Abstract
Background: Child physical abuse is a significant contributor to overall pediatric mortality and morbidity and is associated with both short- and long-term effects on the physical, social and mental wellbeing of the child involved. Fractures are the second most common physical injury in children suffering from physical abuse and are present in up to 55% of cases of physically abused children. Specific fracture patterns may prompt suspicion for abuse, although none are specific. We aim to identify the incidence of fracture types associated with abuse in children under three years old presenting to the ED. Methods: This study was a retrospective descriptive study. The inclusion criteria consisted of (a) children less than three years of age, (b) presenting to the ED, (c) between 1 January 2020, and 31 December 2022, inclusive and (d) with a diagnosis consistent with a fracture type associated with abuse. Results: There were 214 patients diagnosed with fractures who were under 3 years of age. Of these, twenty-one patients fit the criteria for fracture suspcious for non-accidental injury (a rate of one per month if following a normal distribution). The diagnosis of NAI was considered in eight (38%) patients. NAI was not considered in 13 (62%) patients. A medical record review of these patients up to 12 months after initial ED presentation showed that five did not re-present to the ED, one was referred to CSS from outpatients and two re-presented within this period with minor head injuries. Conclusions: Presentations of fractures concerning NAI are rare but important not to miss. Automated systems and targeted education and action are critical to ensure that concerns for NAI are managed appropriately.
1. Introduction
Child physical abuse is a significant contributor to overall pediatric mortality and morbidity and is associated with both short- and long-term effects on the physical, social and mental wellbeing of the child involved [1]. In Australia, there is a child suffering from some form of child abuse (emotional, physical and sexual abuse or neglect) every 11 min and often perpetrated by a guardian or someone known to the child [2]. The estimated rate of violence-related deaths in Australian children is 0.8 per 100 000 [3]. Despite the absence of comprehensive national data on the prevalence of child abuse and neglect, research from 2017 to 2018 shows that approximately 26,400 Australian children (excluding New South Wales) aged 0–12 years had one or more child protection notifications substantiated [4].
Child abuse and neglect are associated with many adverse long-term outcomes such as poor academic performance, limited social skills, higher likelihood of engaging in criminal activities, poorer physical health outcomes and mental health issues [4,5]. Kezelman et al. estimated that the annual cost to Australian taxpayers resulting from unresolved childhood trauma, including child sexual, emotional and physical abuse, is at least $6.8 billion per year [5]. Pivotal research conducted by Felitti et al. explored the link between adverse childhood experiences (ACEs) throughout childhood and the major causes of mortality in adults, identifying a direct correlation between the number of ACEs a child experienced and an increased likelihood of various high-risk behaviors and health issues [6]. According to the literature, these high-risk behaviors can include a 4- to 12-fold increase in alcoholism, drug abuse, depression and suicide attempt and a 2- to 4-fold increase in smoking, poor self-rated health, engagement in sexual activities with over 50 partners and sexually transmitted disease; and a 1.4- to 1.6-fold increase in physical inactivity and severe obesity was noted [6]. A significant dose–response relationship was also identified between the number of ACEs and various physical illnesses where the more ACEs an individual had encountered, the greater their risk of developing chronic health conditions. [6] This correlation was particularly evident in cases of ischemic heart disease, cancer, chronic bronchitis or emphysema, hepatitis or jaundice and skeletal fractures [6].
Recognizing and reporting all forms of suspected child abuse are crucial for the wellbeing and safety of children [1]. Health settings are one place where children may be seen with injuries that may herald abuse [7]. Cognitive bias amongst clinicians and a failure to fully assess, document and report injuries as possible abuse have been reported in the literature as barriers to the appropriate identification and follow-up of children who present with injuries [3]. The emergency department (ED) may be the first and potentially only point whereby medical practitioners can assess a child for injuries and investigate if needed [7]. Children presenting with serious injuries (e.g., fractures), potentially sustained due to some form of abuse, are often evaluated in EDs due to the acute nature of the injury, lack of access to primary care and accessibility of EDs after hours [8]. Nearly one third of children who succumbed to abuse-related fatalities had prior interactions with healthcare professionals, often in the ED, where their injuries were not recognized as abuse [8]. Approximately 20–25% of injuries later identified as child abuse have a prior injury [9]. There is evidence demonstrating higher rates of morbidity and mortality amongst children experiencing recurring abuse [10,11,12].
Research has shown that in healthcare settings, there are missed opportunities for early identification and intervention in cases of child abuse and that there is variability in a clinician’s response to the injury once identified [10,13,14]. This variability in both clinician recognition and response may lead to overlooked instances of abuse, a lack of reporting in suspected cases and an insufficient or inappropriate assessment for further injuries in children [15].
