
Piercing Through: Lefamulin Treatment of an Antibiotic-Resistant Mycoplasma Genitalium Urethritis

{kind=link}
Abstract
1. Introduction
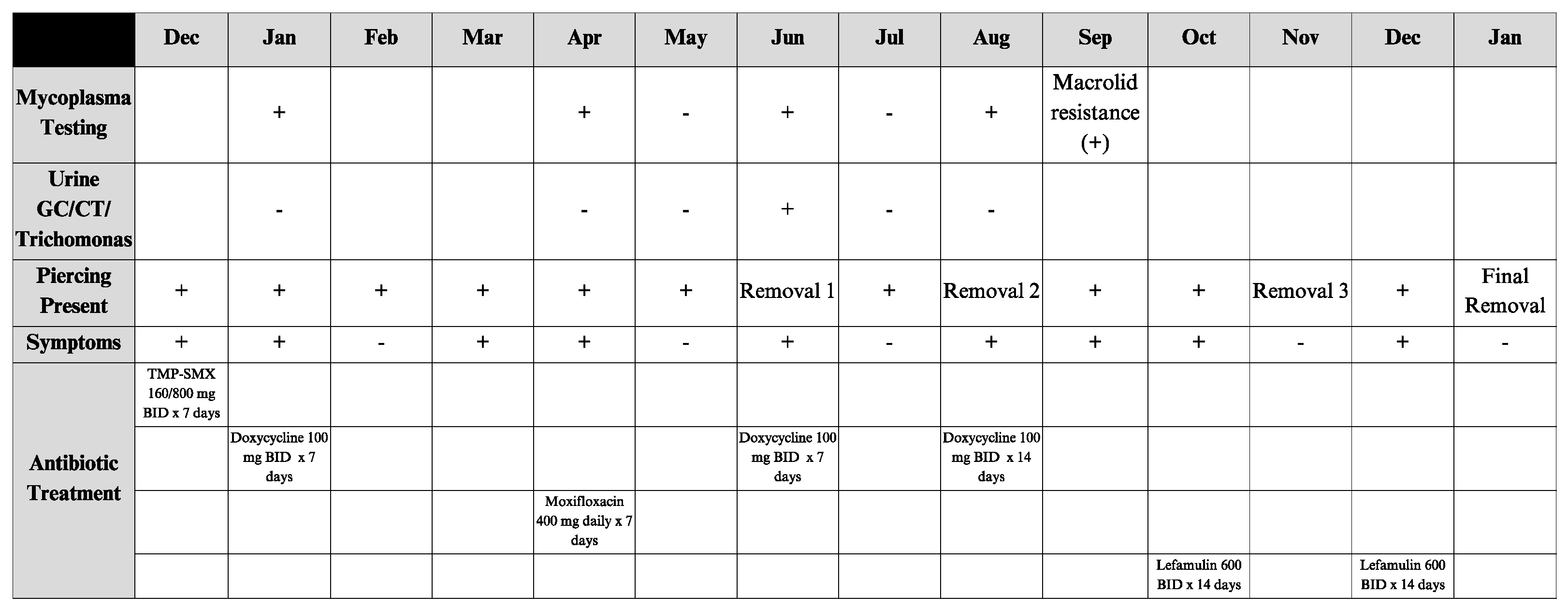
2. Case
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| MDR | Multidrug-resistant |
| M. genitalium | Mycoplasma genitalium |
| STIs | Sexually transmitted infections |
| MDR | Multidrug-resistant |
| TMP-SMX | Sulfamethoxazole-trimethoprim |
| NAAT | Nucleic Acid Amplification Test |
| MSM | Male who has sexual intercourse with men |
| HIV | Human immunodeficiency virus |
| UTI | Urinary tract infection |
| CDC | Centers for Disease Control |
| MICs | Minimum inhibitor concentrations |
References
- Taylor-Robinson, D.; Jensen, J.S. Mycoplasma genitalium: From Chrysalis to multicolored butterfly. Clin. Microbiol. Rev. 2011, 24, 498–514. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Manhart, L.E. Mycoplasma genitalium: An emergent sexually transmitted disease? Infect. Dis. Clin. N. Am. 2013, 27, 779–792. [Google Scholar] [CrossRef] [PubMed]
- Workowski, K.A.; Bachmann, L.H.; Chan, P.A.; Johnston, C.M.; Muzny, C.A.; Park, I.; Reno, H.; Zenilman, J.M.; Bolan, G.A. Sexually Transmitted Infections Treatment Guidelines, 2021. MMWR Recomm. Rep. 2021, 70, 1–187. [Google Scholar] [CrossRef]
- Gaydos, C.A. Mycoplasma genitalium: Accurate Diagnosis Is Necessary for Adequate Treatment. J. Infect. Dis. 2017, 216 (Suppl. 2), S406–S411. [Google Scholar] [CrossRef]
- Gnanadurai, R.; Fifer, H. Mycoplasma genitalium: A Review. Microbiology 2020, 166, 21–29. [Google Scholar] [CrossRef] [PubMed]
- McGowin, C.L.; Totten, P.A. The Unique Microbiology and Molecular Pathogenesis of Mycoplasma genitalium. J. Infect. Dis. 2017, 216 (Suppl. 2), S382–S388. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Yiwen, C.; Yueyue, W.; Lianmei, Q.; Cuiming, Z.; Xiaoxing, Y. Infection strategies of mycoplasmas: Unraveling the panoply of virulence factors. Virulence 2021, 12, 788–817. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- DiMarco, D.E.; Urban, M.A.; McGowan, J.P.; Fine, S.M.; Vail, R.; Merrick, S.T.; Radix, A.E.; Gonzalez, C.J.; Hoffmann, C.J. Mycoplasma Genitalium Management in Adults; New York State Department of Health AIDS Institute: Albany, NY, USA, 2022. [Google Scholar]
- Sethi, S.; Zaman, K.; Jain, N. Mycoplasma genitalium infections: Current treatment options and resistance issues. Infect. Drug. Resist. 2017, 10, 283–292. [Google Scholar] [CrossRef]
- CDC. Mycoplasma genitalium—STI Treatment Guidelines. Available online: https://www.cdc.gov/std/treatment-guidelines/mycoplasmagenitalium.htm (accessed on 23 March 2025).
