
Methenamine as an Alternative Treatment of Neisseria gonorrhoeae Urethritis? An In Vitro and In Vivo Study in Galleria mellonella

 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Neisseria gonorrhoeae Isolates
2.2. Antimicrobial Susceptibility Testing
2.3. Preparation of Live Microbial Inocula for G. mellonella Infection
2.4. Injection of G. mellonella Larvae
2.5. Concentration of Methenamine Injected
2.6. Data Analysis
3. Results
3.1. Minimum Inhibitory Concentrations
3.1.1. In Vitro
3.1.2. Toxicity
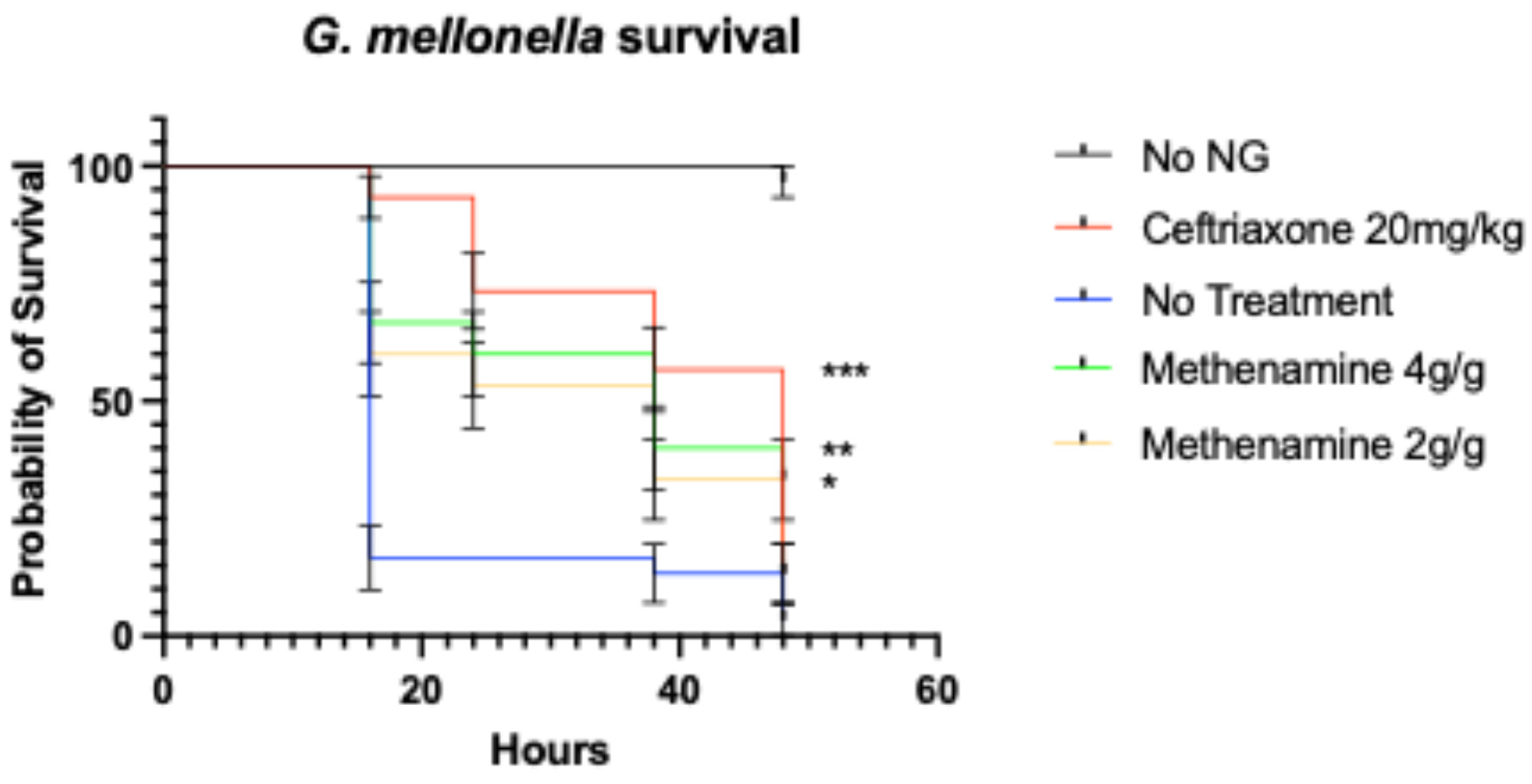
3.1.3. Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| MIC | Minimum Inhibitory Concentration |
| RCT | Randomized Controlled Trial |
References
- Unemo, M.; Bradshaw, C.S.; Hocking, J.S.; de Vries, H.J.C.; Francis, S.C.; Mabey, D.; Marrazzo, J.M.; Sonder, G.J.B.; Schwebke, J.R.; Hoornenborg, E.; et al. Sexually transmitted infections: Challenges ahead. Lancet Infect. Dis. 2017, 17, 235–279. [Google Scholar] [CrossRef] [PubMed]
- Cyr, S.S.; Barbee, L.; Workowski, K.A.; Bachmann, L.H.; Pham, C.; Schlanger, K.; Torrone, E.; Weinstock, H.; Kersh, E.N.; Thorpe, P. Update to CDC’s treatment guidelines for gonococcal infection. Morb. Mortal. Wkly. Rep. 2020, 69, 1911–1916. [Google Scholar] [CrossRef]
- Unemo, M.; Ross, J.; Serwin, A.B.; Gomberg, M.; Cusini, M.; Jensen, J.S. 2020 European guideline for the diagnosis and treatment of gonorrhoea in adults. Int. J. STD AIDS 2020, 69, 345–351. Available online: https://www.ncbi.nlm.nih.gov/pubmed/33121366 (accessed on 12 March 2025). [CrossRef]
- Alirol, E.; Wi, T.E.; Bala, M.; Bazzo, M.L.; Chen, X.-S.; Deal, C.; Dillon, J.-A.R.; Kularatne, R.; Heim, J.; Huijsduijnen, R.H.v.; et al. Multidrug-resistant gonorrhea: A research and development roadmap to discover new medicines. PLoS Med. 2017, 14, 1002366. Available online: https://www.ncbi.nlm.nih.gov/pubmed/28746372 (accessed on 13 March 2025). [CrossRef] [PubMed]
- Kanesaka, I.; Kong, F.Y.S.; Vanbaelen, T.; Santhini Manoharan-Basil, S.; Kenyon, C. An overview of potential combination therapies with ceftriaxone as a treatment for gonorrhoea. Expert Rev. Anti Infect. Ther. 2025, 23, 459–467. [Google Scholar] [CrossRef] [PubMed]