The suspicion and recognition of child abuse has been an important area of research in the literature and public awareness over the last few decades [16]. Identifying sentinel injuries, that is, those injuries that are considered potential indicators of child abuse, is a critical aspect of responding appropriately to child abuse [11]. A retrospective secondary analysis of 30,355 children less than two years old with putative sentinel injuries demonstrated that there was a great variation in the evaluation and diagnosis of abuse across hospital and injury categories [17]. Sentinel injuries themselves are also difficult to describe and standardize given the wide variety of presentations [18]. Red flag signs during history and/or physical examination have been proposed by the American Academy of Pediatrics (Table 1) to guide the clinician to recognize abuse, although there is no international consensus [18].

Table 1.
Red flag history and examination findings associated with abuse.
Orthopedic aspects of child abuse is one area of interest in automating the recognition and referral of potential abuse given the auditability of such injuries [19]. Although no fracture pattern is pathognomonic of child abuse, various studies have described the reported prevalence of some fracture patterns, albeit with individual limitations (Table 2).
Table 2.
Reported prevalence of some fracture patterns.
Internationally, there is no consensus on fractures that should raise concern for non-accidental injury. Some fracture types are consistently described in various guidelines and statements internationally and are summarized in Table 3 [19,23,28,30,31,32,33,34,35,36,37].
Table 3.
Fracture types associated with abuse.
Documentation is also a limiting factor when assessing injuries for possible abuse red flags. [38] A retrospective audit across 2001–2002 evaluating ED assessment and follow-up of possible child abuse in children under 3 years of age with fractures found that in over half of the 98 cases included, there was no physical examination documentation nor documentation regarding whether the injury was witnessed [38]. Additionally, 75% of children with known prior injuries did not have their history documented, and in 80% of all cases, there was no indication that the ED doctor had considered the possibility of child abuse [38].
It is noteworthy that in Australia, emotional abuse (59%) is the most common type of abuse substantiated through investigations, with the remaining 41% comprising neglect (17%), physical abuse (15%) and sexual abuse (9%) [4]. In Tasmania, from 2021 to 2022, of the children who had substantiated claims of child abuse and neglect, there were 50 children (26%) who had been the recipients of physical abuse, and 151 children (80%) were neglected [2]. Fractures are the second most common injury (after soft tissue injury) in children who suffer from physical abuse and are present in up to 55% of cases involving physically abused children [9].
Our research seeks to evaluate the incidence of fractures concerning non-accidental injury (NAI) in children under three years old who presented to a tertiary, mixed ED. Children under three years old have been selected as the target population due to the vulnerability of this age group, with a total of 85% of non-accidental fractures occur in children under three years old, as well as previously published literature utilizing a similar age range [9,38].
2. Materials and Methods
2.1. Setting
This study was conducted in a major tertiary-referral, teaching, mixed ED in Australia with an annual presentation rate of just over 75,000 patients of which approximately 35% are less than 14 years old [39,40]. The admission rate for patients less than 18 years of age is 22.5%. Pediatric patients are defined as less than 14 years of age in line with local definitions. The ED uses a hybrid medical record system with patient tracking and patient notes captured electronically, whilst patient observations, medications and fluids are charted on paper. The ED is staffed by a range of doctors including specialists, registrars, residents and interns and has three specialist pediatric emergency physicians. The pediatric department is mainly staffed by general pediatricians with select pediatric subspecialties available on-site. It is a major pediatric referral center with a dedicated neonatal and pediatric intensive care unit with pediatric medical staff available on site 24 h per day, 7 days per week.
2.2. Objectives
Primary objective: to identify the incidence of fracture types associated with abuse in children under three years old presenting to the ED.
Secondary objectives: to examine the actions taken, including referral processes for fracture types associated with abuse in children under three years old; to evaluate representation or other hospital-based management within 12 months after ED presentation for patients where no concern for NAI was documented.
The purpose of this study is not to validate the diagnostic value of fractures and their relationship to abuse.
2.3. Methods
This study was a retrospective descriptive study. The inclusion criteria consisted of (a) children less than three years of age, (b) presenting to the ED, (c) between 1 January 2020, and 31 December 2022, inclusive and (d) with a diagnosis consistent with a fracture type associated with abuse (Table 3). Exclusion criteria consisted of (a) no fracture on the official radiological report, (b) no medical records to review, (c) patients left after treatment started, (d) congenital bone disease, (e) osteomyelitis and (f) re-presentation to the ED for the same fracture (e.g., plaster cast management).
Data collected included patient hospital number, age, gender, ED primary diagnostic description, triage category, the mechanism of injury, bone fractured, radiology report from the X-ray performed, the location of injury, developmental level, disposition, outpatient follow-up by a hospital-based specialist, child safety service guardianship status and CSS notification status. Medical records were also screened for any suggestion that the treating doctor had considered or excluded the diagnosis of NAI.
