Highlights
What are the main findings?
- Adolescents with high access and sociocultural privilege had more negative urine drug screens during treatment but were more likely to have an alcohol use disorder (AUD) diagnosis and to use multiple substances.
- Socioculturally disadvantaged adolescents had more emergency department visits
- During adolescent substance treatment.
What are the implications of the main findings?
- These findings suggest the importance of assessing sociocultural factors at the outset of adolescent substance treatment.
- Future research should evaluate interventions to address sociocultural factors as a way to improve outcomes and promote health equity.
Abstract
Background: Adolescent mental health and substance misuse is a growing issue, disproportionately affecting diverse youth and those in low-resourced, high-stress environments. Yet, despite recent advances in evidence-based practices for adolescent substance use, perpetuating factors remain under-explored and marginalized, and underserved groups continue to be underrepresented. The current study aimed to investigate sociocultural factors impacting substance misuse and treatment outcomes. Methods: Data from adolescents receiving combined mental health and substance misuse treatment at a regional safety-net hospital were analyzed. Using Latent Class Analysis (LCA), demographic variables including insurance coverage, area deprivation, race, ethnicity, age, gender, court involvement, and primary mental health diagnoses were used to identify unique adolescent subgroups based on these different sociocultural risk factors. Identified classes were tested as predictors of treatment engagement, length of treatment, future service utilization, substance misuse, and urine drug screen results. Results: Five unique subgroups were identified, differentially impacting substance misuse, future service utilization, and treatment outcomes. Conclusions: These results highlight the need for improved access to resources for adolescents who have been marginalized and traditionally underserved. Furthermore, the identified subgroups can inform future research and practice.
1. Introduction
The World Health Organization characterizes adolescence—the developmental period between the ages of 10 and 19—as a critical time for intervention to improve lifelong health [1]. Adolescent substance misuse is a highly prevalent [2,3,4] issue disrupting health with numerous short- and long-term consequences including relational challenges, poor school engagement, justice system involvement, and cognitive impairments [5,6,7]. Adolescent substance misuse is also associated with increased risk of misuse in adulthood [8] and is a leading cause of adolescent mortality [9,10,11,12]. Compounding this significant issue, adolescent substance misuse and mental health concerns often co-occur [13]. Specifically, based on national data reported in 2024, of adolescents with a substance use disorder, 2 out of 5 also had a mental health disorder [3]. Furthermore, adolescents with co-occurring mental health concerns are more likely to engage in some types of substance misuse including binge drinking and tobacco use [3]. The comorbidity of substance misuse and mental health concerns amplify the negative outcomes for adolescents [14,15,16,17] and contribute to the high mortality rates found in past research [9,10,11,12], amplifying the impact of adolescent substance misuse and mental health concerns on society more generally [18].
Despite the obvious need for targeted and effective prevention and treatment options and the recent advances in this area [19,20,21], combined substance misuse and mental health concerns in adolescence continue to be an understudied and under-practiced area. Unfortunately, according to results from the 2024 National Survey on Drug Use and Health, there continue to be major gaps in knowledge, with 93.3% of adolescents who qualify for a substance use disorder not perceiving a need for treatment [3]. Similarly, access to treatment for those who need it is lacking. In fact, while 9.3% of adolescents were in need of substance use treatment in 2024, only 2.8% received treatment due to this knowledge gap and to limitations in access [3]. Furthermore, of those with co-occurring substance use and mental health concerns, 3 in 10 adolescents did not receive treatment for either condition, and only 25% received treatment that addressed both conditions [3]. In other words, less than one-third of adolescents in the United States with a dual diagnosis received adequate care in 2024 [3]. This gap in access, though significant in all populations, disproportionately impacts adolescents from traditionally underrepresented and underserved backgrounds [22,23,24,25], who are also often at higher risk due to environmental factors including resource scarcity [26,27]. While treatments that center sociocultural factors have been created and have shown promise [21], it remains unclear if these treatments are serving adolescents across diverse sociocultural groups and if there are ways to improve prevention and intervention efforts based on individual sociocultural and diagnostic needs.
One way to begin filling this gap is to leverage person-centered approaches to better understand the unique treatment risks, needs, and outcomes of different groups. Latent class analysis (LCA) is one such approach that identifies unique subgroups driven by data [28]. Although other clustering methods exist, LCA has emerged as a preferable method as it allows for the data-driven classification of unobserved subpopulation groupings based on both categorical and continuous variables [28]. Indeed, latent class analysis (LCA) has been applied widely to identify distinct subgroups and investigate the ways in which these subgroups predict outcomes [29]. Research has leveraged LCA to elucidate risk and resilience related to substance misuse in adolescents attending primary care visits [30] and seeking mental health treatment [31], with findings identifying older adolescents and those who have poorer physical and mental health to be at a greater risk of substance misuse and polysubstance use. However, the current literature centers a preventative lens, not yet expanding to better understand the unique presentations and needs within a treatment seeking population to improve and tailor intervention techniques. This next step in research not only serves to advance future research efforts but can also be utilized in clinical conceptualization and treatment alongside the American Society of Addiction Medicine (ASAM) criteria which allows for person-centered treatment matching based on an individual’s risk and relapse potential [32]. Furthermore, implications of adolescent sociocultural and mental health factors on substance use, treatment engagement, and treatment outcomes have yet to be explored, an important next step in understanding unique risk factors and utilizing these factors to inform targeted prevention and treatment.
To address this gap, the current study employs LCA to identify subgroups of adolescents in treatment for combined substance misuse and mental health concerns based on sociocultural and diagnostic factors. Specifically, insurance coverage, area deprivation (a calculation used to assess the social deprivation of an individual’s geographic area [33]), race, ethnicity, age, gender, court involvement, and primary mental health diagnoses will inform the data-driven classes which then can be used to predict substance misuse, treatment engagement, outcomes, and future treatment utilization. The primary purpose of the proposed LCA is to investigate the interplay between unique risk factors and thus encourage a person-centered approach to clinical conceptualization and care. As LCA is designed to be exploratory in nature and a person-centered analysis like the one presented here has not been conducted prior, we do not have specific hypotheses regarding the characteristics of defined groups or their outcomes. However, given the documented impact of sociocultural risk factors on treatment engagement [22,23,24,25], we would expect classes with higher sociocultural risk will display less treatment engagement overall.
