An Instrumental Analysis of the Triad Association Between Sugar-Sweetened Beverages, Screen Time, and Dental Caries in Adolescents

 , , ,
, , , 

Abstract
Highlights
- What are the main findings?
- More screen time on mobile devices was associated with worse dental caries experiences in adolescents.
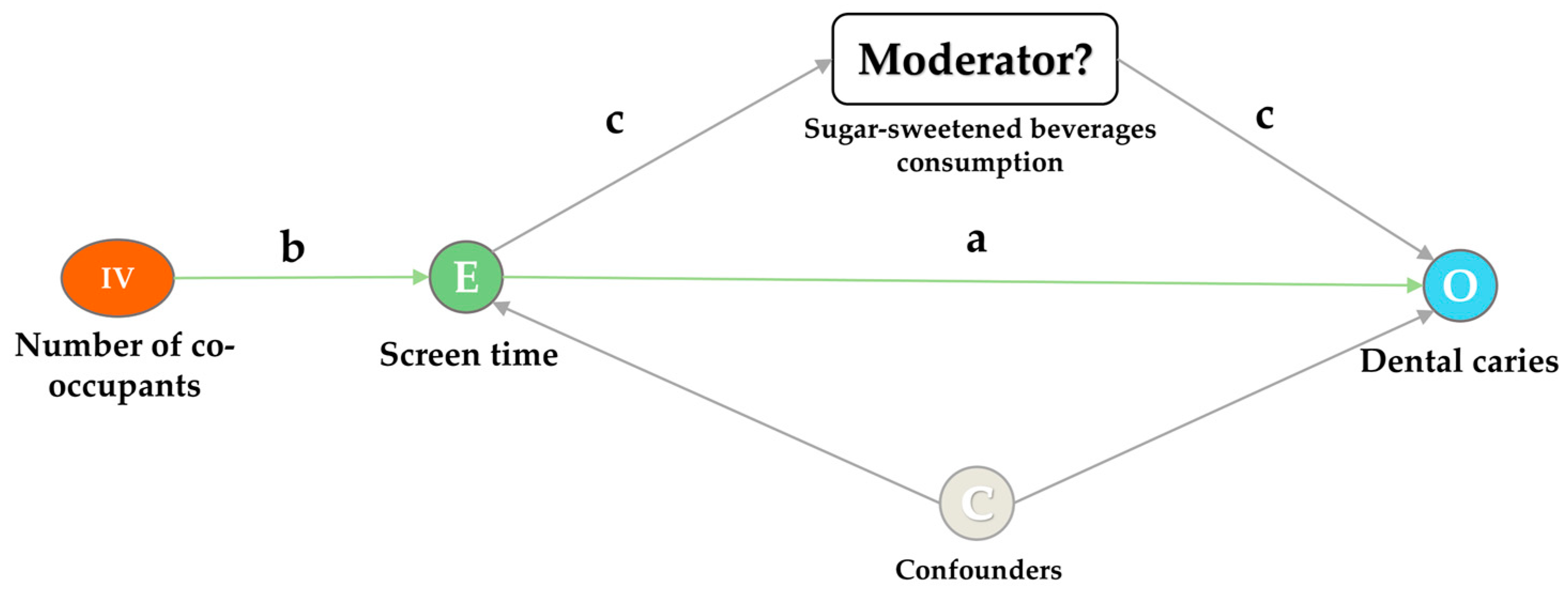
- Sugar-sweetened beverage intake might be an independent influential factor for dental caries instead of the mediator between screen time on mobile devices and dental caries.
- What are the implications of the main findings?
- Our findings highlighted the necessity to alleviate the burden of dental caries in adolescents and called for concerted actions, including the establishment of appropriate intervention strategies with better targeting of excess time on mobile devices to prevent dental caries and promote oral health in adolescents.
- Implementing recommendations on reducing screen time and promoting healthier dietary patterns, including control of sugar-sweetened beverage consumption, could be beneficial in alleviating the burden of dental caries in adolescents.