- Unemo, M. Current and future antimicrobial treatment of gonorrhoea—The rapidly evolving Neisseria gonorrhoeae continues to challenge. BMC Infect. Dis. 2015, 15, 364. Available online: https://www.ncbi.nlm.nih.gov/pubmed/26293005 (accessed on 16 March 2025). [CrossRef]
- Altinoz, M.A.; Ozpinar, A.; Ozpinar, A.; Perez, J.L.; Elmaci, İ. Methenamine’s journey of 160 years: Repurposal of an old urinary antiseptic for treatment and hypoxic radiosensitization of cancers and glioblastoma. Clin. Exp. Pharmacol. Physiol. 2019, 46, 407–412. [Google Scholar] [CrossRef]
- Lo, T.S.; Hammer, K.D.; Zegarra, M.; Cho, W.C. Methenamine: A forgotten drug for preventing recurrent urinary tract infection in a multidrug resistance era. Expert Rev. Anti Infect. Ther. 2014, 12, 549–554. [Google Scholar] [CrossRef]
- Klinge, E.; Männistö, P.; Mäntylä, R.; Lamminsivu, U.; Ottoila, P. Pharmacokinetics of methenamine in healthy volunteers. J. Antimicrob. Chemother. 1982, 9, 209–216. [Google Scholar] [CrossRef]
- Li, J.M.; Cosler, L.E.; Harausz, E.P.; Myers, C.E.; Kufel, W.D. Methenamine for urinary tract infection prophylaxis: A systematic review. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2024, 44, 197–206. [Google Scholar] [CrossRef]
- Mary Ann Liebert, Inc. Final Report on the Safety Assessment of Methenamine. J. Am. Coll. Toxicol. 1992, 11, 531–558. [Google Scholar]
- Gu, C.; Ackerman, A.L. An oldie but a goodie: Methenamine as a nonantibiotic solution to the prevention of recurrent urinary tract infections. PLoS Pathog. 2023, 19, 1011405. [Google Scholar] [CrossRef]
- Vanbaelen, T.; Huis in ‘t Veld, D.; Visser, B.J.; De Baetselier, I.; Van Praet, J.T.; Santhini Manoharan-Basil, S.; Van den Bossche, D.; Kenyon, C. Combination therapy for multidrug-resistant Mycoplasma genitalium infections: A case series. Sex. Transm. Infect. 2025. [Google Scholar] [CrossRef]
- Liu, H.; Taylor, T.H.; Pettus, K.; Trees, D. Assessment of Etest as an alternative to agar dilution for antimicrobial susceptibility testing of Neisseria gonorrhoeae. J. Clin. Microbiol. 2014, 52, 1435–1440. [Google Scholar] [CrossRef]