2. Materials and Methods
Denver Health is Colorado’s safety-net healthcare system that serves almost 300,000 patients annually, of which almost 8% have a substance use disorder (SUD) [34]. We conducted a latent class analysis (LCA) to define subgroups of adolescents enrolled in Denver Health’s Substance Abuse Treatment, Education, and Prevention (STEP) program. STEP is an outpatient behavioral health and substance treatment program that specifically works with adolescent patients, offering a variety of treatment options for adolescents seeking combined mental health and substance use treatment. STEP provides traditional outpatient therapy, an intensive outpatient program (IOP), psychiatric medication management, and medication assisted treatment to those with an opioid use disorder [35]. As a component of the state safety-net healthcare system, the majority of patients seen at STEP are on Medicaid or uninsured [36]. Adolescents in STEP with elevated risk factors may also utilize Denver Health’s other services including the inpatient psychiatric hospital, pediatric emergency department, and inpatient withdrawal management program which provides medication management and inpatient psychotherapy to adolescents in need of support during substance withdrawal and at high risk of relapse [34,35].
Data for the current study were extracted using a retrospective chart review and was approved for exemption by the Colorado Multiple Institutional Review Board. All STEP patients aged 12–19 years who completed an intake assessment between 11 April 2016 (when the electronic health record (EHR) was first launched at Denver Health) and 31 July 2025, were eligible for inclusion in the current study. The patient-level cohort was extracted using Python v3.9 (Python Software Foundation, Beaverton, OR, USA) from the EHR. A total of 1292 adolescents had an intake at STEP within our timeframe. Due to the utilized time range, seasonality tests were conducted based on intake data. These analyses illustrated predictable intake fluctuations yearly, suggesting intake date would not significantly affect outcomes.
Following the initial data extraction, eight categorical indicators were selected and dichotomized into one of two categories prior to identifying latent classes: race (non-White, White), ethnicity (non-Hispanic, Hispanic), age group (<16 years, ≥16 years), insurance type (public, private), gender (cisgender boy, cisgender girl), area deprivation index (ADI; low/moderate, high), court involvement at intake (yes, no), and any mental health diagnosis at intake (yes, no). The non-White group included adolescents identifying as Black, Asian, American Indian or Alaska Native, and/or Pacific Islander. Court involvement at intake was defined as patients who were referred to STEP from law enforcement. ADI is a patient-level calculation using metrics such as income, education, housing availability, and employment. The ADI state decile rank places the least disadvantaged patients at a score of 1 and the most disadvantaged patients at a score of 10. High ADI was defined as a state decile rank greater than 7, with low/moderate defined as a rank less than or equal to 7. Given the number of covariates included in the model, variables were dichotomized to simplify model interpretation. Patients with other or unknown responses for any indicator were excluded from the LCA due to small counts. Similarly, those with missing indicator data were excluded from the latent class analysis and subsequent analyses to ensure model accuracy. Collapsing subgroups that comprise less than 10% of the sample is a common practice in LCA modeling and promotes higher model parsimony [28]. However, although dichotomization and small subsample exclusion allowed for ease of interpretation and larger subsamples, this approach also introduces bias, which could impact class differentiation and generalizability. This exclusion resulted in a total sample of 1148 adolescents. All variables except for ADI were measured at the time of the patient’s intake. Outcomes of interest included measurements of treatment engagement, hospital service utilization, substance use disorder (SUD) diagnoses, and urine drug screen (UDS) results. Treatment engagement outcomes included percent of STEP sessions attended, percent of STEP sessions missed, number of intensive outpatient program (IOP) sessions attended, average days between attended sessions, and number of gaps ≥ 30 days between sessions. Hospital service utilization outcomes included number of emergency department (ED) visits, number of inpatient hospitalizations, and any withdrawal management visits after intake. SUD outcomes included alcohol use disorder (AUD) diagnoses at intake, opioid use disorder (OUD) diagnoses at intake, cannabis use diagnoses at intake, and whether multiple SUD diagnoses were present at intake. A SUD diagnosis was determined by the presence of an F1* ICD-10-CM code at patient intake (e.g., F10 codes for AUD, F11 codes for OUD, etc.). Stimulant use disorder (SUD) was not used as an explicit outcome due to the low prevalence of stimulant use ICD-10 codes (F15) for this population. UDS outcomes only include UDSs collected in the STEP clinic which are collected weekly for each adolescent regardless of referral source (e.g., court referral). UDS outcomes included percent of negative UDSs overall and percent of negative UDSs for the primary substance. Primary substance for UDS results was determined based on whether a substance diagnosis was the primary diagnosis on the patient’s intake. All outcomes were measured after the initial STEP intake, except for SUD diagnoses, which were recorded at intake. Counts of sessions attended, sessions missed, and UDS outcomes were considered, but proportions were ultimately chosen to adjust for differences in treatment plans and testing frequency across our cohort. Listwise deletion was utilized in cases of missing outcomes data which resulted in n = 819 for UDS outcomes analyses and n = 704 for UDS primary substance analyses. No other outcomes data was missing.
Latent class modeling and subsequent analyses were performed in RStudio v4.5.1 (Posit Software, PBC, Boston, MA, USA) using poLCA v1.6.0.1, tidyverse v2.0.0, dplyr v1.1.4, tidyr v1.3.1, purrr v1.1.0, psych v2.5.6, emmeans v1.11.2, rcompanion v2.5.0, and ggplot2 v.3.5.2. Although a specific BCH method [37] package is not available in RStudio, a random seed was set before generating models to keep model and class designations consistent for predicting outcomes. Participants were assigned to classes based on their highest posterior probability of membership. Continuous outcomes were analyzed using one-way analysis of variance (ANOVA) and across classes with Tukey’s Honestly Significant Difference (HSD) tests applied to significant outcomes for pairwise comparisons. p-values of continuous outcomes were subject to a false discovery rate correction to control for false positives across multiple statistical tests. Binary outcomes were analyzed using logistic regression with likelihood ratio tests for overall class differences, followed by pairwise comparisons of estimated marginal means (EMMs) with Tukey adjustment. Statistical significance was set at α = 0.05 for all tests.