Abstract
1. Introduction
2. Methods
2.1. Study Design and Participants
2.2. Measurements
2.2.1. Dental Caries Experiences
2.2.2. Screen Time on Mobile Devices
2.2.3. Consumption of Sugar-Sweetened Beverages
2.2.4. Instrumental Variable
2.2.5. Model Covariates
2.3. Statistical Analysis
3. Results
3.1. Screen Time in Relation to Dental Caries Experiences
3.2. Causal Validation of IV Approach
3.3. Relationship Between Screen Time on Mobile Devices, Sugar-Sweetened Beverages, and Dental Caries
3.4. Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Ji, W.; Shen, J.; Yang, B.; Ji, L. Annual Report on the Internet Use of Chinese Minors (2021); Social Sciences Academic Press: Beijing, China, 2021. [Google Scholar]
- CNNIC. Research Report on Internet Behavior of Chinese Adolescents in 2014; China Internet Network Information Center: Beijing, China, 2015. [Google Scholar]
- CNNIC. Research Report on Internet Behavior of Chinese Adolescents in 2019; China Internet Network Information Center: Beijing, China, 2020. [Google Scholar]
- Odgers, C.L.; Jensen, M.R. Annual Research Review: Adolescent mental health in the digital age: Facts, fears, and future directions. J. Child Psychol. Psychiatry 2020, 61, 336–348. [Google Scholar] [CrossRef] [PubMed]
- Tortorella, G.L.; Narayanamurthy, G.; Sunder, M.V.; A Cauchick-Miguel, P. Operations Management teaching practices and information technologies adoption in emerging economies during COVID-19 outbreak. Technol. Forecast. Soc. Chang. 2021, 171, 120996. [Google Scholar] [CrossRef] [PubMed]
- Pearson, N.; Biddle, S.J. Sedentary behavior and dietary intake in children, adolescents, and adults. A systematic review. Am. J. Prev. Med. 2011, 41, 178–188. [Google Scholar] [CrossRef] [PubMed]
- Lissak, G. Adverse physiological and psychological effects of screen time on children and adolescents: Literature review and case study. Environ. Res. 2018, 164, 149–157. [Google Scholar] [CrossRef] [PubMed]
- Asaka, Y.; Sekine, M.; Yamada, M.; Tatsuse, T.; Sano, M. Association of short sleep duration and long media use with caries in school children. Pediatr. Int. 2020, 62, 214–220. [Google Scholar] [CrossRef]
- GBD 2015 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1545–1602. [Google Scholar] [CrossRef]
- Turton, B.; Sullivan, S.; Chher, T.; Hak, S.; Sokal-Gutierrez, K.; Wieringa, F.; Singh, A. Caries Incidence Is Associated with Wasting among Cambodian Children. J. Dent. Res. 2023, 102, 157–163. [Google Scholar] [CrossRef]
- Zhao, J.; Yu, Z.; Sun, X.; Wu, S.; Zhang, J.; Zhang, D.; Zhang, Y.; Jiang, F. Association Between Screen Time Trajectory and Early Childhood Development in Children in China. JAMA Pediatr. 2022, 176, 768–775. [Google Scholar] [CrossRef]
- Vujicic, M.; Buchmueller, T.; Klein, R. Dental Care Presents the Highest Level of Financial Barriers, Compared to Other Types of Health Care Services. Health Aff. 2016, 35, 2176–2182. [Google Scholar] [CrossRef]
- Moussa, D.G.; Ahmad, P.; Mansour, T.A.; Siqueira, W.L. Current State and Challenges of the Global Outcomes of Dental Caries Research in the Meta-Omics Era. Front. Cell. Infect. Microbiol. 2022, 12, 887907. [Google Scholar] [CrossRef]
- Zhang, X.-Y.; Yang, W.-Y.; Yang, J.; Wang, Y.; Xiang, Y.; Gao, L.-W.; Zhang, F.-Y.; Zhou, Y.-L. Epidemiological characteristics of childhood obesity in eastern China, 2017–2019. World J. Pediatr. 2019, 15, 412–414. [Google Scholar] [CrossRef] [PubMed]
- Huang, F.; Wang, Y.; Xue, H.; Zhang, X.; Tian, Y.; Du, W.; Fan, L.; Yang, J. Are Rural–Urban Differences in Bullying and Poly-Bullying Victimization Associated with Internet Addiction or Depressive Symptoms among Adolescents in Jiangsu Province of China. Future 2024, 2, 1–15. [Google Scholar] [CrossRef]
- World Health Organization. Oral Health Surveys: Basic Methods, 5th ed.; WHO: Geneva, Switzerland, 2013; Available online: https://www.who.int/publications-detail-redirect/9789241548649 (accessed on 20 June 2024).