2.4. Data Analysis
Descriptive statistics were used to summarize the data. Categorical variables were presented as frequencies and percentages, and continuous variables were presented as means and standard deviations (SDs) or medians and interquartile ranges (IQRs), as appropriate. Researchers met to discuss and agree upon the statistical methods and ensured consistency in data interpretation. All statistical analyses were performed using Microsoft Excel (Version 16.88).
2.5. Ethical Approval
Ethical approval was granted by Tasmania Health and Medical Human Research Ethics Committee on 12 December 2023, HREC30070.
3. Results
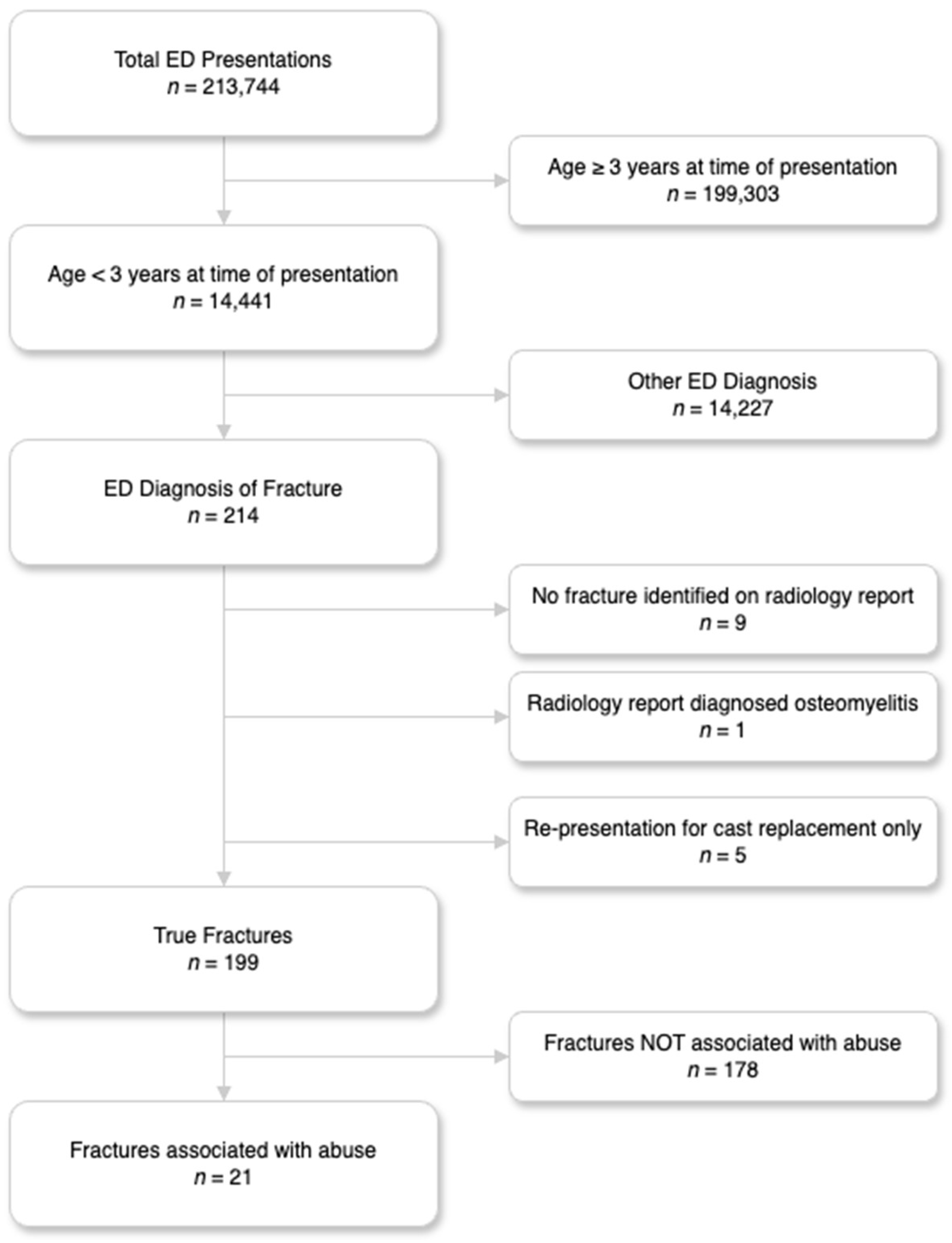
For the study period, 213,744 patients presented to the ED with 14,441 aged under 3 years (Figure 1). Of these, 214 (0.1%) patients had sustained a fracture. Following the application of the inclusion and exclusion criteria for all fractures sustained in children less than 3 years old, 21 (10.5%) patients were identified as having a fracture type associated with an abuse diagnosis. Their characteristics are described in Table 4. The average age was 1.38 years with an absolute range from 3 weeks to 2 years and 11 months. Australian emergency department triage patients were categorized according to the Australian Triage Scale (ATS), where one is the most urgent and five the least. The most common Australian Triage Score (ATS) category assigned on arrival was three (12, 57.14%) followed by three and four (7, 33.33%; 2, 9.53%) with no ATS category of one or two. For all patients with a fracture type associated with abuse, the median ED length of stay was 3.55 h (IQR 2.65–5.58). The length of stay changed when grouped into admitted (8, 38%) and not admitted (13, 62%), with median times of 5.7 h and 2.8 h consecutively. Only one patient was transported to the ED by ambulance, with the remainder walking in. In terms of disposition, thirteen children were discharged from the ED, five admitted under the orthopedic team and three admitted under the pediatric team.