3. Results
The majority of our sample identified as White (71%), followed by Black (13%), Other (11%), Asian (1.5%), American Indian or Alaska Native (1.5%), or Other Pacific Islander (0.1%); almost 3% were missing data for their race. Nearly half of participants (46%) identified as Hispanic, with 52% identifying as non-Hispanic and around 2% missing data for their ethnicity. Around two-thirds of participants self-identified as boys (64%), followed by girls (33%), with the remainder identifying as transgender girls (0.9%), non-binary (0.8%), transgender boys (0.7%), gender fluid (0.4%), other (0.3%), or agender (0.1%). Participants’ ages ranged from 12 to 19 years, with a mean age of 15.8 years. Most participants had Medicaid insurance (65%) at their intake, followed by commercial insurance (32%), with other insurance types comprising less than 2% of the sample. Half (50%) had a documented mental health diagnosis at intake, and 7% were referred to STEP through law enforcement. The mean state decile rank for area deprivation index was 5.2, indicating a moderate level of neighborhood disadvantage within the cohort. See Table 1 for the full distribution of demographic variables pre-dichotomization.

Table 1.
Descriptive Statistics of Study Cohort (n = 1292).
Prior to conducting the LCA, we investigated descriptive statistics and bivariate correlations of the LCA indicators (See Figure 1). Associations between demographic, clinical, and socioeconomic variables were generally small, with a few exceptions. Ethnicity showed the strongest associations, being moderately related to insurance type (ϕ = 0.363) and ADI (ϕ = 0.209). Insurance type was also moderately associated with ADI (ϕ = 0.225) and race (ϕ = 0.206). Likelihood ratio tests of bivariate residual associations indicated strong associations between ethnicity and insurance (p < 0.001), ethnicity and ADI (p < 0.001), and race and insurance (p < 0.001). Moderate associations were found between gender and mental health diagnosis (p = 0.002) and race and mental health diagnosis (p = 0.013). Other variables showed little or no residual dependence.
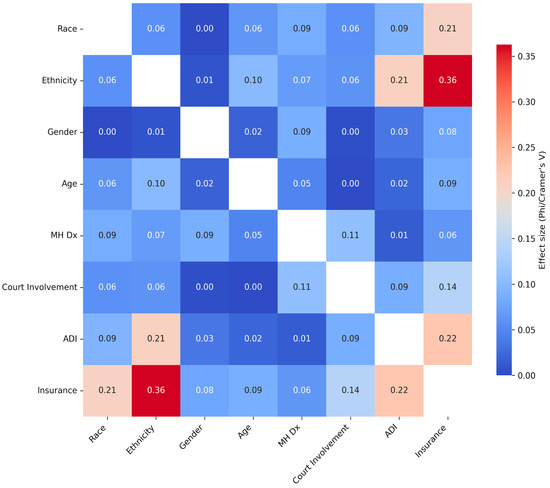
Figure 1.
Bivariate Correlation Heatmap of Indicator Variables (n = 1148). Notes. The figure shows bivariate associations in a heatmap between all of our indicator variables in this study. Variables in orange or red are more closely associated with each other, and variables in blue are not very associated with each other. ADI = Area Deprivation Index.
LCA models with 1–7 classes were defined using maximum likelihood estimation with multiple random starts (n = 5), a maximum of 1000 iterations, and a convergence tolerance of 1 × 10−10. Model fit was assessed using Akaike Information Criterion (AIC), Bayesian Information Criterion (BIC), entropy, log-likelihood, and minimum class size. Final model selection was based on a combination of statistical fit, interpretability, and clinical relevance. Both the 5-class and 6-class models demonstrated favorable fit statistics; however, the 6-class model showed evidence of overfitting, with one class comprising only 6% of the sample and lacking clinically distinct characteristics. Slightly higher average posterior probabilities for the six-class model (range 0.65–0.97) compared to the five-class model (range 0.56–0.88), and the higher entropy score of the 6-class model were considered. However, given that entropy score should not be used as the sole criterion for model selection [28], the more favorable AIC and BIC of the 5-class model and the lack of clinical significance of the additional produced class in the 6-class model outweighed the higher entropy score of the 6-class model (see Table 2 for model fit statistics). As a test of robustness, we replicated these analyses with non-dichotomized variables. The resulting 5-class model demonstrated a highly similar pattern of class characteristics, with the exception of the ADI variable which illustrated a broader distribution. Given the consistency in results overall, we retained the dichotomized models for ease of interpretation and parsimony.
Table 2.
Fit Statistics for All Tested Models.
The key characteristics from each class in the 5-class model are presented below followed by a descriptive class label (see Figure 2 for class characteristic visualization). The most defining features for classes appeared between ADI ranking, ethnicity, race, and mental health diagnoses.
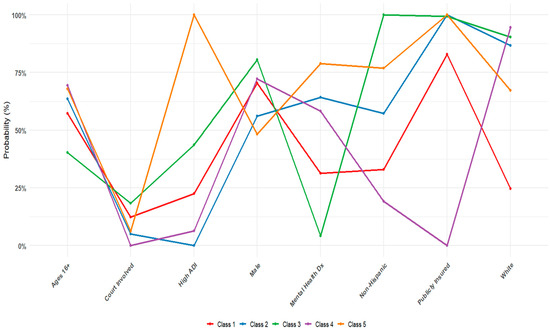
Figure 2.
Latent Class Profile Plot of Indicators in 5-Class Model. Notes. Figure 2 illustrates the probabilities of endorsement for each class. Class 1 = Moderate access, low MH needs; Class 2 = Moderate access, high MH needs; Class 3 = Low access, court-involved; Class 4 = High access, sociocultural privilege; Class 5 = Low access, high MH needs; Error bars were inestimable due to within-class homogeneity.
Class 1: Adolescents presenting with moderate structural access and low mental health (MH) needs accounted for 23% of the sample. This class was predominantly non-White, non-Hispanic, and male, with most holding public insurance and most not having a mental health diagnosis.
Class 2: Adolescents presenting with moderate structural access and high MH needs accounted for 27% of the sample. This class was largely White, Hispanic, with public insurance, all low/moderate ADI rankings, and a high prevalence of mental health diagnoses.
Class 3: Adolescents with low structural access and court-involved accounted for 11% of the sample. This class was almost all White, Hispanic, male, younger than 16, publicly insured, with high ADI rankings, high court involvement, and very low prevalence of mental health.
Class 4: Those with high access and sociocultural privilege accounted for 29% of the sample and was predominantly White, non-Hispanic, and privately insured, with mostly low/moderate ADI rankings and no court involvement.
Class 5: Finally, adolescents with low structural access and high MH needs accounted for 10% of the sample. This class was primarily non-Hispanic, female, and publicly insured, with high ADI rankings, and a high prevalence of mental health diagnoses.