- Lewis II, J.S.; Weinstein, M.P.; Bobenchik, A.M.; Campeau, S.; Cullen, S.K.; Galas, M.F.; Gold, H.; Humphries, R.M.; Kirn, T.J.; Limbago, B. Performance Standards for Antimicrobial Susceptibility Testing: Twenty-Third Informational Supplement, 2022. Clinical and Laboratory Standards Institute. Available online: https://clsi.org/shop/standards/m100/ (accessed on 18 May 2025).
- Hofkens, N.; Gestels, Z.; Abdellati, S.; De Baetselier, I.; Gabant, P.; Martin, A.; Kenyon, C.; Santhini Manoharan-Basil, S. Microbisporicin (NAI-107) protects Galleria mellonella from infection with Neisseria gonorrhoeae. Microbiol. Spectr. 2023, 11, 0282523. [Google Scholar] [CrossRef] [PubMed]
- Gestels, Z.; De Baetselier, I.; Abdellati, S.; Santhini Manoharan-Basil, S.; Kenyon, C. Ramoplanin as a novel therapy for Neisseria gonorrhoeae infection: An in vitro and in vivo study in Galleria mellonella. J. Med. Microbiol. 2024, 73, 001785. [Google Scholar] [CrossRef] [PubMed]
- Dijokaite, A.; Humbert, M.V.; Borkowski, E.; La Ragione, R.M.; Christodoulides, M. Establishing an invertebrate Galleria mellonella greater wax moth larval model of Neisseria gonorrhoeae infection. Virulence 2021, 12, 1900–1920. Available online: https://www.ncbi.nlm.nih.gov/pubmed/34304706 (accessed on 11 February 2025). [CrossRef]
- Andrea, A.; Krogfelt, K.A.; Jenssen, H. Methods and challenges of using the greater wax moth (Galleria mellonella) as a model organism in antimicrobial compound discovery. Microorganisms 2019, 7, 85. [Google Scholar] [CrossRef]
- Serrano, I.; Verdial, C.; Tavares, L.; Oliveira, M. The virtuous Galleria mellonella model for scientific experimentation. Antibiotics 2023, 12, 505. [Google Scholar] [CrossRef] [PubMed]
- Ménard, G.; Rouillon, A.; Cattoir, V.; Donnio, P.-Y. Galleria mellonella as a suitable model of bacterial infection: Past, present and future. Front. Cell Infect. Microbiol. 2021, 11, 782733. [Google Scholar] [CrossRef]
- Wind, C.M.; De Vries, H.J.C.; Van Dam, A.P. Determination of in vitro synergy for dual antimicrobial therapy against resistant Neisseria gonorrhoeae using Etest and agar dilution. Int. J. Antimicrob. Agents 2015, 45, 305–308. [Google Scholar] [CrossRef] [PubMed]