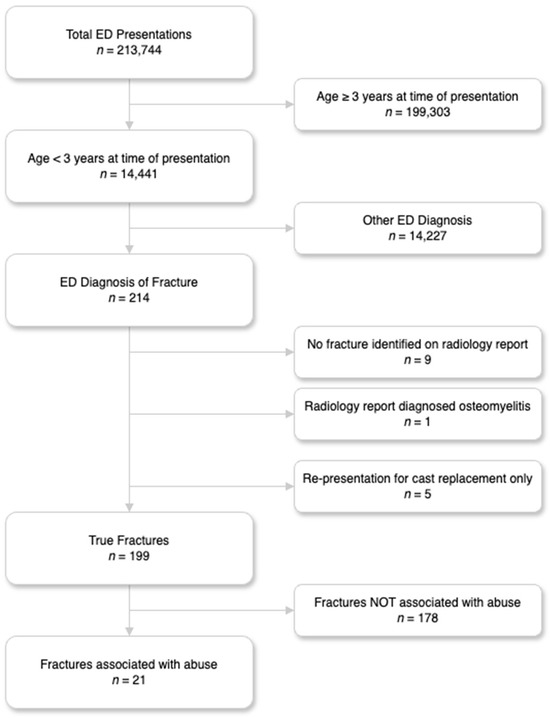
Figure 1.
Flow of patients through the study.
Table 4.
Fractures identified which were concerning for NAI.
Of the eleven types of fractures and fracture patterns associated with abuse, our cohort of 21 patients represented only two of those categories (long bone fractures in non-ambulatory patients and digital fractures in patients less than 3 years of age). The most common fracture types included femur fractures (33%) and phalanx (19%), with humerus, radius and tibia each representing 14% of the cohort.
In terms of ED clinician concern for NAI, this was considered in eight (38%) of the patients, with three of these concerning. For all concerning patients, all were referred to the pediatric team and CSS. Interestingly, three patients were treated as ‘not concerning’ by the ED clinician, and following orthopedic outpatient assessment, they were assessed to be concerning and were referred to the pediatric team but not CSS.
Non accidental injury was not considered in 13 (62) of the patients. The medical record review of these patients up to 12 months after initial ED presentation showed that five did not represent to the ED, one was referred to CSS from outpatients and two re-presented within this period with minor head injuries (Table 5).
Table 5.
The 12-month follow-up of children with fracture type suspicious for NAI where NAI was not considered.
4. Discussion
Over a three-year period from 1 January 2020, to 31 December 2022, there were 14,441 ED presentations for children under 3, of which 214 children (1.48%) presented with fractures. We identified 21 children (10.6%) who had fractures which were concerning for NAI based on the study definition. Based on average ED presentations, this equates to approximately one episode per month assuming a normal distribution. Previous reports have described the proportion of fractures of concern compared to all fractures in children less than 3 as being 4.9% [16,38]. Our study is of significance because infants and toddlers are the age group at the highest risk of child abuse and neglect leading to fatality [41]. Australian data indicate that children under 12 months of age were twice as likely (17 per 1000 children) to have at least one child protection notification substantiated compared to children aged 1–4 years old (9 per 1000 children) or 5–12 years old (8.3 per 1000 children) [4]. These statistics are also reflected in data from other countries, with 2015 data from the USA revealing that 74.8% of child deaths in children under three years of age were from abuse and neglect [41].