- Schwebke, J.R.; Rompalo, A.; Taylor, S.; Sena, A.C.; Martin, D.H.; Lopez, L.M.; Lensing, S.; Lee, J.Y. Re-evaluating the treatment of nongonococcal urethritis: Emphasizing emerging pathogens-a randomized clinical trial. Clin. Infect. Dis. 2010, 52, 163–170. [Google Scholar] [CrossRef]
- Manhart, L.E.; Gillespie, C.W.; Lowens, M.S.; Khosropour, C.M.; Colombara, D.V.; Golden, M.R.; Hakhu, N.R.; Thomas, K.K.; Hughes, J.P.; Jensen, N.L.; et al. Standard treatment regimens for Nongonococcal urethritis have similar but declining cure rates: A randomized controlled trial. Clin. Infect. Dis. 2012, 56, 934–942. [Google Scholar] [CrossRef]
- Mena, L.A.; Mroczkowski, T.F.; Nsuami, M.; Martin, D.H. A randomized comparison of azithromycin and doxycycline for the treatment of mycoplasma genitalium–positive urethritis in men. Clin. Infect. Dis. 2009, 48, 1649–1654. [Google Scholar] [CrossRef]
- Gossé, M.; Nordbø, S.A.; Pukstad, B. Evaluation of treatment with two weeks of doxycycline on macrolide-resistant strains of Mycoplasma genitalium: A retrospective observational study. BMC Infect. Dis. 2021, 21, 1225. [Google Scholar] [CrossRef]
- Getman, D.; Jiang, A.; O’Donnell, M.; Cohen, S. Mycoplasma genitalium prevalence, coinfection, and macrolide antibiotic resistance frequency in a multicenter clinical study cohort in the United States. J. Clin. Microbiol. 2016, 54, 2278–2283. [Google Scholar] [CrossRef]
- Lau, A.; Bradshaw, C.S.; Lewis, D.; Fairley, C.K.; Chen, M.Y.; Kong, F.Y.; Hocking, J.S. The efficacy of azithromycin for the treatment of genital mycoplasma genitalium: A systematic review and meta-analysis. Clin. Infect. Dis. 2015, 61, 1389–1399. [Google Scholar] [CrossRef]
- Samra, R.S.; Plummer, E.L.; Vodstrcil, L.A.; Aguirre, I.; Clarke, E.J.; Fairley, C.K.; Chow, E.P.; Bradshaw, C.S. Efficacy of sitafloxacin for mycoplasma genitalium in an era of increasing antimicrobial resistance. Open Forum Infect. Dis. 2023, 10, ofad590. [Google Scholar] [CrossRef]
- Terada, M.; Ohki, E.; Yamagishi, Y.; Izumi, K.; Mikamo, H. Antimicrobial efficacies of several antibiotics against uterine cervicitis caused by mycoplasma genitalium. J. Infect. Chemother. 2012, 18, 313–317. [Google Scholar] [CrossRef]
- Li, Y.; Le, W.-J.; Li, S.; Cao, Y.-P.; Su, X.-H. Meta-analysis of the efficacy of moxifloxacin in treating mycoplasma genitalium infection. Int. J. STD AIDS 2017, 28, 1106–1114. [Google Scholar] [CrossRef]
- Clarke, E.J.; Vodstrcil, L.A.; Plummer, E.L.; Aguirre, I.; Samra, R.S.; Fairley, C.K.; Chow, E.P.; Bradshaw, C.S. Efficacy of Minocycline for the treatment of mycoplasma genitalium. Open Forum Infect. Dis. 2023, 10, ofad427. [Google Scholar] [CrossRef]