Once the classes were estimated, we examined descriptive statistics and bivariate correlations of the classes and included outcomes (see Figure 3). Diagnostic checks indicated that several indicators (e.g., Court Involvement, Race, Insurance, and Ethnicity) were completely homogeneous within a class, rendering standard errors inestimable. Among outcomes, the strongest associations were observed between treatment engagement measures. The percent of sessions attended had a perfect negative correlation with sessions missed (r = −1.00). This was to be expected, since sessions can only be either attended or missed. In terms of clinical outcomes, the percentage of negative urine drug screens was strongly associated with the percentage of primary SUD-negative tests (r = 0.75). Substance use disorder indicators were also interrelated. Alcohol use disorder (AUD) was strongly associated with polysubstance use disorder (r = 0.55), and opioid use disorder (OUD) was moderately correlated with polysubstance use disorder (r = 0.27) and cannabis use (r = 0.29). Other variables showed little or no residual dependence.
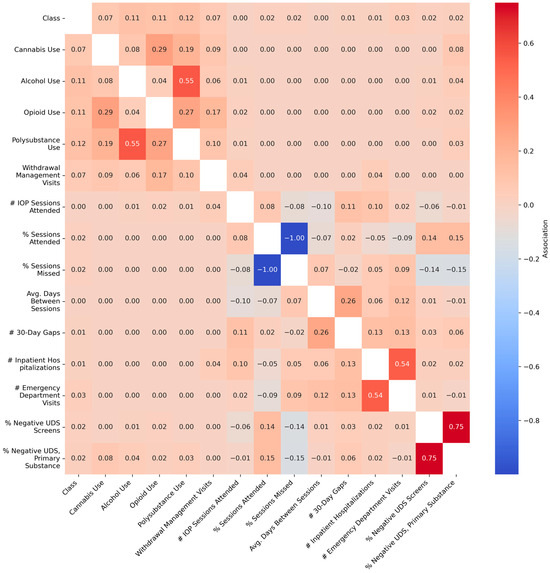
Figure 3.
Bivariate Correlation Heatmap of Class and Outcome Variables (n = 1148). Notes. Figure 3 shows bivariate associations in a heatmap figure between our class groupings and outcome variables in this study. Variables in orange or red are more closely associated with each other, and variables in blue are not very associated with each other. # = variable coded using counts. % = variable is a percentage. UDS = Urine Drug Screen.
Finally, the groups were held constant utilizing the random seed set prior to class estimation and utilized to estimate the intended outcomes. Group differences were observed for several outcomes (Table 3). Among continuous outcomes, significant effects were seen in emergency department visits (p < 0.001, η2 = 0.03), percent of sessions attended (p = 0.002, η2 = 0.02), percent of sessions missed (p = 0.002, η2 = 0.02), percent of negative urine drug screens (p = 0.014, η2 = 0.02), and percent of negative urine drug screens for the primary substance (p = 0.028, η2 = 0.02). Counts of urine drug screens were analyzed as a test of robustness and produced similar significance results. No significant group differences were found for treatment engagement measures (number of IOP sessions attended, average days between sessions, 30-day gaps), inpatient hospitalizations, or withdrawal management visits. For categorical outcomes, significant associations were seen in opioid use disorder diagnoses (p = 0.018, η2 = 0.02), alcohol use disorder diagnoses (p = 0.004, η2 = 0.02), and multiple substance diagnoses (p = 0.005, η2 = 0.02). Cannabis use diagnoses and withdrawal management visits were not significantly different across groups. Effect sizes for all significant findings were small (η2 = 0.02–0.03).
Table 3.
Analysis of Variance (ANOVA) Results for Continuous Outcomes and Logistic Regression Results for Categorical Outcomes (n = 1148).
Post hoc comparisons of significant outcomes revealed several meaningful differences between classes (Table 4). For treatment engagement, Class 4 (high access, sociocultural privilege) attended more sessions than Class 1 (moderate access, low MH; mean difference = 0.07, p < 0.001) and Class 2 (moderate access, high MH needs; mean difference = 0.04, p < 0.04), as well as missed more sessions than Class 1 (mean difference = −0.07, p < 0.001) and Class 2 (mean difference = −0.04, p < 0.04). For emergency department utilization, Class 4 (high access, sociocultural privilege) had fewer visits than Class 2 (moderate access, high MH needs; mean difference = −1.12, p < 0.001), while Class 5 (low access, high MH needs) had more visits than Class 4 (mean difference = 1.42, p < 0.001). These differences represent moderate effects in terms of emergency department utilization. Regarding substance misuse outcomes, Class 4 demonstrated better urine drug screen results, with a higher number of negative screens overall compared to Class 3 (low access, court-involved; mean difference = 3.15, p = 0.012), a higher percentage of negative screens overall compared to Class 3 (mean difference = 0.17, p = 0.008) and a higher percentage of negative screens for the primary substance (mean difference = 0.17, p = 0.019), all reflecting small-to-moderate improvements. For substance diagnosis outcomes, Class 4 had lower odds of an opioid use disorder diagnosis relative to Class 5 (OR = 0.40, p = 0.011), indicating a 60% reduction in odds. Class 1 (moderate access, low MH needs) had reduced odds of an alcohol use disorder diagnosis (OR = 0.49, p = 0.007) and lower odds of multiple substance diagnoses (OR = 0.57, p = 0.019) compared to Class 4, reflecting small-to-moderate effect sizes.
Table 4.
Post Hoc Tests.
4. Discussion
The well-documented challenges in combined treatment for mental health and substance misuse [3,22,23,24,25], including limited knowledge and utilization, difficulties with service access, and discrepancies in care across the most at-risk populations, call for research to elucidate factors perpetuating these challenges. Identifying unique sociocultural factors impacting substance use, treatment, and outcomes is an important first step. To continue advancing research in this area toward informed prevention and intervention efforts, the current study aimed to leverage a person-centered approach to improve understanding of the way sociocultural risk factors and mental health diagnosis co-occur and lead to differences in substance misuse, treatment engagement, and future treatment utilization in adolescents in combined treatment.