- Xu, J.; Gao, C. Physical activity guidelines for Chinese children and adolescents: The next essential step. J. Sport Health Sci. 2018, 7, 120–122. [Google Scholar] [CrossRef] [PubMed]
- Lu, C.; Shen, T.; Huang, G.; Corpeleijn, E. Environmental correlates of sedentary behaviors and physical activity in Chinese preschool children: A cross-sectional study. J. Sport Health Sci. 2022, 11, 620–629. [Google Scholar] [CrossRef] [PubMed]
- Friedman, J.; Hastie, T.; Tibshirani, R. Regularization Paths for Generalized Linear Models via Coordinate Descent. J. Stat. Softw. 2010, 33, 1–22. [Google Scholar] [CrossRef]
- Baron, R.M.; Kenny, D.A. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Pers. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef]
- Hafeman, D.M. “Proportion explained”: A causal interpretation for standard measures of indirect effect? Am. J. Epidemiol. 2009, 170, 1443–1448. [Google Scholar] [CrossRef]
- Fu, R.; Kim, S.J. Inferring causality from observational studies: The role of instrumental variable analysis. Kidney Int. 2021, 99, 1303–1308. [Google Scholar] [CrossRef]
- Stata. 2017. Available online: https://www.stata.com/features/overview/extended-regression-models/ (accessed on 20 June 2024).
- Campbell, J.A.; Walker, R.J.; Egede, L.E. Associations Between Adverse Childhood Experiences, High-Risk Behaviors, and Morbidity in Adulthood. Am. J. Prev. Med. 2016, 50, 344–352. [Google Scholar] [CrossRef]
- Oh, C.; Carducci, B.; Vaivada, T.; A Bhutta, Z. Digital Interventions for Universal Health Promotion in Children and Adolescents: A Systematic Review. Pediatrics 2022, 149 (Suppl. 5), e2021053852H. [Google Scholar] [CrossRef]
- Liu, S.; Zou, S.; Zhang, D.; Wang, X.; Wu, X. Problematic Internet use and academic engagement during the COVID-19 lockdown: The indirect effects of depression, anxiety, and insomnia in early, middle, and late adolescence. J. Affect. Disord. 2022, 309, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Reichenberger, J.; Richard, A.; Smyth, J.M.; Fischer, D.; Pollatos, O.; Blechert, J. It’s craving time: Time of day effects on momentary hunger and food craving in daily life. Nutrition 2018, 55–56, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Robinson, T.N.; Banda, J.A.; Hale, L.; Lu, A.S.; Fleming-Milici, F.; Calvert, S.L.; Wartella, E. Screen media exposure and obesity in children and adolescents. Pediatrics 2017, 140, S97–S101. [Google Scholar] [CrossRef] [PubMed]
- Markovitz, A.A.; Hollingsworth, J.M.; Ayanian, J.Z.; Norton, E.C.; Yan, P.L.; Ryan, A.M. Performance in the Medicare Shared Savings Program After Accounting for Nonrandom Exit: An Instrumental Variable Analysis. Ann. Intern. Med. 2019, 171, 27–36. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Variables | Total n = 24,374 | Screen Time on Mobile Devices (Hours/Day), n (%) a | p-Value b | |