- Pascual, F.; Au, C.; Chikwari, C.D.; Daram, P.; Deal, C.; Espinosa Miranda, A.; Grad, Y.H.; Hook, E.W.; Kittiyaowamarn, R.; Luckey, A.; et al. Recommendations for the optimal introduction of novel antibiotics to treat uncomplicated gonorrhoea in the face of increasing antimicrobial resistance: A case study with zoliflodacin. BMC Glob. Public Health 2024, 2, 58. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Strain ID | Ceftriaxone | Ciprofloxacin | Azithromycin | Methenamine |
|---|---|---|---|---|
| 15.441 | 0.25 | 16 | 0.25 | 300 |
| 17.360 | 0.25 | 16 | 0.5 | 300 |
| 18.227 | 0.19 | 32 | 1 | 300 |
| 18.243 | 0.19 | 16 | 0.25 | 300 |
| 18.293 | 0.19 | 8 | 0.25 | 300 |
| 19.598 | 0.5 | >32 | 0.38 | 300 |
| 20.090 | 0.19 | 32 | 0.25 | 300 |
| 20.442 | 0.19 | 32 | 0.75 | 300 |
| 21.140 | 0.25 | 32 | 0.75 | 300 |
| 21.272 | 0.19 | 32 | 1 | 300 |
| 23.509 | 0.19 | 6 | 0.25 | 300 |
| 24.758 | <0.002 | <0.002 | 0.032 | 300 |
| 24.772 | 0.004 | 3 | 1.5 | 300 |
| 24.773 | 0.003 | 0.002 | 0.003 | 300 |
| 24.774 | <0.002 | 0.002 | 0.5 | 300 |
| ATCC 49226 | 0.008 | 0.002 | 0.25 | 300 |
| WHO X | 2 | >32 | 0.5 | 300 |
| WHO Y | 1 | >32 | 1 | 300 |
| WHO Z | 0.5 | >32 | 1 | 300 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kanesaka, I.; Abdellati, S.; Manoharan-Basil, S.S.; Kenyon, C. Methenamine as an Alternative Treatment of Neisseria gonorrhoeae Urethritis? An In Vitro and In Vivo Study in Galleria mellonella. Venereology 2025, 4, 13. https://doi.org/10.3390/venereology4030013
Kanesaka I, Abdellati S, Manoharan-Basil SS, Kenyon C. Methenamine as an Alternative Treatment of Neisseria gonorrhoeae Urethritis? An In Vitro and In Vivo Study in Galleria mellonella. Venereology. 2025; 4(3):13. https://doi.org/10.3390/venereology4030013
Chicago/Turabian StyleKanesaka, Izumo, Saïd Abdellati, Sheeba Santhini Manoharan-Basil, and Chris Kenyon. 2025. "Methenamine as an Alternative Treatment of Neisseria gonorrhoeae Urethritis? An In Vitro and In Vivo Study in Galleria mellonella" Venereology 4, no. 3: 13. https://doi.org/10.3390/venereology4030013
APA StyleKanesaka, I., Abdellati, S., Manoharan-Basil, S. S., & Kenyon, C. (2025). Methenamine as an Alternative Treatment of Neisseria gonorrhoeae Urethritis? An In Vitro and In Vivo Study in Galleria mellonella. Venereology, 4(3), 13. https://doi.org/10.3390/venereology4030013