The utilized LCA produced five distinct classes that hold clinical and research relevance. Where classes 1, 2, 3, and 5 represented groups of adolescents with high sociocultural risk factors overall, class 4 displayed more sociocultural advantage. Furthermore, despite higher risk across classes 1, 2, 3, and 5, the specifics of these adolescents’ risk factors differed. For example, class 1 was made up of primarily older, non-White boys, from a range of SES backgrounds with high court involvement, whereas class 5 mainly represented older, White girls from low SES backgrounds with mental health diagnoses. These groups, on their own, have clinical utility in terms of serving as a guidepost for clinical conceptualization and resource referrals. To clarify, the identified classes should not dictate clinical judgment but instead can serve to aid clinicians in gathering relevant sociocultural information about their patients and attending to these sociocultural needs. Furthermore, the distinction of the five classes broadly suggests area deprivation as a significant risk factor that should be considered more strongly in clinical work and research. Relatedly, the classes highlight the inherent biases in court involvement. Specifically, the two groups primarily represented by non-White or Hispanic boys with high socioeconomic risk factors also had higher court involvement and lower mental health diagnoses as compared to the other classes. These two classes also displayed worse substance treatment outcomes. It is well known that youth of color are disproportionately represented in the juvenile justice system [38,39] and are less likely to receive an appropriate mental health diagnosis and treatment [40]. These more generalized findings, along with past research that illustrates the prevalence and impact of these disparities [22,23,24,25,26,27], call for systems-level change to (1) address resource scarcity, (2) improve access to treatment, and (3) dismantle the biases that exist within the juvenile justice system.
Differences between the identified classes, while modest and exploratory, were further illustrated when investigating related substance misuse, treatment engagement, and outcomes. First, and notably, no differences in treatment engagement were found between classes. Although unexpected based on past research more generally [22,23,24,25,26,27], research conducted in the STEP clinic specifically has illustrated similar findings [21] such that typical discrepancies in engagement are reduced. Work from our team suggests that the lack of discrepancies observed in the STEP intensive outpatient program (IOP) specifically may be a result of reduced barriers through transportation assistance, contingency management, and meal incentives [21]. The findings from this study may suggest the benefits of barrier reduction techniques seen in STEP IOP extend to the entire clinic, making for meaningful additions to other mental health and substance use clinics. However, additional research is needed to better understand what specific factors are improving treatment engagement in our clinic as compared to other adolescent substance use treatment centers.
We also did not see any significant differences between the higher-risk classes (1, 2, 3, and 5), suggesting that, at least regarding the outcomes we assessed, those in the higher risk classes may be at similar risk. However, when compared to the high access, sociocultural privilege class (class 4), potentially important distinctions emerged. Specifically, the two classes that presented with moderate to low SES and high MH concerns (classes 2 and 5) were significantly more likely to visit the emergency department (ED) than the high access, sociocultural privilege class (class 4). There are many potential reasons for this increased ED utilization. One possibility is that this utilization is being driven by health inequities. Recent research investigating the increased utilization of EDs has found that youth of color and those with public insurance are more likely to be referred to EDs for care, and further, are unlikely to receive behavioral healthcare specifically during their ED visit [41]. Therefore, it is necessary for physical and mental healthcare workers to engage in development of standards and systems, quality improvement, and research and evaluation to effectively improve healthcare and decrease these inequities [41]. Another possible contributor is that mental health concerns can result in higher ED utilization due to the documented comorbidities with substance misuse, suicidality, somatic symptomatology, etc. [42]. Although no significant differences in substance misuse emerged between adolescents with moderate access and high MH needs (class 2) and those with high access and sociocultural privilege (class 4), such a difference did emerge between adolescents with low access and high MH needs (class 5) and the high access, sociocultural privilege class (class 4) such that those in the low SES, high MH class were 60% more likely to have an OUD diagnosis at intake. Therefore, the increased ED utilization of adolescents with low access and high MH needs (class 5) specifically may be driven, in part, by substance misuse and associated concerns including intoxication, overdose, and withdrawal. Finally, as these two groups (classes 2 and 5) represent adolescents with low to moderate SES, access to primary care and outpatient settings may be more limited than other groups, resulting in this increased ED utilization. While our results should be considered preliminary and replicated in additional samples, efforts to increase access and dismantle existing barriers to primary care and mental healthcare alike seem warranted.
Compared to the sociocultural advantaged class (class 4), the low access, court-involved class (class 3) had significantly worse UDS outcomes. Substance misuse in early adolescence is particularly challenging due to the state of brain maturation and is related to increased risk of dependence and lifetime use [43]. This may contribute to increased difficulty in attaining negative UDS results and would suggest that earlier intervention and higher levels of care may be appropriate. Alternatively, it may be that the treatment goals of adolescents with low access and court involvement are different than those of the sociocultural advantaged group. The treatment options at STEP are designed to be non-punitive with a harm reduction focus. Therefore, negative UDSs are not a requirement of treatment. Instead, adolescents are encouraged to make their own treatment goals with their therapist that may or may not include abstinence. In either case, increased attention to younger adolescents’ thoughts and goals around substance use treatment, especially those with court involvement, is clinically indicated.
Although the class of adolescents with high access and sociocultural privilege (class 4) had the best treatment outcomes, they simultaneously had higher odds of an Alcohol Use Disorder (AUD) and of polysubstance use compared to the moderate access, low MH needs class (class 1) specifically. This finding may have emerged due to the increased pressure and monitoring put on class 1 because of their court involvement. Often, court-involved adolescents in our clinic are required to complete UDSs with their probation officers in addition to those completed as a component of treatment. Therefore, in this case, court involvement may be a confounding factor. Additionally, the increased odds of AUD and polysubstance use in class 4 specifically may be due to higher rates of comorbid alcohol and cannabis use, which is unfortunately becoming more common in adolescence [44]. While these increased odds do not seem to be impacting treatment outcomes for these youths, it may be that there are other deleterious outcomes that were not included in this study. For example, alcohol use is associated with neurological changes [45] and high risk of subsequent and risky use [46] as well as alcohol-related harm [47,48]. Thus, future research investigating AUD and polysubstance use in adolescents with high access and sociocultural privilege is warranted. Precipitating factors related to AUD and polysubstance use in this population as well as long-term treatment and health outcomes should be investigated with a focus on informing clinical care for these adolescents.