In 2021–2022, Australia-wide data indicated that out of the three common sources of child safety notifications, 11% were made by medical/health personnel, whereas police (24%) and school personnel (25%) made considerably more notifications [4]. For our study, only eleven patients (5.5%) were referred to the local CSS due to clinical concerns regarding NAI, with only four patients out of twenty-one (19%) from the cohort with fractures of concern referred onwards to CSS. The current literature describing the rate of referrals to local CSS is variable, with reports between 1 and 17% [38,42,43]. Zigler et al. based at the Sydney Children’s Hospital found that 16.3% of patients were referred to CSS for fractures concerning NAI, with 4.1% of the study population having substantiated claims of abuse after investigation by CSS [38]. A 2004 study by Taitz et al. based in an Australian hospital identified that only 1% of their cohort over a two-year period was referred to child safety services, despite having 31% of the cohort identified as having indicators of abuse [43]. Leaman et al. in Pennsylvania identified that 17% of their patients under two years old sustaining fractures, assessed over a two-year period, were due to NAI, keeping in mind that the substantiation of this was not reported due to medico–legal barriers [42]. The end point for all three studies is slightly different, thus potentially resulting in a variation in how the statistics are reported. Other possible explanations for this variation in incidence could include geographical and socioeconomic differences as well as differing levels of training by health professionals in the recognition of child physical abuse and a difference in the age range of children included in the studies.
Based on the results of this study, the rates of referral to CSS from the ED were lower compared to Zigler et al., who were based in Australia in 2008 (5.5% vs. 16%). [38] On the other hand, the percentage of children having fractures concerning NAI in this study cohort was 10.6%, whereas in a comparable Australian study in 2004 by Taitz et al., this was 31%. [43] One additional explanation for this is that eight children (38%) were admitted to the ward with the ED expecting child abuse screening to be performed by the admitting team.
It should also be noted that not all findings that appear abusive in nature result from abuse. [42] For fractures, some age groups and fracture patterns are suggestive whilst the majority do not absolutely differentiate intentional from unintentional injury (Table 2) [20,21,22]. For example, child abuse accounts for 60–80% of femur fractures in children younger than one year of age, with a meta-analysis describing the probability of confirmed or suspected abuse in children with a femur fracture as 43% (95% CI, 32–54%) [20,21,22,23]. This raises concerns for our findings where for femur fractures less than 1 year of age (seven patients), the ED was not suspicious of NAI in five cases and not documented in one. For three patients, there was follow-up in orthopedic outpatients where suspicion warranted a pediatric review with only one referral made to child safety services following this.
The diagnosis of NAI is difficult in the ED setting due to a variety of factors. The combination of overcrowded EDs together with patients who are unable to advocate for themselves, low triage categorization, high staff turnover and uncommon presentation (approximately one per month) complicates accurate diagnosis and effective management. However, there is also a high cost if one is missed. In Tasmania, in 2021–2022, there were 50 children (13% of all substantiated claims of abuse or neglect) who had substantiated claims of physical abuse [2]. Australia-wide, substantiated claims of physical abuse in children constitute 13.5% of all substantiated claims of abuse or neglect [2].
There is documentation in the literature regarding ways to improve the consideration and documentation of NAI. Benger and Pearce were able to demonstrate an improvement in documentation where the diagnosis of NAI was considered from 16% to 71% by incorporating a flowchart in the notes for the assessment of intentional injury [7]. The TEN-4-FACESp rule around bruising in children researched and implemented by Pierce et al. is one example of a now well-recognized tool to aid clinicians in the detection of NAI [44]. Although there is currently no similar clinical rule available for fractures, much can be performed to improve the current rates of identification of NAI.
One other barrier EDs inherently possess is a high turnover of staff with varying expertise [39]. The high turnover of staff means that education for rare scenarios is inefficient and ineffective given the breadth of knowledge required when onboarding. Targeted education and incorporating actions based on the most stable staffing base appear to be the most reliable method to ensure standardized care is provided to a wide variety of scenarios [45]. One example of how this can be incorporated is through targeted education to radiologists and the orthopedic teams who are likely to see proportionally more cases than the ED staff. Automated systems also show promise in identifying these patients and initiating referral processes [46]. For example, electronic medical records may identify keywords that trigger a prompt to consider NAI and provide instructions on next steps [46]. For a hybrid system such as ours, a more innovative approach through paper-based forms may have to suffice, noting the limitations of paper forms [46].
Limitations
This study is also limited by being retrospective in nature, thus being completely reliant on the documentation of the history, as well as the examination and management of the cases discussed, which at times were incomplete. A conservative approach was used to minimize the risk of overdiagnosis of abuse. It is also well established that documentation in EDs is poorly performed which can also limit the interpretation of clinician judgment regarding the consideration of NAI [47]. Additionally, this review focuses on a relatively small sample size which may not be representative of a larger population. We also acknowledge that although we have listed all fractures which occurred in under one-year-old children as being a fracture in a non-ambulant child, there may be variation in attainment of developmental milestones, and some children may be ambulant before reaching their first birthday. Finally, since CSS is a different organization to the health service, we were unable to ascertain the results of CSS investigations once they were referred or if they were referred to CSS outside of the health service within the 12-month follow-up period.