|---|---|---|---|---|
| <2 | ≥2 | |||
| n = 19,315 | n = 5059 | |||
| Covariates: | ||||
| Age (year) | ||||
| 12~15 | 16,318 (66.9) | 13,339 (69.1) | 2979 (58.9) | <0.001 *** |
| 16~17 | 8056 (33.1) | 5976 (30.9) | 2080 (41.1) | |
| Gender | ||||
| Boy | 12,658 (51.9) | 10,037 (52.0) | 2621 (51.8) | 0.843 |
| Girl | 11,716 (48.1) | 9278 (48.0) | 2438 (48.2) | |
| Geographic region | ||||
| South | 9377 (38.5) | 7696 (39.8) | 1681 (33.2) | <0.001 *** |
| Middle | 5596 (23.0) | 4411 (22.8) | 1185 (23.4) | |
| North | 9401 (38.6) | 7208 (37.3) | 2193 (43.3) | |
| Maternal educational level | ||||
| Primary school and below | 3220 (13.2) | 2306 (11.9) | 914 (18.1) | <0.001 *** |
| Junior and senior high school | 17,410 (71.4) | 13,723 (71.0) | 3687 (72.9) | |
| More advanced attainment | 3744 (15.4) | 3286 (17.0) | 458 (9.1) | |
| Tooth brushing habit | ||||
| Yes | 17,944 (73.6) | 14,626 (75.7) | 3318 (65.6) | <0.001 *** |
| No | 6430 (26.4) | 4689 (24.3) | 1741 (34.4) | |
| Obesity | ||||
| Yes | 15,304 (62.8) | 7183 (37.2) | 1887 (37.3) | 0.884 |
| No | 9070 (37.2) | 12,132 (62.8) | 3172 (62.7) | |
| Parental intervention | ||||
| Yes | 15,400 (63.2) | 13,076 (67.7) | 2324 (45.9) | <0.001 *** |
| No | 8974 (36.8) | 6239 (32.3) | 2735 (54.1) | |
| Dietary behaviors: | ||||
| Sugar-sweetened beverage intake | ||||
| Never | 5610 (23.0) | 4886 (25.3) | 724 (14.3) | <0.001 *** |
| Sometimes | 16,368 (67.2) | 12,845 (66.5) | 3523 (69.6) | |
| Every day | 2396 (9.8) | 1584 (8.2) | 812 (16.1) | |
| Dental outcome: | ||||
| Dental caries | ||||
| Yes | 9340 (38.3) | 7137 (37.0) | 2203 (43.5) | <0.01 ** |
| No | 15,034 (61.7) | 12,178 (63.0) | 2856 (56.5) | |
| Decayed teeth (DT) | ||||
| Yes | 7892 (32.4) | 5953 (30.8) | 1939 (38.3) | <0.001 *** |
| No | 16,445 (67.5) | 13,334 (69.0) | 3111 (61.5) | |
| Missing teeth (MT) | ||||
| Yes | 574 (2.4) | 436 (2.3) | 138 (2.7) | <0.05 * |
| No | 23,763 (97.5) | 18,851 (97.6) | 4912 (97.1) | |
| Filled teeth (FT) | ||||
| Yes | 2072 (8.5) | 1651 (8.5) | 421 (8.3) | 0.612 |
| No | 22,265 (91.3) | 17,636 (91.3) | 4629 (91.5) | |
| Variables | Model 1 a | Model 2 b |
|---|---|---|
| OR (95%CI) | OR (95%CI) | |
| Screen time on mobile devices (hour/day) | ||
| <2 | 1.00 | 1.00 |
| ≥2 | 1.32 (1.24–1.40) *** | 1.24 (1.17–1.33) *** |
| Covariates: | ||
| Age (year) | ||
| 12~15 | 1.00 | |
| 16~17 | 1.27 (1.20–1.35) *** | |
| Gender | ||
| Boy | 1.00 | |
| Girl | 1.68 (1.59–1.77) *** | |
| Geographic region | ||
| South | 1.00 | |
| Middle | 1.38 (1.28–1.47) *** | |
| North | 1.05 (0.99–1.12) | |
| Maternal educational level | ||
| Primary school and below | 1.00 | |
| Junior and senior high school | 0.87 (0.80–0.94) ** | |
| More advanced attainment | 0.78 (0.71–0.87) *** | |
| Tooth brushing habit | ||
| Yes | 1.00 | |
| No | 0.99 (0.94–1.06) | |
| Obesity | ||
| Yes | 1.00 | |