Taken together, while the results of this study should be considered preliminary and continued research should replicate and expand these findings, our results begin highlighting ways to provide tailored support to adolescents presenting with specific risk factors. For example, based on the ED utilization of adolescents with low to moderate access and high MH needs, it may be clinically indicated to provide additional support to these adolescents throughout treatment, engage in interdisciplinary care across mental and physical health, elongate step-down care post treatment, and to provide additional resources to families regarding co-occurring mental health and substance misuse. Similarly, developmentally appropriate discussions regarding substance use treatment goals and applied motivational interviewing with adolescents with low access and court-involved may benefit their treatment journey and reduce dependence and long-term use. Finally, adolescents presenting with sociocultural advantage compared to their peers are not without their own risks. As we utilized a treatment sample, the inherent risk in all adolescents included in this study should not be understated. Furthermore, it seems as though adolescents in this sociocultural advantaged group may be at higher risk of AUD and polysubstance use. Thus, particular attention to the adolescent’s purpose of polysubstance use, psychoeducation on the risks of combining substances, and targeted treatment for alcohol use specifically may be beneficial for some patients.
The current study is the first to examine the implications of adolescent sociocultural and mental health factors on substance use, treatment engagement, and treatment outcomes in an adolescent sample of treatment seeking adolescents. Our findings provide meaningful insights into how specific risk factors seem to co-occur within our treatment population and the impact this has on substance misuse and treatment outcomes. This study has many strengths including a large clinical sample, integration of sociocultural and mental health risk factors, and the utilization of a person-centered approach, and should be seen as the first step toward understanding individual differences in substance misuse, treatment engagement, and outcomes.
As with all research, our study is not without limitations, which should be considered in interpretation and addressed in future research. First, it is unclear which risk factors within each class influence each other or if there are other confounding factors impacting our results, making it difficult to identify specific targets. As we collected data through retrospective chart review, we were unable to collect some potentially meaningful demographic and outcome data, such as family composition, individual SES, and progress toward therapeutic goals. These are important variables that should be considered in future research. Relatedly, given that the sociocultural factors, mental health diagnoses, and substance use diagnoses were taken from the same timepoint, we are unable to identify directionality or causality. Thus, research in similar populations should consider potential confounds and investigate other, clinically relevant applications of LCA and alternative models longitudinally. Given our sample size and the number of observed variables included in the LCA, we excluded small subgroups and dichotomized included variables introducing bias that should be accounted for in future research. Although our replication analyses utilizing non-dichotomized data produced comparable results, this area of research would benefit from additional studies investigating the nuances of class membership. In particular, future research should consider the broad distribution of ADI and how this impacts class membership and outcomes. This continued research serves to increase support for our findings and expand generalizability. As our sample is a treatment seeking clinical sample at a safety-net hospital, the classes presented herein may not generalize to non-clinical samples or more affluent populations, making replication studies in diverse populations an important next step. Our significant results should also be interpreted as exploratory and need to be replicated in future work. This is the first study to investigate the overlap of sociocultural and mental health factors in a combined treatment seeking population and our effect sizes for significant results are small. Thus, additional research should be conducted to bolster these findings and clarify the practical significance of our identified classes. Finally, as the data from this study was gathered from a retrospective chart review, there are many indicators and outcomes that may hold clinical significance that we were unable to include. For example, gaining additional information about household SES may help to clarify the classes and testing additional outcomes such as adolescent reported progress and routine outcomes monitoring may highlight additional ways to target treatment and resource referrals. Additionally, future research would benefit from taking a similar approach with continuous variables (e.g., latent profile analysis). Specifically, an adolescent’s external (e.g., social support) and internal (e.g., resilience) strengths may impact and buffer substance misuse, treatment engagement, and outcomes, which should be investigated in future work.
5. Conclusions
Overall, our results identified five unique subgroups of adolescents in combined mental health and substance use treatment that may have clinical and research applications and should continue to be investigated in future research. Specifically, no class was completely protected. Where classes of youth presenting with increased sociocultural risk factors (classes 1, 2, 3, and 5) displayed less treatment engagement, more future service utilization, and poorer outcomes, adolescents with high access and sociocultural privilege had significantly higher rates of AUD and polysubstance use. This illustrates the need for tailored treatment, recognizing the unique needs of specific patients and adjusting care to address those needs. Importantly, the classes are not intended to define adolescents, but instead to encourage clinicians to take a person-centered approach to conceptualization and care, providing additional support and referrals where appropriate. In addition to highlighting unique risk factors for specific subgroups, our results also broadly suggest area deprivation as a significant risk factor and illuminate the inherent biases in court involvement that need to be addressed. Thus, in addition to this work being utilized to inform clinical work and future research, it also calls for systems-level change to promote equity in access, engagement, and outcomes related to adolescent substance treatment.
Author Contributions
Conceptualization, H.D.S., E.C. and E.W.; methodology, H.D.S., L.S. and R.L.; software, L.S.; validation, L.S.; formal analysis, L.S.; investigation, H.D.S. and L.S.; resources, H.D.S.; data curation, L.S.; writing—original draft preparation, H.D.S. and L.S.; writing—review and editing, H.D.S., L.S., E.W., E.C., K.H., R.L. and C.T.; visualization, L.S.; supervision, R.L. and C.T.; project administration, H.D.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved for exemption by the Institutional Review Board of Colorado Multiple Institutional Review Board (protocol code: 25-1475; date of approval: 18 August 2025) as a secondary research study.
Informed Consent Statement
Patient consent was waived due to the data being collected as part of routine clinical care and outcome monitoring. Adolescents consented to their own treatment.
Data Availability Statement
The data and the codes can be accessed by emailing the corresponding author.
Acknowledgments
We would like to acknowledge everyone who has made this research possible, including the incredible clinical team that took their time to aid with data collection and all who took their time to share their thoughts and experiences.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- World Health Organization. Adolescent Health. 2025. Available online: https://www.who.int/health-topics/adolescent-health#tab=tab_1\ (accessed on 20 August 2025).
- Layman, H.M.; Thorisdottir, I.E.; Halldorsdottir, T.; Sigfusdottir, I.D.; Allegrante, J.P.; Kristjansson, A.L. Substance Use Among Youth During the COVID-19 Pandemic: A Systematic Review. Curr. Psychiatry Rep. 2022, 24, 307–324. [Google Scholar] [CrossRef]
- Substance Abuse and Mental Health Services Administration. Key Substance Use and Mental Health Indicators in the United States: Results from the 2024 National Survey on Drug Use and Health (HHS Publication No. PEP25-07-007, NSDUH Series H-60). Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration. 2025. Available online: https://www.samhsa.gov/data/sites/default/files/reports/rpt56287/2024-nsduh-annual-national-report.pdf (accessed on 21 August 2025).