5. Conclusions
Over a three-year period, the incidence of high-risk fractures in the under three-year-old age group was comparable to that stated in the literature with 10.6%. Of those patients, around half (52%) were referred to CSS, lower than the reported literature. More work can be performed to improve the identification and documentation of the possibility of NAI in children under three years old, particularly children under one year old, with only 26% of patients having specific documentation around the consideration of NAI. System changes including further training in screening for child abuse, as well as the provision of guidelines proformas and/or flowcharts supported by education will increase the opportunity to improving this area.
Author Contributions
Conceptualization, A.L., L.P. and V.T.; methodology, A.L., L.P. and V.T.; analysis, A.L., L.P. and V.T.; investigation, A.L., L.P. and V.T.; writing—original draft preparation, A.L.; writing—review and editing, A.L., L.P. and V.T.; visualization, A.L., L.P. and V.T.; supervision, L.P. and V.T.; project administration, A.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethics approval was provided by Tasmania Health and Medical Human Research Ethics Committee on 12 December 2023, HREC30070.
Informed Consent Statement
Patient consent was waived as this was a retrospective review of routinely collected data and ethically approved in this manner.
Data Availability Statement
The data presented in this study are available upon request from the corresponding author. The data are not publicly available due to ethical review board requirements.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- National Institute for Health and Care Excellence. Child Maltreatment: When to Suspect Maltreatment in Under 18s; NICE: London, UK, 2009. [Google Scholar]
- Australian Institute of Health and Welfare. Child Protection Australia 2020–2021. Available online: https://www.aihw.gov.au/reports/child-protection/child-protection-australia-2020-21/contents/summary (accessed on 14 May 2024).
- Damashek, A.; Nelson, M.M.; Bonner, B.L. Fatal child maltreatment: Characteristics of deaths from physical abuse versus neglect. Child Abus. Negl. 2013, 37, 735–744. [Google Scholar] [CrossRef] [PubMed]
- Australian Institute of Health and Welfare. Child Protection Australia 2022–2023. Available online: https://www.aihw.gov.au/reports/child-protection/child-protection-australia-insights/contents/about (accessed on 14 May 2024).
- Fang, X.; Brown, D.S.; Florence, C.S.; Mercy, J.A. The economic burden of child maltreatment in the United States and implications for prevention. Child Abus. Negl. 2012, 36, 156–165. [Google Scholar] [CrossRef]
- Felitti, V.J.; Anda, R.F.; Nordenberg, D.; Williamson, D.F.; Spitz, A.M.; Edwards, V.; Koss, M.P.; Marks, J.S. Relationship of Childhood Abuse and Household Dysfunction to Many of the Leading Causes of Death in Adults. Am. J. Prev. Med. 1998, 14, 245–258. [Google Scholar] [CrossRef] [PubMed]
- Benger, J.R.; Pearce, V. Simple intervention to improve detection of child abuse in emergency departments. BMJ 2002, 324, 780. [Google Scholar] [CrossRef]
- Tiyyagura, G.; Beucher, M.; Bechtel, K. Nonaccidental Injury in Pediatric Patients: Detection, Evaluation, and Treatment. Pediatr. Emerg. Med. Pract. 2017, 14, 1–32. [Google Scholar] [PubMed]
- Ho, C.A.; Scherl, S.A. Orthopedic Aspects of Child Abuse. In UpToDate; Connor, R.F., Ed.; Wolters Kluwer: Alphen aan den Rijn, The Netherlands; Available online: http://112.2.34.14:9095/contents/orthopedic-aspects-of-child-abuse (accessed on 14 May 2024).