- Htaik, K.; Vodstrcil, L.A.; Plummer, E.L.; Matthews, L.G.; Aguirre, I.; Chow, E.P.; Fairley, C.K.; Bradshaw, C.S. Efficacy and tolerability of the combination of minocycline and metronidazole for macrolide-resistant mycoplasma genitalium. J. Antimicrob. Chemother. 2025, dkaf142. [Google Scholar] [CrossRef] [PubMed]
- Gautier-Bouchardon, A.V. Antimicrobial Resistance in Mycoplasma spp. Microbiol Spectr. 2018, 6, 4. [Google Scholar] [CrossRef] [PubMed]
- Paukner, S.; Gruss, A.; Jensen, J.S. In Vitro Activity of Lefamulin against Sexually Transmitted Bacterial Pathogens. Antimicrob. Agents Chemother. 2018, 62, 10-1128. [Google Scholar] [CrossRef] [PubMed]
- Salado-Rasmussen, K.; Nørgaard, C.; Pedersen, T.R.; Paukner, S.; Jensen, J.S. In vitro test of the novel antibiotic lefamulin alone and in combination with doxycycline against mycoplasma genitalium. Antimicrob. Agents Chemother. 2025, 69, e01346-24. [Google Scholar] [CrossRef] [PubMed]
- Jacobsson, S.; Golparian, D.; Oxelbark, J.; Wicha, W.W.; da Costa, R.M.; Franceschi, F.; Brown, D.; Louie, A.; Gelone, S.P.; Drusano, G.; et al. Pharmacodynamic evaluation of lefamulin in the treatment of gonorrhea using a hollow fiber infection model simulating neisseria gonorrhoeae infections. Front. Pharmacol. 2022, 13, 1035841. [Google Scholar] [CrossRef] [PubMed]
- Kalichman, S.C.; Cherry, C.; Kalichman, M.O.; Washington, C.; Grebler, T.; Hoyt, G.; Merely, C.; Welles, B. Sexual Behaviors and Transmission Risks Among People Living with HIV: Beliefs, Perceptions, and Challenges to Using Treatments as Prevention. Arch. Sex. Behav. 2016, 45, 1421–1430. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yuchi, S.; Slotky, N.; Moore, L.; Striker, R. Piercing Through: Lefamulin Treatment of an Antibiotic-Resistant Mycoplasma Genitalium Urethritis. Venereology 2025, 4, 10. https://doi.org/10.3390/venereology4030010
Yuchi S, Slotky N, Moore L, Striker R. Piercing Through: Lefamulin Treatment of an Antibiotic-Resistant Mycoplasma Genitalium Urethritis. Venereology. 2025; 4(3):10. https://doi.org/10.3390/venereology4030010
Chicago/Turabian StyleYuchi, Shukai, Noa Slotky, Laurence Moore, and Rob Striker. 2025. "Piercing Through: Lefamulin Treatment of an Antibiotic-Resistant Mycoplasma Genitalium Urethritis" Venereology 4, no. 3: 10. https://doi.org/10.3390/venereology4030010
APA StyleYuchi, S., Slotky, N., Moore, L., & Striker, R. (2025). Piercing Through: Lefamulin Treatment of an Antibiotic-Resistant Mycoplasma Genitalium Urethritis. Venereology, 4(3), 10. https://doi.org/10.3390/venereology4030010