- Centers for Disease Control and Prevention. Youth Risk Behavior Survey Data Summary & Trends Report: 2013–2023; U.S. Department of Health and Human Services: Washington, DC, USA, 2024. [Google Scholar]
- Yonek, J.C.; Dauria, E.F.; Kemp, K.; Koinis-Mitchell, D.; Marshall, B.D.L.; Tolou-Shams, M. Factors Associated With Use of Mental Health and Substance Use Treatment Services by Justice-Involved Youths. Psychiatr. Serv. 2019, 70, 586–595. [Google Scholar] [CrossRef]
- Simon, K.M.; Levy, S.J.; Bukstein, O.G. Adolescent Substance Use Disorders. NEJM Evid. 2022, 1, EVIDra2200051. [Google Scholar] [CrossRef]
- Tervo-Clemmens, B.; Gilman, J.M.; Evins, A.E.; Bentley, K.H.; Nock, M.K.; Smoller, J.W.; Schuster, R.M. Substance Use, Suicidal Thoughts, and Psychiatric Comorbidities Among High School Students. JAMA Pediatr. 2024, 178, 310–313. [Google Scholar] [CrossRef] [PubMed]
- McCabe, S.E.; Schulenberg, J.E.; Schepis, T.S.; McCabe, V.V.; Veliz, P.T. Longitudinal Analysis of Substance Use Disorder Symptom Severity at Age 18 Years and Substance Use Disorder in Adulthood. JAMA Netw. Open 2022, 5, e225324. [Google Scholar] [CrossRef] [PubMed]
- Thurstone, C.; Etzig, C.; Chen, E.; Seely, H.D.; Loh, R. Mortality following adolescent substance treatment: 21-year follow-up from a single clinical site. Front. Child Adolesc. Psychiatry 2025, 4, 1600101. [Google Scholar] [CrossRef]
- Petrosty, E.; Ertl, A.; Sheats, K.J.; Wilson, R.; Betz, C.J.; Blair, J.M. Surveillance for violent deaths—National Violent Death Reporting System, 34 states, four California counties, the District of Columbia, and Puerto Rico, 2017. MMWR Surveill. Summ. 2020, 69, 1–37. [Google Scholar] [CrossRef]
- Goldstick, J.E.; Cunningham, R.M.; Carter, P.M. Current Causes of Death in Children and Adolescents in the United States. N. Engl. J. Med. 2022, 386, 1955–1956. [Google Scholar] [CrossRef] [PubMed]
- Friedman, J.; Hadland, S.E. The Overdose Crisis among U.S. Adolescents. N. Engl. J. Med. 2024, 390, 97–100. [Google Scholar] [CrossRef]
- Deas, D.; Brown, E.S. Adolescent substance abuse and psychiatric comorbidities. J. Clin. Psychiatry 2006, 67, e02. [Google Scholar] [CrossRef]
- Auerbach, R.P.; Tsai, B.; Abela, J.R.Z. Temporal relationships among depressive symptoms, risky behavior engagement, perceived control, and gender in a sample of adolescents. J. Res. Adolesc. 2010, 20, 726–747. [Google Scholar] [CrossRef]
- Ogundele, M.O. Behavioural and emotional disorders in childhood: A brief overview for paediatricians. World J. Clin. Pediatr. 2018, 7, 9–26. [Google Scholar] [CrossRef] [PubMed]
- Verboom, C.E.; Sijtsema, J.J.; Verhulst, F.C.; Penninx, B.W.; Ormel, J. Longitudinal associations between depressive problems, academic performance, and social functioning in adolescent boys and girls. Dev. Psychol. 2014, 50, 247–257. [Google Scholar] [CrossRef]
- Rowe, C.L.; Liddle, H.A.; Greenbaum, P.E.; Henderson, C.E. Impact of psychiatric comorbidity on treatment of adolescent drug abusers. J. Subst. Abus. Treat. 2004, 26, 129–140. [Google Scholar] [CrossRef] [PubMed]
- Trautmann, S.; Rehm, J.; Wittchen, H. The economic costs of mental disorders. EMBO Rep. 2016, 17, 1245–1249. [Google Scholar] [CrossRef]
- Fischer, N.R. School-based harm reduction with adolescents: A pilot study. Subst. Abus. Treat. Prev. Policy 2022, 17, 79. [Google Scholar] [CrossRef]
- Meredith, L.R.; Maralit, A.M.; Thomas, S.E.; Rivers, S.L.; Salazar, C.A.; Anton, R.F.; Tomko, R.L.; Squeglia, L.M. Piloting of the Just Say Know prevention program: A psychoeducational approach to translating the neuroscience of addiction to youth. Am. J. Drug Alcohol Abus. 2020, 47, 16–25. [Google Scholar] [CrossRef]
- Chen, E.; Seely, H.D.; Thurstone, C. Reducing barriers to promote engagement and retention in adolescent substance use treatment: Results from a quality improvement evaluation. Front. Child Adolesc. Psychiatry 2024, 3, 1393401. [Google Scholar] [CrossRef]
- Pössel, P.; Seely, H.D.; Marchetti, I. Similarities and Differences in the Architecture of Cognitive Vulnerability to Depressive Symptoms in Black and White American Adolescents: A Network Analysis Study. Res. Child Adolesc. Psychopathol. 2024, 52, 1591–1605. [Google Scholar] [CrossRef]
- Seely, H.D.; Pössel, P. Equity and inclusion in prevention: Is prevention efficacious in diverse groups? J. Consult. Clin. Psychol. 2024, 93, 307–316. [Google Scholar] [CrossRef]
- Acevedo, A.; Harvey, N.; Kamanu, M.; Tendulkar, S.; Fleary, S. Barriers, facilitators, and disparities in retention for adolescents in treatment for substance use disorders: A qualitative study with treatment providers. Subst. Abus. Treat Prev. Policy 2020, 15, 42. [Google Scholar] [CrossRef]
- Huey, S.J., Jr.; Park, A.L.; Galán, C.A.; Wang, C.X. Culturally Responsive Cognitive Behavioral Therapy for Ethnically Diverse Populations. Annu. Rev. Clin. Psychol. 2023, 19, 51–78. [Google Scholar] [CrossRef] [PubMed]
- Buttazzoni, A.; Doherty, S.; Minaker, L. How Do Urban Environments Affect Young People’s Mental Health? A Novel Conceptual Framework to Bridge Public Health, Planning, and Neurourbanism. Public Health Rep. 2022, 137, 48–61. [Google Scholar] [CrossRef]