- Jenny, C.; Hymel, K.P.; Ritzen, A.; Reinert, S.E.; Hay, T.C. Analysis of missed cases of abusive head trauma. JAMA 1999, 281, 621–626. [Google Scholar] [CrossRef] [PubMed]
- Sheets, L.K.; Leach, M.E.; Koszewski, I.J.; Lessmeier, A.M.; Nugent, M.; Simpson, P. Sentinel injuries in infants evaluated for child physical abuse. Pediatrics 2013, 131, 701–707. [Google Scholar] [CrossRef] [PubMed]
- Rangel, E.L.; Cook, B.S.; Bennett, B.L.; Shebesta, K.; Ying, J.; Falcone, R.A. Eliminating disparity in evaluation for abuse in infants with head injury: Use of a screening guideline. J. Pediatr. Surg. 2009, 44, 1229–1234. [Google Scholar] [CrossRef]
- Hoehn, E.F.; Wilson, P.M.; Riney, L.C.; Ngo, V.; Bennett, B.; Duma, E. Identification and Evaluation of Physical Abuse in Children. Pediatr. Ann. 2018, 47, e97–e101. [Google Scholar] [CrossRef]
- Thackeray, J.D.; Crichton, K.G.; McPherson, P.; Izsak, E.; Vavul-Roediger, L.; Kim, G.; Spencer, S.; Baker, C.; Eismann, E.A.; Shapiro, R.A. Identification of Initial and Subsequent Injury in Young Infants: Opportunities for Quality Improvement in the Evaluation of Child Abuse. Pediatr. Emerg. Care 2022, 38, e1279–e1284. [Google Scholar] [CrossRef]
- Wood, J.N.; Christian, C.W.; Adams, C.M.; Rubin, D.M. Skeletal surveys in infants with isolated skull fractures. Pediatrics 2009, 123, e247–e252. [Google Scholar] [CrossRef] [PubMed]
- Rosendahl, K.; Myklebust, R.; Ulriksen, K.F.; Nøttveit, A.; Eide, P.; Djuve, Å.; Brudvik, C. Incidence, pattern and mechanisms of injuries and fractures in children under two years of age. BMC Musculoskelet. Disord. 2021, 22, 555. [Google Scholar] [CrossRef] [PubMed]
- Lindberg, D.M.; Beaty, B.; Juarez-Colunga, E.; Wood, J.N.; Runyan, D.K. Testing for Abuse in Children With Sentinel Injuries. Pediatrics 2015, 136, 831–838. [Google Scholar] [CrossRef] [PubMed]
- Christian, C.W. The evaluation of suspected child physical abuse. Pediatrics 2015, 135, e1337–e1354. [Google Scholar] [CrossRef]
- Kocher, M.S.; Kasser, J.R. Orthopaedic aspects of child abuse. J. Am. Acad. Orthop. Surg. 2000, 8, 10–20. [Google Scholar] [CrossRef]
- Beals, R.K.; Tufts, E. Fractured femur in infancy: The role of child abuse. J. Pediatr. Orthop. 1983, 3, 583–586. [Google Scholar] [CrossRef]
- Gross, R.H.; Stranger, M. Causative factors responsible for femoral fractures in infants and young children. J. Pediatr. Orthop. 1983, 3, 341–343. [Google Scholar] [CrossRef]
- McClelland, C.Q.; Heiple, K.G. Fractures in the first year of life: A diagnostic dilemma. Am. J. Dis. Child. 1982, 136, 26–29. [Google Scholar] [CrossRef]
- Kemp, A.M.; Dunstan, F.; Harrison, S.; Morris, S.; Mann, M.; Rolfe, K.; Datta, S.; Thomas, D.P.; Sibert, J.R.; Maguire, S. Patterns of skeletal fractures in child abuse: Systematic review. BMJ 2008, 337, a1518. [Google Scholar] [CrossRef]
- Galleno, H.; Oppenheim, W.L. The battered child syndrome revisited. Clin. Orthop. Relat. Res. 1982, 162, 11–19. [Google Scholar] [CrossRef]
- King, J.; Diefendorf, D.; Apthorp, J.; Negrete, V.F.; Carlson, M. Analysis of 429 fractures in 189 battered children. J. Pediatr. Orthop. 1988, 8, 585–589. [Google Scholar] [PubMed]
- Loder, R.T.; Bookout, C. Fracture patterns in battered children. J. Orthop. Trauma 1991, 5, 428–433. [Google Scholar] [CrossRef] [PubMed]
- Shaw, B.A.; Murphy, K.M.; Shaw, A.; Oppenheim, W.L.; Myracle, M.R. Humerus shaft fractures in young children: Accident or abuse? J. Pediatr. Orthop. 1997, 17, 293–297. [Google Scholar] [CrossRef] [PubMed]
- Paine, C.W.; Fakeye, O.; Christian, C.W.; Wood, J.N. Prevalence of Abuse Among Young Children With Rib Fractures: A Systematic Review. Pediatr. Emerg. Care 2019, 35, 96–103. [Google Scholar] [CrossRef]
- Leventhal, J.M.; Martin, K.D.; Asnes, A.G. Incidence of fractures attributable to abuse in young hospitalized children: Results from analysis of a United States database. Pediatrics 2008, 122, 599–604. [Google Scholar] [CrossRef]
- Akbarnia, B.; Torg, J.S.; Kirkpatrick, J.; Sussman, S. Manifestations of the battered-child syndrome. J. Bone Jt. Surg. Am. 1974, 56, 1159–1166. [Google Scholar] [CrossRef]
