journal of Environmental Research and Public Health, 18(20), 11001. https://doi.org/10.3390/ijerph182011001