- Schwinn, T.M.; Schinke, S.P.; Trent, D.N. Substance use among late adolescent urban youths: Mental health and gender influences. Addict. Behav. 2010, 35, 30–34. [Google Scholar] [CrossRef]
- Sinha, P.; Calfee, C.S.; Delucchi, K.L. Practitioner’s Guide to Latent Class Analysis: Methodological Considerations and Common Pitfalls. Crit. Care Med. 2021, 49, e63–e79. [Google Scholar] [CrossRef]
- Rachid, T.; Abarda, A.; Hasbaoui, A. Latent class analysis: A review and recommendations for future applications in health sciences. Procedia Comput. Sci. 2024, 238, 1062–1067. [Google Scholar] [CrossRef]
- Bohnert, K.M.; Walton, M.A.; Resko, S.; Barry, K.T.; Chermack, S.T.; Zucker, R.A.; Zimmerman, M.A.; Booth, B.M.; Blow, F.C. Latent class analysis of substance use among adolescents presenting to urban primary care clinics. Am. J. Drug Alcohol Abus. 2014, 40, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Karanges, E.A.; Guerin, A.A.; Malignaggi, S.; Purcell, R.; McGorry, P.; Hickie, I.; Yung, A.R.; Pantelis, C.; Amminger, G.P.; Van Dam, N.T.; et al. Substance use patterns among youth seeking help for mental illness: A latent class analysis. Addict. Behav. 2025, 167, 108355. [Google Scholar] [CrossRef] [PubMed]
- Mee-Lee, D. The Criteria: Treatment Criteria for Addictive, Substance-Related, and Co-Occurring ASAM Conditions, 3rd ed.; Change Companies: Carson City, NV, USA, 2013. [Google Scholar]
- Maroko, A.R.; Doan, T.M.; Arno, P.S.; Hubel, M.; Yi, S.; Viola, D. Integrating Social Determinants of Health With Treatment and Prevention: A New Tool to Assess Local Area Deprivation. Prev. Chronic Dis. 2016, 13, 160221. [Google Scholar] [CrossRef]
- Denver Health. Report to the City; Denver Health: Denver, CO, USA, 2024. [Google Scholar]
- Adolescent Substance Abuse Treatment. Available online: https://www.denverhealth.org/services/behavioral-health/addiction-services/adolescent-substance-abuse-treatment (accessed on 25 August 2025).
- Center for Addiction Medicine. Annual Report; Center for Addiction Medicine: Boston, MA, USA, 2023. [Google Scholar]
- Bolck, A.; Croon, M.A.; Hagenaars, J.A. Estimating latent structure models with categorical variables: One-step versus three-step estimators. Political Anal. 2004, 12, 3–27. [Google Scholar] [CrossRef]
- Beardslee, J.; Miltimore, S.; Fine, A.; Frick, P.J.; Steinberg, L.; Cauffman, E. Under the radar or under arrest: How is adolescent boys’ first contact with the juvenile justice system related to future offending and arrests? Law Hum. Behav. 2019, 43, 342–357. [Google Scholar] [CrossRef]
- Padgaonkar, N.T.; Baker, A.E.; Dapretto, M.; Galván, A.; Frick, P.J.; Steinberg, L.; Cauffman, E. Exploring Disproportionate Minority Contact in the Juvenile Justice System Over the Year Following First Arrest. J. Res. Adolesc. Off. J. Soc. Res. Adolesc. 2021, 31, 317–334. [Google Scholar] [CrossRef]
- Bronson, J.; Berzofsky, M. Indicators of Mental Health Problems Reported by Prisoners and Jail Inmates, 2011–2012; Bureau of Justice Statistics: Washington, DC, USA, 2017. Available online: https://bjs.ojp.gov/content/pub/pdf/imhprpji1112.pdf (accessed on 20 November 2025).
- Hoge, M.A.; Vanderploeg, J.; Paris, M., Jr.; Lang, J.M.; Olezeski, C. Emergency Department Use by Children and Youth with Mental Health Conditions: A Health Equity Agenda. Community Ment. Health J. 2022, 58, 1225–1239. [Google Scholar] [CrossRef] [PubMed]
- Santo, L.; Peters, Z.J.; Davis, D.; DeFrances, C.J. Emergency department visits related to mental health disorders among children and adolescents: United States, 2018–2021. In National Health Statistics Reports; No 191; National Center for Health Statistics: Hyattsville, MD, USA, 2023. [Google Scholar] [CrossRef]
- Jordan, C.J.; Andersen, S.L. Sensitive periods of substance abuse: Early risk for the transition to dependence. Dev. Cogn. Neurosci. 2017, 25, 29–44. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.M.; Calhoun, B.H.; Abdallah, D.A.; Blayney, J.A.; Schultz, N.R.; Brunner, M.; Patrick, M.E. Simultaneous Alcohol and Marijuana Use Among Young Adults: A Scoping Review of Prevalence, Patterns, Psychosocial Correlates, and Consequences. Alcohol Res. Curr. Rev. 2022, 42, 8. [Google Scholar] [CrossRef]
- Lees, B.; Debenham, J.; Squeglia, L.M. Alcohol and Cannabis Use and the Developing Brain. Alcohol Res. Curr. Rev. 2021, 41, 11. [Google Scholar] [CrossRef]
- Sjödin, L.; Raninen, J.; Larm, P. Early Drinking Onset and Subsequent Alcohol Use in Late Adolescence: A Longitudinal Study of Drinking Patterns. J. Adolesc. Health Off. Publ. Soc. Adolesc. Med. 2024, 74, 1225–1230. [Google Scholar] [CrossRef]
- Danpanichkul, P.; Duangsonk, K.; Díaz, L.A.; Chen, V.L.; Rangan, P.; Sukphutanan, B.; Dutta, P.; Wanichthanaolan, O.; Ramadoss, V.; Sim, B.; et al. The burden of alcohol and substance use disorders in adolescents and young adults. Drug Alcohol Depend. 2025, 266, 112495. [Google Scholar] [CrossRef]
- Danpanichkul, P.; Ng, C.H.; Tan, D.J.H.; Wijarnpreecha, K.; Huang, D.Q.; Noureddin, M.; Young Alcohol Disease Collaborative. The Global Burden of Alcohol-associated Cirrhosis and Cancer in Young and Middle-aged Adults. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2024, 22, 1947–1949.e3. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).