- Crowe, M.; Byerly, L.; Mehlman, C.T. Transphyseal Distal Humeral Fractures: A 13-Times-Greater Risk of Non-Accidental Trauma Compared with Supracondylar Humeral Fractures in Children Less Than 3 Years of Age. J. Bone Jt. Surg. Am. 2022, 104, 1204–1211. [Google Scholar] [CrossRef]
- Flaherty, E.G.; Perez-Rossello, J.M.; Levine, M.A.; Hennrikus, W.L. Evaluating children with fractures for child physical abuse. Pediatrics 2014, 133, e477–e489. [Google Scholar] [CrossRef]
- Kogutt, M.S.; Swischuk, L.E.; Fagan, C.J. Patterns of injury and significance of uncommon fractures in the battered child syndrome. Am. J. Roentgenol. Radium Ther. Nucl. Med. 1974, 121, 143–149. [Google Scholar] [CrossRef]
- Mitchell, I.C.; Norat, B.J.; Auerbach, M.; Bressler, C.J.; Como, J.J.; Escobar, M.A., Jr.; Flynn-O’Brien, K.T.; Lindberg, D.M.; Nickoles, T.; Rosado, N.; et al. Identifying Maltreatment in Infants and Young Children Presenting With Fractures: Does Age Matter? Acad. Emerg. Med. 2021, 28, 5–18. [Google Scholar] [CrossRef]
- Mitchell, P.D.; Brown, R.; Wang, T.; Shah, R.D.; Samworth, R.J.; Deakin, S.; Edge, P.; Hudson, I.; Hutchinson, R.; Stohr, K.; et al. Multicentre study of physical abuse and limb fractures in young children in the East Anglia Region, UK. Arch. Dis. Child 2019, 104, 956–961. [Google Scholar] [CrossRef] [PubMed]
- Rao, P.; Carty, H. Non-accidental injury: Review of the radiology. Clin. Radiol. 1999, 54, 11–24. [Google Scholar] [CrossRef] [PubMed]
- Tadepalli, V.; Schultz, J.D.; Rees, A.B.; Wollenman, L.C.; Louer, C.R.; Lempert, N.L.; Moore-Lotridge, S.N.; Schoenecker, J.G. Nonaccidental Trauma in Pediatric Elbow Fractures: When You Should Be Worried. J. Pediatr. Orthop. 2022, 42, e601–e606. [Google Scholar] [CrossRef] [PubMed]
- Ziegler, D.S.; Sammut, J.; Piper, A.C. Assessment and follow-up of suspected child abuse in preschool children with fractures seen in a general hospital emergency department. J. Paediatr. Child Health 2005, 41, 251–255. [Google Scholar] [CrossRef]
- Tran, V.; Barrington, G.; Page, S. The Tasmanian Emergency Care Outcomes Registry (TECOR) Protocol. Emerg. Care Med. 2024, 1, 153–164. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics. Regional Population by Age and Sex 2021. Available online: https://www.abs.gov.au/statistics/people/population/regional-population-age-and-sex/2021 (accessed on 14 May 2024).
- U.S. Department of Health & Human Services; Administration for Children and Families (ACF); Administration on Children, Youth and Families; Children’s Bureau. Child Maltreatment 2017. Available online: https://www.acf.hhs.gov/sites/default/files/documents/cb/cm2017.pdf (accessed on 14 May 2024).
- Leaman, L.A.; Hennrikus, W.L.; Bresnahan, J.J. Identifying non-accidental fractures in children aged <2 years. J. Child Orthop. 2016, 10, 335–341. [Google Scholar] [CrossRef]
- Taitz, J.; Moran, K.; O’Meara, M. Long bone fractures in children under 3 years of age: Is abuse being missed in Emergency Department presentations? J. Paediatr. Child Health 2004, 40, 170–174. [Google Scholar] [CrossRef]
- Pierce, M.C.; Kaczor, K.; Lorenz, D.J.; Bertocci, G.; Fingarson, A.K.; Makoroff, K.; Berger, R.P.; Bennett, B.; Magana, J.; Staley, S.; et al. Validation of a Clinical Decision Rule to Predict Abuse in Young Children Based on Bruising Characteristics. JAMA Netw. Open 2021, 4, e215832. [Google Scholar] [CrossRef]
- Geerligs, L.; Rankin, N.M.; Shepherd, H.L.; Butow, P. Hospital-based interventions: A systematic review of staff-reported barriers and facilitators to implementation processes. Implement. Sci. 2018, 13, 36. [Google Scholar] [CrossRef]
- Koh, J.; Ahmed, M. Improving clinical documentation: Introduction of electronic health records in paediatrics. BMJ Open Qual. 2021, 10, e000918. [Google Scholar] [CrossRef]
- Smith, J.D.; Lemay, K.; Lee, S.; Nuth, J.; Ji, J.; Montague, K.; Garber, G.E. Medico-legal issues related to emergency physicians’ documentation in Canadian emergency departments. Can. J. Emerg. Med. 2023, 25, 768–775. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).