| No | 1.28 (1.22–1.36) *** | |
| Parental intervention | ||
| Yes | 1.00 | |
| No | 1.09 (1.03–1.15) ** |
| Variable | Model 1 a | Model 2 b | ||
|---|---|---|---|---|
| Dental Caries | Screen Time on Mobile Devices (hour/day) | Dental Caries | Screen Time on Mobile Devices (hour/day) | |
| β (95%CI) | β (95%CI) | β (95%CI) | β (95%CI) | |
| Screen time on mobile devices (hours/day) | ||||
| <2 | 0 | 0 | ||
| ≥2 | 1.35 (0.97–1.73) *** | 1.27 (0.80–1.75) *** | ||
| The number of co-occupants | 0.03 (0.01–0.04) *** | 0.03 (0.01–0.04) *** | ||
| Corr (screen time on devices, dental caries) | −0.72 *** | −0.67 *** | ||
| Variables | Model 1 a | Model 2 b | Model 2 b | |||
|---|---|---|---|---|---|---|
| Dental Caries | Mediating Effect c | Dental Caries | Mediating Effect c | Dental Caries | Mediating Effect c | |
| Marginal Effect (95%CI) | (% of Association Explained by Sugar-Sweetened Beverages) | Marginal Effect (95%CI) | (% of Association Explained by Sugar-Sweetened Beverages) | Marginal Effect (95%CI) | (% of Association Explained by Sugar-Sweetened Beverages) | |
| Screen time on mobile devices (hours/day) d | <2:≤0 ≥2:0.9 | <2:≤0 ≥2:0.7 | <2:≤0 ≥2:0.7 | |||
| <2 | 0.371 (0.364–0.377) *** | 0.374 (0.367–0.380) *** | 0.374 (0.351–0.396) *** | |||
| ≥2 | 0.432 (0.419–0.446) *** | 0.420 (0.406–0.434) *** | 0.418 (0.215–0.621) *** | |||
| SSBs intake | ||||||
| Not every day | 0.378 (0.372–0.384) *** | 0.377 (0.371–0.384) *** | 0.377 (0.350–0.405) *** | |||
| Every day | 0.433 (0.413–0.453) *** | 0.440 (0.420–0.459) *** | 0.438 (0.413–0.463) *** | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xue, H.; Wang, X.; Lai, L.; Li, Y.; Huang, F.; Ni, X.; Tian, Y.; Li, M.; Fan, L.; Yang, J.; et al. An Instrumental Analysis of the Triad Association Between Sugar-Sweetened Beverages, Screen Time, and Dental Caries in Adolescents. Future 2024, 2, 149-163. https://doi.org/10.3390/future2040012
Xue H, Wang X, Lai L, Li Y, Huang F, Ni X, Tian Y, Li M, Fan L, Yang J, et al. An Instrumental Analysis of the Triad Association Between Sugar-Sweetened Beverages, Screen Time, and Dental Caries in Adolescents. Future. 2024; 2(4):149-163. https://doi.org/10.3390/future2040012
Chicago/Turabian StyleXue, Hui, Xin Wang, Linyuan Lai, Ying Li, Feng Huang, Xiaoyan Ni, Yong Tian, Meng Li, Lijun Fan, Jie Yang, and et al. 2024. "An Instrumental Analysis of the Triad Association Between Sugar-Sweetened Beverages, Screen Time, and Dental Caries in Adolescents" Future 2, no. 4: 149-163. https://doi.org/10.3390/future2040012
APA StyleXue, H., Wang, X., Lai, L., Li, Y., Huang, F., Ni, X., Tian, Y., Li, M., Fan, L., Yang, J., & Du, W. (2024). An Instrumental Analysis of the Triad Association Between Sugar-Sweetened Beverages, Screen Time, and Dental Caries in Adolescents. Future, 2(4), 149-163. https://doi.org/10.3390/future2040012